
Abstract
The Adaptive® knee joint is a microprocessor-controlled prosthetic knee that incorporates both pneumatic and hydraulic control in one electronic unit. Pneumatic control is said to provide control during swing phase and the hydraulic control during the stance phase of the gait. This hybrid controller is triggered by a computer contained within the knee that responds to input from force, time and angle sensors. The microprocessor then selects an appropriate speed and stability setting. The Catech® knee joint is a conventional hydraulic knee joint. The aim of this study was to compare the Adaptive® and Catech® knee joints in established trans-femoral amputees. The patients meeting the inclusion criteria were all established trans-femoral amputees using the Catech® knee joint. The study was carried out by performing gait analysis, assessing energy requirements using the Physiological Cost Index (PCI) and using questionnaires. There was no significant benefit gained from the use of the Adaptive® knee over the Catech® knee joint in our small study group.
Introduction
The knee joint is approximated as a hinge joint allowing flexion and extension in the sagittal plane. The prosthetic knee joint aims to reproduce this movement whilst allowing for variability in stability to take into account the patient's disability. During the stance phase of the gait cycle the prosthetic knee joint must be stable to support the weight of the amputee and during the swing phase the knee joint must flex sufficiently to allow the leg to swing through without touching the ground but must be in extension by the end of the swing phase to allow stability at initial contact.
Prosthetic knee joints are currently broadly described as mechanical or microprocessor controlled knees. Hydraulic dampers are commonly used in mechanical knees to achieve variable cadence control to allow the amputee to walk at a wide range of speeds, usually for active amputees with powerful stumps. Non-microprocessor controlled pneumatic swing phase control only allows swing at a speed decided during fitting. A slower or faster walking speed can then only be achieved by unacceptable gait deviation.
The microprocessor controlled prosthetic knee unit was initially marketed by Chas A Blatchford and Sons in the UK as the Intelligent Prosthesis® (IP) in 1993 (Buckley et al. 1997) in which a microprocessor adjusted the swing phase damping of the pneumatic cylinder.
The Adaptive® knee (Chas A. Blatchford & Sons Ltd, UK) is a second-generation microprocessor-controlled knee that incorporates both pneumatic and hydraulic control in one electronic knee unit. The pneumatic control is said to provide control during the swing phase and the hydraulic control during the stance phase of the gait. This hybrid controller is triggered by a computer contained within the knee that responds to input from force, time and angle sensors. The microprocessor then selects an appropriate speed and stability setting. The microprocessor has a 5-speed cadence control, stancerest (limb stabilizes when limb wearer comes to rest) and stumble control (to provide immediate stability to prevent a fall), ramp and stair settings.
There have been several studies into the benefits or otherwise of the intelligent knee (Buckley et al. 1997; Datta and Howitt 1998; Heller et al. 2000; Datta et al. 2005). However, there is no independent evaluation available in peer-reviewed journals regarding the Adaptive® knee. This study aimed to assess the function of the Adaptive® knee joint compared to the Catech® Knee by comparing the gait characteristics, energy requirements and the patients' perceptions and daily functional activities in order that the benefits and deficits of this complex and expensive prosthesis may become clearer.
Materials and methods
Subjects
Inclusion criteria (established unilateral trans-femoral amputee using an Endolite prosthetic system with a hydraulic Catech® knee joint, established limb user, medically fit to undergo the length of walking necessary to complete tests and able to give informed consent) and exclusion criteria (specific stump problems, other temporary disability which affected gait, medically unfit, significant cognitive problems, awaiting resolution of compensation claims) were met by 5 patients (mean age 41.2 (28.8 – 55.7) years).
All the patients were seen in clinic by the same consultant physician and prosthetist, they were provided with an information sheet and informed consent was obtained followed by a thorough check of the patients existing limb, socket fit, alignment and a mechanical inspection. If no problems were identified a cast of the socket was taken to produce a duplicate socket for a new prosthesis incorporating the Adaptive® knee joint. If modifications were made then an appointment was made 4 weeks later to allow the patient to become accustomed to the changes.
A programme of four physiotherapy sessions was arranged for all the patients after delivery of the prosthesis with the Adaptive® knee.
Gait analysis
Gait analysis was performed using the Vicon 370® (Oxford Metrics Limited, Oxford, UK) 3 dimensional movement analysis system. This system optically tracks reflective markers placed on anatomical landmarks and calculates the kinematics of the lower limb joints in the mediolateral, anteroposterior and vertical directions.
A Kistler 9281C force plate was used for the measurement of kinetic data. The information
obtained from such systems is seen as the gold standard in movement analysis (Coutts 1999). The marker placement
protocol was that of Davis et al. (1991). A retro-reflective marker was placed on the side of the knee, aligned
with the observable knee joint axis. The width of the knee was measured; the Davis
protocol then placed the assumed knee-joint centre mid-way along the joint axis on the
artificial limb. To assess the variable walking speed capabilities of the Adaptive® knee
the test was carried out at the subject's preferred walking speed and at speeds 10% faster
and slower. The walking speed was regulated by a series of custom-built light emitting
diodes embedded into a plastic strip along the walkways in the gait lab that the patient
had to keep pace with. Gait analysis was performed after the recruitment using the Catech®
knee and then after 8 weeks following delivery of the Adaptive® knee joint, to allow
familiarization with the new knee joint. Spatial symmetry was calculated using the
Symmetry Index formula below, adapted from Sadeghi et al. (2000). The results are expressed as a percentage
with perfect symmetry being 0%. Negative values indicate that the prosthetic side has the
longer step length and positive values the non-prosthetic side (Herzog et al. 1989). 

Physiological cost index (Nene 1993)
A steady state physiological cost index (PCI) (Chin et al. 1999) was performed at the time of gait analysis. The PCI is calculated from the measurement of heart rate during a walk over a 25 m figure-of-8 course (Butler et al. 1984). The heart rate was measured using a Polar S610 heart rate monitor (Polar Ltd, Finland) whilst walking at 5 cadences. The cadences were imposed by a metronome starting with the slowest cadence and finishing with the fastest. Cadences were 80%, 90%, 100%, 110% and 120% of preferred cadence (as established from gait analysis). For each cadence the patient walked until their heart rate reached an approximately steady state for 3 min.
Amputee questionnaire
At the time of the study, the authors were aware of no validated questionnaires that was felt were appropriate to this study thus a questionnaire was created to test the perceptions, benefits and usage of the prosthetic knee joint by the subject. This consisted of 14 questions concerning walking ability on level ground, slopes, stairs, stumbling, falling, and the weight and comfort of prosthesis (see Appendix 1). Since carrying out this study there has been some development in this area (Heinemann et al. 2003).
Delivery of knee
The patients attended the Rehabilitation Centre over a 2-day period for the Adaptive® knee to be fitted and programmed by a research prosthetist from the manufacturer. An experienced Adaptive® knee joint user provided further advice and a further appointment was made two weeks after the initial delivery of the limb for any necessary readjustments.
Analysis of data
The kinetic data obtained from the gait analysis were normalized to the subject's body weight prior to analysis. The kinematic data were resampled using cubic spine interpolation so all trials had 50 samples. Paired Student t-tests were used to compare results for the original and the Adaptive® knee prosthesis in the same individual.
Survey
A survey was carried out after the completion of the study. The aim was to assess the personal views of the patients regarding the prosthesis, the study and the physiotherapy programme (Appendix 2).
Results
The mean age of the cohort was 41.2 (28.8 – 55.7) years. The mean time since amputation was 12.2 (0.8 – 35.68) years. The average weight was 88.0 (73.6 – 104.3) kg and the height was 1.803 (1.777 – 1.830) m.
The physiotherapy programme was not well attended with 3 patients only attending 1 session; 2 of whom stating that they did not require any further sessions; and 1 patient had a hardware problem in the second session and did not attend the third session. The other 2 patients attended 3 physiotherapy sessions but engaged in only 2 of them due to socket problems and fatigue. All patients felt that further physiotherapy would not have made any difference to the outcome of the study.
Six months following the conclusion of the trial only 2 of the cohort were still using the Adaptive® knee Joint and at present only one patient is using it (2 year post-study).
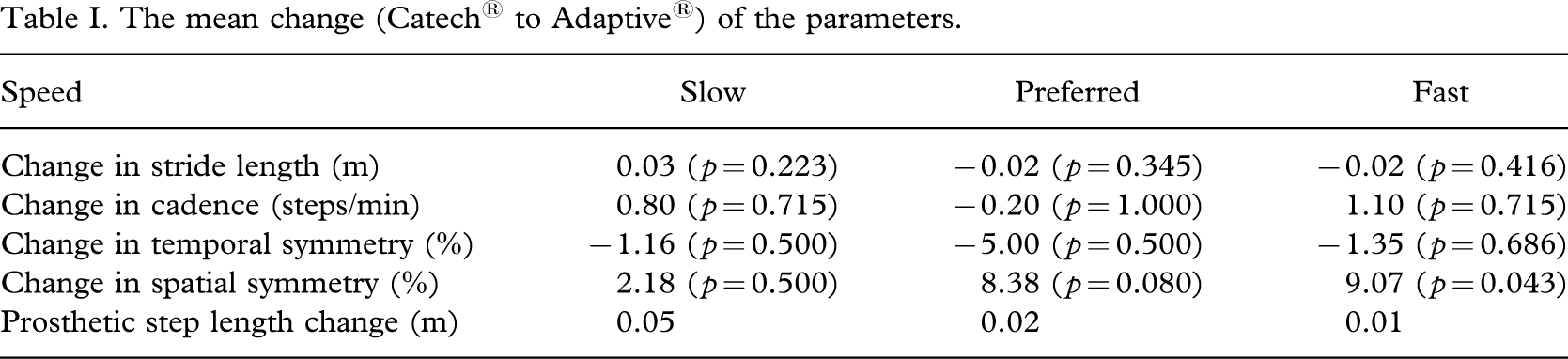
The gait analysis results demonstrated no significant changes; they are listed in Table I. Force data was collected, initial inspection showed no apparent differences between legs and it was not analysed further.
The mean change (Catech® to Adaptive®) of the parameters.
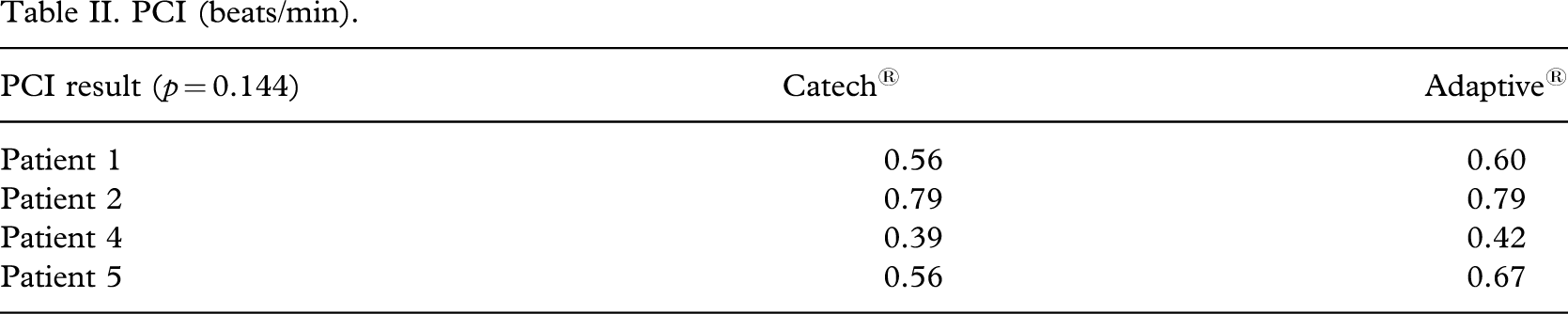
The PCI results were variable with one subject performing equally and the other three performing worse with the Catech® Knee Joint (Table II).
PCI (beats/min).
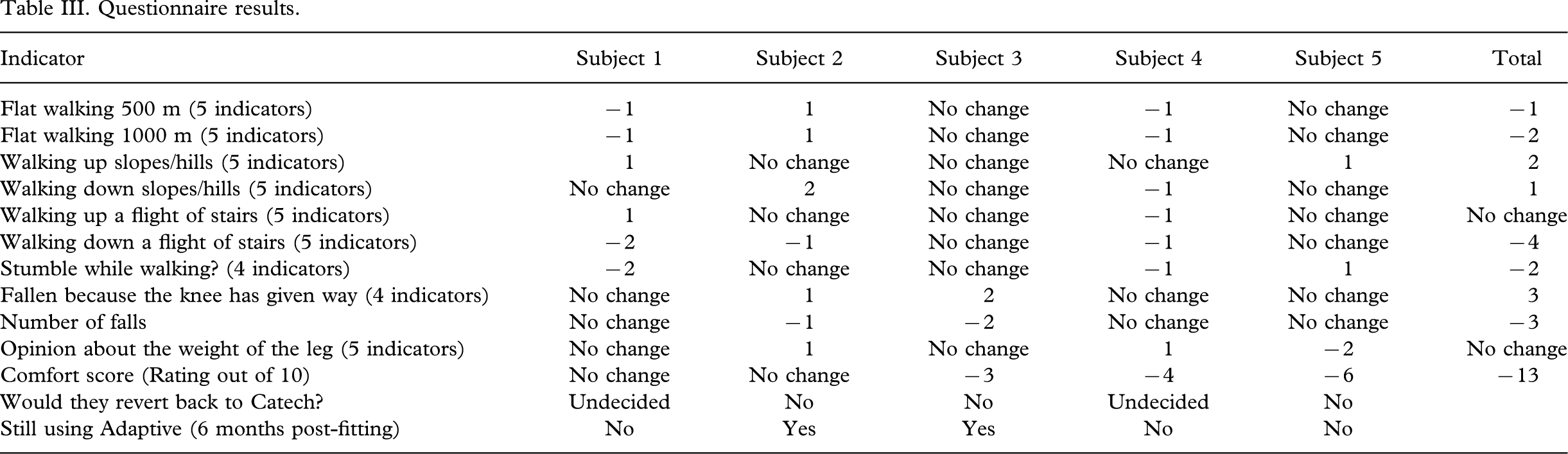
The results of the questionnaire demonstrated that overall three of the patients demonstrated significant worsening (1,4,5), one showed minimal change and one significant improvement (Table III).
Questionnaire results.
The second questionnaire demonstrated that all the patients were initially keen to use the Adaptive® knee however all but one were disappointed with it. Two out of four responders stated that the weight of the unit was a major reason for cessation of use of the Adaptive® knee. One patient stated they had difficulty with recharging the unit. Two of the responders felt they would have had improved results if they had been provided with the Adaptive® knee as their initial prosthesis rather than after a period of using an alternative prosthesis.
Discussion
The study was a pragmatic clinical trial. The aim of the study was to assess the benefits of the use of the Adaptive® knee for existing Catech® users. The adaptive knee concept is to maximize voluntary control of gait on different terrain. When programming the Adaptive® knee each situation (walking, standing, stairs, slopes or stumble recovery) is analysed and the appropriate level of assistance for that individual is programmed in. In theory after completion of programming when each situation is encountered the pre-determined level of assistance is automatically selected, enabling the wearer to negotiate the situation in a more controlled manner.
The Catech® knee was chosen for comparison as it is a hydraulic stance and swing phase control prosthetic knee that was felt would give rise to the best comparison (Pneumatic swing phase units with weight activated stance phase stabilization were excluded). One of the advantages of the Catech® knee is its reported ease of use with slopes and ramps, although this was not directly compared in this study.
Neither the gait analysis nor the PCI demonstrated improvement with the use of the Adaptive® knee. Possible explanations include: Mechanical faults (one unit failed due to mechanical problems, there were also problems with the higher level of maintenance required compared to the Catech® knee such as problems with recharging); and the ‘hassle’ factor, such as having to learn how to use a new prosthesis and undergo a physiotherapy program that none of the patients completed. In addition to learning how to use and maintain a new prosthetic component, all the patients had the Catech® first which might have influenced the outcome by this inherent order effect.
There are no formal psychometric tests available to assess the ability to learn and re-learn in the field of prosthetics. It is possible that established amputees may have a much greater difficulty, both physically and mentally in adjusting to different characteristics of a new knee unit. Though not proven, it may be possible that benefits offered by the Adaptive® knee could not be appreciated without a full and intensive gait-retraining program. It is interesting to note that the only amputee to continue using the Adaptive® knee is the most recent amputee and thus had used the Catech® knee for the shortest length of time.
Conclusion
Patient selection led to a varied group with a wide variety in age range (28.8 – 54.6 years), duration since amputation (0.8 – 35.7 years), ambulation duration (mean 12 years but 3 of the patients ambulating for less than 3 years).
In summary, there was no significant benefit gained from the use of the Adaptive® knee. There was some improvement in temporal symmetry and some worsening of spatial symmetry. All but one of the subjects performed worse with the Catech® in the PCI measurement but the changes were not statistically significant. Some previous papers (Buckley et al. 1997; Datta et al. 2005) found a slight benefit with the use of the IP as regards O2 consumption, whilst others (Orendurff et al. 2006) had similar results with most patients not demonstrating significant changes in oxygen cost (C-leg® compared to Mauch SNS®). PCI is a recognized research tool (Nene 1993) and whilst it is appreciated that it does not have the accuracy of O2 consumption it did allow our subjects to ambulate over ground rather than on a treadmill with the constraints of mask and gas collection/analysis equipment.
In this small group of established unilateral trans-femoral amputees no objective benefits were seen by substituting the Adaptive® knee unit for the Catech® knee joint. It is possible that as the amputees in this group were accustomed and satisfied to continue with their established Catech® knee joint, they might not have been prepared to put in the necessary physical and mental efforts to switch to a different knee unit. The additional weight of the knee unit and initial mechanical problems may have contributed to the rejection of the Adaptive® knee.
The authors also feel that the study group were generally happy with their existing prostheses and while agreeing to take part in this study they did not have any specific goals to achieve with the Adaptive® knee. Therefore adjusting to the new knee in terms of gait and movement characteristics, the additional weight of the knee unit and attending the physiotherapy sessions etc caused much disruption of their daily routine and lifestyle without any obvious advantages.
Whether the outcome would have led to improved rehabilitation if the patients had been provided with the Adaptive® knee from the beginning of their rehabilitation process, following their trans-femoral amputation, remains speculative.
The authors did not attempt to objectively measure any benefits regarding stumble control, slope walking or stair walking which are claimed to provide significant benefits by the manufacturers of the Adaptive® knee. It is not known whether the subjects actually had opportunities to test these aspects in their daily activities.
Since the research was completed, the manufacturers have now brought out a second generation of Adaptive® knee. The authors are informed by the manufacturer (personal communication) that the safe mode has been enhanced for training and use, a program wizard has been created making programming easier and simpler, the controls, cosmesis, cabling system and power system have been improved. However, so far no independent evaluation of this upgraded knee unit is available at the time of writing this paper.