
Abstract
Classification of any mental disorder is likely to have clinical utility only if it is based on a valid underlying model. The depressive disorders have long provoked debates as to whether a categorical or a dimensional model is all explanatory. This paper will argue that no single (categorical or dimensional) model is likely to be valid, and that a mix of models is required to classify, diagnose and shape management decisions for the mood disorders. After reviewing limitations to the dimensionally based official classificatory systems (DSM-IV and ICD-10), and noting some of the consequences, a set of alternative strategies is outlined. In essence, identifying syndromal ‘fuzzy sets’ from phenotypic and aetiological clustering, a model that occurs in the rest of medicine.
Any diagnostic system is dependent on a valid classificatory model. If the model is atheoretical and/or invalid, both research into the conditions and their management will be compromised. This overview identifies major limitations to the current atheoretical dimensional models underlying the DSM-IV [1] and ICD-10 [2] systems for the mood disorders, before overviewing alternate models that seek to categorize (where categories exist) and then dimensionalize non-categorical conditions, with both approaches weighting phenotypic expression and cause.
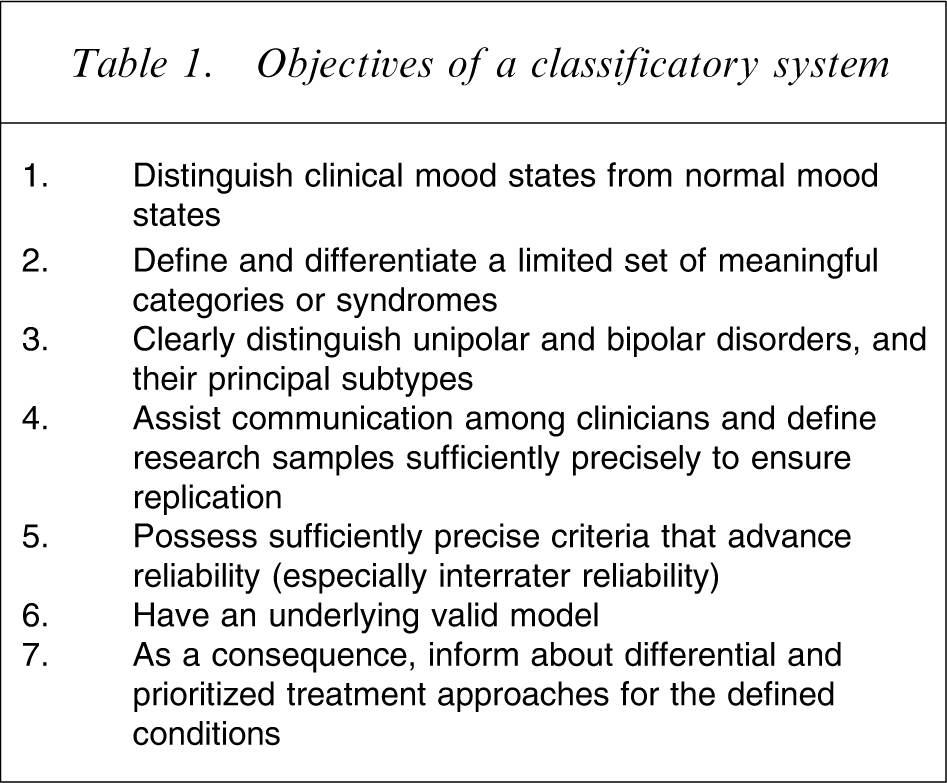
The topic can be approached by identifying expectations of any diagnostic classificatory system. Table 1 lists candidate objectives. We can now consider the extent to which such objectives are met by current classificatory systems.
Objectives of a classificatory system
Clinical and subclinical definition
In classifying depressive disorders, both the DSM-IV and ICD-10 systems essentially use dimensional models: dimensionalizing severity, persistence and recurrence. These dimensional models have expanded in the last decade to include ‘subsyndromal’ and ‘subclinical’ expressions of depression which, by their naming alone, raises questions about how substantive the ‘conditions’ could actually be. In application, the extended dimensional model effectively changes our long-standing concept of ‘clinical’ depression. Prior to introduction of the DSM-III system in 1980, clinical depression had an approximate 5% lifetime risk. Now, as a consequence of dimensional modelling, it is almost a ubiquitous human experience. For example, we have followed a non-clinical group from their early 20s. As noted elsewhere, by their early 40s 42% had met lifetime criteria for major depression and 79% had met symptom and duration criteria for a lifetime major, minor or subsyndromal depressive episode [3]. Although clinical depression was almost certainly under-diagnosed in the past, such data raise the question of whether it now, in effect, risks being over-diagnosed as a consequence of such extended diagnostic groupings.
Those who ‘dimensionalize’ depression commonly argue support for that model by quantifying significant disability in individuals with subsyndromal expressions – in some studies even comparable to that quantified for major depression [4], and, if a simple population-based approach is prioritized, this might appear to be a persuasive argument supporting its validity. In practice, however, many of those who meet criteria for subsyndromal disorders are experiencing a range of psychosocial stresses, whether reflecting socioeconomic status, other social factors, or personality or coping limitations. Thus, even if significant disability is present in those with subsyndromal depression, to assume that it is necessarily a consequence of ‘depression’ (as against a cause or an iterative cause–consequence circle) is to take a very narrow approach. Those who advance this component of the unidirectional model (i.e. subsyndromal depression is a driver of substantive morbidity and disability) often then argue that findings establish the need for assertive treatment of the ‘depression’. In reality, the evidence base supporting such advocacy is quite limited, and even more desultory than evidence in regard to major depression. By itself, it does not validate the extreme consequences of the dimensional approach: that expanding the boundary of ‘depression’ is necessarily associated with successful intervention across the spectrum. Thus, in defining the boundaries of clinical depression we need to establish a case/non-case boundary that is clinically meaningful, and for dimensionalists to test for causal and treatment trend breaks (especially to establish where treatment impact moves from being non-existent or negligible to distinctive). The latter findings would ideally approximate to caseness definition, but this would not be a mandatory requirement.
Thus, the key issue is whether such a dimensional model effectively defines and demarcates clinical depression from non-clinical states of depression. I argue that the dimensional model has been extended too far, and that the consequences (e.g. clinical depression being a near-ubiquitous lifetime experience) strain credulity and undermine the model's credibility.
A similar expansion has occurred for the bipolar disorders: clinicians are increasingly encouraged to view ‘soft signs’ as sufficient to make a diagnosis of bipolar disorder. Ghaemi et al. have offered several examples of such ‘soft signs’: more than three episodes of major depression; major depression coming on at an early age; people who experience ‘poop out’ while taking an antidepressant; and the experience of atypical symptoms (such as hyperphagia and hypersomnia) [5]. Akiskal has suggested the ‘rule of three’ to consider bipolar disorder: three episodes of major depression; three failed antidepressants; three simultaneous jobs; proficiency in three languages; taking three substances of abuse; and the patient's family being eminent in three fields [6]. In addition, Akiskal includes flamboyance in dressing and the so-called hyperthymic or exuberant personality. Thus, the dimensional or ‘spectrum’ model of bipolar disorder allows a diagnosis of bipolar disorder to be proposed on the basis of such soft signs and in the absence of the patient ever reporting a high or bipolar pattern. Again, such a model strains credulity and risks both over-diagnosis and over-treatment.
In relation to the bipolar disorders, ICD-10 contains only one bipolar category (‘bipolar affective disorders’). DSM-IV uses exactly the same criteria and the same criterion cut-off in defining mania and hypomania. Distinction is minimal. The only differentiation between the classification of those two conditions is that DSM-IV imposes a minimum duration of 7 days for mania and 4 days for hypomania, but neither of these duration criteria were empirically developed, and subsequent studies have failed to find support for them [7]. DSM-IV-defined mania does not link directly with bipolar I disorder, nor does DSM-IV-defined hypomania link directly to bipolar II disorder. DSM-IV differentiates bipolar I from bipolar II on the basis of (i) mania with or without psychosis; or (ii) mixed episodes; or (iii) the patient being hospitalized. Thus, while the presence of ‘psychosis’ weights the diagnosis of mania, it is not mandatory, and thus what would seem clinically to be essentially a categorical feature is not given categorical status in the diagnostic system. The DSM-IV inclusion of ‘hospitalization’ is also problematic, in that it is uncommon in medicine (and in the DSM system) to include the consequence of an illness as an illness criterion. In essence, neither ICD-10 nor DSM-IV differentiates distinctly between bipolar I or bipolar II disorders, while neither system possesses decision rules building to categorical distinction.
A limited set of meaningful diagnostic categories?
The DSM-IV and ICD-10 systems have an excessively large number of formalized diagnosed categories, certainly well beyond a limited set that would both encapsulate principal categories and meet clinicians’ needs for communication. And any advantages of such large sets to research endeavours has, as yet, to be demonstrated.
While it is difficult to be absolute in terms of the number of DSM- and ICD-defined conditions – as a consequence of the multiple matrices – we estimate that the ICD-10 system has approximately 100 unipolar depressive conditions, while DSM-IV has more than 200. The latter high number partially reflects the DSM system having a number of specifiers (e.g. ‘melancholia’, ‘psychotic’, ‘catatonic’, ‘atypical’, ‘post-partum’, ‘due to medical condition’) but also its dimensionalizing of severity, persistence and recurrence – persistently and recurrently. The point raised here is whether dimensionalizing such parameters is worthy of formal subclassification, or better viewed as belonging to the clinical domain (i.e. being informative but not diagnostically definitive).
How well are categorical unipolar subtypes handled in formal classificatory systems?
If we assume that categorical depressive subtypes exist, it is worth questioning how well they are addressed in formal classificatory systems.
There are two clear candidate depressive subtypes: melancholic depression and psychotic depression. Melancholic depression is advanced as a putative category because there has been long-standing recognition of such a subtype, albeit variably called endogenous, typical, Type A, classical or melancholic depression with a number of ascriptions – including a more distinctive genetic and biological underpinning, minimal placebo response, and preferential response to antidepressant medication above and beyond psychotherapy. Psychotic depression has also been assumed to reflect a diagnostic subtype, partially because of its categorical clinical feature (delusions and/or hallucinations), as well as showing a preferential treatment response where combination antidepressant and antipsychotic drugs, or electroconvulsive therapy (ECT), are distinctly superior to antipsychotic or antidepressant alone, and here too, the placebo response rate is extremely low.
Turning to the formal classification, ICD-10 allows depressions to exist with ‘somatic symptoms’, but which it states could also be called ‘melancholic’, ‘vital’, ‘biological’ or ‘endogenomorphic’. ICD-10 goes on to note that the ‘scientific status of this syndrome is …. somewhat questionable’ so that ‘this syndrome can be recorded by those who wish, but can be ignored without loss of any other information’. Because the ICD-10 system allows melancholia to either be recorded or not recorded, it neither positions melancholia according to a unitary or binary model, but effectively adopts an arbitrary model.
In DSM-IV, melancholia is positioned as a subtype of ‘major depression’. Logically then (reflecting its subordinate status), we would anticipate it having defining clinical symptoms that are independent of the criteria for major depression. If we compare the criteria sets for major depression and for melancholia, however, then all but three features are shared. Thus, an individual who has the following criteria: anhedonic mood, early morning wakening, weight loss, excessive or inappropriate guilt, and psychomotor disturbance, would meet criteria for (i) major depression and for (ii) melancholia. Such an overlap effectively risks defining major depression and melancholia by the same criteria. The minimal differentiation therefore predictably risks failure to identify any differential cause or treatment for melancholia, which then advances the conclusion that there is little utility to diagnosing melancholia. This then further leads to the view that subtyping is not important, and promotes a default dimensional approach. The problem, however, lies in the intrinsic construction flaws in the DSM model.
Do current diagnostic labels assist communication?
‘Major depression’ is perhaps the best example of a category that is derived dimensionally, and it is certainly one of the commonest DSM diagnoses. It is more than a shorthand communication strategy for clinicians. For many it is also sufficient to initiate treatment. In research it is the principal category used to test the efficacy of drug therapies, psychotherapies and other treatments. It has medico-legal connotations, being sufficient in many countries to ensure hospitalization or medical benefits, and it is a diagnosis often used to quantify severity in medico-legal reports.
Although major depression has been progressively reified as an entity, it is better understood as a pseudo-entity and is responsible for pseudo-profound communication. Its history is worth noting. As previously detailed [8], the initial descriptive profile of major depression in the DSM-III system essentially profiled melancholic depression, with an emphasis on the clinical features ascribed historically to the melancholic subtype. The actual criteria, however, and, more importantly, the decision rules for reaching each of the criteria, were somewhat at variance with the clinical description. Partially, this reflected the DSM-III rule that criteria be set at the ‘lowest level of inference’. This meant that a positive rating could be achieved fairly readily on many criteria, leading to a positive diagnosis of major depression, and so contributing to the substantive increase in lifetime clinical depression noted earlier. Thus, an individual can reach DSM-IV criteria for a major depressive episode if they (i) feel sad or empty; (ii) have a change in appetite; (iii) feel fatigued; (iv) have insomnia or hypersomnia; and (v) are indecisive, for ≥2 weeks, and if the symptoms ‘cause clinically significant distress or impairment in … functioning’. The criteria required to reach such a diagnosis are therefore not necessarily substantive, while the impairment criterion is loosely operationalized. ‘Major depression’ therefore is likely to subsume depressive conditions ranging from major to quite minor expressions as a consequence of the low threshold for caseness.
I suggest that major depression is better viewed as a ‘domain’ diagnosis – in the same way that ‘major dyspnoea’ might suggest a respiratory domain of relevance rather than a definitive diagnosis. Few physicians or patients would view a diagnosis of ‘major dyspnoea’ as sufficient – either as a diagnosis or to dictate treatment. Each would wish to know the underlying condition or pathology (be it asthma, pneumonia, pulmonary embolus or emphysema), because treatment would only then become rational.
In reality ‘major depression’ and other dimensionally based diagnoses subsume multiple different depressive conditions, each of which may have their unique or overrepresented causes, differing pathologies, and differing intrinsic capacities to respond to differing treatments. Effectively homogenizing these multiple conditions into a single dimensionally based categorical diagnosis does not offer an effective tool for clinician communication. At best, a diagnosis of ‘major depression’ is an approximate of the possibility of clinical depression but, because the diagnosis can be achieved for relatively minor depressive expressions, it remains unclear what a diagnosis of ‘major depression’ actually means. Because the DSM systems from DSM-III through to DSM-IV have been atheoretical, with no consistent causes identified as leading to ‘major depression’, no consistent neurobiological underpinnings, and no treatment specificity, it is difficult to view ‘major depression’ as a valid entity or category, and it is therefore better viewed as a pseudo-entity that has led to sterility of research and clinical practice.
Reliability failures of the classificatory systems
The architects of the DSM-III classificatory system argued that one of the principal advantages of their criterion-based approach to diagnosis was to promote and achieve reliable diagnoses. Many claims were made that the DSM-III system ensured reliable diagnoses of the mood disorders. In fact, the field trial reliability data were so poor that they were never formally reported [9]. Following the release of the DSM-III system, independent post-release studies showed extremely poor reliability data for DSM categories such as ‘major depression’. For example, Anthony et al. quantified a kappa coefficient of 0.25 for ‘major depression’ [10]. Subsequently, other commentators noted that ‘major depression’ was one of the most unstable diagnoses in terms of reliability. Thus, while the DSM architects claimed high reliability for the system, such claims were never substantiated, leading Kirk and Kutchins to conclude that ‘It was the claims of success, however, that were successful’ [9]. Because few formal studies have examined the reliability of ICD-10 depression diagnoses, it must be suspected that, as for the dimensionally based DSM systems of recent times, the ICD-10 system is also intrinsically unreliable.
Do formal diagnoses inform about treatment options?
As reviewed elsewhere, the evidence base in relation to treatments for major depression is the largest database we have in psychiatry [11]. In one meta-analysis old and new antidepressants were compared (150 studies, 160 000 subjects), with quantified response rates of 54% for each group [12]. In another meta-analysis comparing exemplar old antidepressants (i.e. tricyclic or TCA drugs) and new antidepressants (selective serotonin re-uptake inhibitors or SSRIs), no difference in efficacy rates was determined [13]. In a meta-analysis comparing psychotherapy trials against pharmacotherapy only trivial superiority to the pharmacotherapy was demonstrated [14]. In another meta-analysis of 28 randomized control trials for psychotherapies, response rates of 50% for cognitive behaviour therapy (CBT), 52% for interpersonal psychotherapy (IPT), and 55% for behaviour therapy (BT) were derived [15]. In essence, meta-analyses found similar response rates for all antidepressants and all tested psychotherapies, allowing an ‘equipotency’ model.
Consequences of an equipotency treatment finding
So, the randomized control trial efficacy database fails to demonstrate any single treatment as being superior to any other for major depression – and a similar overall finding has been generated in regard to the other DSM-IV category, ‘dysthymia’. Thus the risk is that treatment is more likely to be determined by the background training or interest of the professional rather than by characteristics of the disorder: the patient is fitted to the therapy rather than the therapy being fitted to the disorder. Such a non-rational model is out of kilter with practice in other fields of medicine. We can return again to the example of major dyspnoea. A domain diagnosis such as this might include subpopulations of those with asthma, pneumonia and a pulmonary embolus – as well as a range of other conditions. If varying specific therapies (e.g. bronchodilators, antibiotics, anticoagulants and other treatments) were to be compared as treatments for major dyspnoea, it would be conceivable (albeit depending on the prevalence of the constituent disorders within the overall group) that such differing therapies might appear to be of equivalent effectiveness. The average respiratory physician and the average patient would not, however, be sanguine about such an approach. Most patients would expect their clinician to subtype the pathological process and to prescribe a disorder-specific treatment rather than a treatment selected from a smorgasbord of treatments for ‘breathlessness’. Applying a single therapy as if it has universal application – a consequence of a dimensional model – should be of major concern.
Clinical limitations of dimensionalizing classification and assessment
There are many who argue for a dimensional model and, as we are briefed about new developments in the DSM system, we learn of the greater likelihood of an even more distinctive dimensional model in DSM-V. In reality it is possible to dimensionalize everything that we might seek to classify. Asked to distinguish between Australia and New Zealand we could simply say that the former was bigger. Asked to advise on a car to buy we could merely recommend a ‘large’ or ‘small’ car, and ignore make or any other categorical specification. Studies have been undertaken in large community populations that factor analyse every DSM symptom, with imposed two-factor solutions demonstrating underlying internalizing and externalizing constructs. Scores on such dimensions may correlate with a range of varying factors (e.g. gender, age, use of services), but how useful are they at the clinical level? How many psychiatrists operate to a Minnesota Multiphasic Personality Inventory report or other dimensional model, as against seeking to derive a more specific clinical diagnosis or formulation?
Turning again to a medical analogy, we could, for example, dimensionalize breast lumps as ‘big’ or ‘small’. Few women with a breast lump, however, would be likely to appreciate such a model. They would want to know whether it was a benign cyst or a malignant tumour, because subtyping of the pathological process would inform them about both prognosis and rational treatment.
A dimensional model is appropriate only if the subsumed conditions truly lie along a dimension and do not have any distinct attributes. As noted earlier, melancholia has long been viewed as a distinctive and categorical depressive subtype; but if any of its prototypic categorical or distinctly overrepresented clinical features are not included in the clinical definition or in analytic databases, then identification of any such depressive subtype will be prevented. Again as noted earlier, the overlap between criteria used to define major depression and melancholia in DSM-IV build to such a risk.
Psychiatry is not alone
In A short history of nearly everything Bryson noted how, before Linnaeus, botany had ‘a highly reasonable classificatory system’ with multiple binary models (e.g. wild vs domesticated, large vs small). Now botanists offer varying estimates of phyla (20s to high 80s) with the model depending on whether biologists are ‘lumpers or splitters’ and, as noted by Bryson, there is, in fact, ‘more disorder in the system than most people realize’. Bryson went on to note that ‘Taxonomy is described sometimes as a science and sometimes as an art, but really it's a battleground’ [16].
How might the mood disorders be better modelled?
In a relatively recent paper McHugh noted that ‘Psychiatry's most obstinate challenge … is how to bring its diagnoses and explanations together’, and that since the 1980s ‘quite simply, the [DSM] process got out of hand’ [17]. McHugh argued that ‘Psychiatry must do what medicine did in the nineteenth century, and adopt a synthesizing set of etiopathic clusterings’. This is akin to the anthropological approach of adopting ‘thick description’ or pursuing a ‘fuzzy set’ logic to disorder definition.
McHugh argued for four clusters, of which three are relevant here. One comprises ‘brain diseases that directly disrupt neural functioning’, and we might include psychotic depression, melancholic depression, and bipolar I and bipolar II conditions in this cluster. A second cluster comprises those ‘vulnerable to mental unrest because of their make-up’ and we might put here depressive disorders predisposed to by personality vulnerabilities. A third cluster comprises ‘distressing mental conditions provoked by events’ – and here stressful life events are viewed as of aetiological importance. Such a model will be developed shortly.
A model for proceeding
Psychiatry long debated whether the depressive disorders could be modelled according to a simple categorical binary view (i.e. endogenous vs reactive/neurotic) or, alternately, modelled dimensionally. Because depression can manifest in multiple ways (including diseases, syndromes, disorders, existential states and even as a normal response), it would appear wiser to concede multiple models. The task then would be to derive categories when valid and, when not valid, to consider what domains might be able to be dimensionalized. Some personal models will now be overviewed for consideration.
Bipolar disorder
In a large clinical sample we established that the core elevated ‘mood/energy’ state was only marginally higher in those who met DSM-IV criteria for bipolar I disorder than in those who had a bipolar II condition, suggesting that the core dimensional state was unlikely to differentiate those two conditions [18]. Those, however, who had been psychotic during a high had a 50% chance of having experienced a psychotic episode when depressed. In contrast, of those who had never been psychotic when high, none had experienced psychotic symptoms when depressed. This suggested that psychosis oscillates independently of the core mood/energy domain, and is a categorical feature (i.e. present in bipolar I and absent in bipolar II elevated mood states). Further, it suggested an ‘isomer’ or ‘mirror image’ model for conceptualizing bipolar I and bipolar II states. Specifically, those with a bipolar II disorder oscillate across increases and decreases in core mood and energy parameters, but do not experience categorical psychotic states. In contrast, those with a bipolar I disorder experience similar oscillations but, in addition, have psychotic features during the elevated state and are likely also to experience psychotic features during the depressed state. The proposal then is that a diagnosis of bipolar I disorder should be restricted to those who experience psychotic features at some stage of their bipolar illness, and that bipolar II disorder is quintessentially a non-psychotic condition. This is a heuristic model presuming that differing factors contribute to independent mood/energy and psychotic components, and providing a simple structure for pursuing aetiological and treatment implications.
Because treatment guidelines for bipolar disorder are invariably written for those with bipolar I disorder and clinicians commonly extrapolate management of bipolar II conditions from guidelines for bipolar I disorder, this categorical model (weighting the respective presence or absence of psychotic features) has the capacity to pursue quite contrasting management possibilities – either that bipolar I and II disorders are similarly responsive to differing intervention strategies or that there are condition-specific differences.
Depressive disorders
In a series of publications [overviewed 11] we have detailed structural and functional models for three principal depressive subtypes. Basically, we have proposed that both psychotic and melancholic depression are categorical conditions, and phenotypically distinct from a residual set of non-melancholic disorders. Melancholia is distinguished from the non-melancholic conditions by the specific presence of psychomotor disturbance (PMD). While the PMD is even more severe in psychotic depression, psychotic depression is distinguished from melancholic depression by the specific presence of psychotic features (i.e. delusions and/or hallucinations). The functional model argues that, if there is any neurotransmitter contribution to the non-melancholic disorders, it is principally serotonergically mediated. In contrast, there is a greater noradrenergic contribution to melancholia and a greater dopaminergic contribution to psychotic depression. If that model is valid, then we would expect to see differing responses to differing treatments across the three broad depressive conditions.
Does the three-class subtyping model demonstrate treatment differentiation?
There have been two meta-analyses in relation to psychotic depression [19], [20]. These analyses in effect quantified an 80% response rate to ECT and a similar 80% response to combination antidepressant and antipsychotic; a 33% response to antipsychotic alone; and a 25% response to antidepressant alone, while the placebo response rate was estimated to be approximately 5%. This is a striking gradient, quite at variance with the equipotency finding for treatments of major depression.
In relation to melancholic depression, the antidepressant drug response was quantified at approximately 60% in comparison to a placebo response rate of 10% [11], while the evidence-based psychotherapies (CBT and IPT) appeared to have lower response rates than the antidepressant drugs [21], [22]. ECT has also been quantified as highly effective [23], albeit being required far less frequently.
Importantly, for those with melancholia, we have shown differential response rates across differing antidepressant drug classes and in conjunction with an age effect. For instance, in one study we specifically compared the response rate to SSRIs and TCAs [24], [25]. There was no differential for those with a non-melancholic depression. A different pattern emerged, however, for those with melancholia: for those aged under 40 years of age the TCA was only marginally superior to the SSRI; for those aged 40–60 years the TCA was twice as effective; and for those aged 60 or older the TCA was fourfold as effective. Because the phenotypic picture of melancholia changes with age – with psychomotor disturbance becoming far more overt and distinctive – there may be a link between the changing phenotypic picture and such a differential drug response. For example, for those who have melancholia, there might be a progressive recruitment of monoaminergic systems with increasing age, resulting in more psychomotor disturbance during the melancholic episode – so providing an answer as to why a narrow-spectrum antidepressant such as an SSRI may either ‘poop out’ or be comparatively less effective than a broad-action antidepressant.
In summary, delineation of psychotic and melancholic depression is important because these conditions have different response gradients to differing treatments, with those gradients being at sharp variance with research studies of groups selected by a diagnosis of ‘major depression’ – and for whom most treatments (drug or psychotherapy) have comparable efficacy rates and where active treatment commonly fails to differentiate from placebo in randomized control trials.
Modelling the non-melancholic disorders
As noted earlier, the non-melancholic disorders do not form a categorical class; they are more a class capturing residual non-psychotic and non-melancholic conditions. For this expression of depression there are no distinct clinical features. Features that were once held to define reactive and neurotic depression (e.g. mood reactivity) are merely the converse expression of the non-reactive mood state that is likely to be evident in melancholia. Because there are no distinctive or phenotypic clinical features, a dimensional model is the default option, and we have argued [11] for dimensionalizing two key constructs – stress, and temperament or personality style – akin to two of McHugh's clusters.
This model allows that some individuals may develop a non-melancholic depressive condition purely as a consequence of acute salient and/or severe stressors that impact on their self-esteem (previously called ‘reactive depression’) or, if the stressor (and/or its impact) is persistent, causing an ongoing chronic stress-based non-melancholic disorder.
In terms of any dimensional personality contribution, we have developed the Temperament and Personality measure [26], which was derived from a clinically observed ‘bottom up’ a priori model that posited eight personality types. Subsequent investigation of the model in two large samples supported the a priori model but also explicated the structure of the eight dimensions. Three emerged from a higher-order personality style of intraversion (‘perfectionism’, ‘personal reserve’, and ‘social avoidance’) while five emerged from a higher-order ‘neuroticism’ factor. Of these five, one (‘anxious worrying’) reflected internalized high-trait anxiety while another (‘irritability’) more reflected externalized high-trait anxiety. ‘Self-criticism’ and ‘sensitivity to rejection’ were, again, strongly related to anxiety, while the final personality style (‘self-focused’) captured a style of entitlement and poor tolerance to stress and frustration.
We presume pure stress-determined and pure personality-determined non-melancholic disorders to be rare: it is more common clinically to observe their interaction. In consequence, we have developed a ‘spectrum’ model. This model assumes that such personality styles not only increase the risk to a non-melancholic depressive condition but ‘fuzzily shape’ the phenotypic picture. The clinical picture is, of necessity, fuzzy because the personality constructs do not comprise independent dimensions but somewhat interdependent ones. Nevertheless, we have been able to flesh out non-melancholic spectrum conditions for at least six of the eight candidate personality styles [27]. Individuals who internalize their high trait anxiety and who have an anxious worrying personality style are likely, when faced with a stressful offence that impacts on their self-esteem, to develop a picture of ‘anxious depression’ (marked by worry, anxiety, keeping to themselves, crying), while those who externalize their high trait anxiety along an irritable personality dimension, are more likely to develop a phenotypic picture of irritable depression (in being irritable and crabby). Those who are more self-focused tend to develop a ‘hostile, volatile and impulsive’ state when depressed and often diffuse their anger on those around them. Those who have essentially shy personalities (i.e. ‘social avoidance’ and ‘personal reserve’) are likely to withdraw socially when depressed, becoming insular and resisting support. Those who have a ‘perfectionistic’ personality tend to work harder, seek distraction and try to control things during their depression, making it difficult to form a treatment alliance. Those who have a personality style of ‘rejection sensitivity’ are inclined to feel rejected and abandoned when depressed, and engage in a rich repertoire of self-consolatory coping strategies, including the development of the so-called atypical symptoms of hyperphagia and hypersomnia.
DSM-IV has one spectrum disorder (‘atypical depression’) in that its criteria both comprise clinical symptoms as well as a personality style of ‘interpersonal rejection sensitivity’ as an accessory feature. We would reframe that definition of atypical depression to prioritize the personality style of rejection sensitivity as the primary feature (i.e. personality style as a fulcrum) and then view many of the symptoms as either a reflection of that personality style and/or coping repertoires used by people with such a personality style. It is unlikely, however, that atypical depression is the only spectrum condition, and thus we suggest that there may be considerable utility in developing the concept to include other personality-based non-melancholic disorders, and then determine whether treatment differentiation occurs across those non-melancholic spectrum disorders.
It might be expected that those with the more reactive disorders would show preferential response to strategies that assist them to come to terms with the stresses or effectively neutralize the stresses, while for individuals with personality-based conditions, differing treatment modalities might be expected to have differential impacts. For example, for those with a distinct anxiety-based non-melancholic disorder, an SSRI antidepressant might be expected to have greater benefit than for those with personality styles unassociated with high trait anxiety. Conversely, for those whose introversion contributes to their depressive disorder, then a BT-based approach might be of benefit, while for those who have high levels of self-criticism and the associated cognitive schema, a CBT approach might be anticipated.
In essence, testing such an approach approximates to much clinical practice, where the clinician effectively undertakes a pattern analysis to partition differing clinical subgroups or vignettes, and then provides differential interventions based on hypothesized or formulated putative causal factors – rather than merely provide a universal treatment or one based merely on the severity of the condition. The extent to which each contrasting approach provides a model for a superior outcome would clearly benefit from fine-focused research.
Conclusions
In the Introduction to DSM-IV it is stated that the manual's highest priority is to provide a helpful guide to clinical practice, with the ‘additional goal’ being ‘to facilitate research and improve communication among clinicians and researchers’.
In reality, that atheoretical and non-specific dimensionally based diagnostic system creates non-specific entities such as ‘major depression’ and ‘dysthymia’, and therefore courts non-specific results in relation to causes, outcomes and treatment differentiation. Such an expectation has been realized.
It is, then, of concern that there is so little unease about dimensional classificatory models that ignore aetiology, weakly differentiate normal depressed mood states from clinical depression, define subordinate conditions such as melancholia with redundant and non-differentiating criteria, have poor reliability, do not identify treatment differential effects, nor inform us about treatment options nor advance research studies. Further, subclinical constructs such as ‘subsyndromal depression’ and ‘soft sign’ bipolar disorder suggest a reductio ad absurdum scenario that should invite disquiet from professionals and from the public.
Such issues should raise a set of questions about a principal dimensional model for classifying mood disorders. Why is such a lack of commonsense reified rather than challenged? Why are those in the field not embarrassed about such a limited model in highly sophisticated times when there is so much active research? The current dimensional models encourage ‘one size fits all’ therapeutic approaches, which – across randomized controlled trials – have failed to demonstrate any treatment specificity when such a model is adopted. By comparison, when a subtyping model is respected (to the extent that it has explanatory power), treatment differentiation effects emerge. The latter finding alone should encourage further studies that seek to identify fuzzy sets from phenotypic and aetiological clustering, for progressive refinement, and then for advancing relevant differential clinical management – such, as McHugh has argued [17], as occurs across the rest of medicine.
If the challenge put here is rejected (i.e. that an overall dimensional severity-based model is of low utility), then the onus is on those supporting such a model to detail how diagnoses such as ‘major depression’ inform them about differential causes and treatment selection. Until then we must suspect that our classificatory systems for mood disorders are taking us down blind alleys rather than providing useful road maps.
Footnotes
Acknowledgements
My thanks to Kerrie Eyers, Yvonne Foy and Matt Hyett for manuscript assistance. Research supported by an NHRMC Program Grant (510135) and funding from the NSW Department of Health.