
Abstract
It is commonly accepted that suicidal behaviour is multifaceted and has a complex aetiology. As Leenaars stated, at the end of the day, ‘No one really knows why human beings commit suicide’ [1], p.221]. Suicidal behaviour incorporates a complicated array of demographic, psychiatric, genetic, familial, personality and social factors. Therefore, a social–ecological model that considers how individuals interact with their social and environmental contexts is needed to adequately capture the nature of suicidal behaviour. Suicide is a public health issue the response to which should involve a community-wide risk reduction approach coupled with a focus on the enhancement of protective factors the latter of which is an area not yet exploited by researchers or interventionists [2].
Our knowledge and understanding of the risk factors for suicide attempts is crucial for several reasons including assisting clinicians with risk assessment, designing evidence-based suicide prevention and early intervention efforts, understanding the aetiology of suicide attempts, the development of evidence-based mental health policy, and because suicide attempts is one of the strongest risk factors for completed suicide [3, 4]. It has been acknowledged that still too little is known about suicidal behaviours to adequately inform effective suicide prevention [5].
Prevalence rates for suicidal behaviour among Australian and New Zealand samples of young people range from 0.2% to 1.9% for attempts in the past 12 months, with up to 6.9% (15–24 year olds) and 7.5% (by 21 years of age) having ever tried to kill themselves [6–8]. These rates and the concomitant costs of suicide attempts for the individuals involved, their families, the broader community and the health care system give rise to suicide attempts being a significant mental health issue.
Even a quick perusal of the research on completed suicide and attempted suicide will reveal an overwhelming number of potential risk factors across a range of populations. Beautrais [9] provided a concise review of this literature in which she noted that many of the studies in this area are subject to a series of methodological limitations including: (i) the use of only clinical samples; (ii) no comparison groups of non-suicidal young people; (iii) a lack of longitudinal studies; and (iv) no controlling for confounding factors, sampling bias and measurement error.
The current case–control study overcomes many of these limitations in that it is based on a sample of medically serious suicide attempts compared to a control group of non-suicide attempters drawn from a population-based study. Furthermore, it involves a large sample size allowing for a broad range of potential risk factors to be measured and controlled for in multivariate statistical analysis thereby minimizing the effects of confounding variables. The notion of examining protective factors for suicidal behaviour is in its infancy and Beautrais in her review stated that ‘… relatively little research has focused upon identifying individual, family, and community factors which may protect against the development of suicidal behaviour in young people’ [9], p.428]. In response, the current study investigates several potential protective factors. Because not all risk factors are modifiable, a better understanding of protective factors is invaluable in these circumstances.
Method
Study design and sample
The study design was case–control, with cases recruited from a hospital emergency department and matched controls drawn from a population-based survey. An identical pen and paper self-report questionnaire was used for both the cases and the controls.
The hospital-based sample consisted of 100 participants aged 18–24 years, who presented to the emergency department of a public metropolitan hospital in Queensland, Australia, following a suicide attempt. All emergency department daily attendance sheets were examined over a 9-month period to identify all those young adults treated for self-inflicted injuries. The medical records of those initially selected were then reviewed. The criterion for final inclusion was evidence or strong suspicion that the self-harm was deliberate or suicidally motivated. Cases were excluded if suicidal thoughts were recorded but there was no evidence of a specific act of self-harm or of a suicide attempt. Cases of unintentional self-harm (e.g. accidental overdose) or unconsciously motivated self-harm (e.g. addictive behaviour) were also excluded. A clinical psychologist administered the questionnaire to the hospital-based sample within 1week of their contact with the emergency department. A participation rate of 78.7% was achieved.
The population-based sample was a subset of a survey of young people aged 15–24 years from throughout the state of Queensland. The survey used telephone recruitment followed by an anonymous self-report postal questionnaire. A total of 78 108 telephone calls were made to a random sample of 35 509 households, 4594 (12.9%) eligible households were contacted and 3092 questionnaires were returned, resulting in a participation rate of 67.3%. Only one young person from each household was selected –the 15–24 years old who had the next closest birthday. Details of the methods used for this survey have been published elsewhere [7, 10]. The subset included only those participants who were aged 18–24 years and who reported no history of attempted suicide.
The dataset for the present analysis comprised 95 participants (49 males and 46 females) from the hospital-based sample and 380 matched controls (1:4 matching) from the population-based sample (n=475). The other five participants from the hospital-based sample could not be matched. Matching was conducted by age, gender, indigenous Australian or non-indigenous Australian and location of residence (city or country town/farm). Overall, 230 (48%) participants were female.
Measures
Based on a review of the literature regarding suicidal behaviour the questionnaire was designed using a social–ecological risk and protective factor model. A variety of groupings for risk and protective factors has been used in previous research [11–13]. For instance, Gould et al. [11] use the risk factor categories personal characteristics, family characteristics, adverse life circumstances and socioenvironmental and contextual characteristics; and the protective factor categories family cohesion and religiosity. Six risk factor and four protective factor categories were used in the current study (Tables 1,2).
Measures of risk factors
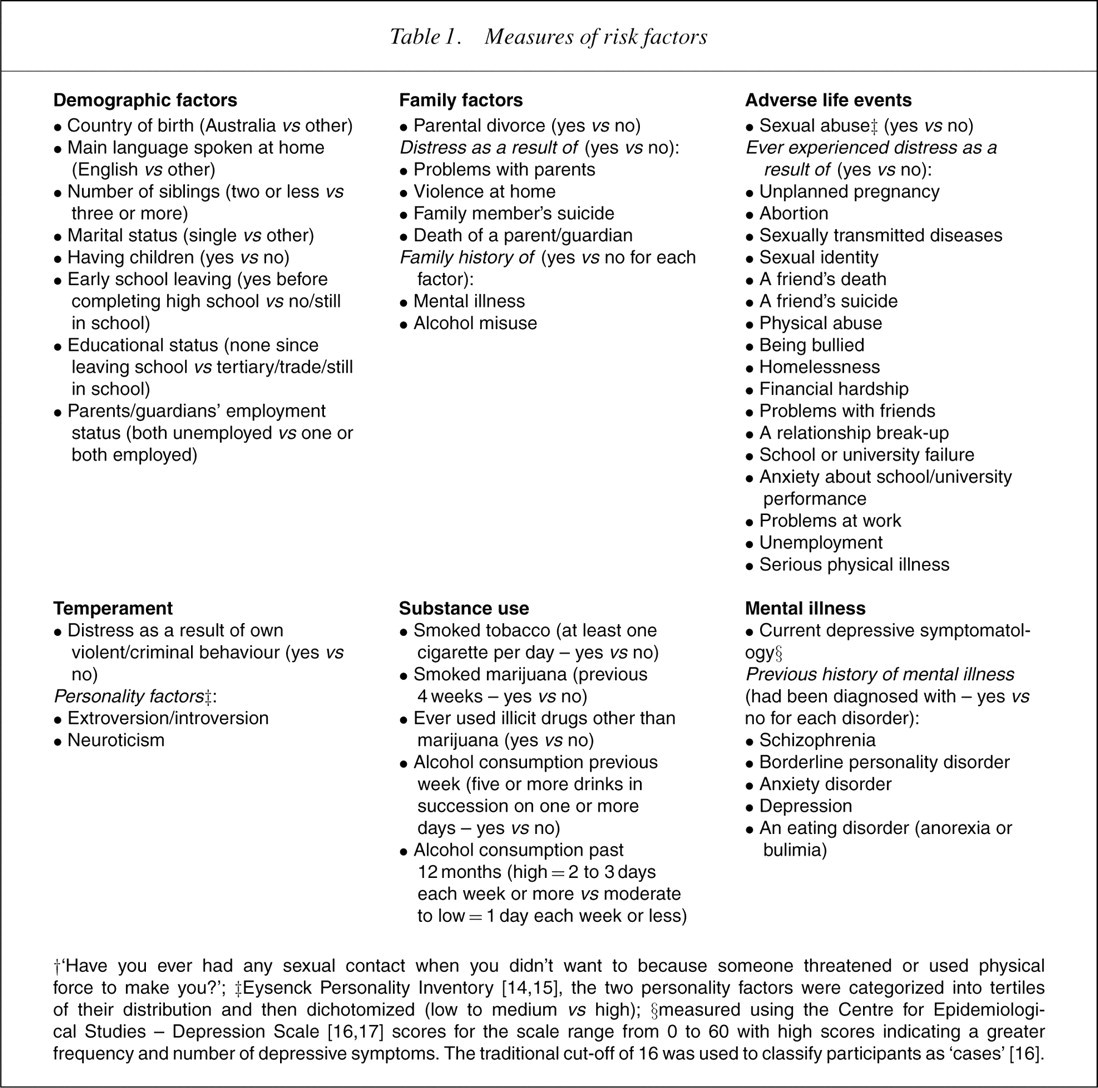
†‘Have you ever had any sexual contact when you didn't want to because someone threatened or used physical force to make you?’; ‡Eysenck Personality Inventory [14, 15], the two personality factors were categorized into tertiles of their distribution and then dichotomized (low to medium vs high); §measured using the Centre for Epidemiologi-cal Studies – Depression Scale [16, 17] scores for the scale range from 0 to 60 with high scores indicating a greater frequency and number of depressive symptoms. The traditional cut-off of 16 was used to classify participants as ‘cases’ [16].
Measures of protective factors
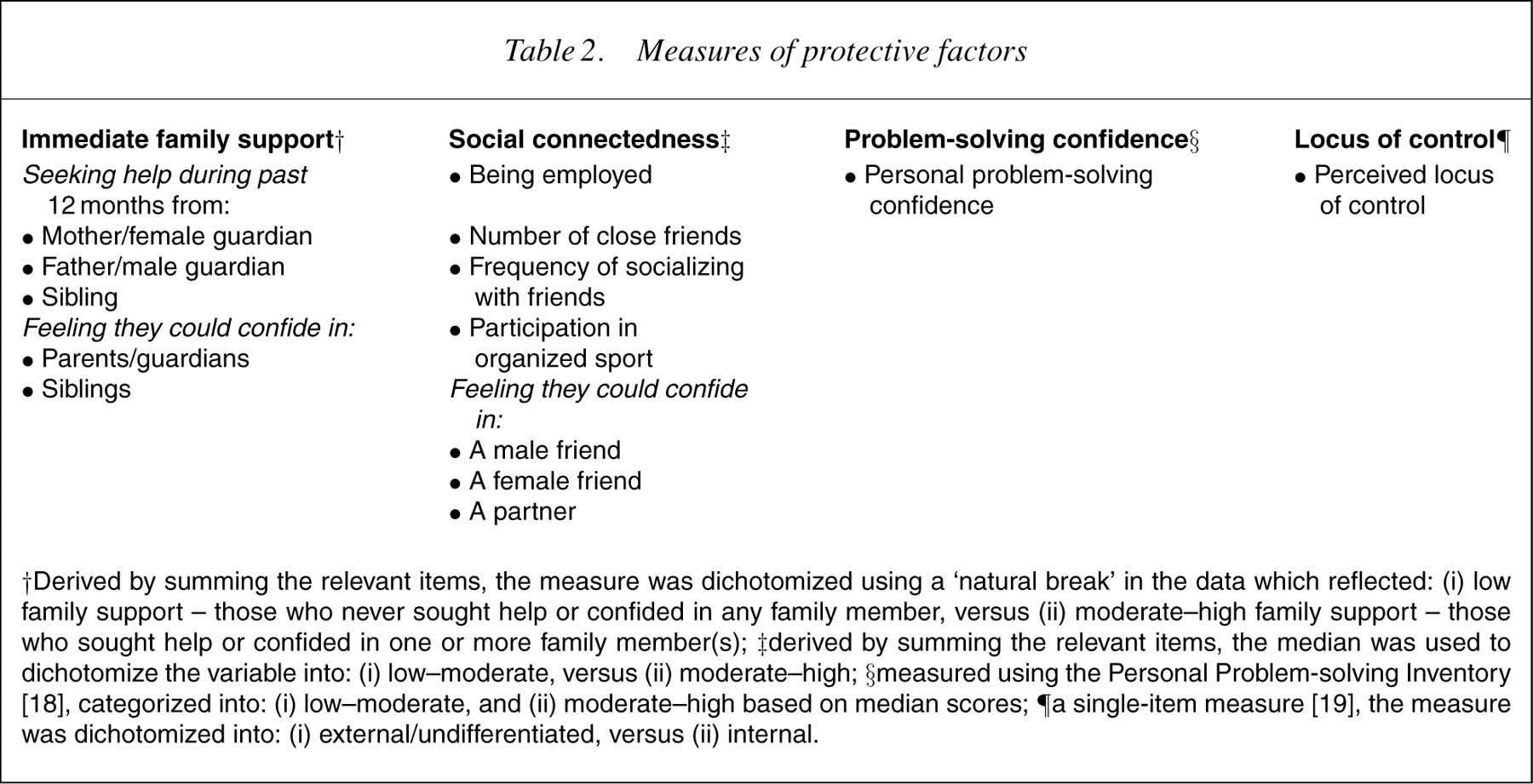
†Derived by summing the relevant items, the measure was dichotomized using a ‘natural break’ in the data which reflected: (i) low family support – those who never sought help or confided in any family member, versus (ii) moderate–high family support – those who sought help or confided in one or more family member(s); ‡derived by summing the relevant items, the median was used to dichotomize the variable into: (i) low–moderate, versus (ii) moderate–high; §measured using the Personal Problem-solving Inventory [18], categorized into: (i) low–moderate, and (ii) moderate–high based on median scores; ¶a single-item measure [19], the measure was dichotomized into: (i) external/undifferentiated, versus (ii) internal.
Analytical method
SPSS version 11.0 and SAS version 8.02 for Windows were used to conduct the analyses. The analysis of the risk factors was undertaken in four stages. Stage one involved chi-squared analyses to estimate the strength of association between the outcome variable (attempted suicide) and each of the risk factors. Because of low numbers in some cells, several of the risk factors were excluded from further analysis. These included schizophrenia, borderline personality disorder, anxiety disorder, eating disorders, distress as the result of suicide of a family member and distress due to abortion.
All other risk factors with a p-value ≤0.1 were included at the second stage of the analysis, which involved a multivariate logistic regression analysis to identify the independently associated risk factors within each of the six risk factor categories. A conservative cut-off for the p-value was used so that potentially important risk factors would not be eliminated in the preliminary analysis. The third stage involved entering those risk factors (from stage two) with a p-value ≤0.1 into a multivariate logistic regression analysis in order to identify the most strongly associated risk factors for attempted suicide. The fourth stage involved entering the interaction effects for gender into the model. A backward elimination procedure [20] was conducted at stages two, three and four. For stages three and four, only those variables with a p-value <0.05 were kept in the models. The final model is presented as a nested model with stratification by gender only for those risk factors having statistically significant interactions with gender. For the purpose of brevity only the results of the stage four analyses are presented.
Protective factors were explored two ways. First, the direct effects of the factors in relation to suicide attempts and second, the effect of protective factors within high- and low-risk subgroups were investigated. For the direct effects, all four protective factors were entered into a logistic regression model and backwards elimination used to remove those risk factors with p<0.05. Interactions between each risk factor and gender were also entered into the model and backwards elimination used to remove those interactions with p<0.05. For the subgroup analysis, only protective factors that were shown to be independently associated with suicide attempts were investigated. Low- and high-risk subgroups were based on the risk factors included in the final model. Tests of heterogeneity were performed using interaction terms in logistic regression models.
Results
Risk factors
The final best-fit multivariate risk factor model included nine risk factors (Table 3). Only two significant interactions for gender emerged. Parental divorce was more likely to be associated with a medically serious suicide attempt for males than females, whereas distress due to problem with parents was more likely to be associated with a suicide attempt for females than males.
Final multivariate logistic regression model of risk factors and gender effects for suicide attempt (attempted suicide n=95; matching controls n=380)
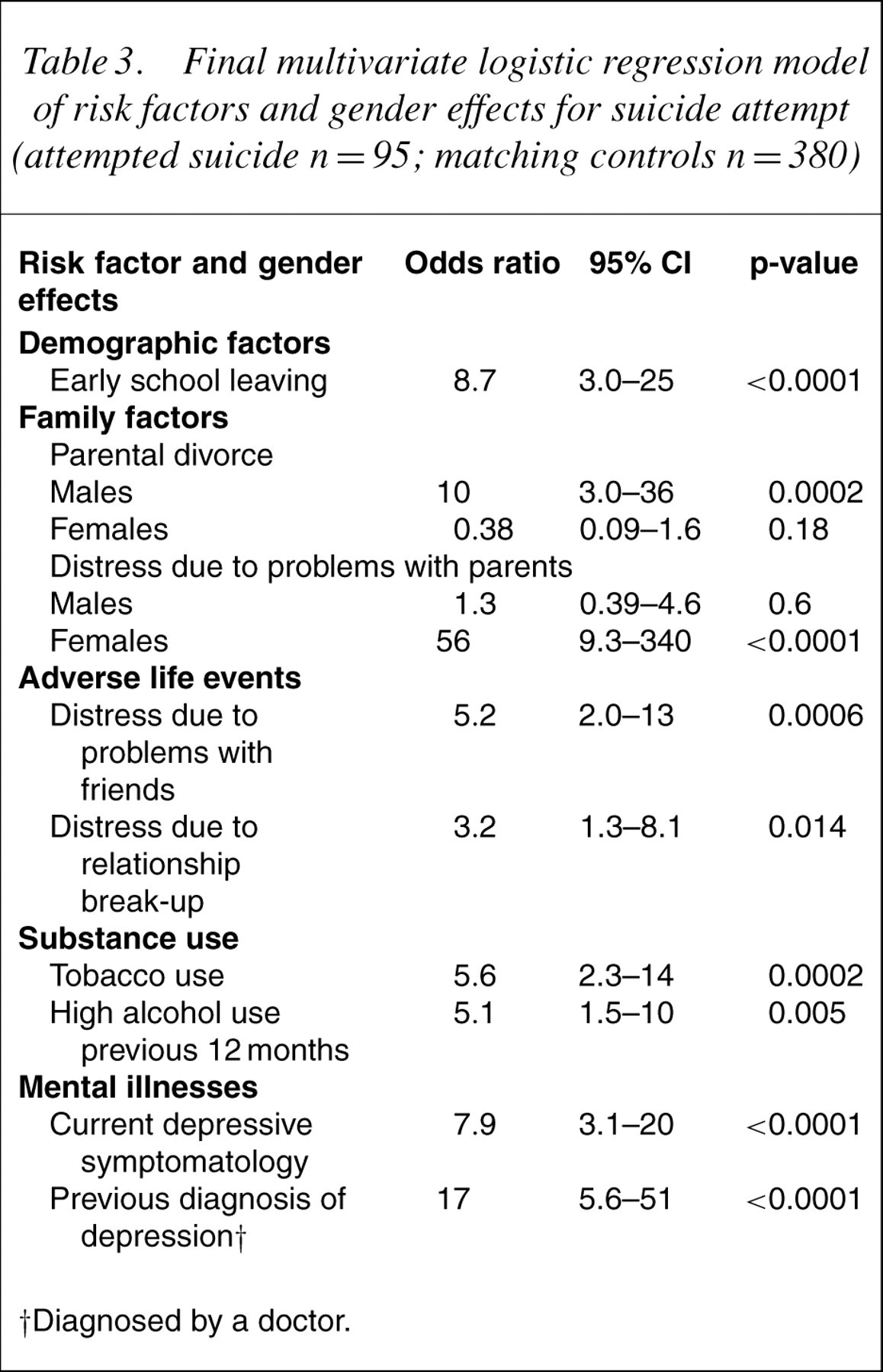
†Diagnosed by a doctor.
Direct effects of the protective factors
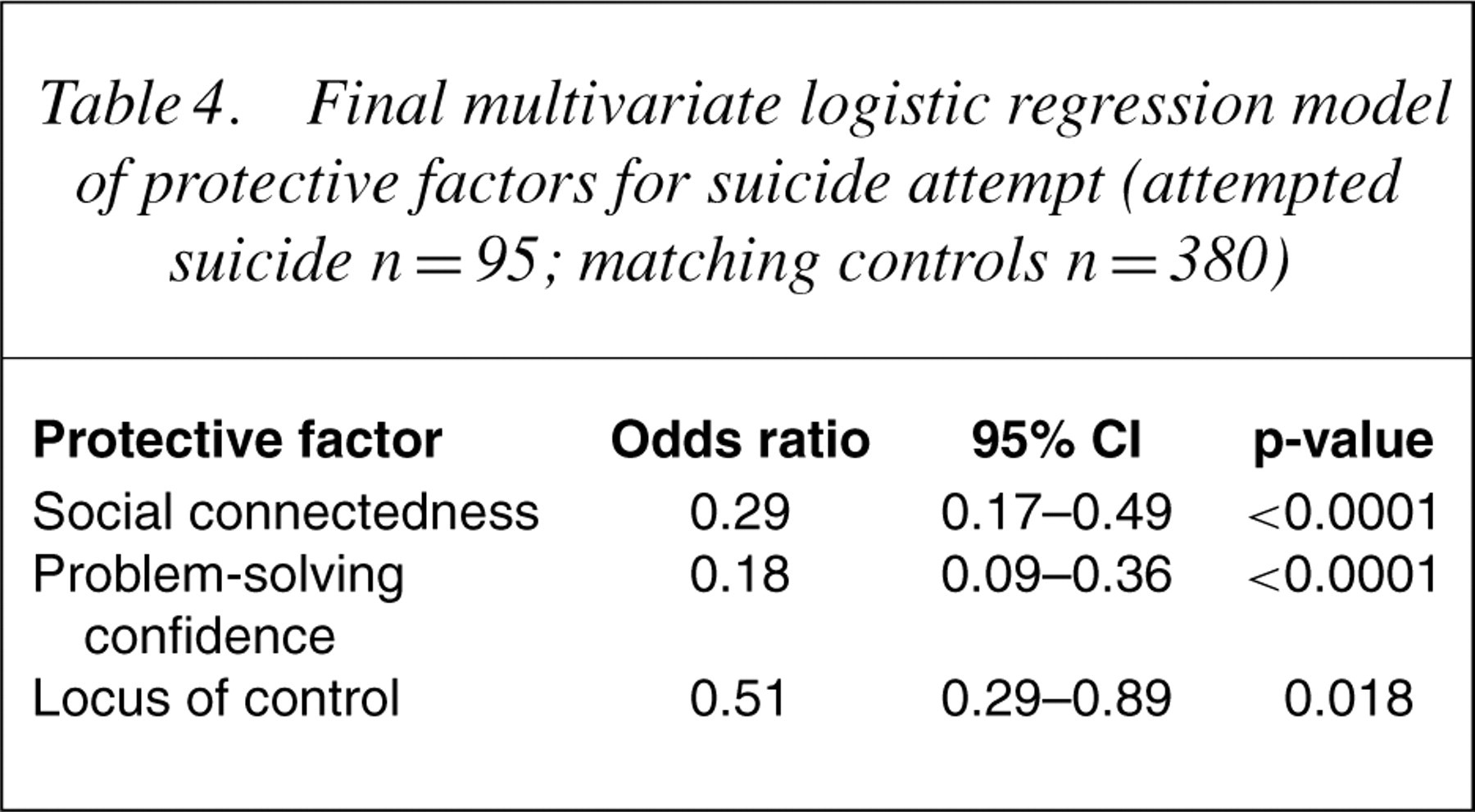
Table 4 shows the protective factors that were significantly associated with a suicide attempt. Social connectedness, problem-solving confidence and an internal locus of control were protective against a suicide attempt. There were no statistically significant effects for gender. Immediate family support was not found to be protective.
Final multivariate logistic regression model of protective factors for suicide attempt (attempted suicide n = 95; matching controls n = 380)
Subgroup analysis of the protective factors
Based on the risk factors that were included in the multivariate regression model we investigated the ‘buffering effect’ of the three independently significant protective factors on both the high- and low-risk groups within each of the nine risk factors. Results from these analyses are displayed in Tables 5–7. Note that the estimates of effect size for protective factors are different in Tables 5–7 compared to Table 4. The estimates presented in Table 4 are based on a multivariate model whereas the estimates presented in Tables 5–7 are based on univariate models.
Subgroup analysis of social connectedness by risk groups
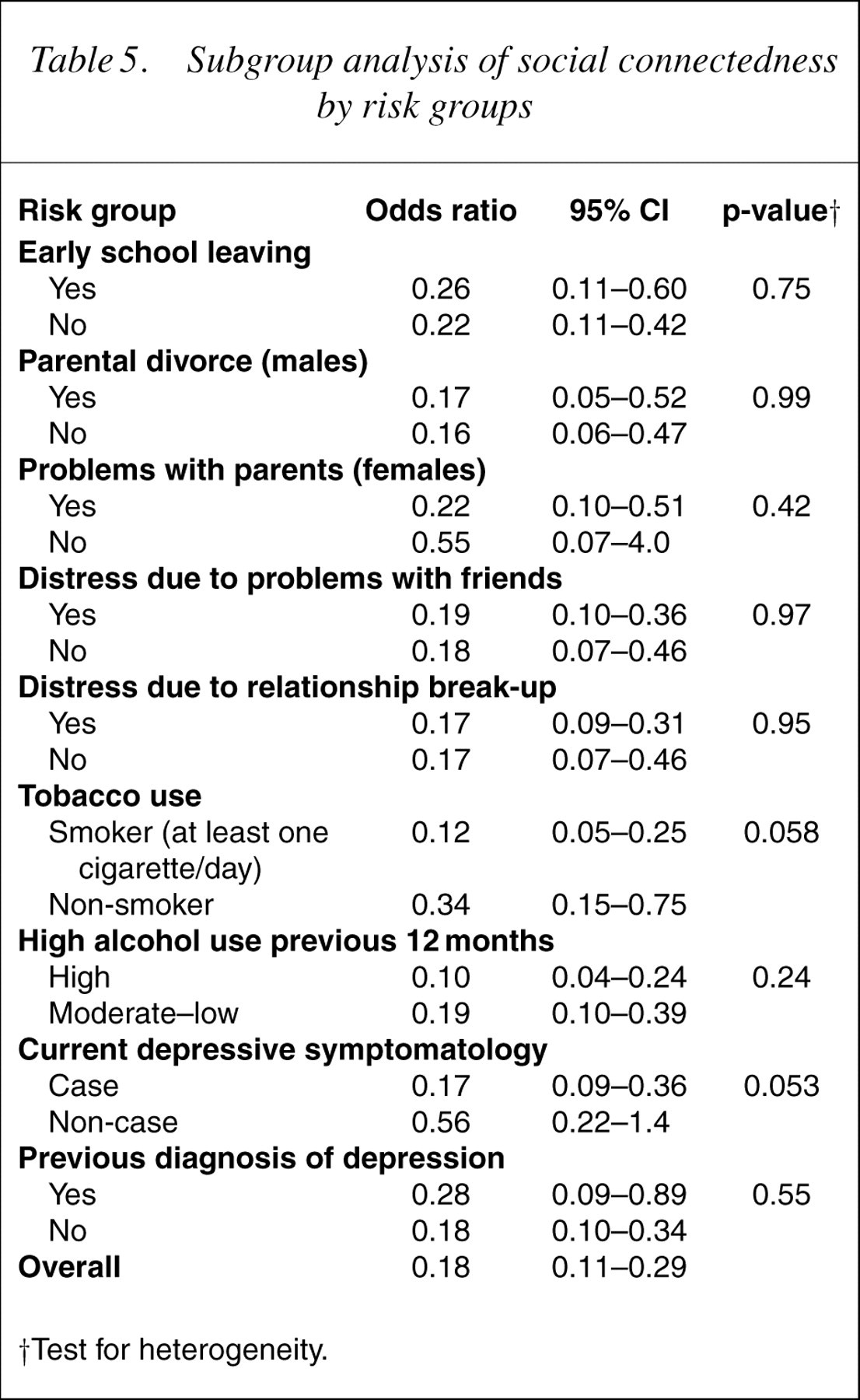
†Test for heterogeneity
Subgroup analysis of problem-solving confidence by risk groups
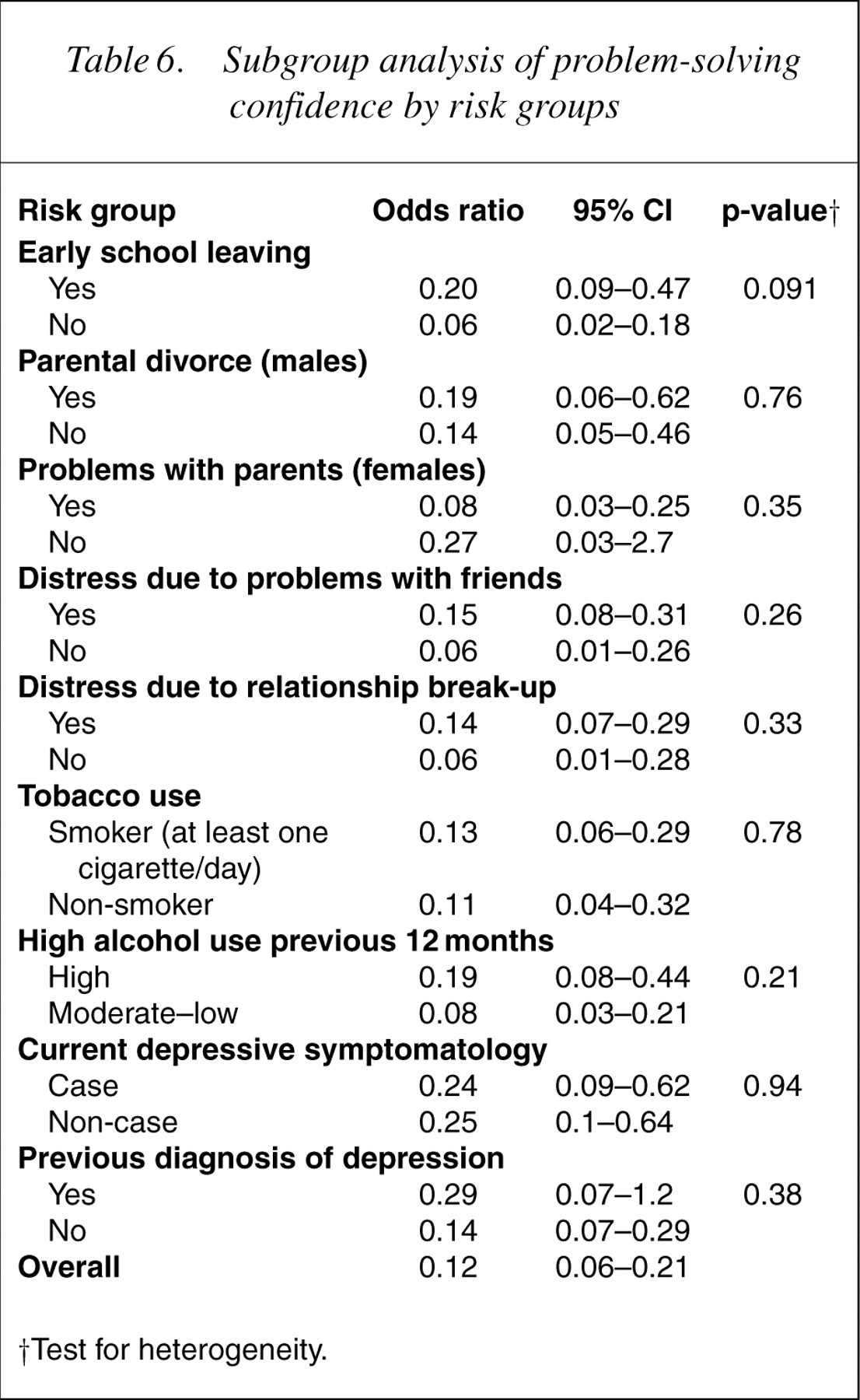
†Test for heterogeneity.
Subgroup analysis of locus of control by risk groups
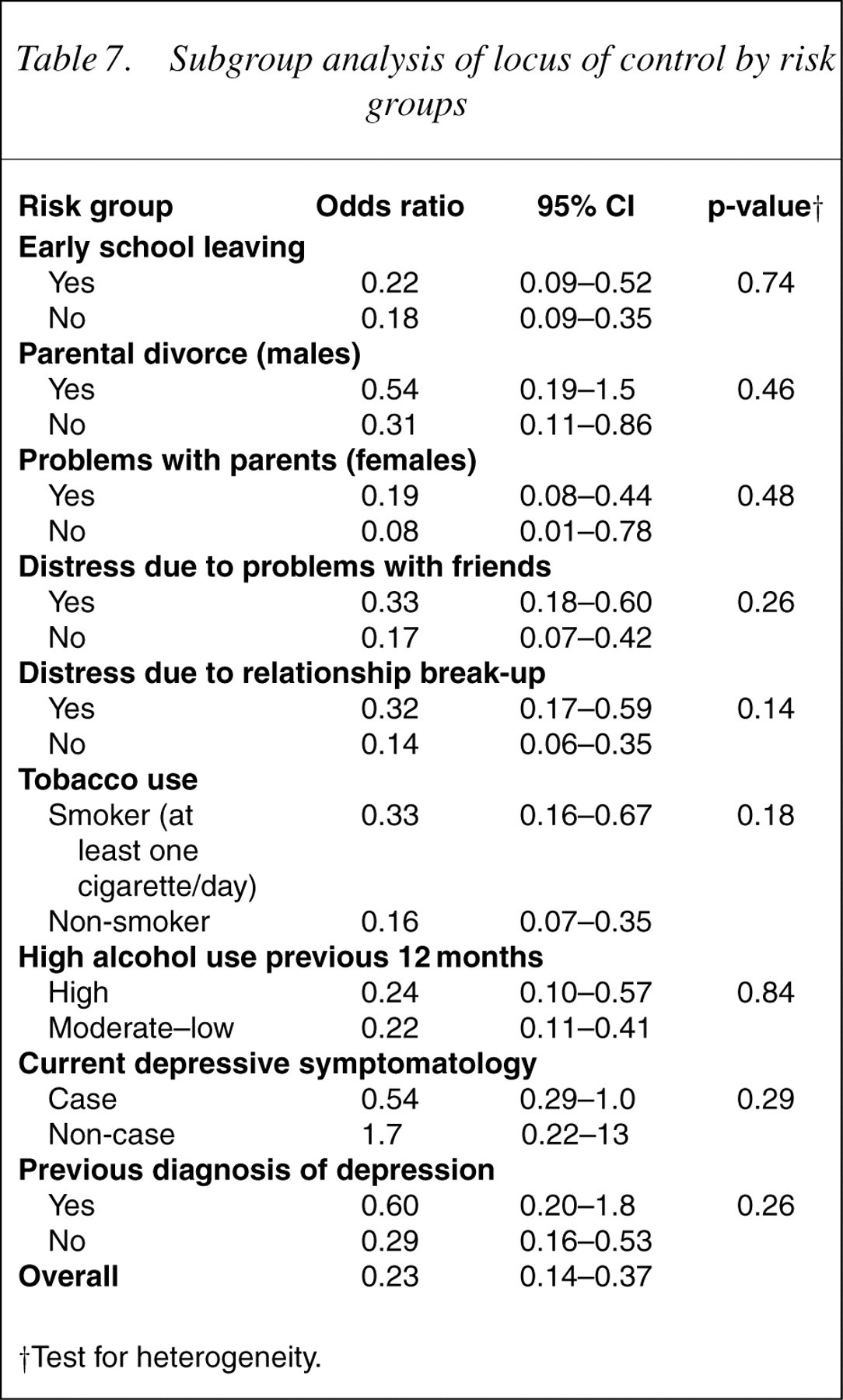
†Test for heterogeneity.
Tests for heterogeneity suggest that social connectedness does not protect differentially for each of the nine high- and low-risk groups (Table 5). There were, however, trends that almost reached statistical significance for social connectedness to protect more for those in the high-smoking group than those in the low-smoking group (p=0.058) and for those in the high-depression group than those in the lowdepression group (p=0.053). There was no evidence of heterogeneity for the other two protective factors within the nine risk factors, indicating that problem-solving confidence and locus of control were protective for both high- and low-risk groups (Tables 6, 7).
Discussion
Risk factors
Within a social–ecological model of suicidal behaviour, which measures a plethora of risk factors, it is worth noting that non-significant risk factors may still play a role, albeit a lesser role than those remaining in the final model. However, as stated by Ayyash-Abdo ‘… it is crucial to understand that any suicidal outcome is a complex, multidomain, interactive effect of many factors over fairly long periods of time. Therefore none of the commonly cited risk factors are definite signs of suicide’ [21], p.471]. The value of the approach used in the current study lies in the identification of robust risk factors, which ultimately provides part of the evidence necessary to channel resources and guide suicide prevention activities. Without such an approach we would be overwhelmed by the multiplicity of risk factors.
Overall, the findings in relation to risk factors in the current study support the conclusions drawn by Fergusson et al. [6] in their analysis of risk factors for suicidal behaviour among young people participating in a study cohort in New Zealand. Specifically, their proposed model of suicidal behaviour that incorporates both a stress model associated with life circumstances and adverse experiences, combined with a mental health model associated with diagnosable mental illness, in particular depression, is supported by the study findings reported here.
The risk of suicide has been found to increase among young people who leave school early, who do not attend higher education and who are from families of lower socioeconomic status [6, 22]. In the present study, leaving school early was a significant risk factor. However, other indicators of disadvantage such as educational status, parental employment status, and distress due to homelessness, financial hardship or unemployment did not remain in the final model. Leaving school early, rather than socioeconomic disadvantage more broadly, is of particular importance in terms of its contribution to suicidality among young Australians.
In a review of the literature, Beautrais found that ‘a large number of studies have reported that young people from families with histories of parental separation and divorce have increased risks of suicide or suicide attempt’ [9], [p.421]. Similarly, Beautrais' review suggested ‘impaired parent–child relationships, poor family communication styles, and extremes of high and low parental expectations and control’ (p.423) were associated with greater risk of suicide attempt. It may be parental discord rather than single-parent status that is more important in determining psychological distress during adolescence [23]. In our study, parental divorce was a significant risk factor for males, whereas distress as the result of problems with parents was a significant risk factor for the females. Perhaps the absence of a parent through divorce (more commonly an absent father) impacts more negatively on males, whereas for females, rather than divorce per se, the quality of the relationship with parents is more influential. The extremely high odds ratio for females who report distress due to problems with parents requires explanation. Although it represents a real finding, the estimate is unrealistically high due to only four females attempting suicide who did not report distress due to problems with their parents.
It has been known for sometime that young adults' relationships with their family and peers have a significant impact on their wellbeing [24, 25], what has emerged more recently is the important role that romantic relationships play in regard to young adults' mental health. For example, distress as the result of a relationship break-up was an important risk factor for suicide attempts among this 18- to 24-year-old age group, a finding consistent with other emergent evidence regarding the strong contribution of interpersonal difficulties, particularly the breakup of romantic relationships, to risk of mental health problems [10,26–28]. It is possible that the relative influence of romantic relationships for young adults is only now being emphasized as research explores suicidal behaviour during young adulthood rather than the adolescent age group so often recruited through school-based studies.
Of the many adverse life events measured in the study, two – distress due to problems with friends and distress due to a relationship break-up – remained statistically significant in the final multivariate model. Consequently, we have concluded that young adults' interpersonal relationships are critically important in determining risk for medically serious suicide attempts. And therefore, skills training and education about how to deal with interpersonal conflict and the break-up of romantic relationships should be a primary focus in school-based life skills education.
Substance misuse has been commonly associated with attempted suicide among young people [6, 9,28–30]. A link between tobacco use and suicidal behaviour for both males and females has been previously reported [31–33] although it is not clear if this association is causal or if unmeasured risk factors play a role. In a study of 49 323 men, itwas concluded that the increased risk of completed suicide among smokers in early adulthood ‘was almost entirely explained by increased prevalence of heavy alcohol consumption and low mental well-being among smokers’ [34], p.1000]. The present study, however, has found a strong association between attempted suicide and cigarette smoking among young adults even after controlling for alcohol consumption in the previous year. Both smoking and alcohol misuse were strongly associated with attempted suicide.
The final comment concerning risk factors is reserved for the well-documented association between mental illness and suicidal behaviour which has been shown in epidemiological studies undertaken in several countries in the developedworld [6, 9, 24, 28, 30,35–37]. The present study has shown that both a previous diagnosis of depression and current depressive symptomatology are strongly associated with medically serious suicide attempts among young Australian adults. This emphasizes the importance of recent efforts in Australia aimed at alleviating the burden of depression.
Protective factors
The identification and measurement of protective factors has become a priority in the rhetoric of suicide prevention literature yet to date little empirical work has been undertaken to unravel the important protective factors [2, 9, 38]. Although the issue of protective factors for suicide is still in its infancy and there is scope for improvement, our study has begun the complex process of empirically disentangling the important from the less important protective factors. Social connectedness, problem-solving confidence and an internal locus of control protected young adults from medically serious suicide attempts. Immediate family support was not a significant protective factor. Corroborating our previous research, which also found that immediate family support is not consistently protectivewhen current depressive symptomatology, rather than suicidality, was the outcome of interest [10].
Esposito et al. suggested that problem solving is not a key factor in discriminating suicidal from non-suicidal adolescents. However, the authors reported that a lack of confidence about being able to solve problems is related to suicidal behaviour, suggesting that it is the cognitive component of problem solving rather than ability or style which influences suicidal behaviour [39]. Although the current study did not measure problem-solving ability, we are able to concur that confidence in problem solving has a direct effect as a protective factor for medically serious suicide attempts. Also, young people who engage in suicidal behaviour have been characterized as having an external locus of control [40, 41] involving a low sense of mastery over one's life or attributing consequences to chance, luck or fate [42]. The current study shows that an internal locus of control protects against medically serious suicide attempts. Cognitive attributes such as problem-solving confidence and locus of control contribute to resilience [43]. Our study provides further support for investment in the enhancement of these cognitive factors within universal prevention activities for mental health and wellbeing, including suicide prevention.
There is a well-established link between social integration and physical health [44, 45]. There is also evidence of a link between social integration and mental health, although the nature of this association is less well-established [46]. The current study found a direct relationship between social connectedness and lower risk of suicidal behaviour and also found a trend for social connectedness to protect against suicide attempts more among those with high levels of depressive symptomatology than those with lower levels of depressive symptomatology. This is a critically important finding, which demands further research. To date there has been general agreement that social connectedness has a direct effect on mental health but there has been limited evidence of a buffering-effect in the face of adversity or stress [47]. Our findings lend support, though only a trend, to the idea that social connectedness has a buffering effect for at least some adversities, in this case depression, and subsequent medically serious suicide attempts.
According to Cohen [47], interventions aiming to improve social integration may be best to target ‘naturally occurring social networks’ rather than support groups comprised strangers. Central to Cohen's thesis is that we must: (i) understand the mechanisms through which social connections influence health; and (ii) acknowledge that negative social interactions can do harm. For example, Kawachi and Berkman [46] point out that ‘close-knit’ social ties can, under some circumstances, be harmful to mental health, perhaps by creating a sense of dependence or pressure to conform. Further research is required with the sensitivity to investigate the mechanisms through which social connectedness protects young adults from making suicide attempts.
Implications for future suicide prevention practice, theory and research
Several considerations are usefully considered in relation to operationalizing findings from risk and protective factor studies and a synthesis of these will determine at what level it is realistic and meaningful to prevent and intervene. A useful conceptualization of protective factors is their relative importance in the face of un-modifiable risk factors. For example, the breakdown of romantic relationships between young adults will inevitably be difficult to prevent, therefore modifiable protective factors provide a more efficient focus for prevention. Conversely, it may be argued that the value of targeting protective factors for risk behaviours such as smoking and heavy alcohol consumption may be less useful and our efforts would be more appropriately and efficiently used in the prevention of these risk factors per se.
Another question is whether to design and implement universal prevention strategies to enhance protective factors for all young adults or alternatively to design interventions to enhance protective factors only among those young adults at high risk? Absolute risk reductions will be greater in the high-risk groups because the prevalence of suicide attempts is higher in these groups. Hence, it is more cost-effective to target those high-risk groups with interventions that aim to improve levels of protective factors. However, the notion of protective factors implies the introduction of a skill, attribute or circumstance which will divert the occurrence of the adverse outcome and as such implies the prevention, or ‘inoculation’, before the experience of adversity. Therefore, it is likely best to continue to intervene to promote protective factors across the spectrum of intervention from universal prevention programs, through early intervention initiatives right the way through to treatment approaches.
Future research must aim to improve our conceptualization and measurement of protective factors. If we are to make headway toward uncovering viable protective factors in relation to suicidal behaviour then studies with larger sample sizes, which ensure the statistical power required to examine the ‘buffering effects’ of protective factors in multivariate statistical models, are well overdue, as are longitudinal studies. Furthermore, advances have been made in recent years in defining and measuring resilience and protective factors and these should be incorporated into future studies. In particular, additional protective factors may include coping styles [48], cognitive hardiness [49] and a range of community factors such as a sense of community belongingness and civic or community participation [46, 50].
Due attention should be given to potential risk factors with small cell sizes that could not be reliably investigated in the current study, including distress as the result of a family members suicide, distress due to abortion, and several mental illnesses. For example, of those young adults who attempted suicide 14.9% (n=14) reported a diagnosis of schizophrenia compared with 0.5% (n=2) among the non-suicide attempters. Studies with larger sample sizes are essential if less prevalent risk factors such as these are to be adequately investigated in multivariate statistical models.
Other limitations of the current study need to be acknowledged. First, almost all participants were Australiaborn and therefore the findings cannot be generalized to other culturally diverse groups. Furthermore, we know from previous analysis of the population-based survey that some populations were underrepresented, for example, young indigenous Australians, young adults from non-English-speaking backgrounds, those from households without private telephones, homeless young people and those living in university colleges [7, 10]. Second, the study has limitations common to cross-sectional selfreport data, particularly those related to cause-and-effect issues. Third, the participants in the population-based survey were drawn from a larger catchment area than that which routinely presents patients to the Metropolitan hospital and therefore although the samples were matched for place of residence, selection bias in relation to young people from urban areas is likely. Fourth, additional risk factors such as genetic, neuroendocrine and biologic processes, and broader cultural and social issues (e.g. media influences and access to methods of suicide) were not explored. Fifth, the regression models did not account for cumulative risk.
Conclusion
Despite these limitations, the current study provides further evidence of the risk factors for medically serious suicide attempts among young Australian adults. Additionally, the research has taken the first critical steps in demonstrating the role that protective factors play both directly and in regards to mitigating the risk factors for suicidal behaviour. Although there remains much to be researched, particularly through the conduct of longitudinal studies with larger sample sizes, the findings presented here nonetheless assist in the further fine-tuning and development of priorities for suicide prevention.