
Abstract
Background:
Foot orthoses have been applied for the management of lower limb disorders, mainly for those who develop foot pain. The Central Stabilizer Element (CSE) is a new element that contains the midfoot laterally when a plantar insole is manufactured.
Objectives:
To determine the effect on foot pain of adding the Central Stabilizer Element during the manufacturing process of foot orthosis, and to describe the proportions of Central Stabilizer Element in terms of width and length of this element.
Study design:
A clinical study.
Methods:
A sample comprising 130 patients (57 males and 73 females) with foot pain was recruited for this study, with the patients having supinated, neutral, pronated and overpronated feet. All the patients received a custom-made foot orthosis with the Central Stabilizer Element. The Central Stabilizer Element was made of resins of polyvinyl chloride, and is a device insert in foot orthosis that contains the midfoot laterally to control pronation and supination movements. Perceived patient’s foot pain was collected using a Visual Analog Scale at baseline, 15, 60 and 90 days after treatment.
Results:
A statistically significant decrease was found after foot orthosis application at all times in all foot types. There was a statistically significant correlation between all the ratio proportions according to foot posture (Foot Posture Index scores), except for heel length proportion.
Conclusions:
The Central Stabilizer Element, applied at midfoot level of a custom-made foot orthoses through a directly mould technique, can reduce foot pain, when a previous foot posture status is considered.
Clinical relevance
The Central Stabilizer Element can be of interest for those professionals who are involved in the manufacturing process of foot orthosis, throughout the control of an excesive pronated or a supinated foot condition that is provoking foot pain.
Background
Foot orthoses are frequently prescribed for the treatment of lower limb pathologies, especially for treating plantar pain and pronation control,1–3 and although it is not very well known, the mechanisms by which plantar supports act help to reduce symptoms.
Since 1947, when the Whitman-type 4 insole was patented, considerable progress has been made in the development of new materials5–7 and manufacturing methods8,9 meaning that today we have a wide range of foot orthoses and techniques used in the field of foot orthopaedics.
For therapeutic effect, even though the material is considered a very important issue when a foot orthosis is designed, it is crucial to take the wedging into account. In this sense, there are several elements described by different authors that could be used in orthopaedic settings to achieve the insole’s desired effect. Some of them use the lifting of planes, 10 the inclination of planes, 11 the lifting of the internal longitudinal arch 12 and the control of rear-foot pronation. 13
There have been limited studies on the elements that cover laterally the plantar surface, as part of the wedging process, that is, lateral contentions, that can generate a shift in foot posture. Ankle foot orthosis (AFO)14,15 has been traditionally used to treat foot drop, and ankle support bandages have been used for the treatment of excessive rear-foot pronation.16,17 However, the evidence of studies investigating hard thermoplastic materials that embrace the plantar surface laterally is even more scarce. 18
The Central Stabilizer Element (CSE) is an element that contains the midfoot laterally in order to control pronation and supination, when a plantar insole is manufactured. The CSE has been used in clinical setting, but this element has not been very well documented. If we could find any positive effect of CSE in relieving foot pain when a plantar insole is designed, we could contribute to increasing the knowledge in this area, and it could be an alternative to traditional plantar foot treatments.
Hence, the aim of this study is twofold: first, to determine the effect on foot pain of adding the CSE in the manufacturing process of plantar insoles and second, to describe the proportions of CSE in terms of width and length of this element.
Methods
Study design
A sample comprising 130 patients (57 males and 73 females), who required podiatric care services due to foot pain at Faculty of Health Sciences, University of Malaga and two private clinics, was recruited for this study. The inclusion criteria were as follows: (a) patients suffering from foot pain above 5 in Visual Analog Scale (VAS) for pain and (b) patients from 18 to 65 years of age. The exclusion criteria were as follows: (a) any previous foot surgery and (b) diabetic ulcers in plantar sole. Sample characteristics are shown in Table 1.
Sample anthropometric data.
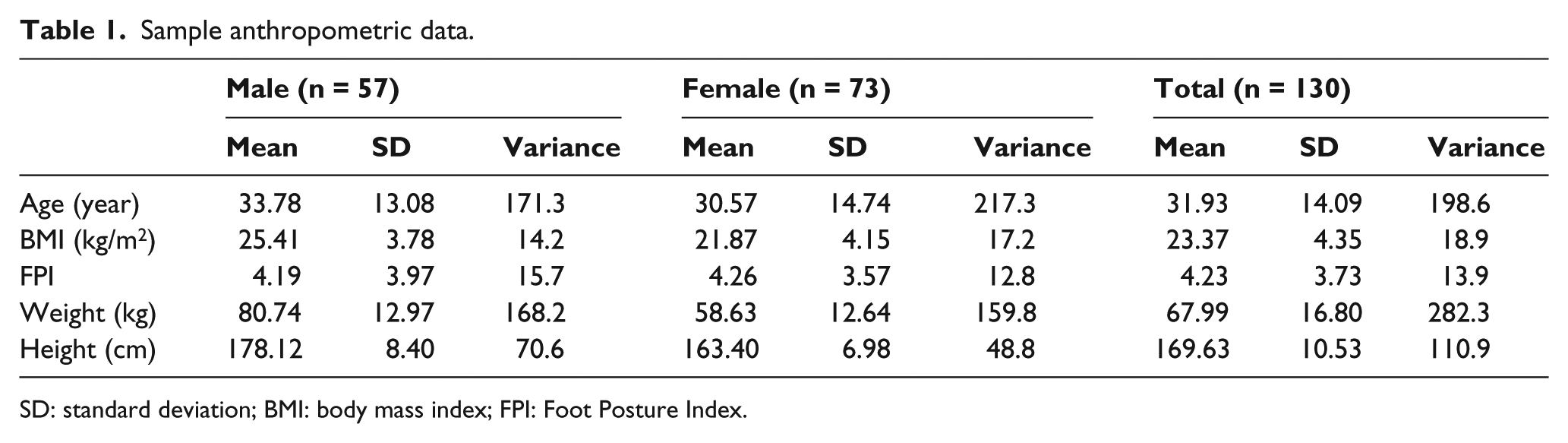
SD: standard deviation; BMI: body mass index; FPI: Foot Posture Index.
The study protocol was in accordance with standard ethical and human research principles. Written informed consent for participation and publication was given of each patient, including the publication of photographs. The study was approved by the Research Ethics Committee of the Faculty of Health Sciences, University of Malaga.
Procedure
Outcome measures
Perceived foot pain reported by subjects was collected using a VAS for pain at baseline and at 15, 30 and 90 days after treatment. VAS measurements have been traditionally used for measuring foot pain when a custom-made foot orthosis has been applied.19–21
The foot posture was determined using the Foot Posture Index (FPI). 22 The FPI evaluates the multi-segmental nature of foot posture in all three planes and does not require the use of specialised equipment. Each item of the FPI is scored between −2 and +2, to give a sum total between −12 (highly supinated) and +12 (highly pronated). Items include talar head palpation, curves above and below the lateral malleoli, calcaneal angle, talonavicular bulge, medial longitudinal arch and forefoot to rear foot alignment. The FPI measurements were collected at baseline in order to classify feet into supinated (−12 to −1), neutral (0 to +5), pronated (+6 to +8) and overpronated (+9 to +12). 23
Once the patient met the inclusion criteria, the outcome measurements were collected at baseline by a blind assessor who did not know the purposes of the study, and the plantar insole was made by three experimented podiatrists (G.G.N., M.G.N. and E.C.J.). Patients received recommendation of wearing the plantar insole the maximum amount of time per day. While wearing the insole, VAS measurement was taken at 15, 30 and 90 days after the beginning of the study.
Intervention
A technique of directly mould orthoses (DMOs) to the non-load-bearing foot by vacuum forming was utilised in the custom-made foot orthosis manufacturing process to apply CSE. This direct technique has been used in the past in the management of Sever’s disease 18 with good results.
The CSE constitutes the central part of the plantar insole. It is applied on plantar sole, from Chopart joint up to metatarsal heads (not included), while embracing midfoot structures laterally (Figure 1). This element is designed within the foot orthosis in order to synchronise the dynamic helicoidal movement of the midfoot, 24 regulate the eversion–inversion movements, control the Hendrix torsion bar, 25 stop proprioceptive stress, 26 and therefore increase stability and maintain the physiological position of the midfoot structures, even acting at a muscular level, balancing the action of the tibialis posterior muscle and the peroneus longus tendon and releasing tensions in the plantar fascia. 27

Drawing and model of the central stabiliser element.
This element may be cut out of different flexible materials such as polyvinyl chloride (PVC) resins or ethylene vinyl acetate (EVA), adapted to moulds 28 or directly on the foot. 18 In our study, the CSE was made of resins of PVC. This element must be combined with a cover that enables it to be inserted into the shoe.
Design of CSE
To manufacture the CSE, first the outline of the patient’s foot is drawn on paper in a stand-up position, and points of reference are marked. These points are as follows: the posterior area of the first and second metatarsophalangeal joint, and the talonavicular joint. Afterward, the metatarsal line is drawn.
Depending on FPI-scores and hence, the foot type, an outer edge that starts at the beginning of the heel and follows the plantar sole outline in a parallel manner is drawn up to the fifth metatarsal head, and using the same process, an inner edge making an ascending curve, matching the talonavicular joint reference. At this point, the line drawn on the paper mould descends in a ‘toboggan’ manner heading to the first metatarsal head. The internal edge has a shape similar to a hill for feet in a neutral or supinated position and a Gauss bell for pronated feet (Figure 2).

Central stabiliser element applied to the foot orthosis.
Once the mould on paper is finished, the whole foot insole is cut based on this measurement, and applied to the patients’ feet using the DMO technique. Plantar insoles were worn in both feet for the patients in their most usual footwear during 90 consecutive days. In case of any discomfort, patients had the option of contacting the research team.
CSE proportions
All the plantar insoles were analysed in order to calculate the proportions of width and length. A blind assessor to this study collected the following distances, using a software (AutoCAD system 2009 Autodesk Inc, San Rafael, CA): (a) longitudinal line (foot midline), from the heel to the second toe; (b) transversal line 1, from first to fifth metatarsal head; (c) transversal line 2, from talonavicular joint to the outer point in the external edge; and (d) transversal line 3, understood as the diameter of a circumference drawn on the heel (Figure 3).
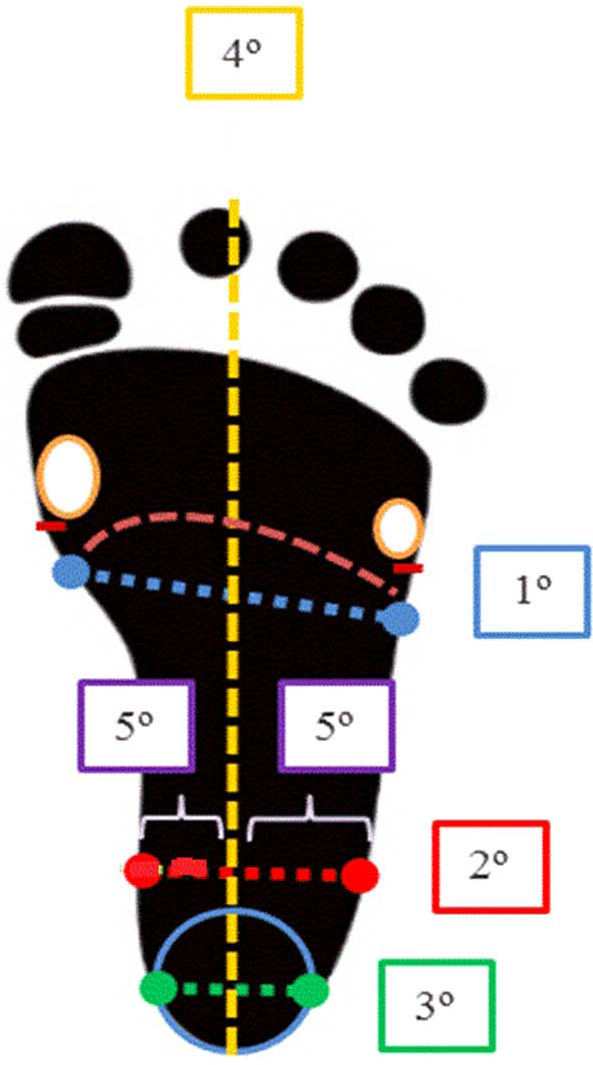
Diagram of measurement of lines for to make of proportion – 1: transversal line 1; 2: transversal line 2; 3: transversal line 3; 4: longitudinal line; 5: internal/external lines.
These new four measurements originated six new variables to describe the standard proportions when the CSE is designed to be applied on plantar insoles:
Forefoot length/width proportion (FLP) (longitudinal line/transversal line 1);
Midfoot length/width proportion (MLP) (longitudinal line/transversal line 2);
Heel length/width proportion(HLP) (longitudinal line/transversal line 3);
Midfoot/heel width proportion (MHP) (transversal line 2/transversal line 3);
Midfoot/forefoot width proportion (MFP) (transversal line 2/transversal line 1).
The last variable was created, internal–external edge proportion (IEP). To that, a line from the crossing point between longitudinal and transversal line 2, to the talonavicular joint (internal) or its equivalent in the external edge (external) were determined.
Statistical analysis
Data were analysed with the IBM SPSS19® (SPSS Science, Chicago, IL). A p < 0.05 was considered to be statistically significant. Data were tested for normality using the Kolmogorov–Smirnov test, and all data were normally distributed. All the variables (pain and different proportions) were grouped in accordance with the FPI categories (supinated, neutral, pronated and overpronated feet), producing a descriptive analysis using the mean, standard deviation (SD) and variance.
The Pearson coefficient was used for correlations between FPI measurements and proportions. And analysis of variance (ANOVA) test with Bonferroni test was used to analyse differences of means according to foot types. A two-point decrease in VAS-score was considered as minimally clinical change.
Results
The sample was composed of 130 patients (57 males and 73 females) with foot-related pathologies generating foot pain. The characteristics of the sample are shown in Table 1. Table 2 shows the patient foot pain perceived, measured by VAS. A decrease statistically significant, and clinically significant, was found after plantar insole application at all times (15, 60 and 90 days) in all foot types (supinated, neutral, pronated and overpronated foot).
VAS values for foot pain in patients with supinated feet, neutral feet, pronated feet and overpronated feet.
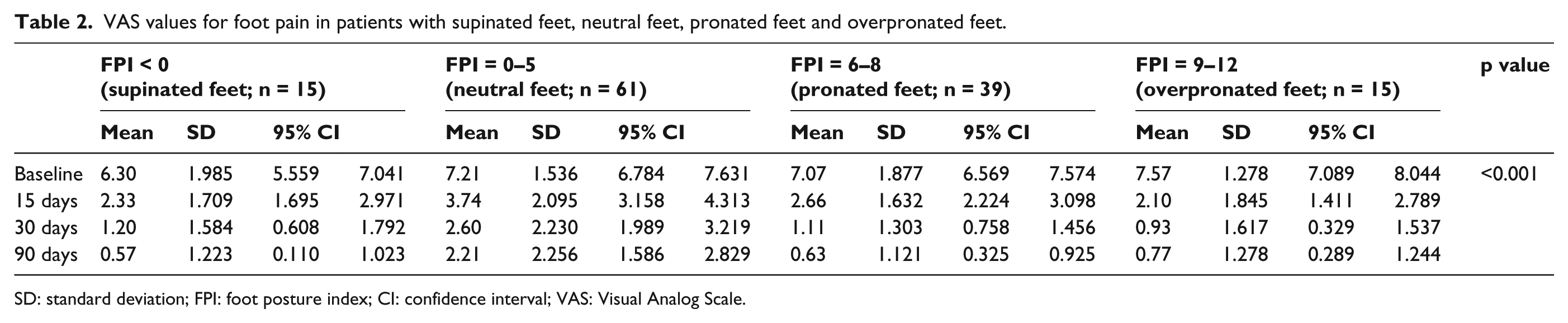
SD: standard deviation; FPI: foot posture index; CI: confidence interval; VAS: Visual Analog Scale.
The ratio for the proportions used to create the CSE in accordance to the patient’s foot type is shown in Table 3. There was a statistically significant correlation between all the ratio proportions according to foot posture (FPI-scores), excepted for HLP (Table 4).
Ratio proportions for the CSE.
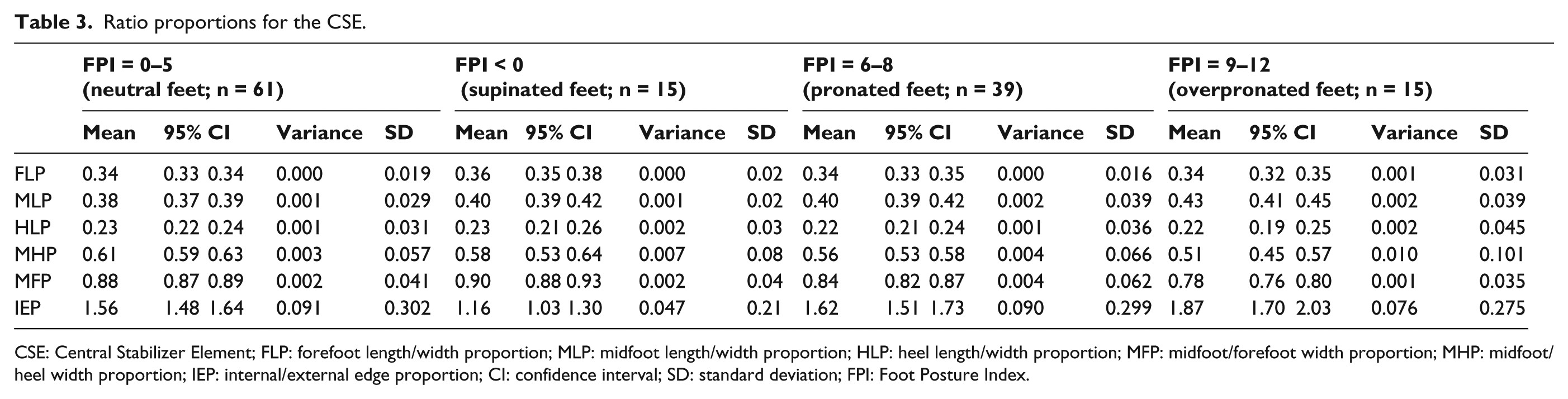
CSE: Central Stabilizer Element; FLP: forefoot length/width proportion; MLP: midfoot length/width proportion; HLP: heel length/width proportion; MFP: midfoot/forefoot width proportion; MHP: midfoot/heel width proportion; IEP: internal/external edge proportion; CI: confidence interval; SD: standard deviation; FPI: Foot Posture Index.
Correlations between ratio proportions and foot type.
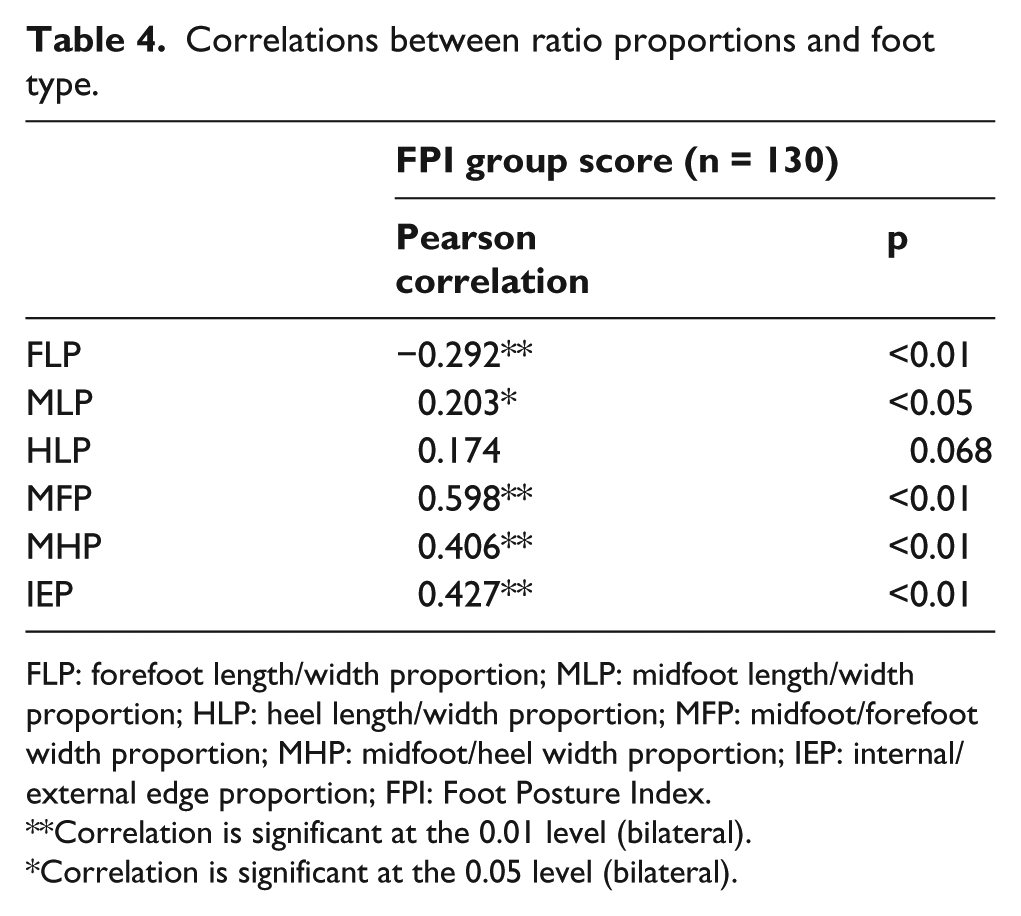
FLP: forefoot length/width proportion; MLP: midfoot length/width proportion; HLP: heel length/width proportion; MFP: midfoot/forefoot width proportion; MHP: midfoot/heel width proportion; IEP: internal/external edge proportion; FPI: Foot Posture Index.
Correlation is significant at the 0.01 level (bilateral).
Correlation is significant at the 0.05 level (bilateral).
Discussion
The first aim of this study was to analyse the effect on foot pain of the CSE in patients suffering from foot pain due to different conditions. Our results suggest that using the CSE as a part of a custom-made plantar insole, manufactured by a technique of DMOs to the non-load-bearing foot by vacuum forming, and considering an external or internal wedging based on previous status of foot posture, a significant decrease of foot pain can be achieved.
From the wide range of variety of interventions for the management of foot pain, custom-made orthosis are one of the options available for clinicians, defined as contoured, removable in-shoe devices that are moulded or milled from an impression of the foot and fabricated according to practitioner-prescribed specifications. Some studies in the past have concluded in the same direction of our study. Custom-made foot orthosis decreased foot pain in several studies.29–31 Nevertheless, other studies did not find any positive effect in reducing foot pain after custom-made foot orthosis applications in comparison with sham applications.19,31,32
To our knowledge, this is the first study investigating the ratio proportions of CSE in custom-made plantar insoles, in terms of width and length, when a decrease in foot pain is desired. In our study, we have defined six new measurements (ratio proportions) to be taken into account when a clinician is seeking to manufacturing a custom-made orthosis to control a supinated or pronated foot posture.
The main strength of our study is the methodological rigour. We attained a follow-up of 100% of study patients, outcome measure was collected up to 90 days after intervention and there was blinding of the assessor and statistician. However, there are some limitations that should be taken into account. First, a placebo group was not used in the study, so we cannot conclude whether the decrease in foot pain achieved after plantar insole application could be attributable to the intervention or not. Other similar studies investigating the effect of custom-made foot orthoses and a release in foot pain in different conditions19,29,31 have used a control group in their studies, so we cannot conclude strongly in this sense. Furthermore, our intervention was based on the realignment of a previous condition of pronated, overpronated or supinated foot posture (not in neutral foot) using a wedging in the internal or external edge of plantar insole, midfoot level (CSE). However, we cannot ascertain whether a realignment in foot posture was attained or not, because of the absence of biomechanical measurements that assured it. Last, heterogeneity of foot pain patient conditions meeting the inclusion criteria, and the fact that the usual patient’s footwear 33 was not considered in our analysis, could have generated bias.
Due to the absence of biomechanical measurements in the assessment of foot posture correction in the present study, we can only speculate about the mechanisms why foot pain was decreased after plantar insole intervention. A redistribution of plantar pressures and a reduction in the amount and speed of the pronation or supination movements could occur,3,34 and hence, a decrease in the patient’s foot pain can be perceived.
In future studies, a biomechanical analysis of the effects of wedging using CSE on foot pain would be of interest. Also, the application of CSE concept in custom-made foot orthosis in specific conditions such as plantar fasciitis or diabetic foot pain could help to understand if this new method could be useful. Until then, the results of this study should be taken with caution for clinicians.
Conclusions
The CSE, applied at midfoot level of a custom-made foot orthoses through a directly mould technique, can reduce foot pain, when a previous foot posture status is considered.
Footnotes
Acknowledgements
To Adelina Dorca Coll who, together with a group of professors in foot orthopaedics at the University of Barcelona, developed this element and gave the authors the adequate training to the clinical practice.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.