
Abstract
Background:
Factors that are related to mobility apprehension were measured in a sample of persons with lower-limb amputation.
Objectives:
The purpose was to determine whether intensity, interference, or catastrophizing are associated with mobility apprehension.
Study design:
Cross-sectional study.
Methods:
Persons with amputation of a lower limb who were attending a national limb loss conference were recruited to complete a survey. Subjects were administered the Tampa Scale for Kinesiophobia to measure mobility apprehension. The Brief Pain Inventory was administered to quantify the affect of pain on general activity, walking ability, and enjoyment of life. The Pain Catastrophizing Scale was administered to assess the tendency to ruminate and magnify pain sensations. A multivariable linear regression was performed to determine factors associated with mobility apprehension.
Results:
Fifty-three people with lower-limb amputation participated in the study. The mean (standard deviation) score for mobility apprehension was 34.2 (6.0). Mean (standard deviation) pain intensity and interference scores were 1.6 (1.7) and 2.5 (2.6), respectively. The mean (standard deviation) pain catastrophizing score was 9.1 (10). Pain catastrophizing was the only variable associated with higher mobility apprehension (β = 0.31, p < 0.001, R2 = 0.32). Results suggest that for every one-point increase in the pain catastrophizing score, mobility apprehension will increase by 0.3 of a point.
Conclusion:
These preliminary results suggest that pain catastrophizing was related to mobility apprehension in this cohort of persons with lower-limb amputation. This relationship indicates that the exploration of avoidance behaviors, such as pain catastrophizing, may be useful when developing a program for physical rehabilitation.
Clinical relevance
Pain catastrophizing, an avoidance behavior, may be associated with higher levels of mobility apprehension in persons with major lower-limb amputation. Understanding the impact of fear-avoidance behavior will allow clinicians to identify individuals at risk for poor outcomes following amputation surgery and to develop psychological strategies to complement treatment.
Background
In 2005, the prevalence of a major lower-limb amputation in the United States was estimated at 623,000 instances. 1 A “major” lower-limb amputation is defined as the removal of the limb at or proximal to the ankle, including transtibial and transfemoral amputation, and will be considered as a lower-limb amputation throughout this article. 2 Outcomes after a major lower-limb amputation appear to be poor in a small, but important percentage of cases. For instance, approximately 10% of persons with a transtibial amputation required amputation of the contralateral limb 1 year after the index surgery. 3
In an attempt to better understand health outcomes following amputation of a lower limb, cross-sectional and prospective cohort studies have investigated whether different socioeconomic (e.g. age, gender, education level), clinical (e.g. etiology of amputation, comorbidities), physical (e.g. balance, strength), and psychosocial (e.g. quality of life, depression) characteristics might affect patient outcomes.4–7 Results from these studies suggest that the characteristics that contribute most to poor health outcomes are depression and perceived quality of life. Also, a greater number and higher severity of comorbidities influence mental health-related factors 8 (e.g. depression), which is associated with a greater incidence of falls. 9 Studies also report that after lower-limb amputation, patients have high levels of pain in the form of chronic low-back pain, residual limb pain, and phantom pain leading to restrictions in functional activity.6,8
Patients with high levels of pain 6 and disability 10 are at risk of developing avoidance behaviors. Vlaeyen et al. 11 developed the fear-avoidance model, which suggests that after an injury or surgery there are two pathways a patient will take based on their interpretation of acute pain. Pain as a result of injury or surgery that is perceived as non-threatening generally leads to the patient’s recovery and return to normal activities of daily life. In contrast, pain that is perceived as threatening causes anxiety and induces mobility apprehension or fear of movement. Mobility apprehension that continues beyond the expected healing time leads to avoidance behaviors (Figure 1).
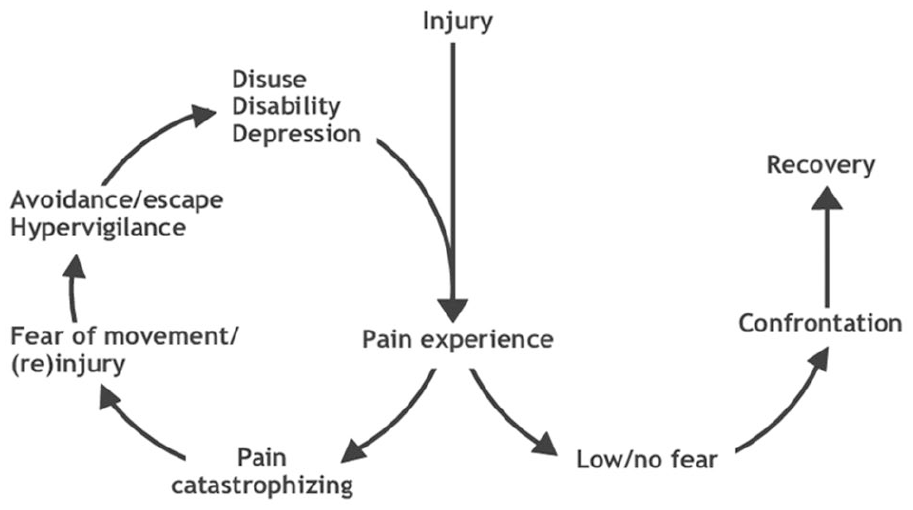
Fear-avoidance model of Vlaeyen et al. 11
Pain catastrophizing is the tendency to ruminate and magnify painful thoughts leading to feelings of helplessness, and may cause or prolong avoidance behaviors. 11 Pain intensity and pain interference explain how pain restricts general activity, walking ability, and enjoyment of life. An apprehension about activity and walking may take root during recovery from surgery due to the pain and physical deconditioning that occurs during this time. As a result, persons with lower-limb amputation are at risk of developing avoidance behaviors when there is a presence of a high level of pain catastrophizing. These thoughts and feelings can then lead to greater pain, depression, and disability. Furthermore, physical and muscular deconditioning may lead to a decrease in balance, an increased risk of falls, and depression, which subsequently increases avoidance behaviors and perpetuates the process.11–17
Mobility apprehension is an avoidance behavior that has not yet been explored in persons with lower-limb amputation. Measurement of mobility apprehension and related health outcomes will provide data to aid in the development of rehabilitation models for persons with lower-limb amputation. Therefore, the purpose of this study was to determine whether avoidance behaviors are present in persons with lower-limb amputation and to identify factors that may lead to mobility apprehension. The hypothesis was that pain catastrophizing, pain intensity, and pain interference would be directly associated with mobility apprehension.
Methods
Participants
The University of Alabama in Huntsville’s ethics board, the Institutional Review Board, approved procedures prior to data collection (application number: E2016107), and participants signed an informed consent document. To ensure all participants had a major lower-limb amputation, recruitment occurred in-person rather than online. Participants were recruited from the 2017 Amputee Coalition National Conference (3–5 August 2017; Louisville, KY). Research assistants recruited participants by word-of-mouth, posters, and flyers presented at a booth in the exhibition hall for the conference and were present to answer questions about the questionnaire and self-report instruments. Specific inclusion criteria were (1) age older than 18 years, (2) ability to read and speak English, (3) an acquired amputation at or above the ankle in one or both limbs.
Procedures
Eligible participants completed a questionnaire consisting of demographic questions and self-report instruments. All assessments were provided in English language only. Demographic data recorded included age, sex, race, education, number of years since amputation, amputation etiology, use of an assistive device and/or a prosthetic limb(s), employment history, comorbidities, current medications, presence of chronic pain, and location of pain. Participants were allowed to choose to complete questionnaires using paper surveys or with an Online Survey Software (Qualtrics, Provo, UT) survey loaded onto an iPad (Apple, Cupertino, CA). Data entered into the Online Survey Software on the iPad were directly recorded into a Qualtrics Database. Data collected on paper surveys were entered by a single research assistant into the Qualtrics database and verified by a second research assistant. Self-report instrument data included questionnaires used to measure mobility apprehension and indices of pain.
Mobility apprehension
To measure mobility apprehension, participants were asked to complete the Tampa Scale for Kinesiophobia (TSK). 18 The TSK is a 17-item instrument that uses a 4-point Likert-type scale, with scoring options ranging from 1 as “strongly disagree” to 4 as “strongly agree.” A score of 39 or above is used to differentiate those with a high level of mobility apprehension. The TSK has been found to be a reliable index of fear of movement and has good internal consistency (Cronbach’s alpha > 0.70) and test–retest reliability (Pearson’s r > 0.70) in persons with chronic pain.19–21 Reliability of the TSK has not been reported in a sample of persons with lower-limb amputation. Thus, the TSK was analyzed for internal consistency, or the consistency that a participant’s responses agree across items within the questionnaire. A split-half correlation measure revealed a Spearman–Brown coefficient of +0.80 (p < 0.01), representing a high level of internal consistency of items in the questionnaire.
Pain
The Brief Pain Inventory (BPI) was administered to measure pain. 22 This questionnaire has two subscales, pain intensity and pain interference with activities of daily living, physical and psychosocial health. Both pain intensity and interference are assessed with 0–10 numeric scales. For example, “0” represents no pain or no interference and “10” represents severe pain or pain that completely interferes. Participants were also asked to rate their worst, least, and average pain over the last week, along with present pain. Participants rated the degree to which pain interferes with the following seven areas of daily life: general activity, mood, walking, work, relations with others, sleep, and enjoyment of life. The BPI is reliable in different disease states and in persons with low-back pain. It is highly correlated with the Short Form-36 (SF-36), the Roland Disability Questionnaire, the McGill Pain Questionnaire, and the Visual Analog Scale (VAS) for pain in both surgical patients and patients with chronic low-back pain.22,23 Validity and reliability of the BPI for persons with lower-limb amputation have not been published.
The Pain Catastrophizing Scale (PCS) rates the frequency with which participants experienced 13 different thoughts and feelings related to pain and catastrophic thinking associated with pain. 24 Respondents rate statements on a 5-point scale with the endpoints “0” representing “not at all” and “4” representing “all the time.” Example statements are “I’m afraid that I might injure myself if I exercise”; “My body is telling me I have something dangerously wrong”; and “I am afraid that I might injure myself accidently.” The instrument provides three subscale scores assessing rumination, magnification, and helplessness. Those with a score greater than 24 are classified as “catastrophizers.” The PCS has been determined to be a reliable (Cronbach’s alpha = 0.87) measurement of catastrophizing in persons with low-back pain, 24 but reliability has not yet been assessed in persons with lower-limb amputation.
Fall and fear of falling
Participants who were administered the online survey were asked several additional questions about fall status (i.e. history of falls) and fear of falling using an approach similar to previously recorded methods. 25 As with prior studies, a fall was defined to participants as “falling to the floor unintentionally.” To determine fall status, participants were asked to answer the yes/no question “Have you fallen in the past 12 months?” Similarly, fear of falling was quantified by asking participants “Are you afraid of falling?” These questions were inadvertently not included in the paper survey. Responses were recorded at the same time as other study data were collected.
Data analyses
Descriptive statistics were determined to present mean (M) and standard deviations (SDs) for all measures. A multivariable linear regression model was used to determine whether any of the indices of pain (intensity, interference, or catastrophizing) were related to mobility apprehension. Stata (StataCorp LLC, College Station, TX) statistical analysis software, version 14, was used to analyze data. Significance level was set at an alpha of 0.05.
Results
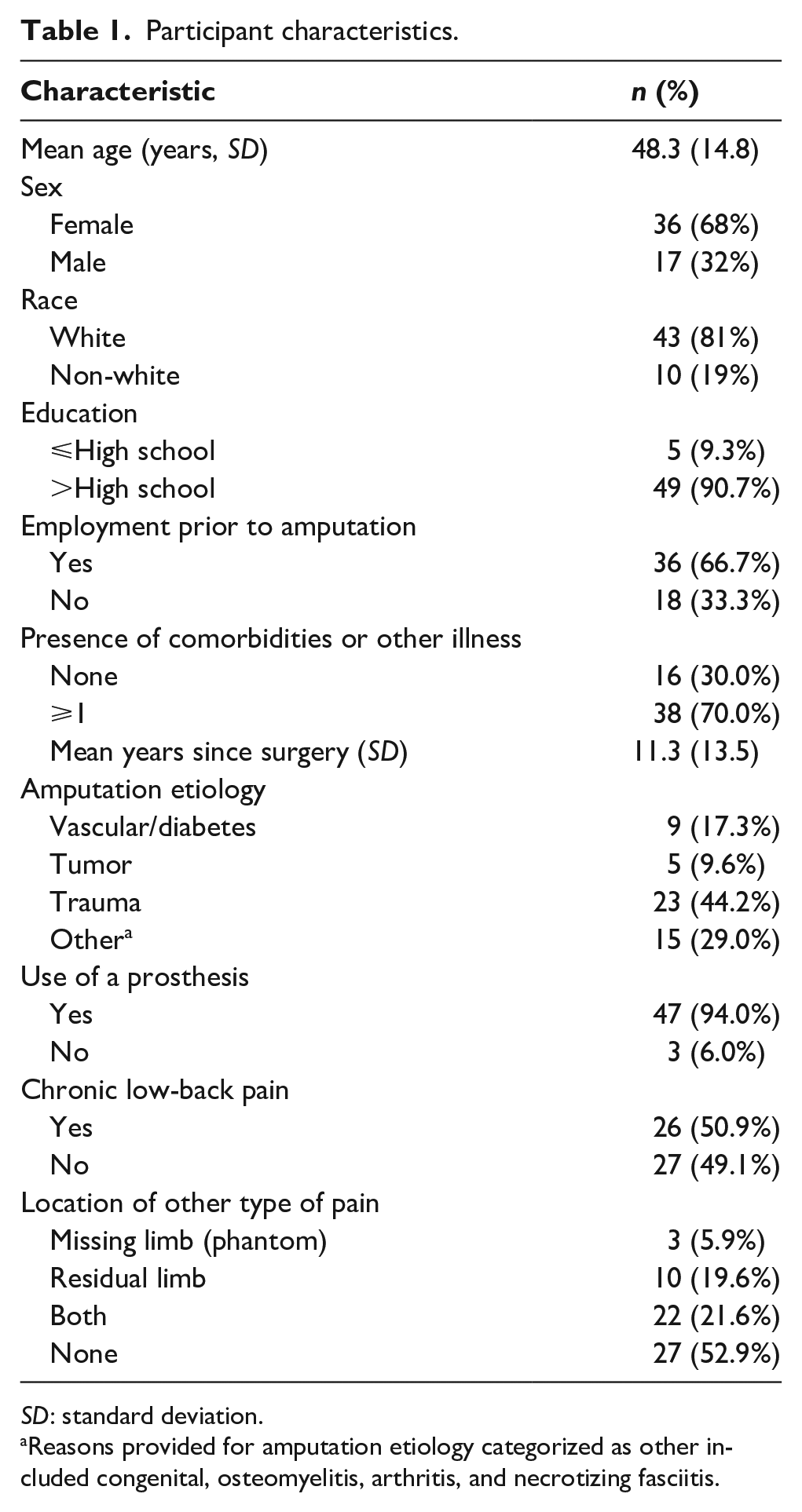
A total of 53 persons who had undergone major lower-limb amputation were enrolled in the study; a total of 40 participants provided answers to all questions and were included in the analyses. The mean (SD) participant age was 48.3 (14.8) years. Participants reported a mean of 11.3 (13.5) years since surgery for amputation. Of the participants, 47 (94%) reported regular use of a prosthetic limb(s); 15 (28%) participants described the amputation as unilateral transfemoral (above knee (AK)); 32 (60%) participants described the amputation as unilateral transtibial (below knee (BK)); and 6 (12%) reported having a bilateral amputation (either AK/AK, BK/BK, or AK/BK). Assistive devices were used by 22 (40.7%) participants (Table 1).
Participant characteristics.
SD: standard deviation.
Reasons provided for amputation etiology categorized as other included congenital, osteomyelitis, arthritis, and necrotizing fasciitis.
The current study sample consisted of predominantly female (68%) participants with most reporting more than a high school level of education (91%). At least 70% reported having comorbidities of high blood pressure and diabetes with heart disease being the most prevalent. Non-smokers were most prevalent (67%), and 31% reported taking medication for a psychological condition such as depression or anxiety. Less than 10% of the study population reported taking narcotic medication for pain even though 47% of the study sample reported having either phantom limb pain, residual limb pain, or both.
Participants’ mean mobility apprehension, as measured by the TSK, was 34.2 (SD = 6.0). The range of the TSK score reported by participants was 21–45 (Table 2). There were no significant relationships between demographic (age, sex, race, education, employment) or health state covariates (comorbidities, years since surgery, presence of back pain) and TSK score. There were no statistically significant differences in the mean TSK score between participants who reported having pain (M = 33.5, SD = 5.6) and those who reported no pain (M = 34.5, SD = 6.3), t = −0.51, p = 0.55.
Self-report instrument data.
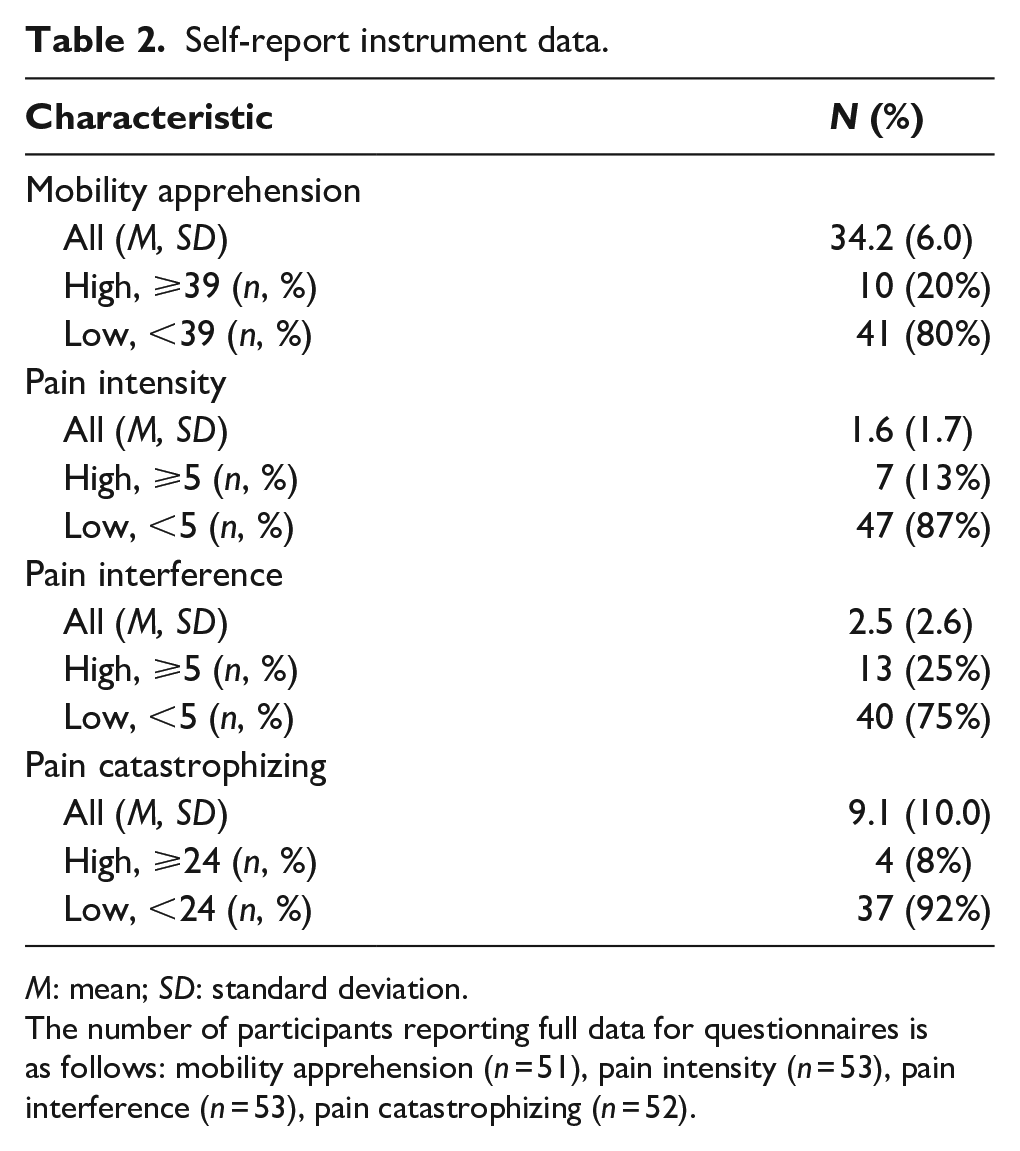
M: mean; SD: standard deviation.
The number of participants reporting full data for questionnaires is as follows: mobility apprehension (n = 51), pain intensity (n = 53), pain interference (n = 53), pain catastrophizing (n = 52).
A subset (n = 31) of participants were asked to report fall history and presence of a fear of falling. From this subset, 52% reported falling in the past 12 months and 29% reported a fear of falls. However, there was no relationship between fall history and those with a high (⩾39) versus low (<39) level of mobility apprehension (X2 = 0.3, p = 0.60).
With the regression analysis model, 32% of the variance in mobility apprehension can be explained by the variables in the model (pain intensity, pain interference, and pain catastrophizing). Pain catastrophizing was the only pain variable that was associated with higher mobility apprehension (B = 0.31, p < 0.001). Specifically, the regression results indicate that with every one-point increase in pain catastrophizing, mobility apprehension will increase by 3/10 of a point on the TSK scale (Table 3).
Regression analysis summary for factors associated with mobility apprehension.
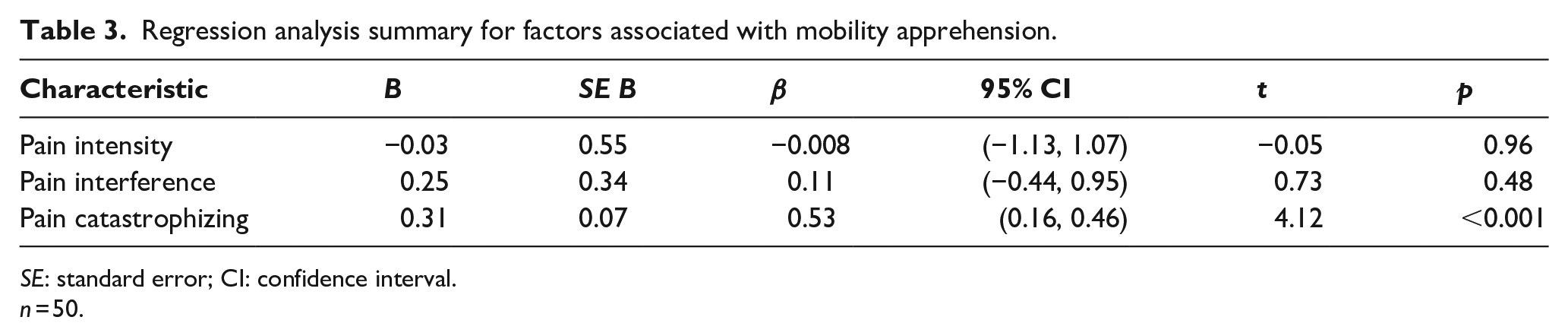
SE: standard error; CI: confidence interval.
n = 50.
Discussion
This study presents an initial attempt to determine whether fear-avoidance behaviors are present in people with major lower-limb amputation. The primary aim of the study was to determine whether pain-related factors, such as pain catastrophizing, pain intensity, or pain interference are associated with mobility apprehension. The findings indicate that persons reporting a higher level of pain catastrophizing were more likely to report a higher level of mobility apprehension. For this particular sample population of conference attendees, it was also found that 20% of participants reported a high level of mobility apprehension (TSK ⩾ 39). Furthermore, of the 31 respondents to the fall prevalence questions, 52% reported experiencing a fall within the last year and 29% reported fear of falling. This fall prevalence is similar to that reported in other studies.9,15,16
Demographics, including participants’ age, race, education level, and the amount of time of daily prosthesis use, in the present study are similar to a larger (n = 914) cross-sectional study of Amputee Coalition members contacted by mail and telephone. 26 The current study sample included individuals who were generally more distant from their amputation (i.e. 11 years in the current study compared to 4 years in the prior study). There was also a larger percentage of women in the current study relative to the prior study (i.e. 68% as compared to 40%). Finally, while both studies included a similar percentage of people with amputation due to trauma, the present study had a smaller percentage of people with amputation due to dysvascular disease or tumor (i.e. cancer). Prevalence of pain in the current study was also generally similar to that reported in the prior study. Reports of residual limb pain (64% in the current study vs 68% in the prior study) and back pain (51% in the current study vs 62% in the prior study) were relatively similar. However, a much lower percentage of participants in the current study (50%) reported phantom limb pain than in the prior study (80%). As such, the current sample may not be entirely generalizable to the population of people with lower-limb amputation.
Chronic pain is well known to limit physical function27–29 and employment. 30 In the current sample, moderate to severe pain intensity was reported in 13% of the participants, whereas moderate to severe levels of pain that interferes with daily activities, mood, sleep, and enjoyment of life was reported in 25% of the participants. Ephraim et al. 26 reported depressive symptoms to be a significant predictor of moderate to high levels of pain intensity located in the residual or intact limb. Others have reported a negative correlation between pain intensity and residual limb length (ρ = −0.92, p < 0.001) and usage of a prosthetic limb (ρ = −0.96, p < 0.001). 31
Pain catastrophizing is the tendency to ruminate and magnify painful thoughts and feelings leading to feelings of helplessness which can prolong tendencies to avoid physical activities. 24 These behaviors induce a fear of movement, or mobility apprehension. 12 Pain catastrophizing was associated with mobility apprehension in this sample of persons with lower-limb amputation. For persons with lower-limb amputation, pain catastrophizing may interrupt the patient’s post-amputation rehabilitation, return to normal activities of daily life, and induce mobility apprehension. As a result, persons with lower-limb amputation may be at risk for further development of avoidance behaviors, which can then lead to greater pain, depression, and disability. 12
High levels of pain will restrict functional activity and prevent an individual from returning to normal daily activities.6,8 The impact of mobility limitations, pain, and fall risk in persons with lower-limb amputation is profound.6,15 For example, limb loss has an impact on a person’s ability to become or stay employed. 8 Of the participants in this study who were not currently employed, 44% reported that unemployment was due to their current disability. This is similar to data reported by Sinha et al. 8 who outlined the need to address the impact of amputation on employability.
Informed clinical decision-making is a key factor for a successful practice. 32 This work demonstrates a potentially successful use of a questionnaire that could be used as a screening tool for assisting clinicians in identifying and measuring patients’ fear-avoidance behaviors after lower-limb amputation surgery. Once recognized, cognitive-behavioral strategies may compliment rehabilitation to improve recovery. 6 However, these data also indicate that a similar trial with a larger sample is warranted to verify whether these noted associations are present among the larger population of people with major lower-limb amputation. Future study protocols may benefit from including potential confounders, such as age, amputation etiology, comorbidities, depression, and quality of life, to provide a more in-depth understanding of the reasons one may experience mobility apprehension.14,26,27 Examination of pain catastrophizing in persons having degenerative lumbar spine conditions, a population known for experiencing musculoskeletal pain and severe nerve pain, has led to two main findings.12,13 First, early postoperative identification of persons with a high level of pain catastrophizing has been shown to predict health outcomes as late as 6 months post-surgery. Second, cognitive-behavioral strategies combined with physical therapy have also been a noteworthy method for improving health outcomes following surgery. 14 Translating these methods to persons with lower-limb amputation may also yield positive results.
Limitations
Several limitations to this study are present. First, the convenience sample made up of prosthesis users who are relatively young is not fully representative of the general amputee population. Therefore, the results of this study may only apply to a subset of individuals who are prosthesis users. Similarly, one may assume that because these individuals traveled to a national conference, they are more active compared to the general population of persons having surgery for a major lower-limb amputation. Within this sample, less than 10% of the participants reported having severe pain. Although the TSK has a high level of internal consistency (+0.80) for this sample, further study of the reliability and validity of the self-report instruments included in our questionnaire (i.e. TSK, BPI, and PCS) among people with major lower-limb amputation is needed to verify the results presented here.
Conclusion
This work demonstrates that identification of the tendency for pain catastrophizing may be valuable to help patients overcome mobility apprehension and break the fear-avoidance cycle. By further understanding the relationship between pain catastrophizing and mobility apprehension, clinicians may explore the idea of treating psychological factors when developing models for physical rehabilitation.
Footnotes
Acknowledgements
The authors are grateful to Caitlin E. Lindquist and Victoria R. Blakely for collecting data at the Amputee Coalition Conference. The authors appreciate their hard work.
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Alabama in Huntsville New Faculty Research award (grant number: 2017-817; NFRFY18Mathis).