
Abstract
Keywords
Attention-deficit–hyperactivity disorder (ADHD) is a common childhood psychiatric disorder characterized by developmentally inappropriate levels of hyperactivity, inattention and impulsivity (DSM-IV) [1, 2]. The majority of neuropsychological deficits associated with ADHD involve the executive functions (EFs), such as response inhibition, planning and organization, problem solving and working memory 3–8. Contemporary brain–behaviour models of ADHD integrate the neurocognitive and behavioural impairments with neurobiological data and hypothesize that ADHD arises from disruption to neural networks that involve the prefrontal cortex, basal ganglia and their dopaminergically modulated interconnections 9–14. In contrast to such hypotheses, however, neuropsychological studies generally find no reliable association between the magnitude of impairment on tasks of EF and the severity of behavioural disturbance in ADHD [3, 6, 7], 15–20. Consequently, debate continues regarding the nature of any relationship between neurocognitive impairments and symptoms in ADHD.
One complication when examining relationships between neurocognitive function and symptom levels in ADHD is the high prevalence (40–90%) of comorbid oppositional defiant disorder (ODD) and conduct disorder (CD) in samples recruited from child psychiatry clinics and, to a lesser degree, in samples recruited from the community 21–24. Both ODD and CD are associated with poor neurocognitive performance independent of an ADHD diagnosis [3], 25–27 and many studies report more severe hyperactive, impulsive or inattentive symptoms in ADHD with comorbid ODD or CD [22], 28–30. It is unclear, however, whether the presence of comorbid ODD or CD also increases the magnitude of the EF impairment in ADHD. Some studies report that impairments in EF are greater in children with ADHD and ODD or CD than in children with ADHD without ODD or CD 31–33. Other studies find no additional impairment in EF in children with ADHD and comorbid ODD or CD [4, 29], 34–37. If ODD or CD were associated with more severe impairment in EF in addition to their more severe symptoms, then reliable robust associations between symptom severity and EF are likely to be observed in samples of ADHD + ODD/CD. If, however, the magnitude of impairment in EF in ADHD + ODD/CD is equivalent to that for ADHD alone, but symptom severity is greater, any associations between symptoms and EF function would be weakened. Given this uncertainty, the association between symptom severity and neurocognitive function should be investigated in samples of ADHD that do not contain comorbid ODD or CD.
Studying children with ADHD without cormorbid disruptive disorders is more difficult when attempting to control for DSM-IV subtype [38]. CD and ODD are less prevalent in children with the ADHD-inattentive (ADHD-I) subtype than the ADHD-combined (ADHD-CT) subtype [24, 39]. Therefore, in studies in which ADHD subtype has not been controlled or determined, it is possible that ADHD-I is overrepresented in experimental groups classified as having no comorbid ODD or CD (i.e. pure ADHD). Conversely, children with ADHD-CT may be overrepresented in ADHD + ODD/CD groups. Because ADHD-I may be associated with a less severe profile of neurocognitive impairment than ADHD-CT, researchers may in fact be measuring differences between ADHD subtypes rather than determining the effects of comorbid disruptive disorders on EF 40–43. It is therefore important to control ADHD subtype in neuropsychological studies that seek to determine the effect of ODD or CD on cognitive function in ADHD.
As part of our ongoing research into neurocognitive function in ADHD, we have now recruited enough children with ADHD-CT to obtain estimates of neurocognitive function and symptom levels in groups with (i) ADHD alone, (ii) ADHD with CD, and (iii) ADHD with ODD. Therefore, the first aim of the study was to measure the effect of comorbid ODD and CD on symptom levels in ADHD. It was hypothesized that children with ADHD and comorbid disruptive behaviour disorders would be rated higher on measures of ADHD symptoms than children with ADHD alone. The second aim was to determine the relationship between neurocognitive impairment and symptom severity in the different groups of children with ADHD-CT with or without a cormorbid disruptive behaviour disorder. We hypothesized that ADHD children with comorbid disruptive behaviour disorders would show greater impairment on the neurocognitive tests than children with ADHD alone.
Methods
Participants
The current sample was selected from a database of 200 children with ADHD-CT, who had undergone a comprehensive assessment of behavioural symptoms, neurocognitive function, intellectual functions and academic performance. All children were recruited from referrals to a specialist ADHD clinic in metropolitan Melbourne, Australia [44] and were aged between 6 and 12 years old. All were living with at least one biological parent and were attending general primary schools. All children had a full-scale IQ (FSIQ) score >75, and were excluded if they had any neurological and/or endocrine conditions, bipolar or psychotic disorders as established through parental interview. All diagnoses were confirmed by a consultant psychiatrist and administration of the IQ, academic and neuropsychological tests were performed by registered or trainee clinical psychologists. To be classified as ADHD, children were required to meet DSM-IV criteria for ADHD-CT based on diagnostic DSM-IV semi-structured interview administered to at least one parent to establish diagnoses of ADHD and other existing disorders including ODD, CD. The Child Behaviour Checklist (CBCL; parent and teacher forms) and the Conners’ Global Index (CGI; parent and teacher forms) were obtained to confirm pervasive impairment and to rate the severity of the disorder.
To be included in the current study, all children with ADHD were required to be medication naïve. Twenty-three children who did not meet the DSM-IV criteria for ODD or CD were identified (ADHD only). Twenty children who met the clinical criteria for ADHD and CD were identified (ADHD/CD). Twenty-two children were randomly selected from the remainder of the sample, all of whom met the clinical criteria for ADHD and ODD (ADHD/ODD). Twenty-five children who were healthy control participants were recruited from local primary schools. They did not manifest any medical and psychiatric disorders, via the same structured clinical interview and parent/teacher questionnaires used to define the three ADHD groups. The demographic characteristics of these four groups were inspected to determine whether there were any differences in age, gender distribution or intelligence between the groups (Table 1).
Measures
The Anxiety Disorders Interview Schedule for DSM-IV (ADIS-parent form) is a semi-structured interview designed for the diagnosis of psychiatric disorders in children and adolescents. Symptoms are judged by the parent as present or absent and the total number of affirmative responses is calculated to obtain a symptom score. If the number of symptoms present meets DSM-IV criteria, the parent is asked the extent to which the symptoms cause impairment or interference for the child. Impairment ratings are made using an 8-point scale, and must be ≥4 to be diagnostically relevant [45].
The CBCL is a widely used standardized instrument for the assessment of behavioural problems and competencies. The questionnaire consists of 118 behaviour problem items rated on a 3-point scale (0 = not true to 2 = very true) as to how well each describes the child over the past 6 months. An externalizing subscale, composed mainly of ODD/CD symptoms, and an ADHD subscale are generated from parent (CBCL) and teacher (Teacher Report Form (TRF)) ratings. T scores (norms) are provided for children aged 4–5, 6–11 and 12–16 by gender [46].
The CGI is a 10-item questionnaire particularly useful for screening for the core symptoms of ADHD [47]. Items are rated on a 4-point scale (0 = not at all to 3 = very much) indicating the extent to which the child has been affected by the problem (e.g. constantly fidgeting) during the past month [47].
The Wechsler Intelligence Scale for Children–third Edition was used to provide FSIQ scores. Eleven of the 13 WISC-III subtests were administered, with the exception of Symbol Search and Mazes [48].
Computerized neuropsychological tasks
Cognitive function was assessed using tests from the (Cambridge Neuropsychologist Test Automated Battery (CANTAB)). The CANTAB is a series of computerized tests presented to subjects on a high-resolution IBM colour monitor with a touch-sensitive screen. The six subtests used in this study were mostly administered in one testing session lasting no more than 70 min. Participants were seated approximately 50 cm from the monitor with the instruction that they were required to respond to stimuli by touching the screen. The tests have been described extensively in the literature and will be outlined only briefly here. Based on findings from past studies using the same neurocognitive tests in children with ADHD, only tasks that previously demonstrated impairment in ADHD were included here [8, 49, 50], or those that demonstrated a large effect between control and ADHD groups.
The Spatial Span task is a computerized version of the Corsi Block Tapping Test that measures the subject's ability to remember a sequence of squares presented on the screen. After an incorrect attempt at choosing the squares in sequence, the next trial remained at the same difficulty level. The spatial short-term memory span was calculated at the highest level at which the subject successfully remembered at least one sequence of boxes [51].
The Spatial Working Memory task is a self-ordered searching task that measures working memory for spatial stimuli and requires the subject to use mnemonic information to work towards a goal. Subjects were required to search through boxes that appeared on the screen with the aim of finding the blue tokens hidden inside. Returning to an empty box already targeted (and hence emptied of its blue token) on a particular search constituted a ‘forgetting’ or ‘between search’ error (BSE). After two practice trials with two boxes, there were four test trials with each of two, three, four, six and eight boxes [52].
The Delayed Matching to Sample (DMTS) task assessed the ability to recall a complex target stimulus (an abstract pattern), which was presented on the screen for 4 s. In the simultaneous trials, the target stimulus remained on the screen with the choice stimuli. In the delayed matching trials, the target stimulus was removed followed by a 0, 4 or 12 s delay before the choice stimuli was presented. In all trials, subjects were required to choose the target stimulus in a four-alternative forced choice procedure. Performance was measured according to the percentage of correct responses at the simultaneous and each of the delay levels [53].
The spatial recognition task assessed the ability to recognize spatial locations of target stimuli. Four sets, each with five stimuli, were presented, and performance was defined as the percentage of correct responses for the 20 trials [51].
The Tower of London task (TOL) assessed spatial planning and behavioural inhibition. Subjects were required to rearrange their set of coloured balls so that their positions match a goal arrangement in the other half of the screen. The copying trials are scored by (i) the number of test trials completed within the minimum number of moves and (ii) the total number of moves in excess of the minimum. These provide scores of accuracy. The following trials provide a yoked control condition to measure motor initiation and execution times, independent of thinking times [54].
Procedure
The CBCL and CGI parent and teacher forms were generally completed before the assessment sessions began. The child was given the WISC-III and the academic achievement tests. For younger children, sometimes the academic achievement tests were administered in a separate session. The neurocognitive battery of tests was administered using standard instructions and equipment, and generally took no longer than 70 min to complete. The parents were given the diagnostic interview in a separate session.
Statistical analysis
Performance on the spatial span, spatial recognition, DMTS and TOL was compared between groups using a series of one-way ANOVAs. On the spatial working memory task that contained varying levels of difficulty, performance between groups was compared using a group×level of difficulty repeated measures ANOVA. To investigate any differences between groups in the relationship between scores on the CBCL and the CGI and performance on the neurocognitive tests, Pearson product moment correlation coefficients were calculated. This is appropriate rather than using Spearman's rho because the ordinal variables of the CBCL and CGI are effectively rank transformed. Therefore, Pearson product moment correlation between the ordinal variables (CBCL/CGI) and the continuous neurocognitive variables is appropriate. Significance level was set at p < 0.05. Significant correlations were compared with others using the method described by Crawford et al.[55]: ‘both correlations were converted to Fisher's z and the difference between them divided by the standard error of the difference to yield a normal curve deviate (z)’.
Results
Demographic and clinical characteristics of the sample
Sample characteristics and symptom scores
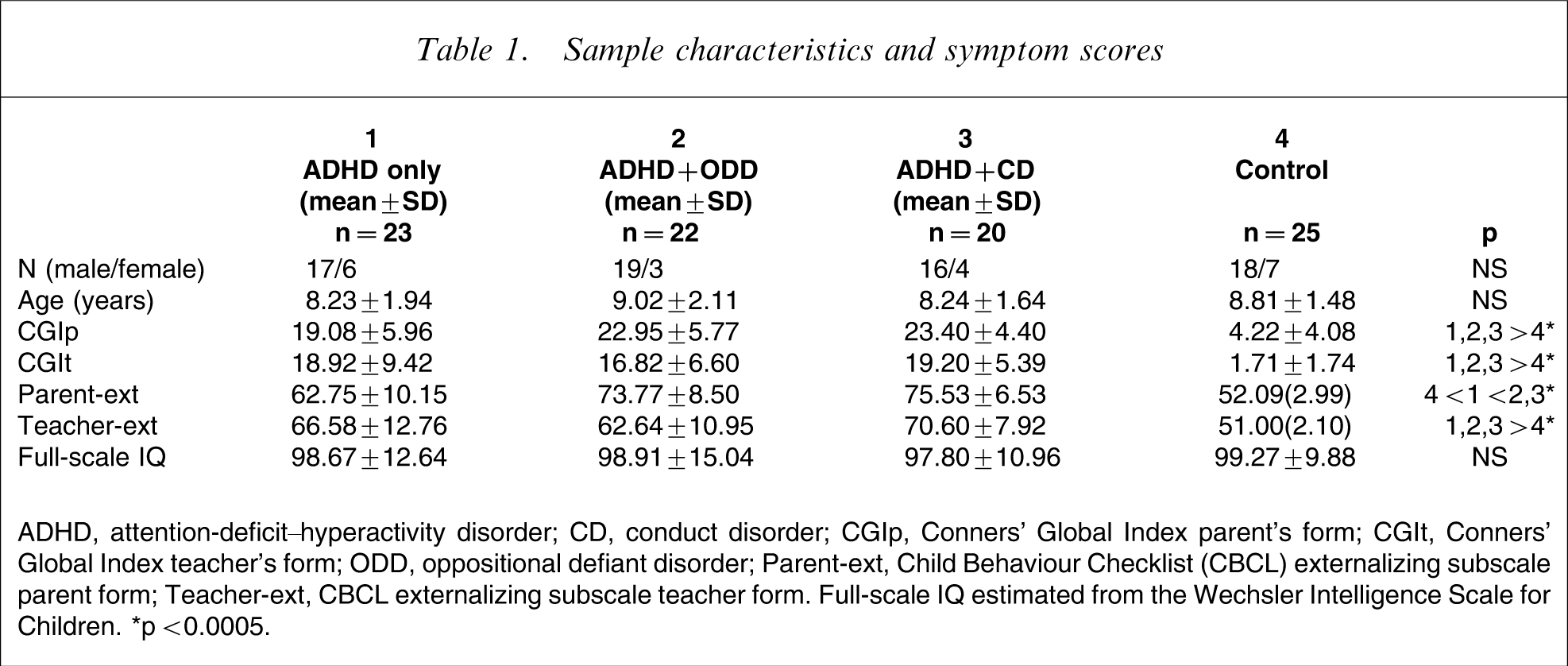
ADHD, attention-deficit–hyperactivity disorder; CD, conduct disorder; CGIp, Conners’ Global Index parent's form; CGIt, Conners’ Global Index teacher's form; ODD, oppositional defiant disorder; Parent-ext, Child Behaviour Checklist (CBCL) externalizing subscale parent form; Teacher-ext, CBCL externalizing subscale teacher form. Full-scale IQ estimated from the Wechsler Intelligence Scale for Children. ∗p < 0.0005.
Neurocognitive performance
Group comparisons on neurocognitive tasks
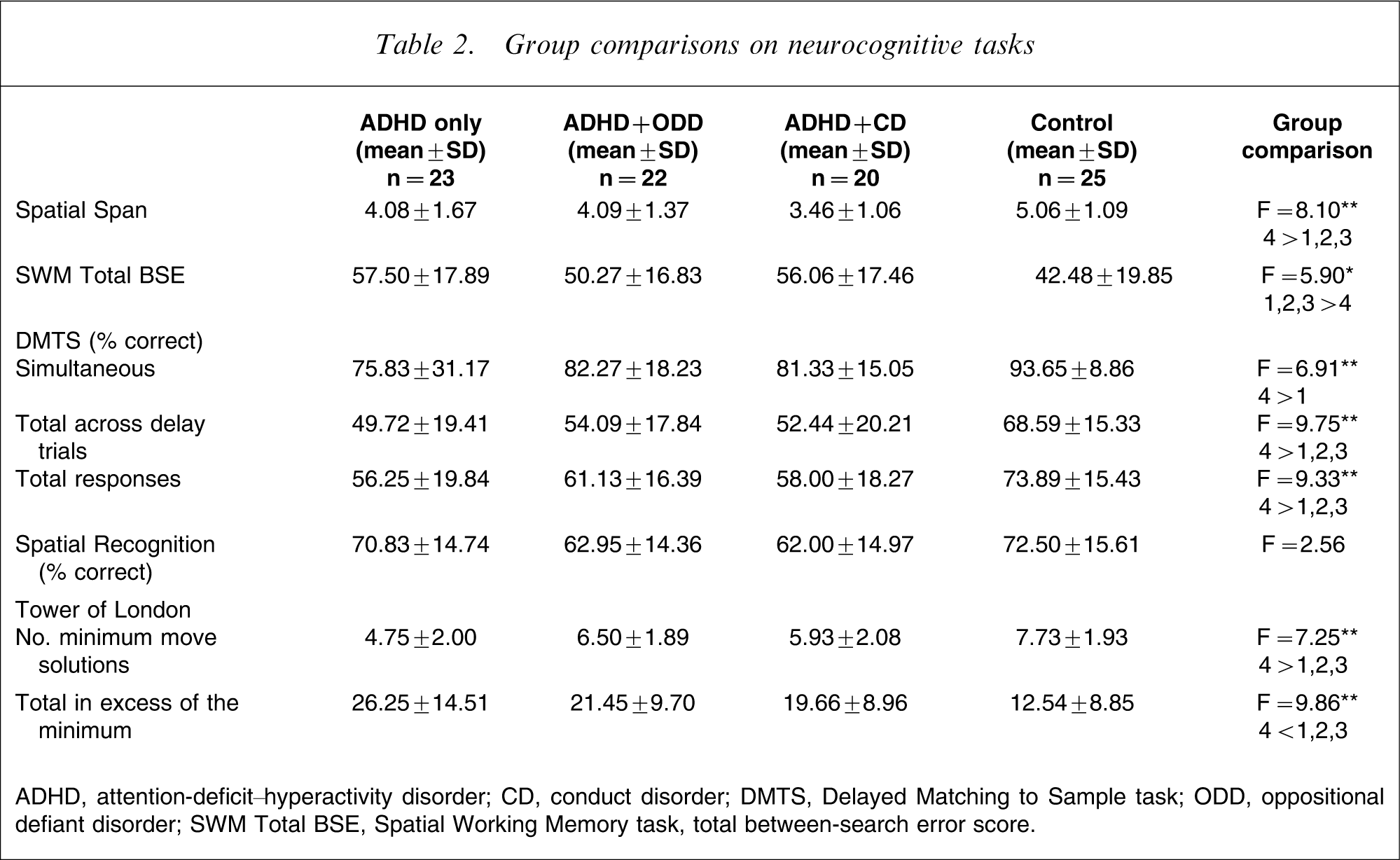
ADHD, attention-deficit–hyperactivity disorder; CD, conduct disorder; DMTS, Delayed Matching to Sample task; ODD, oppositional defiant disorder; SWM Total BSE, Spatial Working Memory task, total between-search error score.
Correlations between neurocognitive measures and severity of symptoms
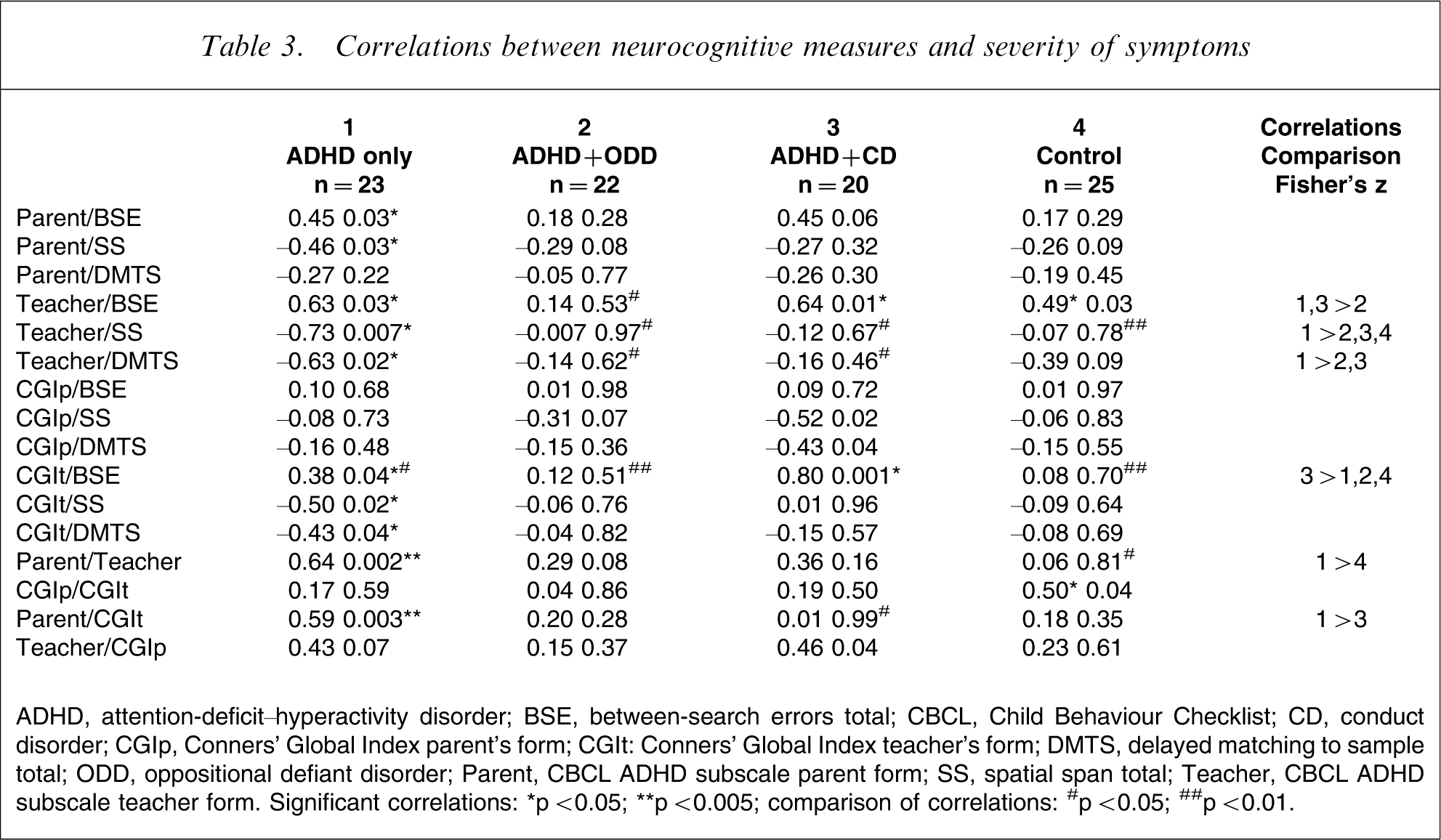
ADHD, attention-deficit–hyperactivity disorder; BSE, between-search errors total; CBCL, Child Behaviour Checklist; CD, conduct disorder; CGIp, Conners’ Global Index parent's form; CGIt: Conners’ Global Index teacher's form; DMTS, delayed matching to sample total; ODD, oppositional defiant disorder; Parent, CBCL ADHD subscale parent form; SS, spatial span total; Teacher, CBCL ADHD subscale teacher form. Significant correlations: ∗p < 0.05; ∗∗p < 0.005; comparison of correlations: #p < 0.05; ##p < 0.01.
Discussion
In the current study we observed no differences in neurocognitive function between children with ADHD-CT with and without ODD or CD. In contrast to this, the severity of externalizing symptoms rated by parents on the CBCL was higher in children with ADHD/CD and ADHD/ODD than in children with ADHD alone. When rated by teachers, children with ADHD/CD were rated as having more severe symptoms than children with ADHD alone, but this was not significant. This trend in mean scores was expected given the selection bias inherent in the current sample, because all children were recruited from a specialist ADHD clinic in a child mental health service.
The strongest associations between teacher symptom ratings and neurocognitive function were identified for the relationships between symptom severity and spatial span, spatial working memory and DMTS in the ADHD alone group. Associations of a similar magnitude were observed between teacher symptom severity and the number of between search errors in the ADHD/CD group. In both groups, these relationships were detected at a significant level (z) only for symptoms rated by teachers.
Taken together, these results suggest that the severity of symptoms is associated with the magnitude of impairment in EF in children with ADHD alone, but that these relationships can be obscured by the presence of comorbid disruptive disorders. If a relationship between ADHD symptoms and impaired EF exists, this lends support to recent neurobiological models that assume that abnormal behaviours and neurocognitive functions in ADHD arise from disruption to the same neural networks or neurobiological systems [10], 56–58. It is unclear whether models such as these can be applied to all children with ADHD, due to the heterogenous nature of the disorder. Taylor highlighted various sources of heterogeneity in ADHD and the various predominant types of symptoms and subtypes that are emerging in the literature examining the cognitive and behavioural symptoms of ADHD [59]. Therefore, children with ADHD and comorbid CD may demonstrate impairments in behaviour and neurocognitive measures likely to have stemmed from a similar underlying dysfunction [60, 61]. ADHD/ODD, however, may be better understood as a maladaptive response to the abnormal behaviours and neurocognitive functions in ADHD [25, 59].
The neurocognitive measures used in the current study were selected on the basis of their demonstrated sensitivity to ADHD in our previous studies [8, 49, 50], and because they have been used successfully with normally developing children in past research [62]. Furthermore, impairments in aspects of EF such as the ability to hold information ‘online’, as is required in the spatial working memory, spatial span and DMTS, have been well documented in ADHD [6]. In our previous studies we found that performance on the measures used here differentiated between unmedicated children with ADHD and healthy controls, with approximately a 44–52% overlap between the two distributions (i.e. effect sizes range between 0.8 and 1.0) [63]. Importantly, the performance of each of the three ADHD-CT subgroups on the EF were impaired, similar to our previous published data [8, 49, 50].
Despite the modest sample sizes in the current study, the magnitude of the relationships between symptom severity and measures of memory and EF detected in the ADHD alone group was larger than any observed in our previous studies (highest correlation: r = 0.31) [8]. Further, the relationships between performance on neuropsychological tests and symptom severity detected in the current study were stronger than in many past neuropsychological studies of ADHD. When detected, most relationships were of low to moderate strength [23, 64]. Many past studies, however, may have included children with comorbid CD or ODD in their ADHD groups. To the best of our knowledge, the contribution of comorbid disorders to the relationship between symptom severity and EF performance has not been examined directly. When considered with the current results, the lack of associations, or small associations observed in previous studies, is not surprising because perhaps the relationship between symptoms and neurocognitive impairment became evident in the current group due to the ADHD subtype and comorbid disruptive behaviour disorders being controlled.
When compared to a normally developing control group, children with ADHD consistently demonstrate impairment on the same EF tasks that were used in the present study [8, 49, 50]. The present study demonstrated that comorbid disruptive behaviour disorders do not necessarily alter the performance of children with ADHD on tasks of EF, despite differing levels of behavioural symptoms. This finding lends support to the premise that ADHD and other disruptive behaviour disorders may reflect a common underlying deficit, and suggests that children with ADHD and comorbid CD may present a more severe form of ADHD [23, 60, 61]. Alternatively, the finding of similar EF impairment in children with ADHD and ADHD with CD and ODD may merely reflect the large overlap in symptoms observed in these childhood disorders. Groups of children who meet the clinical criteria for CD or ODD without ADHD are necessary to investigate the question of whether the EF impairments observed in ADHD are specific to the disorder or reflect a general deficit found in children with any attentional disorder.
Interestingly, no statistically significant relationship (z) was found between parent ratings of behaviour and performance on any EF task. Parent–teacher agreement regarding symptomatology is reportedly low [65, 66], and teachers have been found to rate children's behaviour as less severe than parents, and distinguish less between the subtypes compared with parent ratings [67]. The reliability of parents more than teachers in rating ADHD behaviour has been questioned due to artefactual factors, such as maternal education or single-parent households. In addition, recall biases or halo effects may interfere with objective reporting of parents and/or teachers [22], or the intensity of ADHD symptoms may fluctuate [68]. Therefore, most researchers consider teacher ratings of symptoms to be more reliable than parent ratings.
The present results must be interpreted with caution due to the small sample sizes used. In addition, a selection bias may exist in the current sample, because the children with ADHD were recruited from a hospital outpatient clinic. The current findings need further support by future studies that examine the proposal that relationships between symptom severity and EF impairment are most apparent in children with ADHD-CT without comorbid disruptive disorders and are therefore specific to children with ADHD-CT. In our entire sample of unmedicated children with ADHD-CT, 60% had comorbid ODD and 11% had comorbid CD [8]. High prevalence rates of disruptive disorders are common in clinic-referred samples of ADHD, as was found in the current group [29]. Therefore, ADHD without comorbid disruptive disorders may be relatively rare, especially in groups of children referred to hospital child psychiatry clinics. If this is the case, then the current finding that ADHD symptom level and neurocognitive performance are strongly related in children with ADHD without ODD/CD will apply to a relatively small group of children with ADHD. The present findings may therefore be of greater importance to brain–behaviour models of ADHD than to the management of the disorder itself. Nonetheless, in most cases parents and teachers of children with ADHD-CT could be informed that the severity of a child's symptoms do not predict a great deal about their cognitive function.
In summary, a question of considerable importance in the present study was whether the neurocognitive and behavioural symptoms that characterize ADHD are related, as would be expected given the cotemporary neurocognitive models currently underpinning much of the research into ADHD. In our previous study we found no relationship between symptoms and performance on EF tests. When comorbidity in the sample was controlled for, however, the relationship between teacher-rated symptoms and neurocognitive impairment was strong in the ADHD alone group. The pattern of relationships differed for the comorbid groups, because only the comorbid CD group showed a relationship between teacher ratings of symptoms and the number of between-search errors.