
Abstract
Objectives: The aim of this study was to explore the issues around continuing professional development (CPD) for physiotherapists working as lone practitioners in amputee rehabilitation in the United Kingdom (UK).
Design: Qualitative method using a phenomenological approach via one to one semi-structured interviews and thematic data analysis.
Setting and participants: Ten physiotherapists with responsibility for amputee rehabilitation working as lone practitioners in hospitals or specialist centres in the UK.
Results: CPD is valued and there is commitment towards the process. Current solutions are identified but there are frustrations around more structured CPD and organizational issues. These include inadequate access to learning opportunities, lack of professional feedback, insufficient time and limited learning skills.
Conclusion: There are opportunities for improving CPD through organizational structures but specialist input is recommended to support lone practitioners and managers with the process, e.g., consultant or peripatetic therapists.
Introduction
Continuing professional development
During recent years there has been increasing emphasis in the National Health Service (NHS) in the UK on improving quality and accountability through clinical governance. One important aspect of this is the responsibility of healthcare professionals for updating practice through continuing professional development (CPD) (Department of Health [DoH]1998). The term CPD is used to denote the process of ongoing education and development, to maintain competence and increase professional proficiency and expertise (Alsop 2000). CPD activities range from familiar types of ‘formal’ learning such as courses and post-graduate qualifications to increasingly recognized ‘informal’ work-based learning and reflective practice.
The UK's Chartered Society of Physiotherapy's (CSP) Rules of Professional Conduct (CSP 2002) and Core Standards of Practice (CSP 2005) stipulate that physiotherapists are expected to undertake CPD. This is largely an individual responsibility but requires support from management, peers, and professional and regulatory bodies (Spalding et al. 1999; Pringle and Moore 2001; Health Professions Council [HPC]2006). As from 2010 the registration of physiotherapists in the UK will be dependant on evidence of relevant CPD (HPC 2006). Whilst there is professional and organizational support for CPD, constraints such as busy clinical caseloads, finance, time and personal commitments, presents barriers to many physiotherapists participating in it effectively (O'Sullivan 2003).
Physiotherapists, amputee rehabilitation and lone working
Many physiotherapists work in small clinical specialties one of which is amputee rehabilitation. Professional guidelines (Broomhead et al. 2003) recommend that physiotherapists specialized in amputee rehabilitation be responsible for the management of this patient group. Despite the guidelines, the amount of experience (in this clinical speciality in the UK), varies in physiotherapists. Most physiotherapists with clinical responsibility for amputee rehabilitation work in hospitals where the caseload may also include non-amputee patients. Physiotherapists also work in Disability Service Centres (DSCs) where the caseload is predominantly amputees and are managed by a specialist multi-disciplinary team (MDT).
In either setting physiotherapists with responsibility for amputees may work alone, or alongside junior physiotherapists or assistants, but only occasionally with other physiotherapists with experience in amputee rehabilitation. In DSCs the amputee physiotherapist may be the only physiotherapist. Whilst not necessarily geographically isolated, they can be described as lone practitioners in that they are professionally isolated and face a deficiency in available colleagues with whom they can relate, or a lack of involvement with peers of the same profession (Shreffler 1992; Solomon et al. 2001). Whilst there are some benefits to lone working such as greater independence and autonomy (Davis and Droes 1993), lone practitioners can face considerable challenges, such as little peer support, review or relevant supervision (Bithell and Minns Lowe 2000).
The purpose of the study
Given the challenges outlined above, the question arises how these physiotherapists achieve the skills and knowledge development for clinical practice. Literature exists describing barriers to CPD for physiotherapists (Titchen 1987; Spalding et al. 1999; Pringle and Moore 2001; O'Sullivan 2003) however little refers to CPD and physiotherapists in the context of lone practice (Bithell and Minns Lowe 2000; Solomon et al. 2001) and none relates to physiotherapists working in amputee rehabilitation. There are examples of how CPD is or could be achieved for health professionals, however in these studies the context is primarily in relation to geographical isolation (Dunning et al. 1994; Bithell and Minns Lowe 2000; Parkin et al. 2001).
The focus of this study was to explore the challenges of CPD by interviewing a sample of physiotherapists, with the aim of identifying if further support or strategies could contribute to professional development.
Method
The study employed a phenomenological approach which explores the meanings individuals give to particular experiences they have had (Jensen 1989; Krefting 1991; Grbich 2003) in this case being a lone practitioner working with amputees. Data were collected through one to one semi-structured in-depth interviews.
Ethical approval for this study was granted from the University of Brighton, School of Health Professionals. Participants were recruited by virtue of their membership of a professional organization i.e. clinical interest group (CIG) – in this case BACPAR (British Association of Chartered Physiotherapists in Amputee Rehabilitation). Participants were identified as eligible if they were:
A senior physiotherapist with responsibility for amputee rehabilitation, part or full-time; and The sole physiotherapist with responsibility for amputee rehabilitation within workplace setting or working alongside a more junior staff member and/or assistant only.
Twenty-eight physiotherapists were identified from the CIG membership within the London Region from which a purposive sample was selected to provide a group representing a range of different characteristics (i.e., different workplace settings and job roles).
Ten physiotherapists with a mean age of 34 within a range of 28–44 years were interviewed. Experience of working with amputees ranged from six months to 20 years, with the mean length of time being six and half years. Seven participants worked in a hospital setting, two in DSCs, and one worked in both. Eight held permanent posts, six held senior posts; two with additional managerial responsibilities, and two were less senior in grade and their posts were rotational. Four participants worked part-time. Three participants worked solely with amputees.
A semi-structured approach allowed the researcher to explore issues around CPD and lone practice, and included questions around how CPD was achieved and what constraints were experienced. Prompt questions were used as necessary to guide the conversation. Signed written consent was obtained before each interview and in total 10 interviews were conducted. Interviews were conducted by one researcher and were tape recorded and transcribed anonymously. Field notes were made immediately after each interview to document impressions and perceptions, the dynamics of the interaction and any problems encountered (Clifford 1997).
Data analysis
Data were analysed for thematic content using an iterative process systematically categorizing and coding the interview transcripts through various stages (Burnard 1991; Hancock 1998; Grbich 2003). As interviews were performed, concepts evolved which were reflected in the researcher's ‘field journal’.
A common criticism of qualitative research is that is subject to researcher bias (Pope and Mays 1995). Triangulation (Burnard 1991) was chosen to address validity and reliability. An unmarked transcript was read by a second party experienced in qualitative data analysis, highlighting sentences and key words perceived as relevant, and the same process of categorizing and ‘collapsing’ was followed (Lincoln and Guba 1985). Additionally one randomly selected participant was asked to check the accuracy of their interview transcript and the interpretation of the data according to the categorization process.
Findings
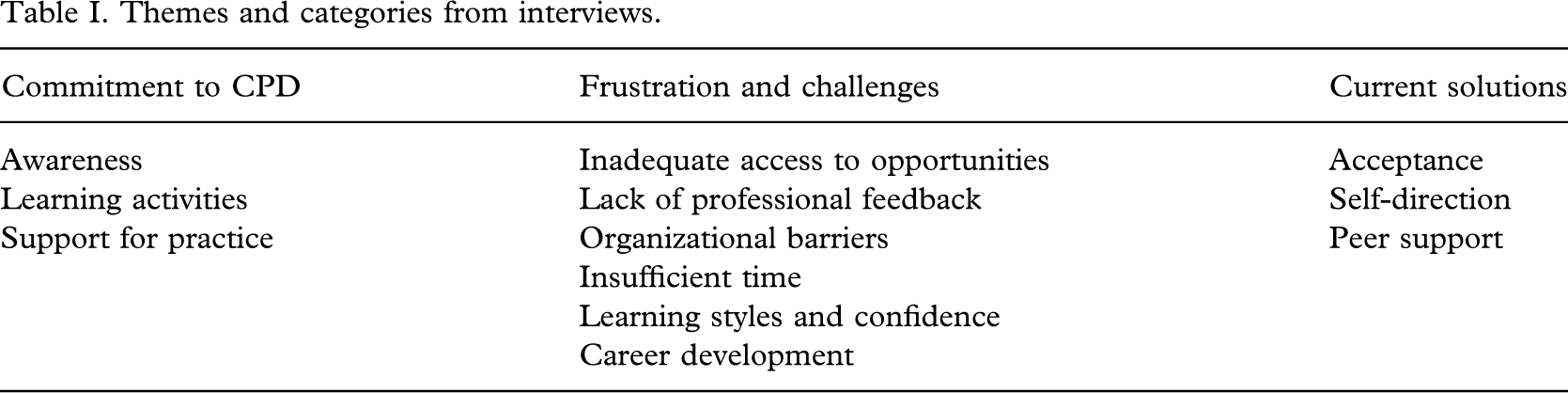
CPD was raised and discussed by all participants and constituted a major part of each interview. The experience of being a lone practitioner was also described. Three themes representing commonalities emerged, namely:
‘Commitment to CPD’, ‘Frustrations and challenges’, and ‘Current solutions’.
Each theme comprised several categories. See Table I.
Themes and categories from interviews
Commitment to CPD
Awareness
There was awareness of the need for CPD amongst participants and a commitment to undertaking it. CPD is absolutely essential … if I'm not keeping up my own CPD I'd be letting my colleagues down, and the juniors and students.’ (P10)
However, as seen later, this commitment could conflict with responsibilities towards patients.
Activities
CPD activities described were not limited to formal training opportunities and included other aspects such as practice education, working with other disciplines, and management responsibilities. This was more apparent in participants who were either older or had had more experience in the field. Teaching keeps you abreast of what's going on because they [the students] are constantly questioning you. (P1) Joint sessions with the prosthetists … we try to do as many of our fit-deliveries together so that if they're learning a new casting technique I learn as well. (P10) I'm active with benchmarking groups … . , and although that's not learning a new technique for managing an amputee, it's around the service and it's a clinical issue … . , it works both ways, I've taken my physiotherapy experience to those … . and I've learned from those experiences in my own practice. (P1)
Support for practice
Participants identified and recognized limitations in their knowledge and skills. If I've got a real problem with something I can ring someone from the limb centre; I've got a lot of colleagues and contacts. (P5) She's [colleague in DSC] brilliant and she sometimes comes over to spend some time and do problem-solving with our patients … she's always at the end of the phone and doesn't mind how stupid queries are. (P8)
Frustrations and challenges
A number of barriers and frustrations were identified.
Inadequate access to opportunities
There were few opportunities to access in-service learning. There isn't anybody to deliver it. That's the big difficulty. (P2) We do a multidisciplinary in-service four times a year but other things overtake it… (P6)
Lack of professional feedback
Not having easy access to specialist staff was seen as a barrier to CPD for less experienced physiotherapists. Not having other amputee therapists on site is certainly a constraint because the knowledge isn't passed over quickly … . and I'm going to have to take days away and it's time I've got to agree with other staff, it's not easy to do that. (P3) The amount you learn from your seniors is huge and they have massive experience in respiratory, and have been there for years and years. It's brilliant and you get so much good feedback and help and learning. Not having anyone with that in amputees, you lack that almost completely. (P8)
Individual practitioners viewed the lack of direct observation of their practice as problematic. It's a bit difficult in terms of seeing how you develop when you've not got anybody senior who is a specialist and who has the skills to observe. It's [observation of practice] uncomfortable but it's important. If you don't have that you don't know what you're doing wrong, you don't know where you need to develop and you could quite easily coast along thinking that everything's hunky dory. (P2) I've never seen another physio teach a patient how to use a prosthesis. So I only know from what I've done. I don't know if I do know! Maybe I don't … (P7)
Instead, feedback regarding practice came only directly from patients, or indirectly as a result of patient outcomes.
Organizational barriers
Whilst managers appeared supportive of clinicians attending courses and study days, frustrations were expressed when managers failed to understand the individual or amputee service needs. Only one participant used her appraisal as a tool to provide focus for CPD. My appraisal is done by a very respiratory focused person. There's no one above us who has that interest or knowledge to say ‘OK, this is what you're doing, why don't you go and …’ because they don't know, and that is key … (P8) If it's in your appraisal you've got the back-up to make sure you're given time to attend relevant meetings and conferences … otherwise she wouldn't have seen that as important, to see and meet colleagues. (P1)
This seemed to be compounded by a lack of formal recognition of the necessity for CPD at an organizational level. Within the Centre there is vast knowledge, both clinical and managerial … that we don't disseminate, but until we are forced to show evidence, priority will always be patients, and until the whole culture changes people won't do it (CPD). (P10)
Insufficient time
Time for CPD was viewed as an important resource but could be limited despite policies. Our trust (hospital) says you can have half a day a month. When you're the only senior, to choose between sorting out a folder, or offering patients appointments, patients always win hands down. (P10)
Taking time for CPD had implications for those with other responsibilities. Time is the biggest thing, really. My responsibilities lie outside amputee rehab as well, so for me to attend a study day I have to make sure that the rest of the caseload is covered, not just the amputee side of things. Taking a day off isn't just taking a day off the amputee service, it's taking a day off everything else as well. (P4) My biggest constraint is time. I find it very difficult working part-time. (P6)
Learning and confidence
Limited understanding and application of adult learning principles and personal factors such as age, experience and attitude could influence CPD. I need help (with reflective practice) because I don't know where to begin, I've been saying ‘what do we put down, what do we put down?’. (P9) I was in the generation before… where we didn't have CPD diaries and so although we all know it's right and should be done, it's not integral in your existence. (P5)
Career development
Limited CPD opportunities and lone working were perceived as impacting on career development for some participants. That's another issue with the isolation, I've not had the opportunity to develop my managerial skills whereas if I was in a classic neuro team in an acute setting I might be the senior one of a team of 6 or 7 … . and you're doing your management stuff, whereas I struggle with that. (P10) Where do you go, where do your clinical skills take you? Clinical specialist roles within the amputee world are few and far between. It's dead man's shoes. Where do you go with that expertise? (P1)
Current solutions
Acceptance
To some extent participants accepted that as lone practitioners they needed to be proactive in approaching CPD. There are downsides to being isolated but you just have to get on with it and shout out for help as and when. (P10)
Self-direction
There were examples of self-directed learning. Where I've found a lot of support is BACPAR and in particular interactive CSP (website), the question forum, putting questions out and answering them. People ask questions and you think ‘that wasn't such a silly problem that I had’; it's not just me who's thinking that … . So that's been useful, that's been a good place to turn to… (P2) I went off and did 6 months in musculo-skeletal outpatients to further improve my skills… that was an important part of my CPD. (P5)
Peer support
Networking and meeting up with like-minded physiotherapists was considered helpful. I really take value when we meet, and we've done them at XXX and we do them at XXX and there'll be 5 or 6 physios, all from different trusts (hospitals), all get together, thrash out problems, work together, maybe have a bit of in-service training … that to me, makes a big difference. (P1)
Whilst a few participants consciously reflected on work-based learning or specific learning opportunities, thinking about practice was easier with a colleague. If I look at what my CPD involves around amputees, it's very much based on reflection on what we're doing. I try and put some reflections on negative things in my CPD diary, and particular issues that come up that maybe I will have discussed with the OT. On a normal day-to-day level, because myself and the OT are so new, we spend ages discussing things, it's your reflections, to bounce ideas off … because we don't have enough experience it's much easier with two of you. (P8)
Discussion
This study examined issues of CPD through exploring the experiences of physiotherapists working as lone practitioners in amputee rehabilitation. Whilst the sample was small and purposively selected, participants were diverse in terms of posts and experience. Data saturation was achieved when no new themes emerged after a certain number of participants' interviews were analysed, categorized and coded. It is possible that the participants' membership of the CIG could imply they were more self-directed and motivated to seek support and achieve CPD than non-members and selection may have reflected a degree of response bias. Despite these limitations, the findings illustrate a commitment to CPD but frustrations and challenges were identified which need resolution for CPD to be most effective.
Lone practitioners' commitment to, and recognition of, CPD
All participants were engaged in CPD to a degree and all reported valuing opportunities. This correlates with previous studies of other health professionals (Gessner and Armstrong 1992; Grant and Stanton 1998). A range of CPD opportunities were described from formal study days, informal peer support networking via the CIG and the internet, to teaching and non-clinical responsibilities. Indeed informal learning was clearly important to the participants and this contrasts with other work which suggests most physiotherapists do not value informal work-based activities (Gosling 1997; Pringle and Moore 2001). This is heartening particularly as this approach to learning is encouraged within the profession (CSP 2004).
O'Sullivan (2003) and Titchen (1987) have suggested that the understanding and relevance of work-based learning appears to be poor. Interestingly, the interviews themselves enabled participants to recognise the learning that occurred through a variety of activities, such as participating in research and audit, which had not been previously associated with CPD.
Some participants clearly described learning through reflection. Reflecting on practice with others was valued and apparent when participants talked about meeting up with peers or colleagues. This supports Roth and Esdaile (2003) who discussed using peers as a ‘sounding board’ to talk through feelings about work. However only a few participants documented reflections or used a portfolio to structure CPD which suggests that there was little conscious association between the two (Boud et al. 1993; Dadds 1997) and indicates that there needs to be a greater understanding of portfolios particularly in view of the UK Health Professions Council requirements around registration (HPC 2004, 2006)
Frustrations related to structured CPD opportunities
Whilst some participants revealed engagement in informal or reflective CPD there were frustrations related to more structured CPD and organizational issues.
Firstly, in-service training (IST) and shared learning opportunities were often problematic. Whilst IST is the most familiar type of informal learning for physiotherapists (CSP 1999) and has many benefits such as improving communication between groups and professions (Alsop 2000) participants described only limited IST in relation to amputee rehabilitation. Frustration was expressed by some who wanted to capitalize on potential opportunities for interprofessional learning but other departments did not always participate. Pringle and Moore (2001) explored the perspectives of CPD from a range of stakeholders and highlighted that practitioners working in specialist areas, where CPD needs were often linked to the specialization, could benefit from shared learning.
Secondly, whilst some managers were seen as generally supportive, frustration was expressed where managers did not appreciate the CPD needs for amputee physiotherapists. Whilst participants reported wanting professional feedback to improve their clinical practice this was not always possible and has implications for patient care and clinical competency. One participant admitted that she did not know if she had the knowledge for some areas of practice. The issue of whether participants were competent to practise was not addressed in this study however it is one of great importance. Clearly, an individual has a responsibility to identify their own learning needs, but what someone feels they need and what they actually need may be two very different things (Orme and Trickett 1983). This is particularly relevant where physiotherapists are new in post and have minimum knowledge or experience of the speciality. In addition, they may also have a line manager from a different professional group who may lack amputee knowledge or experience. There is a need to ensure that skills and competencies are in place particularly as recommendations (Broomhead et al. 2003) that physiotherapists with responsibility for amputee care should be specialized are an unlikely reality in the UK; the small number or amputee patients in hospital settings may not justify a permanent senior physiotherapy post where prior experience is a pre-requisite.
Thirdly, participants illustrated that time away from patients was difficult to arrange and it is argued that time away from patient contact evokes guilt at an individual level (O'Sullivan 2003). Indeed, time was cited as a barrier to CPD and whilst this was not the greatest hurdle, as other studies have described (Spalding et al. 1999; Roth and Esdaile 2003), it was a practical constraint in staff-depleted environments, where posts were split or where participants worked part-time, mirroring previous studies (Dunning et al. 1994; Bellaver et al. 1999; Townsend et al. 2006). Whilst policies encouraged individuals to engage in CPD and recognized the importance of ‘protected’ time, this may not be sufficient; employees need the relevant skills to use this time effectively.
Finally, participants reported lacking personal development reviews or supervision as tools to encourage self-direction, facilitate CPD or provide feedback. Only one participant used her appraisal as a tool to provide focus for CPD, negotiating resources to enable her learning objectives to be fulfilled as recommended (O'Sullivan 2003).
Developing a CPD culture
The frustrations outlined indicate that there needs to be more effective mentoring, supervision, performance and peer review to foster the culture of ‘learning organizations’ where learning is valued as a means of enhancing service and individual professional development (Senge 1994). Whilst there are clear opportunities for improving CPD via appraisals and personal development plans – for example, via the UK Knowledge and Skills Framework (DoH 2004; CSP 2006) – those reviewing development and practice need to appreciate the knowledge and skills required for a particular role. Reviewers may need to consult other professionals to help assess an individual's development needs (CSP 2006). This raises the questions of who to consult, and where to deliver CPD.
Ways forward
In 1997 the UK Department of Health (DoH 1997) highlighted that ‘the more isolated a physiotherapist is professionally, the more important it will be to ensure adequate professional advice and support is available in order to support the individual, protect the public, and ensure high quality services are provided’. Physiotherapy consultants could be of help in this respect with their focus on national initiatives and government priorities, innovation, clinical leadership and practice development, and their explicit remit around education, training and CPD. To date the take up of these posts has been slow and there are less than 40 in existence and few in smaller clinical specialties, with none in amputee rehabilitation. The CSP has indicated that more consultant roles are needed in most parts of the UK (Limb 2005).
Another approach could be the development of a ‘roving’ educator (Dunning et al. 1994) or a preceptor (Dusmohamed and Guscott 1998; Parkin et al. 2001). A preceptor is a skilled practitioner who facilitates professional development and whose roles include that of a needs assessor, educator, mentor, role model, resource person and facilitator of change. A roving or peripatetic clinical specialist role would draw upon these principles and attempt to reduce isolation and provide CPD for lone practitioners with different levels of knowledge and experience.
The question of career development arose in some interviews. From a clinical perspective there is presently a career ceiling within amputee rehabilitation. This study's findings would suggest there is potential for experienced physiotherapists' skills and knowledge to be used more systematically in supporting the needs of others. Such a development could be self-fulfilling, providing opportunities for professional and career development for experienced physiotherapists who wish to remain in the clinical field, contributing to greater motivation and satisfaction, recruitment and retention. Simultaneously, less experienced therapists would receive support. This example ties in with this study's findings and the literature which indicates that feedback from and the presence of someone with specialist knowledge is valued (Alsop 2000). Indeed, this concept has been developed further with recommendations being made for regional posts for amputee therapists in order to standardise the quality of care for this patient group (Evans et al. 2003).
The benefits of a peripatetic specialist could ease the frustrations illustrated here. For example, its on-site nature means that the development needs of individuals could be identified more clearly through clinical supervision. Collaboration with line managers for appraisal may ensure that development needs link to job purpose and service needs. Additionally, where support is provided in the clinical setting, time constraints for CPD are eased by reducing time away from the department which would otherwise be required to access the relevant knowledge or support.
Underlying such developments there should be acknowledgement by managers that professional practice settings – inter-professional and CIG practice, for example – are fruitful contexts for CPD where individual practitioners can gain the confidence and skills to facilitate self-directed professional development.
Such developments would support clinical governance ensuring that physiotherapists improved competence through CPD thus contributing to improved quality of care for patients. Practitioners that do not engage in CPD risk being disadvantaged and managers risk having unregistered staff (White 2005).
Conclusion
This study has illustrated that CPD challenges faced by lone practitioners in amputee rehabilitation are linked to professional isolation and the organizational cultures in which they work. Suggestions are made for on-site support for both lone practitioners and their managers when meeting CPD needs. These include utilizing the knowledge and skills of experienced physiotherapists in the field, developing peripatetic specialist roles, and the implementation of consultant physiotherapists in this clinical specialty.
By addressing the issues that been have expressed, there will be greater assurance that lone practitioners working in amputee rehabilitation will be able to keep up with professional demands around undertaking and evidencing CPD (CSP 2002, 2005; HPC 2004, 2006) contributing to clinical governance in improving services and care for patients. Further work could examine the links between CPD and competency for practice.
Footnotes
Acknowledgements
The authors thank the clinical interest group BACPAR for their support and participation, Barbara Maguire of Wandsworth Primary Care Research Centre, St George's Hospital Medical School, University of London librarians, members of the writing group at Queen Mary's Hospital, Roehampton, in particular Sally Durham, Dr David Ewins and Tom Collins, and to Professor Ann Moore for her comments.