
Abstract
Disarticulation of the thumb at the metacarpophalangeal joint level is not beneficial either aesthetically or functionally without additional surgery because it requires a bulky and an unacceptable prosthesis to be made for this amputation level. In this study, the authors have presented our experience of 12 metacarpal distractions in thumb amputated patients. Twelve male patients who had thumb amputation due to gunshot wounds were included in the study. Before the operation, aesthetic hand prostheses were made for 5 of the12 patients. Callus distraction was performed with the use of a mini Ilizarov type external fixator in 7 cases and uniplanar dynamic mini external fixator in 5 cases too. External fixators were removed after the completion of the radiographic consolidation. Five patients whose prosthesis had been made before the operation wore their prosthesis for an average 6.8 months (5 – 14) due to poor appearance and poor construction. Union of the lengthened segment was observed in all cases. Average lengthening was 28.9 mm (range from 25 – 37). Average healing time was 2.1 months (range from 1.8 – 2.5). Average healing index was 0.73 month/cm (range from 0.65 – 0.88). Pin tract infection was seen in 7 cases (58.3%). Volar angulation developed after removing the external fixator in 1 case. Webplasty was performed in all cases. Patients were evaluated by means of Disability of the Arm, Shoulder and Hand (DASH) score and pick-up test. It was concluded that the metacarpus lengthening by callus distraction technique may be a functionally and cosmetically effective reconstruction method for traumatic thumb amputations. It is believed that the possibility for a functionally and aesthetically acceptable fabrication of a thumb prosthesis, by providing a suction suspension with distraction and/or webplasty procedures.
Introduction
The power of the human hand depends on the length, strength, free lateral motion and perfect mobility of the thumb (Mansoor 1969). Thumb amputation thus causes a marked functional limitation of the hand, especially of the pinch and grasp. In addition, these functional limitations are often accompanied by psychological and aesthetic problems (Zimmermann et al. 2003). An amputated thumb should definitely be reconstructed and replantation is the first preferred method. If replantation cannot be performed successfully, secondary reconstruction procedures (toe-to-hand transfer, osteoplastic reconstruction, callus distraction) and thumb prosthesis should be considered (Lister 1985; Zimmermann et al. 2003).
Disarticulation of the thumb at the metacarpophalangeal joint level is not beneficial both aesthetically and functionally without additional surgery because bulky and unaesthetic prostheses are made for this amputation level (Alison and Mackinnon 1992; Pererira et al. 1996; Shim et al. 1998; Hopper et al. 2000).
Metacarpal lengthening was firstly described by Mansoor (1969). In 1967, Matev presented his experience with satisfactory results on many cases and he suggested metacarpal lengthening for thumb amputations (Matev 1967, 1997, 1980). For continuous distraction of an osteotomized first metacarpal, there should be good mobility of the trapezometacarpal joint, and adequate soft tissue coverage of the stump with preserved sensation (Zimmermann et al. 2003).
In this study, the experience of 12 metacarpal lengthenings in thumb amputated patients is presented. Using Disability of the Arm, Shoulder and Hand (DASH) score and the pick-up test, patients returned function has been evaluated.
Materials and methods
Twelve male patients between January 2001 and December 2004 who had a thumb amputation due to gunshot wounds were included in this study. Thumb amputations had occurred in the middle one-third (9 patients in zone A, 3 patients in zone B) according to Srickland and Kleinman (Lee and Salyapongse 2005). The injury was in the right hand (dominant) in 8 patients and in the left hand in 4 patients. An isolated injury to the thumb was seen in 9 patients, while in the remaining patients other fingers had been injured. Before the operation, aesthetic hand prostheses were made for 5 of 12 patients. The thumb metacarpal was lengthened in all patients. The average patient age was 21.9 (range from 20 – 27 years). The subjects had contraindication for replantation due to either severe injury or stump revision. All patients were operated by the same surgeon using similar lengthening technique.
Functional status of the patients was evaluated with the DASH questionnaire as follows: The score was transformed from 0 – 100 (0 = normal, 100 = complete impairment of the upper limb) (Hudak et al. 1996).
A second test used for functional evaluation of the patients was the pick-up test. Patients were asked to pick up a pencil (tip-pinch), a cup of water (grasp) and an A4 sheet of paper (key pinch).
Surgical technique
All procedures were performed under axillary block. Stump revision was applied to all fingers at the initial operation (Figure 1). Callus distraction was performed with the use of mini Ilizarov type external fixator in 7 cases and uniplanar dynamic mini external fixator in 5 cases. Subperiosteal diaphyseal osteotomies were made in all cases. After a 7-day interval; lengthening was started with 0.25 × 4 mm/day. Distraction was stopped after adequate length was obtained and ossification of the distracted callus was confirmed with X-rays (Figure 2). External fixators were removed after completion of the consolidation radiologically. After appearance of a new digit at the thumb's space; webplasty was performed in all patients for gaining enough web depth (Figure 3). Patients did not accept using aesthetic finger prosthesis which was suggested after the operation.
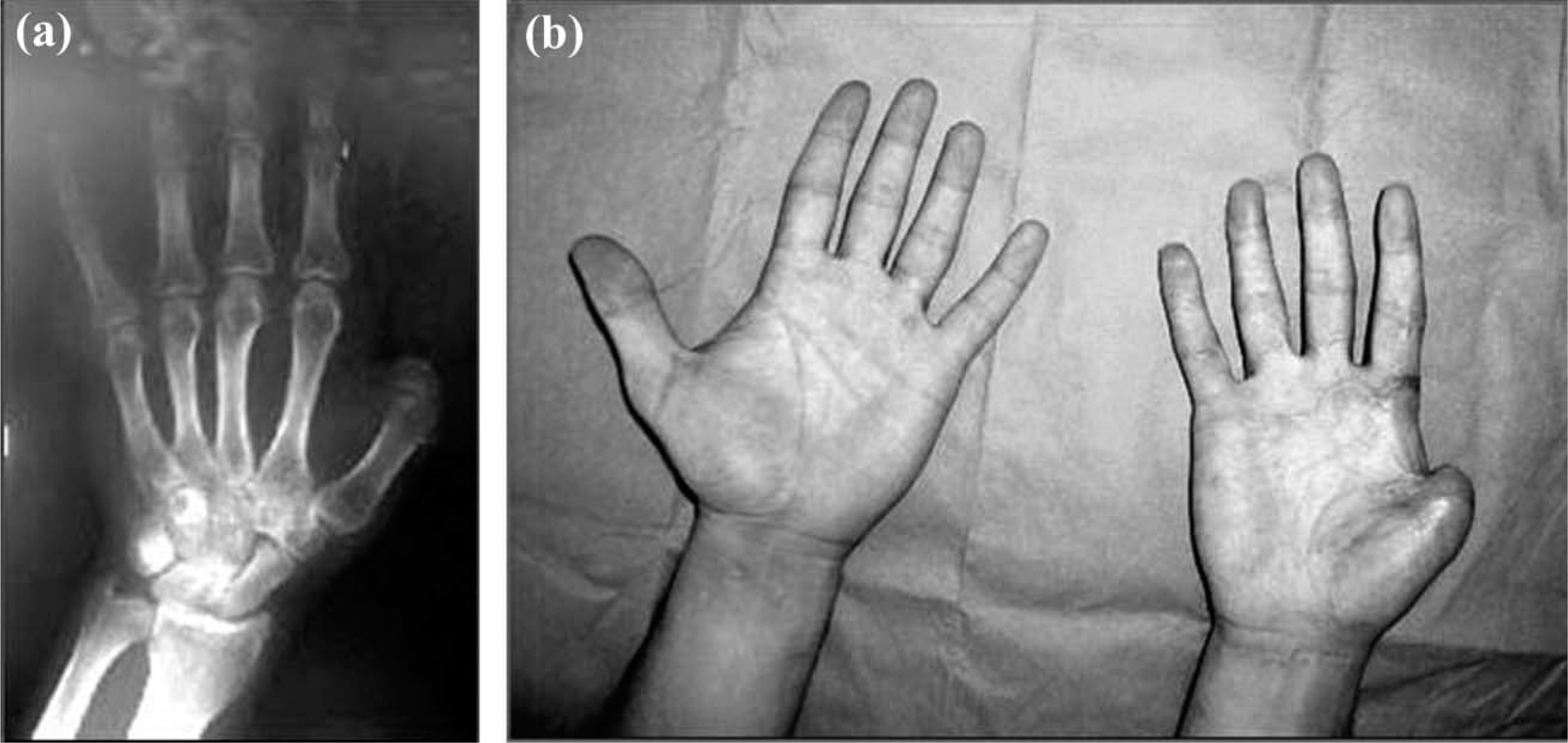
(a) Appearance of the thumb which is amputated at the level of proximal phalanx, in direct roentgenograms (AP); (b) Clinical appearance of the patient before distraction.

The callus tissue is formed after distraction.
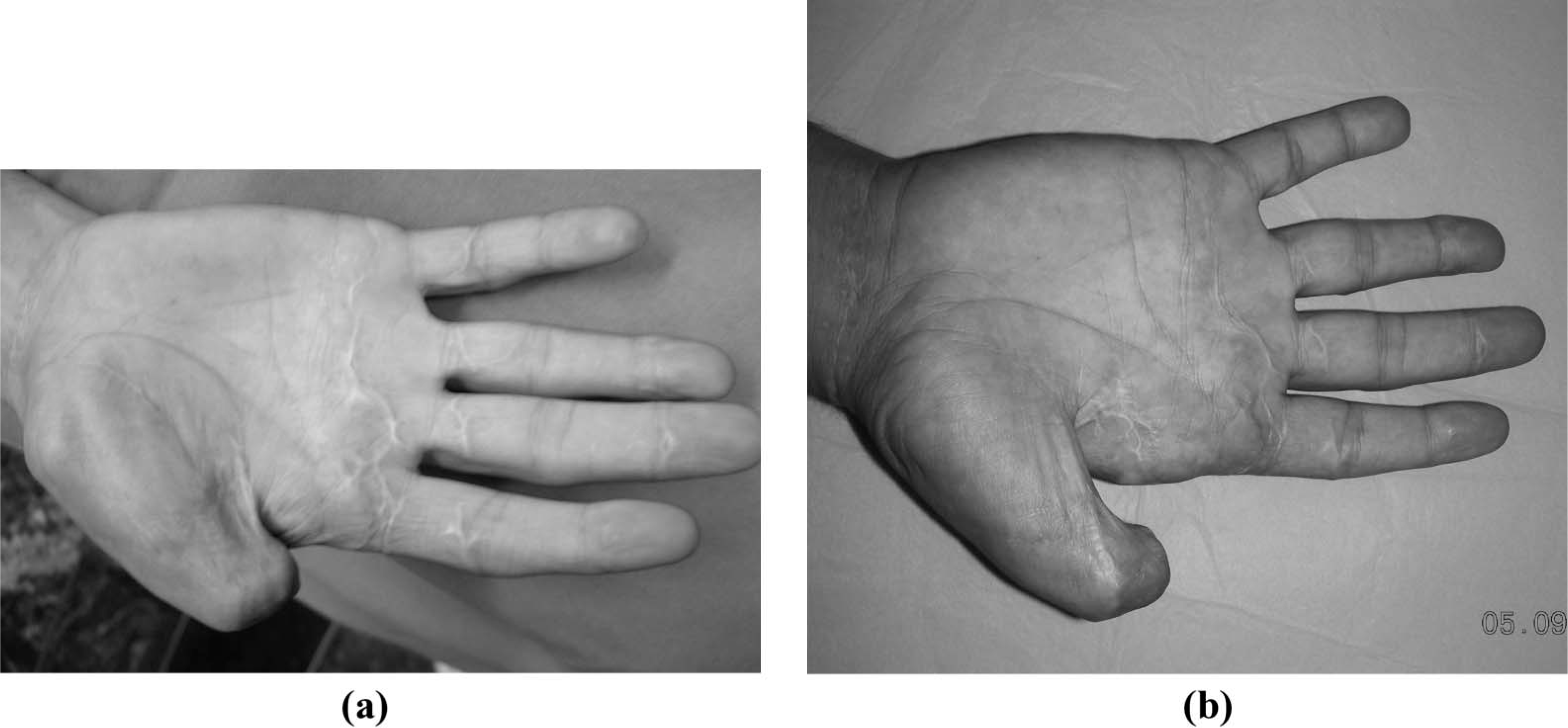
(a) Clinical appearance of the thumb after distraction and before webplasty; (b) Clinical appearance of the thumb after webplasty.
Results
The mean follow-up period was 42.08 months (range from 24 – 60). Five patients whose prosthesis had been made before the operation wore their prosthesis an average of 6.8 months (5 – 14) because of unaesthetic and bulky prosthetic construction. All patients were pleased and satisfied with their aesthetic appearance and daily activities (Figure 4). Union of the lengthened segment was observed in all cases. Average lengthening was 28.9 mm (range from 25 – 37). The mean distraction percentage for the patients was 54% of to the length of the original first metacarpal. Average healing time was 2.1 months (range from 1.8 – 2.5). Average healing index was 0.73 month/cm (range from 0.65 – 0.88). Localizations of patients' trauma, healing index, amount of lengthening and the type of the external fixators are shown in Table I. Pin tract infection was seen in 7 cases (58.3%) which were treated with wound care and antibiotics. Volar angulation developed after removing the external fixator in 1 case. However, no functional problem was observed in that patient.

The functional appearance after thumb reconstruction with distraction. (a) Holding pen (tip-pinch); (b) Grasping glass (grasp); (c) Picking up sheet of A4 paper (key pinch).
Evaluation results of the patients
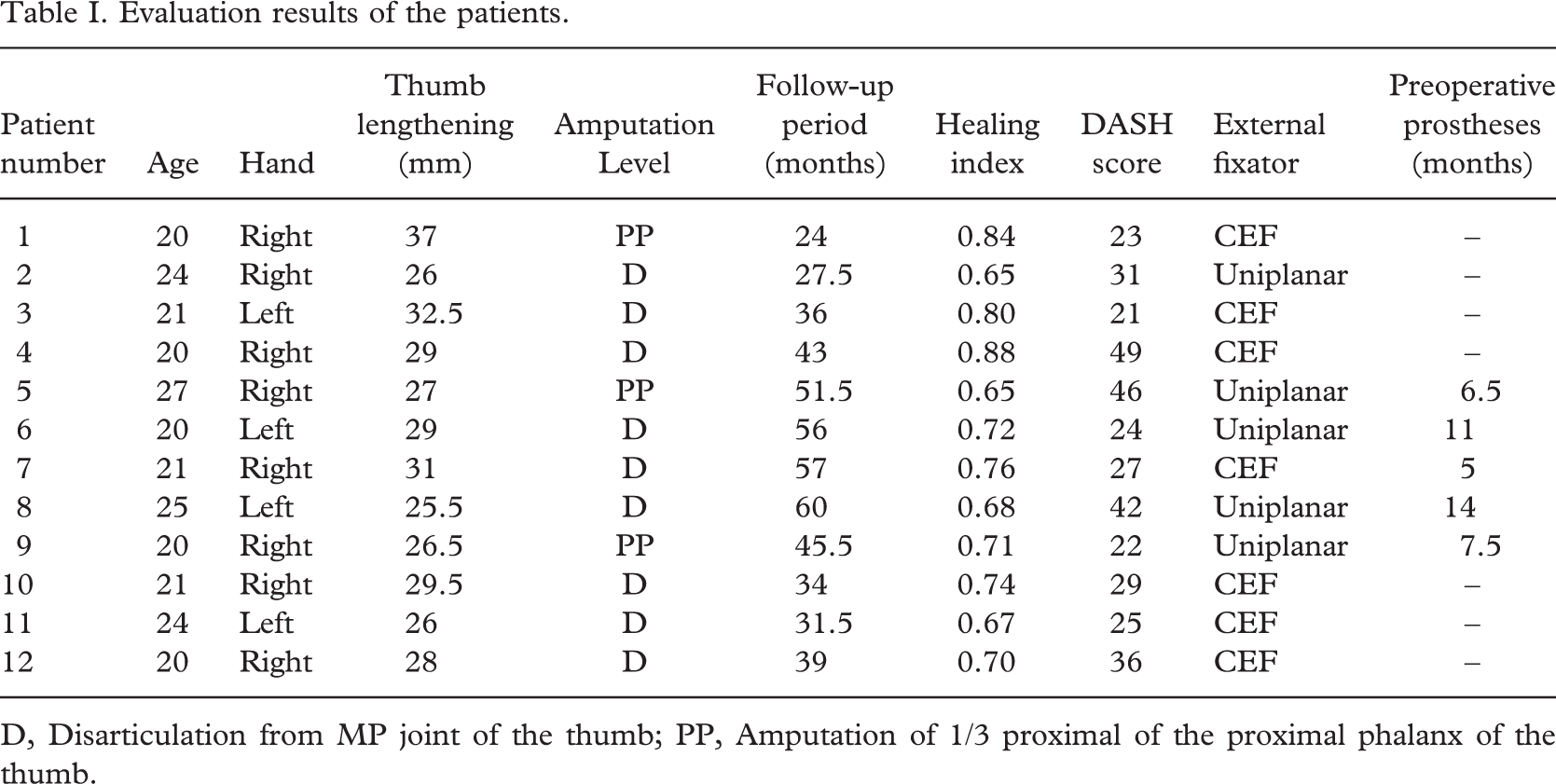
D, Disarticulation from MP joint of the thumb; PP, Amputation of 1/3 proximal of the proximal phalanx of the thumb.
Webplasty was performed in all cases; simple in 6 cases, four flap Z-plasty in 5 cases and local flap in 1 case (in which a distraction of 3.7 cm was performed).
Mean DASH score was 31.3 points (range 21 – 49). Multiple amputations were seen in the patient whose DASH score was higher than 40. Strength of pinch improved by an average of 37% and that of grasp by 48% compared to the preoperative values.
In the pick-up test all patients were able to pick up a pencil but writing ability was worse in patients with the injury of the dominant hand and some of them had begun to use the other hand as a dominant hand. All patients were able to pick up an A4 sheet of paper and a cup of water. The results of tip-pinch, grasp and key pinch of the pick-up test in 3 of the patients who had the partial amputation of second finger were not as satisfactory as the results in other patients.
Discussion
Amputation of the fingers, and especially of the thumb, due to gunshot wounds considerably affects hand function (pinch, grasp, etc.). Position, strength, length, motion, stability, sensibility and appearance make the thumb unique. The purpose of a first ray reconstruction is to facilitate improved function in accordance with the anatomical limitations of the injury.
Functional reconstruction of an amputated finger differs depending on which finger is injured, level of injury and the patient choice or expectations. This affects the choice of treatment (McGregor and Simonetta 1964). If primary replantation is impossible or fails, different methods are used for thumb reconstruction (toe-to-hand transfer, osteoblastic procedure, callus distraction) and for the thumb prosthesis.
Suspension problems of interphalangeal amputations are solved by the suction effect of finger prostheses. However, if the same problem occurs at the level of the first metacarpophalengeal joint disarticulation procedures, it cannot be solved by suction suspension (Shim et al. 1998). Thus, the authors prepared hand prostheses for 5 patients, but the design of these prostheses had poor aesthetics. The patient compliance with aftercare to reduce oedema and aid stump shape leads to unacceptable reconstruction. In these patients, a stump that allows adequate suction is needed for suspension. The required stump may be gained by using both distraction and/or webplasty techniques.
Callus distraction has some advantages when compared with the other methods. First, it is one of the less invasive methods, and bone grafting is usually unnecessary. The synchronous lengthening of bone, vessel, nerve and soft tissue is effective (Wakisaka et al. 1988). In the case of callus distraction, the risk of delayed union and non-union could be decreased by way of following the principles of the distraction and performing subperiostal osteotomy thus preserving the periosteum. According to the literature, the risk of non-union for patients older than 25 years increases with distraction more than 3 cm (Moy et al. 1982; Pensler et al. 1998; Toh et al. 2002; Zimmermann et al. 2003). Four patients distracted more than 3 cm (3.1 – 3.7) did not have delayed union or non-union. Subperiosteal osteotomy was performed in all the patients after multiple drilling at the level of osteotomy. The periosteum was carefully preserved and resutured after the osteotomy.
The first web space's depth and width are changed by lengthening of the thumb. The osteotomy site is proximal to the insertion of the intrinsic muscles while the proximal phalanx lengthening is performed. Therefore, first web space's depth and width are enlarged by lengthening of the thumb. If the level of the osteotomy is at the metacarpus, the decrease in the depth and the width of the first web will occur as the intrinsic muscles insert on the proximal site of the proximal phalanx; so inadequacy of the first web depth may be a problem in reconstructions with the first metacarpal lengthening. Webplasty operations (simple or four flap Z-plasty, local flaps, free flaps, distal radial flaps and trident flaps) were performed to solve this problem (Mansoor 1969; Rudolf et al. 2000; Zimmermann et al. 2003). The authors performed webplasty in cases with up to 29 mm of distraction, simple Z-plasty in cases between 29 and 32.5 mm of distraction and webplasty with a local flap in a case with 32 mm distraction. The depth and width of the web space were observed to be adequate after the webplasty operations and the functions of tip-pinch, key pinch and grasping improved and the aesthetic appearance was better.
In the literature, mean DASH scores and pick-up test (pinch and grasp) results have been reported to be better than this study's results (McGregor and Simonetta 1964; Colen et al. 1985; Zimmermann et al. 2003). The mean DASH score was 25 in the study of Zimmermann et al. and in this study the score was 32.8. In the study of Zimmermann et al., while the amputation level was zone B (the entire proximal phalanx or most of the proximal phalanx was preserved) in 58% of the cases, in this study the amputation level was zone B in 78% of cases. The second fingers were not amputated in the cases of Zimmermann et al. Pick-up test results of the 3 patients in the present study who had index finger partial amputation were worse than the other 5 patients. DASH scores of 3 patients were above 40; therefore, for satisfactory results of the patients who had thumb and index finger amputations, it is believed that index finger must also be distracted with the thumb finger simultaneously.
Even if the restoration of thumb length, stability, sensation and mobility problem seem to be solved by this surgical technique, one must not eliminate functional silicone prosthetic approaches such as metal thumb covered with polyurethane foam that is attached to the plastic socket or osseointegrated silicone prostheses (Michael and Buckner 1994; Sacchetti et al. 2004). In order to compare functional and cosmetic results of metacarpal lengthening with functional thumb prostheses, and fit cosmetic silicone digital prostheses, further research needs to be carried out.
Conclusion
Overall, in the light of this study; it may be concluded that metacarpal lengthening by a callus distraction technique may be a functionally and aesthetically effective reconstruction method for traumatic thumb amputations. Moreover, by providing a suction suspension with distraction and/or webplasty procedures, it is believed that a functional and aesthetically acceptable constructed thumb prosthesis is possible.