
Abstract
Keywords
Around 1992, we came to the conclusion that Australia should have its own estimates of the distribution of mental disorders within the population. It was inappropriate to continue relying on imported estimates from other countries. What information there already was about mental disorders in Australia was of two types, both with fatal defects. In the first, the information was based only on those who had reached health services: a subset of all who have the disorders in question. In the second, there had indeed been prevalence studies, but only for particular communities such as Heyfield [1], Prahran [2], Botany Bay [3] or Canberra [4]. None of these could represent the Australian population. A National Survey was the only way to correct the deficiency if national policy was to be guided by sound data. A National Survey has now been completed, providing information on Australia's mental health at the close of this millennium.
The beginning
We took the first step towards an Australian Survey by approaching the then Commonwealth Department of Health and Family Services in 1993. It had by that time a Mental Health Branch with a Director, Harvey Whiteford, who was initially sceptical. We let the issue simmer. In 1994 he spontaneously came back to us to agree that the National Mental Health Strategy would be more likely to prosper if there were credible national data. By December of that year, he had convened a national meeting in Canberra of all those who might be involved in a national survey. These included mental health service consumers and carers as well as research clinicians, representatives of particular community groups, the Australian Institute of Health and Welfare and the Australian Bureau of Statistics. In that one day, remarkable clarity of aims was achieved. The decision was that a survey would be carried out and it would have three aims: (i) to estimate the 1-month and 1-year prevalence of mental disorders and of significant psychological symptoms in the Australian population; (ii) to estimate the amount of disablement associated with such morbidity; and (iii) to estimate the use of health and other services by persons with such conditions. To achieve these aims, the survey had to have three complementary parts: (i) a survey of adults in the general population; (ii) a survey of children and young persons; and (iii) a survey of people with the low-prevalence disorders, the psychoses.
At the Editor's invitation, we give an overview of the Survey of Adults and its implications. More detailed accounts can be found in McLennan, [5]; Andrews et al. [6] and Hall et al. [7]. Because these publications provide a more detailed description of the methods, the account given here is more brief. A major report on people with psychoses is now available [8]. For children and young persons, a report is in preparation.
Measuring a nation's mental health
For the adult survey, we needed to examine several thousand people of all ages from 18 years to the very elderly. It was here that we first encountered problems that are partly methodological, partly political and administrative. For example, everyone recognises that the expanding numbers and high morbidity of elderly people is an important issue for health services. Should we therefore over-sample this age group, especially very elderly people, to ensure more stable estimates? If we did so, what would be the consequences? At least two quickly emerged: there would be less money for the rest of the survey in all its three parts; and there were other demographic groups who also had claims to be well-studied, such as the Aboriginal and Torres Strait Islands (ATSI) peoples, persons from non-English-speaking backgrounds (NESB), and persons in rural communities. To include, for example, the NESB community in the survey, we knew that a substantial number with enough English to have the psychiatric assessment would already be included in the adult survey, but there would be too few of any one ethnic group for satisfactory analyses. To extend the sample to include interviews in various European and South East Asian languages would have been impossibly expensive. That needed a special study. Likewise, it would have been valuable to know the prevalence of mental disorders in Australian prisons or nursing homes, but these, too, would require special studies. We therefore decided to use an unweighted sample with no group represented in a proportion greater than its frequency in the population.
As a consequence, the Adult Survey is open to the criticism of not producing information on some of the most significant elements in our society. We particularly regret not having anything about ATSI people's mental health. But at a special meeting held in the planning stages to see what could be done, it became clear that the ATSI population was itself so diverse and our case ascertainment methods so inappropriate that a survey was not practicable. So we have had to postpone having nationally representative epidemiological knowledge about the common mental disorders in indigenous Australians.
The Adult Survey was undertaken on contract by the Australian Bureau of Statistics (ABS) for the Commonwealth Department of Health and Family Services. We had a Technical Advisory Committee, which included each of us, to oversee the survey design and its implementation.
The interview
Psychiatric disorders
In a general population survey of mental disorders and problems, one is seeking access to people who have not sought to be examined in the way that patients usually have. For a survey, few researchers have ever been able to employ psychiatrists or clinical psychologists. Fewer still have been able to employ experienced clinicians who are calibrated to the same method of eliciting symptoms. For the Australian Survey, we knew that we would have to use professional survey interviewers, and that they would have no experience of psychiatry. After careful consideration, we decided on the Composite International Diagnostic Interview in its automated presentation (CIDI-A) [9]. The CIDI-A is a psychiatric interview for research, developed in Sydney by one of us (GA) and his colleagues, now in wide international use. A massive investment of effort went into its development. The CIDI-A systematically explores the diagnostic criteria required for the most common mental disorders defined by the two major psychiatric classification systems, the 10th Edition of the International Classification of Diseases (ICD-10) [10] and the Diagnostic and Statistical Manual, Fourth Edition, of the American Psychiatric Association (1994) (DSM-IV) [11]. Although data were collected to allow both ICD-10 and DSM-IV diagnoses to be made for the common disorders, this report is concerned only with ICD-10 mental disorders. When ‘diagnoses’ are made by the CIDI-A, they can be looked upon only as an approximation of what an experienced research clinician would produce in such a setting. They are certainly not clinicians' diagnoses. Peters and Andrews [9] have shown that the CIDI-A has satisfactory procedural validity for the anxiety disorders. The research community must await more information on its validity across a range of other diagnostic groups; these groups, of course, as set out in ICD-10 and DSM-IV, are themselves only an arbitrary nosology.
It has not yet been possible to calculate confidence intervals for the prevalence estimates because this requires access to the definitive data set from the ABS, which has not yet been released. Meanwhile, methods for calculating approximate standard errors are given on pages 54–56 of the ABS Report by McLennan [5].
Cognitive impairment
People over the age of 65 were given the Mini-Mental State Examination (MMSE) [12] to assess cognitive impairment. Until the present survey, there was limited information on the prevalence of dementia and severe cognitive impairment among adults in Australia [13]. While the MMSE cannot substitute for a clinical diagnosis, it does measure the probability that a person is substantially compromised in memory, thinking and information processing. By convention, persons with a score of 17 or less out of 30 are designated as having ‘severe cognitive impairment’ and may have a dementia. Those with a score of 18–23 have ‘mild cognitive impairment’ and persons with scores above 23 are considered normal.
Other conditions
Five screening questions were also used to identify persons who possibly had a psychosis. Additional questions assessed symptoms of ICD-10 neurasthenia and eight personality disorders.
Common psychological symptoms
One of us (SH) insisted from the start that expressing Australia's mental health only by an enumeration of people with ICD-10 or DSM-IV diagnoses would be seriously inadequate. Such a binary world populated only by cases and non-cases is perhaps appropriate in some contexts, but it is not appropriate in the general population or in general practice. The survey therefore included an efficient screening instrument, the 12-item General Health Questionnaire developed by David Goldberg [14]. The findings on the GHQ-12 and its correlates for the Australian national sample will be reported in a forthcoming publication.
Disablement
As well as assessing specific mental disorders, the interview gathered information about the degree of disablement in the previous 4 weeks associated with specific mental and physical disorders. Not being able to carry out one's usual activities and responsibilities at home and at work is called here ‘days out of role’. It indicates disturbance to the individual's role performance at work and as a member of a family or social group, irrespective of age. Lastly, the interview covered the use of health services for mental disorders, in this case during the previous 12 months.
Results
Public response
About 13 600 private dwellings were selected by the ABS, and one person aged 18 years or over was randomly selected in each and an interview sought. The ABS interviewers are very highly skilled and experienced professionals. Their supervisors from each state or territory were trained by one of us (GA) and his team in the administration of the CIDI-A. Across the country, the interviewers successfully completed the whole interview on 78%% of the candidate persons. Analyses have not yet been completed on the extent to which this achieved sample is representative of the Australian population on sociodemographic variables. The response rate is very similar to household surveys elsewhere that involve a similarly long interview on a personally sensitive topic. It was 76%% in the Epidemiologic Catchment Area (EGA) Study in the USA [15] and 80%% in the subsequent National Comorbidity Survey [16] where special efforts were made to induce reluctant respondents to participate. From the field interviewers, we learned that the great majority of respondents told them that they enjoyed the interview: it gave them a rare opportunity to talk about their health and their day-to-day lives. Often, the interviewer's difficulty was not in obtaining the person's cooperation, but in finding a way to disengage without being discourteous.
Total case rates
The National Survey found that just under one in five Australian adults (17.7%%) had had an anxiety, affective or substance-use disorder in the past year. Figure 1 shows the pattern.
Twelve-month prevalence of ICD-10 mental disorders in Australia: □, anxiety; ▪, depression; ▪, substance use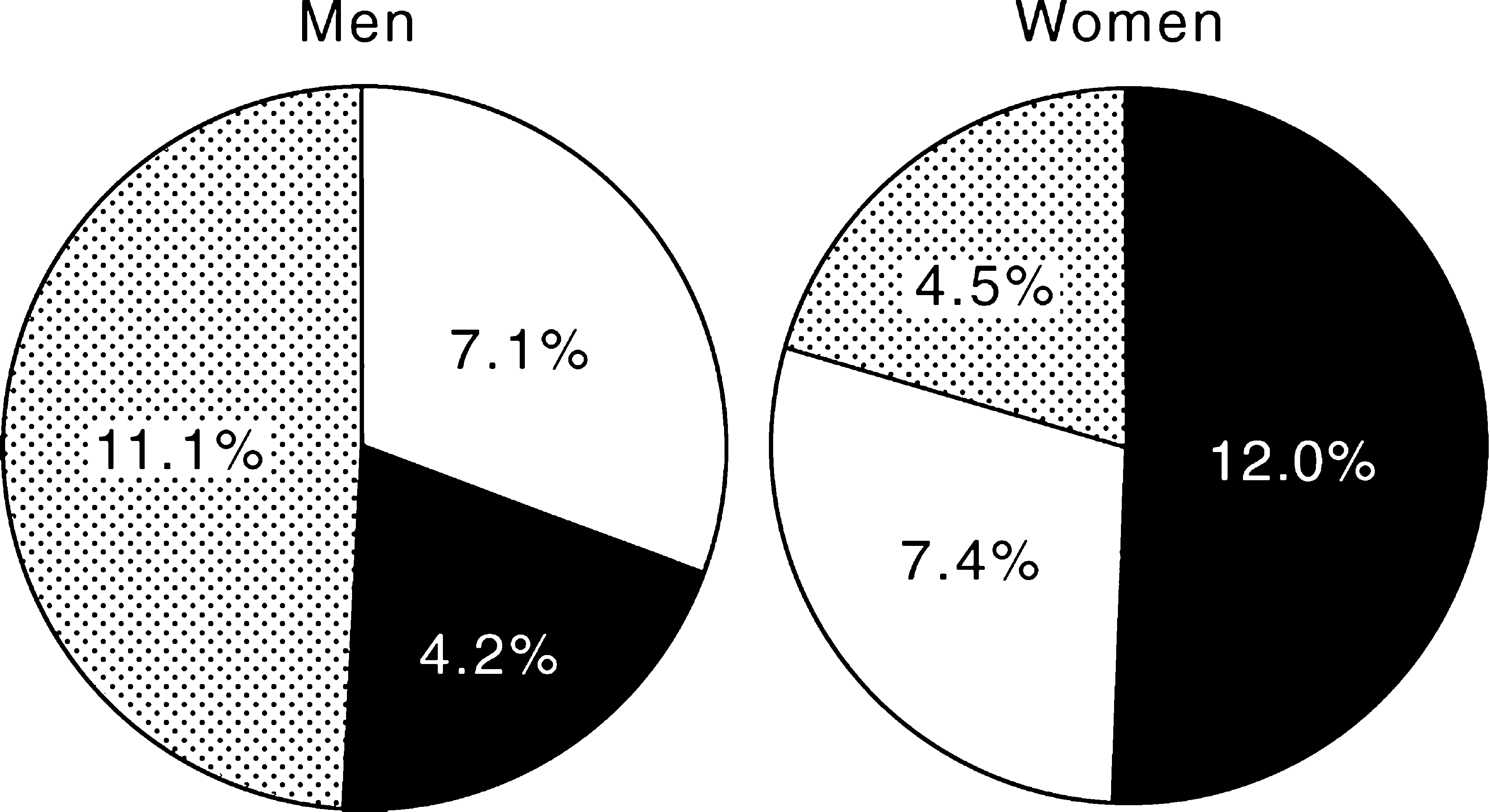
Anxiety disorders were the most common. They affected just under one in ten adults (9.7%%), followed by substance-use disorders which affected 7.7%% and affective disorders which affected 5.8%% of adults. Men were much more likely to have a substance-use disorder than women (11.1%% v 4.5%%) and women are much more likely than men to have an anxiety (12.1%% v 7.1%%) or an affective disorder (7.4%% v 4.2%%). These prevalence rates mean that overall approximately 2.38 million Australian adults had a mental disorder within the previous 12 months (1.15 million men and 1.23 million women. These rates probably underestimate the prevalence of all mental disorders among Australian adults. First, they do not include mental disorders such as schizophrenia, dementia and the personality and somatoform disorders. Second, there is reason to expect that in the 22%% of the target sample who repeatedly could not be found or who refused an interview, the rate of mental disorders is likely to have been higher.
The disablement caused by the common mental disorders is very considerable, as shown in Figure 2. There was an average of 3 days of disablement in the previous 4 weeks, compared with 1 day for the general population.
Average days out of role in the past four weeks by sex and mental disorder: ▪, men; □, women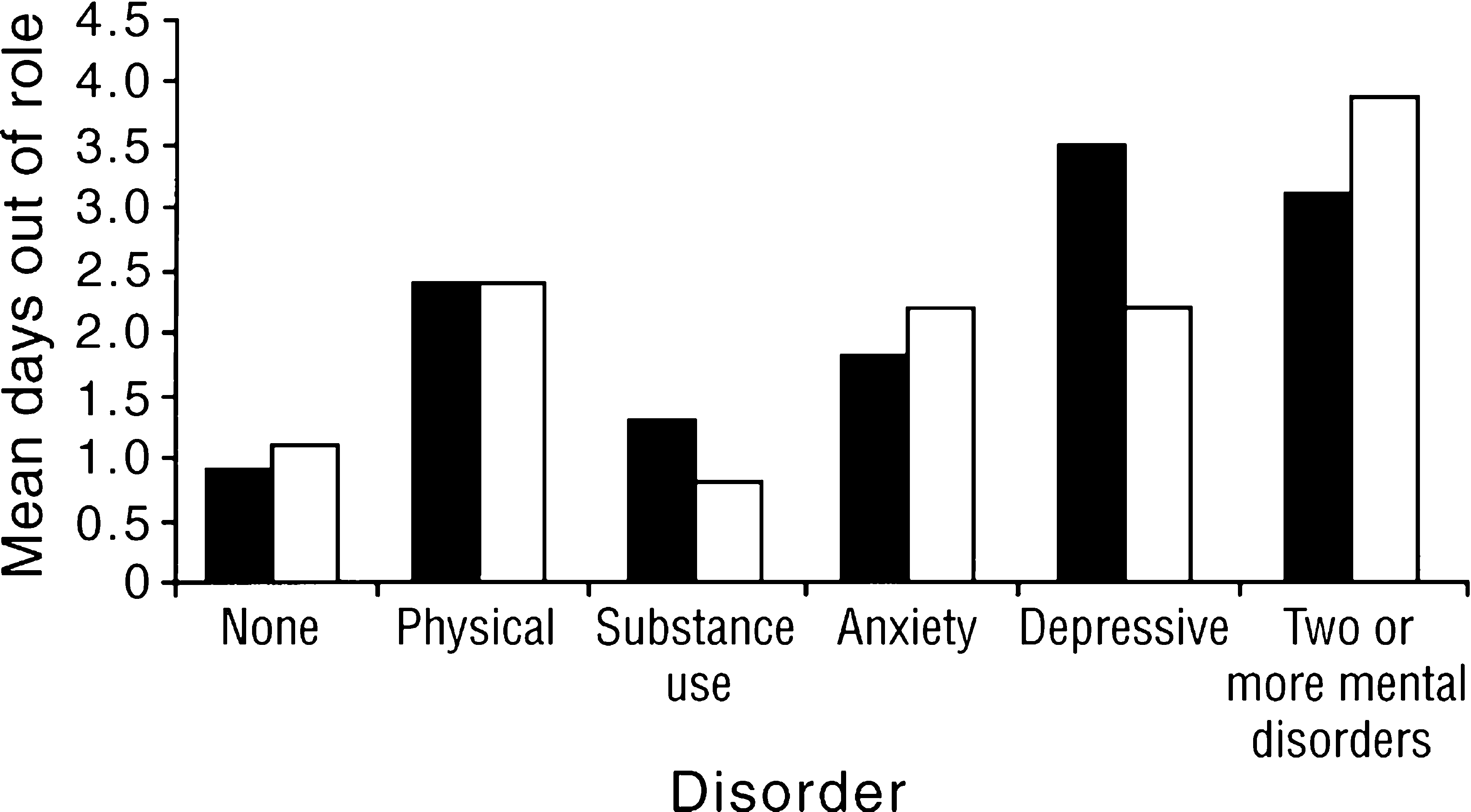
For all persons who had one or more of the common mental disorders, 65%% had not used any form of health service in the previous 12 months.
Anxiety disorders
For the anxiety disorders, 9.7%% of adults reported symptoms that qualified for a diagnosis of one or more of these disorders in the past 12 months. This comprised 1.3 million Australian adults (470000 men and 830 000 women). Posttraumatic stress disorder was the most common of the anxiety disorders (3.3%%) and obsessive-compulsive disorder was the least common (0.4%%).
Correlates
The anxiety disorders, especially panic disorder, agoraphobia and posttraumatic stress disorder, are more common in women (Fig. 3). The disorders are most prevalent in people aged 18–54. Their prevalence begins to decline only after the age of 55 years along with that of other mental disorders.
Prevalence (%%) of anxiety disorders by sex and age: ▪, men; □, women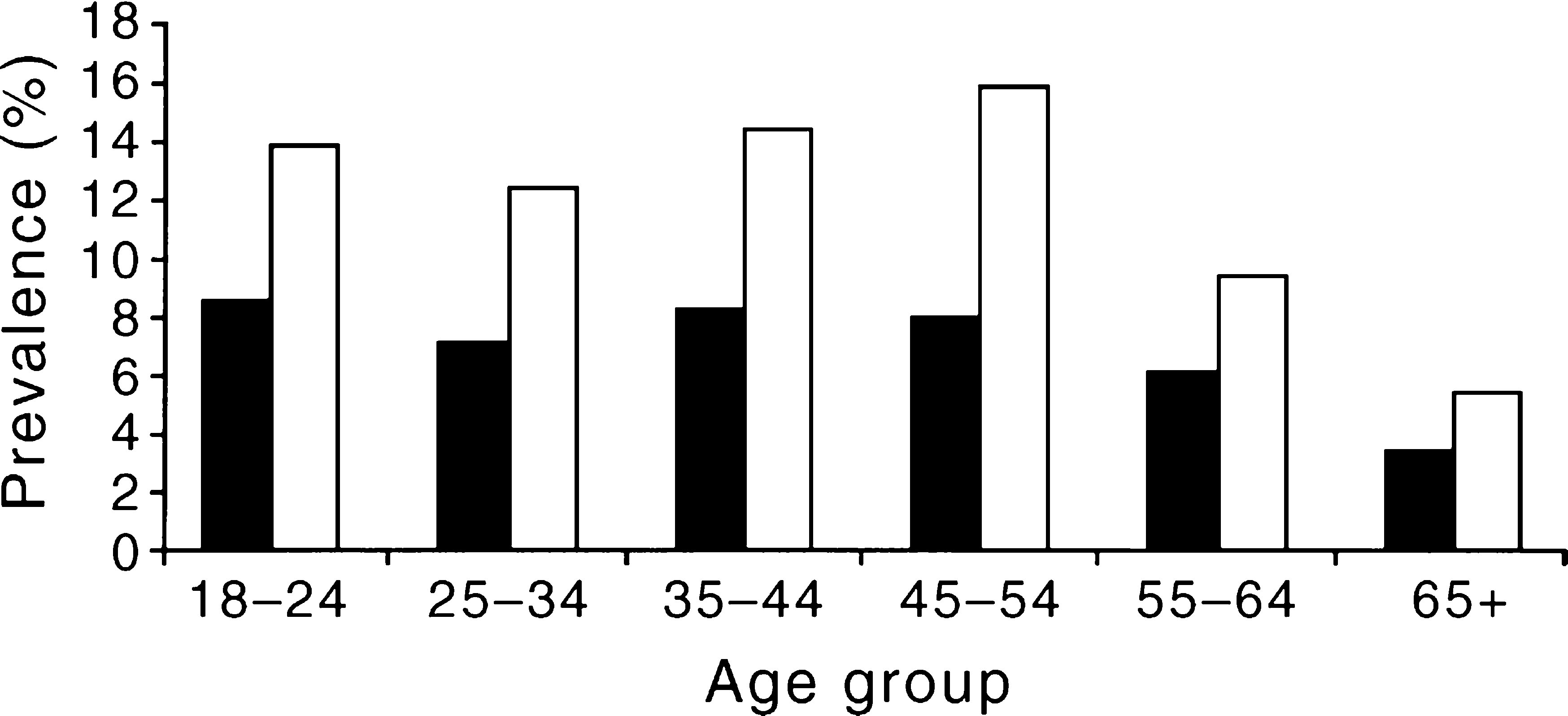
Comorbidity
Approximately 40%% of women with an anxiety disorder met criteria for at least one other mental disorder. In men with an anxiety disorder, half (49%%) had at least one other type of mental disorder, such as depression or alcohol abuse.
Disablement
The disablement data suggest that anxiety disorders can have a considerable impact on the lives of those who suffer from them. People with anxiety disorders alone reported an average of 2.1 days out of role. Thus anxiety disorders account for some 2.7 million person-days out of role per month among adults in Australia. The corresponding figures for affective disorders and substance-use disorders are 2.1 million and 1.1 million person-days per month respectively.
Use of Health Services
Only 38%% of people with any mental disorder were seen by the health services during the survey year. But it was much worse for anxiety disorders, where only 28%% of people sought treatment (Figure 4), half the rate at which people with an affective disorder as their sole complaint did so. Treatment was much more often from a general practitioner rather than from a psychiatrist or clinical psychologist.
Type of professional help used for anxiety disorders: ▪, men; □, women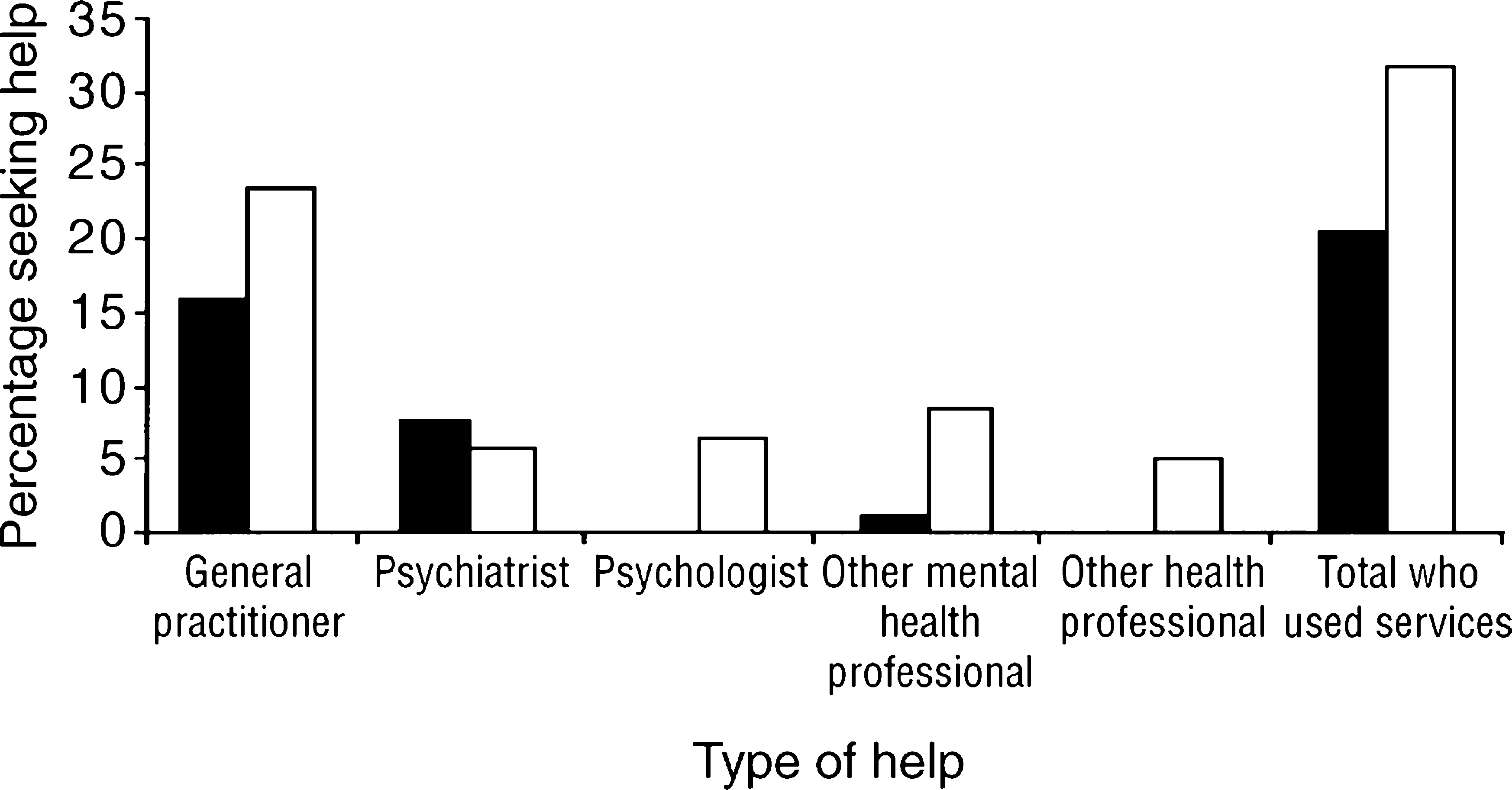
Some unexpected findings
The survey revealed some unexpected findings about anxiety disorders.
Older people are less likely to have anxiety disorders than younger and middle aged persons.
Anxiety disorders are less likely to occur among persons who were currently married.
Anxiety disorders are unrelated to education.
Anxiety disorders cause much more disablement in people's lives than was realised.
Three-quarters of all cases have not sought help from health services.
Depressive disorders
What follows refers to depressive episodes and dysthymia as defined in ICD-10, hereafter referred to collectively as the depressive disorders. In the 12 months prior to the interview, 5.8%% of the adult population had one or more depressive disorders. They were more frequent in women (7.4%%) than in men (4.2%%). This means that in Australia, about 778 000 adults had experienced these conditions in the previous year (275 000 men and 503 000 women).
Correlates
As well as sex, age has some association with the risk of being depressed (Figure 5). For men, depression is a little more common in mid-life than in other life stages. But in women, the highest rates are in those aged 18–24 years where one in 10 had had it in the previous year. Thereafter, it gradually decreases with age. The association between depressive disorders and other important socio-demographic variables has been reported in Andrews et al. [6].
Prevalence (%%) of depressive disorders by sex and age: ▪, men; □, women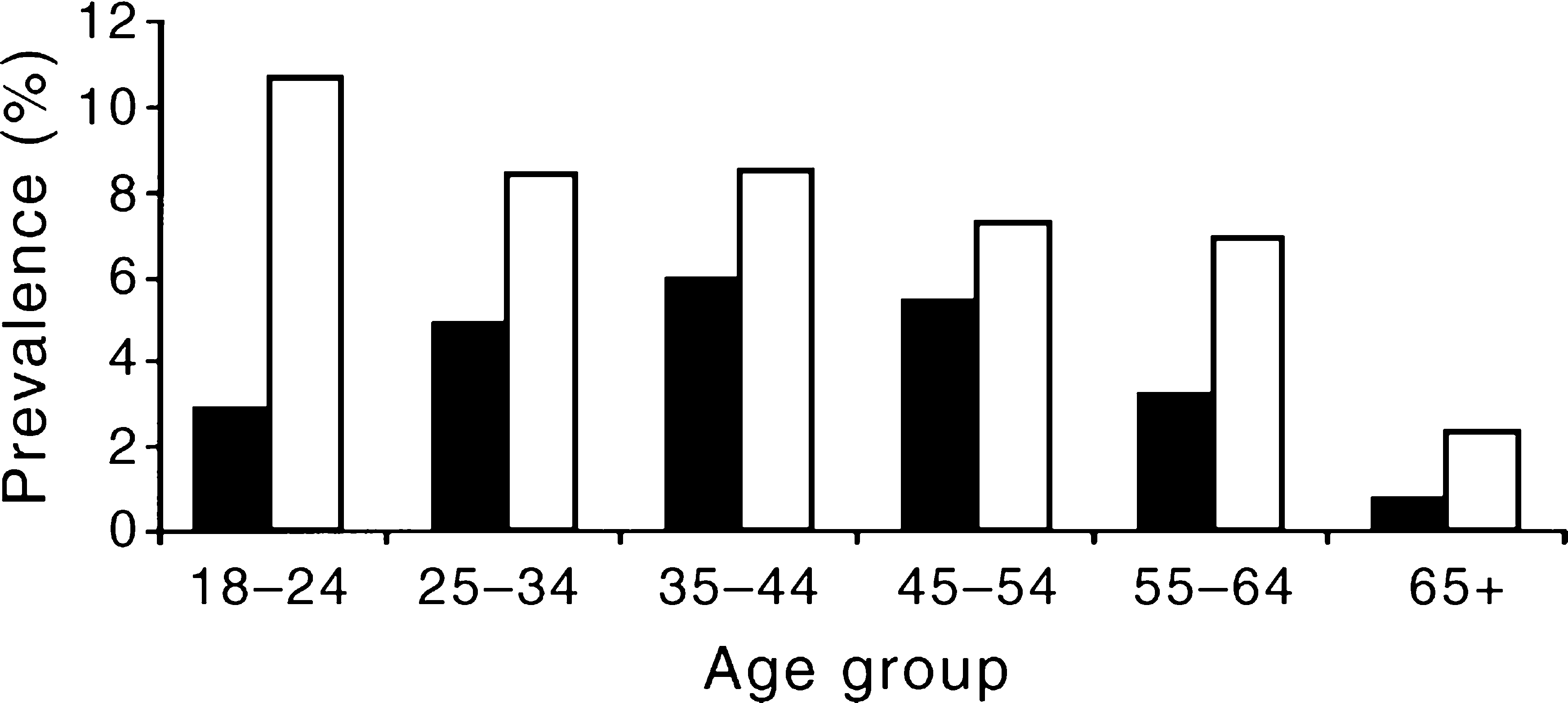
Comorbidity
Of women with a depressive disorder, over half (57%%) had at least one other mental disorder. Approximately two-thirds (66%%) of men with a depressive disorder had at least one other mental disorder.
Disablement
Persons with depression had, on average, 2.7 days out of role in the previous 4 weeks. If they had both a depressive disorder and a physical condition, it rose to 6.3 days. One interpretation is that in terms of people's ability to function in day-to-day life, the depressive disorders cause considerable disruption to sufferers and to those around them.
Use of health services
The pattern of service use is shown in Figure 6. For people with neither a physical nor an ICD-10 mental disorder, only 3%% had consulted a general practitioner for mental health problems in the year prior to the interview. In marked contrast, 40%% of persons with a depressive disorder had consulted their GP in the same period. It is not known from this survey whether the GP had recognised that the person was clinically depressed, as the survey interview had done. But it is clear in Australia, as elsewhere, that GPs are in an excellent position to diagnose a large proportion of all persons who are depressed, and to treat them, where appropriate. Psychiatrists saw only 8.4%% and psychologists 6.2%% of those depressed, very much less than the GPs. Other health professionals saw 29.0%% of them.
Type of professional help used for depressive disorders: ▪, men; □, women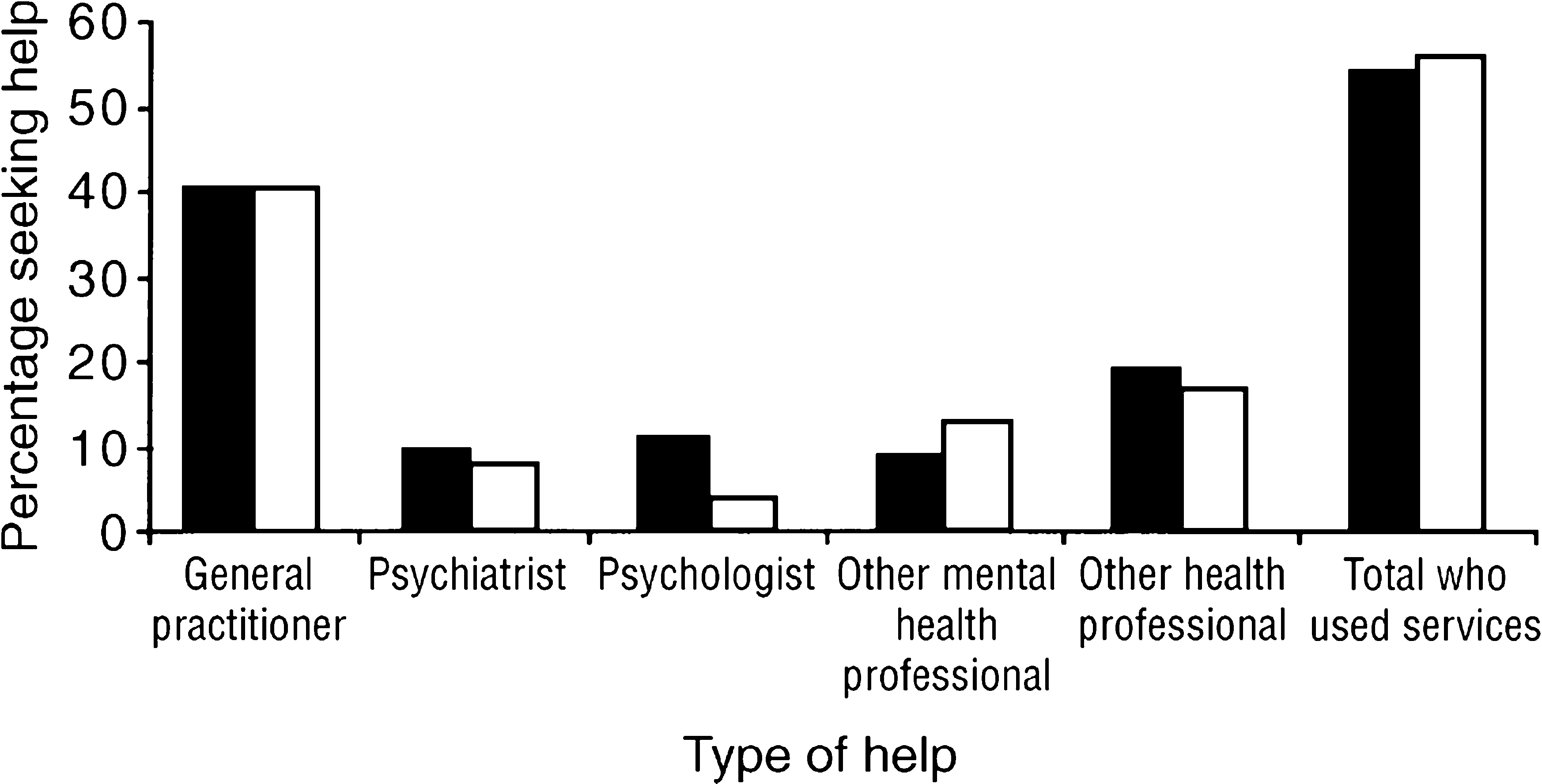
Some unexpected findings
There are some factors commonly considered to increase the risk of becoming depressed but for which there was no evidence in Australia in the present study. Four examples follow.
The elderly: contrary to the belief of many in the general public and among health professionals, there is some evidence that in the general population, the prevalence of depressive disorders is in fact lower in persons aged 65 and over than in younger adults [17]. This has been reported in research in Australia and other industrialised countries. The National Survey has confirmed this trend. The finding applies to the elderly in the community, not those in nursing homes or other special accommodation, where the prevalence of depression is known to be high.
Country of birth: migrants and other persons born outside Australia have slightly less depression than persons born in Australia do. This is consistent with the finding that persons born overseas have much lower rates for alcohol and substance-use.
Capital city versus the rest of each state: the survey has shown that depression is no higher in either the capital cities or the rest of each State and Territory. It should be borne in mind that the numbers of persons living in truly rural settings was necessarily small in the survey.
Help-seeking: only 40%% of depressed people had sought help from health services in the previous 12 months.
Substance-use disorders
One in thirteen Australian adults aged 18 years and older (7.7%%) had a substance-use disorder in the past 12 months. There were 1.04 million Australian adults with a substance-use disorder (734 000 men and 307 000 women). Alcohol-use disorders were about three times as common as drug-use disorders. In comparison, 2.2%% of Australian adults had had a drug-use disorder in the past year. Cannabis accounted for more drug-use disorders than any other illicit drug: 1.7%% of Australian adults had a cannabis-use disorder in the past 12 months.
Correlates
The prevalence of substance-use disorders declined steeply with age for both men and women (Figure 7). One in six Australians aged 18–24 had a substance-use disorder but only one in 90 Australians aged 65 years and over. Other important sociodemographic correlates can be found in Hall et al. [7] and Andrews et al. [6].
Prevalence (%%) of substance-use disorders by sex and age: ▪, men; □, women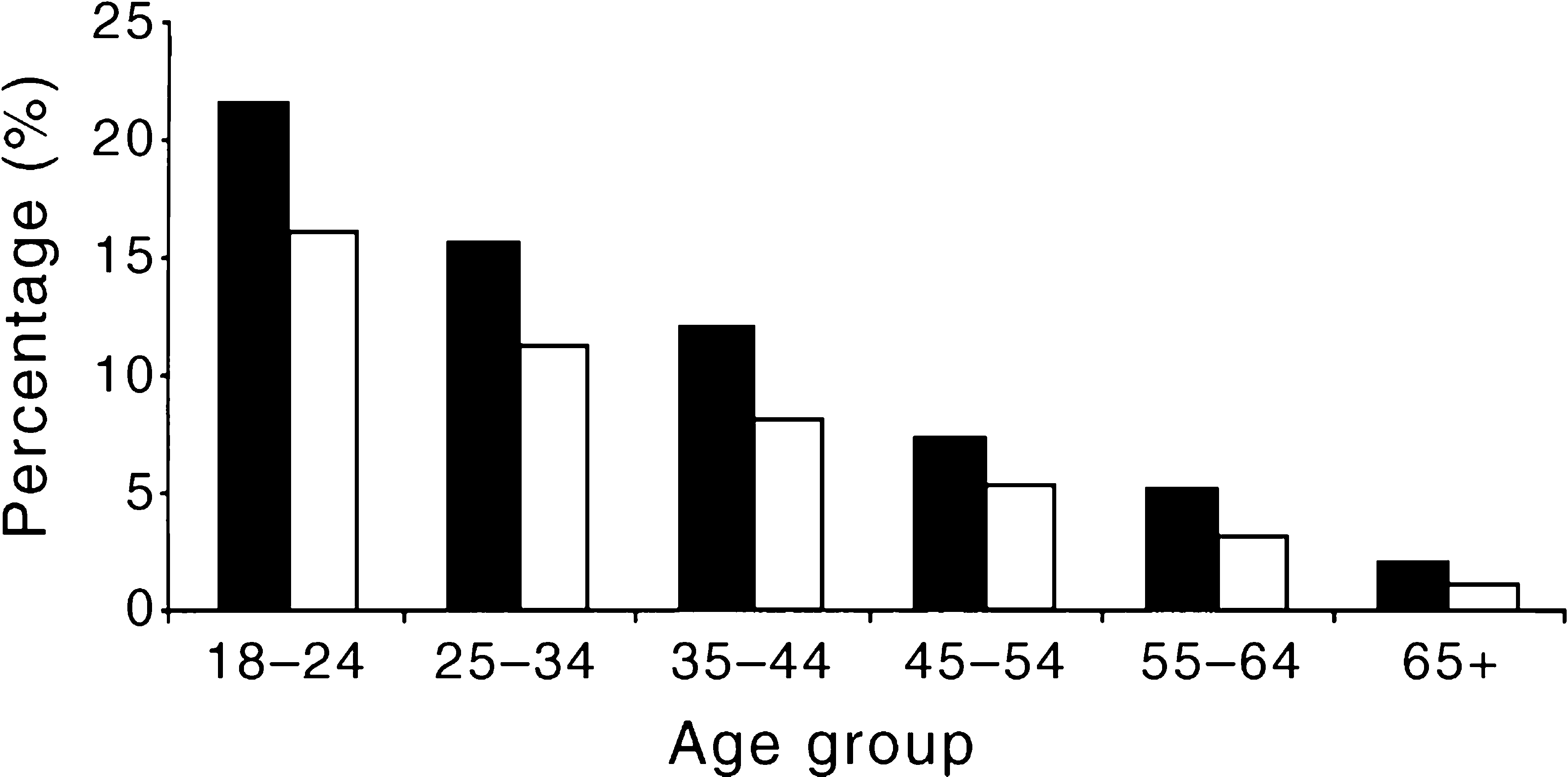
Disablement
Men with substance-use disorders and a combination of substance-use disorders and physical disorders had more days out of role in the last 4 weeks than men with no mental and physical disorders. Women with substance-use disorders had fewer days out of role than those women with no mental or physical disorders. Women with both a substance-use disorder and a physical disadvantage had more than twice as many days out of role than women with no mental or physical disorders. These data should be treated with caution, however, because substance-use disorders are more common in younger age groups, so younger women might be expected to have fewer days out of role than older women.
Comorbidity
Just under half of women with a substance-use disorder (46%%) met criteria for an anxiety or affective disorder, and one-fifth (18%%) met criteria for both an anxiety and an affective disorder. A quarter of men with a substance-use disorder (25%%) met criteria for another mental disorder, with 10%% meeting criteria for both an affective and an anxiety disorder.
Use of health services
The use of services is shown in Figure 8. Only about one in seven Australians with a substance-use disorder (14%%) sought assistance from a health professional for their disorder in the previous 12 months. This is half the rate at which people with an anxiety disorder sought treatment. Almost twice as many women (21%%) as men (12%%) sought such assistance. Most of this treatment was from a general practitioner rather than from a psychiatrist, psychologist or other mental health professional.
Type of professional help used for substance-use disorders: ▪, men; □, women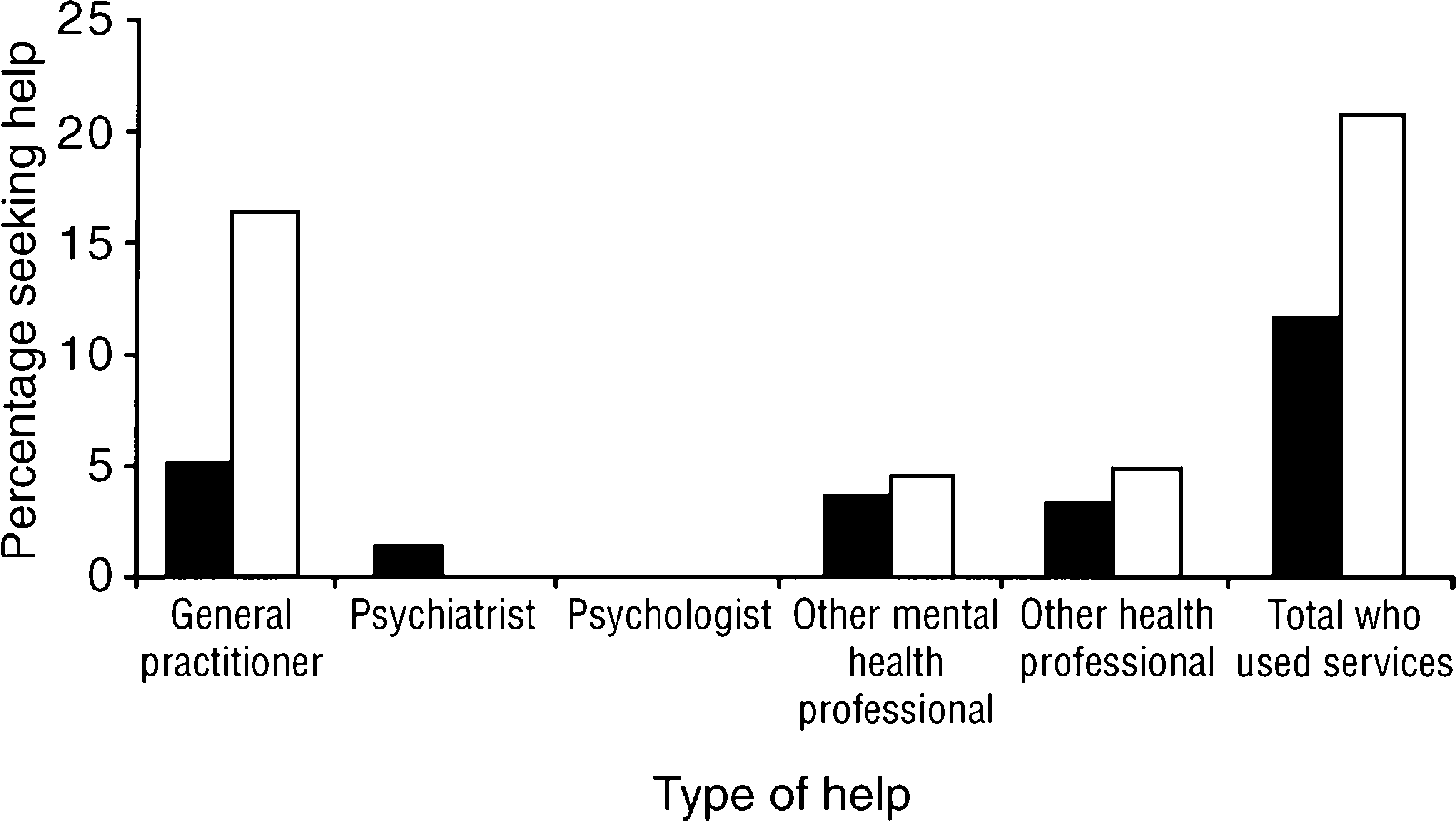
Some unexpected findings
Substance-use disorders are most common in the young, affecting as many as one in four young men, with frequency declining steeply with age.
There are only small differences in the rate of substance-use disorders between people who live in the cities and in other areas.
Persons from non-English-speaking backgrounds are less likely than other Australians to have a substance-use disorder.
Even fewer than expected seek help from services.
Other conditions
‘Neurasthenia’ is a term that has come back into general usage in psychiatry. It is characterised by persistent feelings of fatigue after quite minor mental or physical effort, usually occurring with muscular aches, dizziness, tension headaches, sleep problems, inability to relax and irritability. This condition is known to be common in primary care in many countries [18]. Neurasthenia is somewhat more common in women than men. In both sexes, the prevalence is much lower in persons aged 55 years and over. The amount of disablement it causes in the lives of people is far from trivial: about 28%% with the condition had been unable to function for 2 days or more in the previous month. This is over four-fold higher than in persons without this condition.
Personality disorders
In the National Survey, it was not possible to assess each personality disorder separately. The data presented here describe the prevalence of any of these disorders as one group. In both men and women there is a notable decrease with age in the prevalence of personality disorders (Figure 9). Personality disorders are associated with considerable disablement in day-to-day life: 15%% of cases had experienced at least 2 days of impaired functioning in the previous month. This is more than twice as high as the rest of the population.
Prevalence (%%) of personality disorders by sex and age: ▪, men; □, women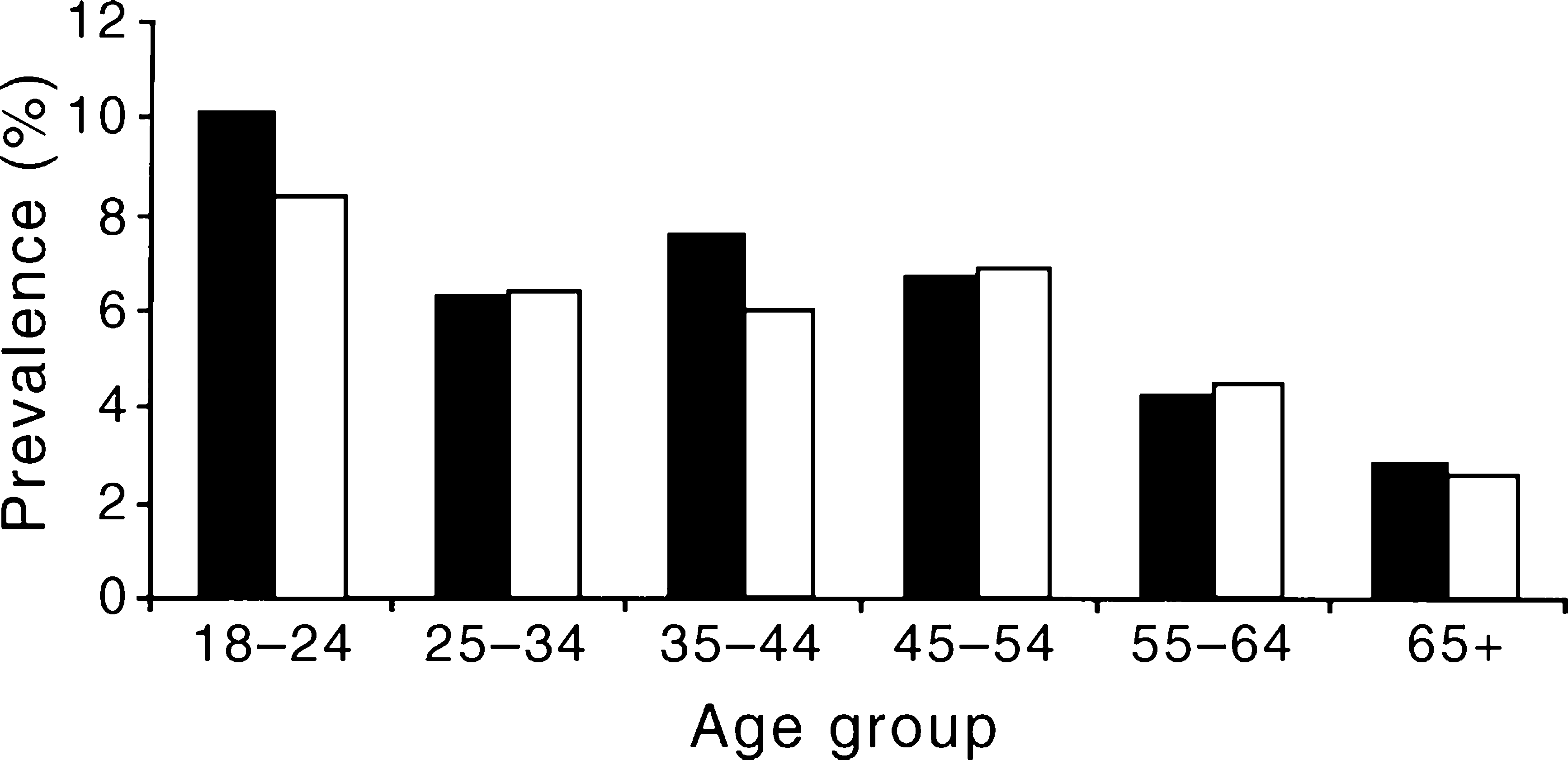
Cognitive impairment
The frequency distribution was highly skewed, with most people having a normal MMSE score and progressively fewer with impairment of increasing severity. At the accepted cut-off point of 23–24 for the detection of cognitive impairment, the prevalence was 8.6%% among those aged 70 and above. The values for Australia are similar to those obtained in comparable samples of the elderly: the ECA [16] and two earlier surveys in Hobart and Canberra [19].
Key findings
This is the first time that a survey of the mental health of a sample of Australian adults has been attempted. The 1-year prevalence for any mental disorder is likely to be more than one in five after psychosis, neurasthenia, personality disorder and cognitive impairment are included, and after one allows for the one-fifth of the sample who could not be contacted or who refused to be interviewed in the Survey. Anxiety disorders were the most prevalent, followed by substance-use and then affective disorders. Approximately half as many Australians have a mental disorder as have a chronic physical disorder, such as kidney disease or chronic bronchitis.
Are these prevalence rates believable? The overall pattern of morbidity is very similar to that reported for the United Kingdom by Jenkins et al. [22],[23]. Our view is that having symptoms, even at case level, is necessary but not sufficient to justify treatment. A careful analysis of the need for treatment, including the reality of un-met need, can be found in Andrews and Henderson [20]. In that volume, Henderson [21] acknowledges that it is irrational to suggest that one in five adults need treatment for a case-level mental disorder. So there are three possible interpretations. First, the case-finding instrument may have too low a threshold, especially when in the hands of non-clinicians. Second, some people's symptoms may be manageable to self and to others: a group we need to know more about. Third, symptoms and disablement may be non-linearly related.
Of those with a mental disorder who had sought help from a health professional for their disorder, in most cases this was from a general practitioner rather than from a specialist mental health professional such as a psychiatrist, psychologist or mental health worker. Women were generally more likely than men to have sought help. It is important to note that 29.4%% of cases had seen a GP at least once in the previous 12 months, compared to only 3.2%% of those with no mental disorder. Not unexpectedly, only 7.0%% of the cases had seen a psychiatrist. What is striking is that 64.6%% of persons with a mental disorder had not sought any professional help for mental health problems. The reasons for this now need to be pursued. It cannot be assumed that all of these people should have sought professional help, but there is a need to know about possible barriers to help seeking.
The National Survey is unique among large-scale population surveys in that it provides information not only about symptoms but also about disablement, health service use and self-perceived need for services. When the results summarised here are coupled with the results from the Survey of People with Psychoses and the Survey of Children and Young Persons, Australia will know more about the mental health and well being of its citizens than most other countries. The National Survey has generated information that has already proved invaluable for advocacy in keeping mental health prominent in the agenda of governments. It has shown how mental disorders are actually distributed in the general population, the disablement they cause and where un-met need [20] is most apparent. For the Second National Mental Health Plan (1998–2003) and beyond, the Commonwealth, states and territories can now make better-informed changes to the way Australia's mental health can be protected and improved.
Footnotes
Acknowledgements
This report is based on Andrews G, Hall W, Teesson M and Henderson S. The mental health of Australians. Canberra: Mental Health Branch, Commonwealth Department of Health and Aged Care, 1999. The authors gratefully acknowledge permission from the Commonwealth Department to use this source. They express their warm appreciation to Harvey Whiteford for his major contribution to making the survey happen.