
Abstract
In The Netherlands, about 50% of all amputations of the lower limb are toes and forefoot amputations. Traumata of toes and mid-foot are rare. Preservation of the foot is the primary goal for treatment. Crush injuries of the foot may be associated with prolonged morbidity. This case study presents an insole solution for the solitary first phalangeal bone after amputation of the phalangeal bones II – V. The normal adaptation for forefoot amputations is stiffening of the sole of the shoe and a rocker bar to improve the toe off phase with load reduction of the forefoot. Because the patient had to do excessive stair climbing during work another solution was chosen. As a foot orthosis, a metal soleplate was made in order to have free movement during loading and toe-off during walking. The soleplate gives safety and provides self-adjusting properties after toe off. This enables the shoe technician to make a shoe without a rocker bar or an extra stiff insole. The 0.5 mm custom-made spring-steel plate is also used as a protective in industrial safety shoes. To improve shoe adaptation more research and case reports have to be published in order to inform doctors and shoe technicians about everyday solutions to partial foot amputations.
Keywords
Introduction
In The Netherlands, about 50% of all amputations of the lower limb are toes and forefoot amputations (Prismant 2002). Earlier reports from Finland on amputation surgery in the general population give about 25% toe amputations (Pohjolainen and Alaranta 1999).
In most cases vascular pathology and diabetes are the principal reason for amputation (Prismant 2002; Pohjolainen and Alaranta 1999). Traumata of toes and mid-foot are rare (Richter et al. 2001). Preservation of the foot is the primary goal for treatment. Crush injuries of the foot may be associated with prolonged morbidity. Initial management should be directed towards recognition and treatment of compartment syndromes, early soft-tissue coverage, and rigid skeletal stabilization to enhance soft-tissue healing (Myerson et al. 1994).
In trauma surgery, however, there is discussion about the preservation of the 1st metatarsal with fractures. If removal of the II – V phalangeal bones is inevitable adequate positioning of the 1st metatarsal bone is essential for normal use of the foot. For the amputated part of the foot pressure distribution and protection of tissue is essential. In literature there is, to the authors' knowledge, ample evidence for pressure distribution and insole construction of the shoe in traumatic foot cases. This case report presents an insole solution for the solitary first phalangeal bone after amputation of the phalangeal bones II – V.
Case
A healthy man of 53 years without a history of previous injury, diabetes or vascular pathology was involved in an industrial accident which resulted in phalangeal fractures of the I – V and wide soft tissue damage with skin and muscle damage.
After fracture stabilization of the II – IV phalanges with K-wires the crushed tissue was beyond healing. See Figure 1. The consultant in Rehabilitation Medicine advised amputation by exarticulation in the MTP joints of the II – V toes in order to preserve the function of the first metatarsal and adequate possibilities for shoe adaptation to optimize walking. After fracture and wound healing of several weeks there was limited joint mobility in the MTP 1 without pain or strain. See Figure 2. The patient was referred to the rehabilitation outpatient clinics for shoe adaptation and walking exercises.

Multiple fractures and fracture stabilization.

Clinical situation after amputation and wound healing.
Shoe adaptation
The primary goals of shoe adaptation are protection, support in weight loading of the foot and walking comfort. There are several solutions for an adequate support of the first toe. In the long term, there is a risk of rotation of the first toe and pressure on the nail of the toe. In normal shoes there is the problem of progressive dorsiflexion of the 1st toe in full weight bearing and the need for extra dept shoes for stabilization of the first toe. Because of the limited mobility of the 1st MTP joint an insole adjustment is necessary during walking. Usually a rocker bar is placed in the shoe sole with an insole with first ray support. When a rocker bar is chosen all normal and safety shoes should be adapted. Because the patient had to do excessive stair climbing during work another solution was chosen.
Insole adaptation
As a foot orthosis, a spring-steel metal soleplate was made in order to have free movement during loading and toe-off during walking. The soleplate gives safety and provides self-adjusting properties after toe off. This enables the shoe technician to make a shoe without a rocker bar or an extra stiff insole. The 0.5 mm custom-made spring-steel plate is also used as a protective in industrial safety shoes. See Figure 3.

Custom-made spring-steel metal sole plate 0.5 mm.
A plaster mould of the foot was made during stance with crutches. With this model the building of the insole started. The base-layer consists of multiform with additional cork for horizontal lining. The fixation of the metal sole plate with contact glue gives support to the plastozote top layer with an additional support in order to align the first metatarsal during mid-stance and toe-off. See Figure 4.
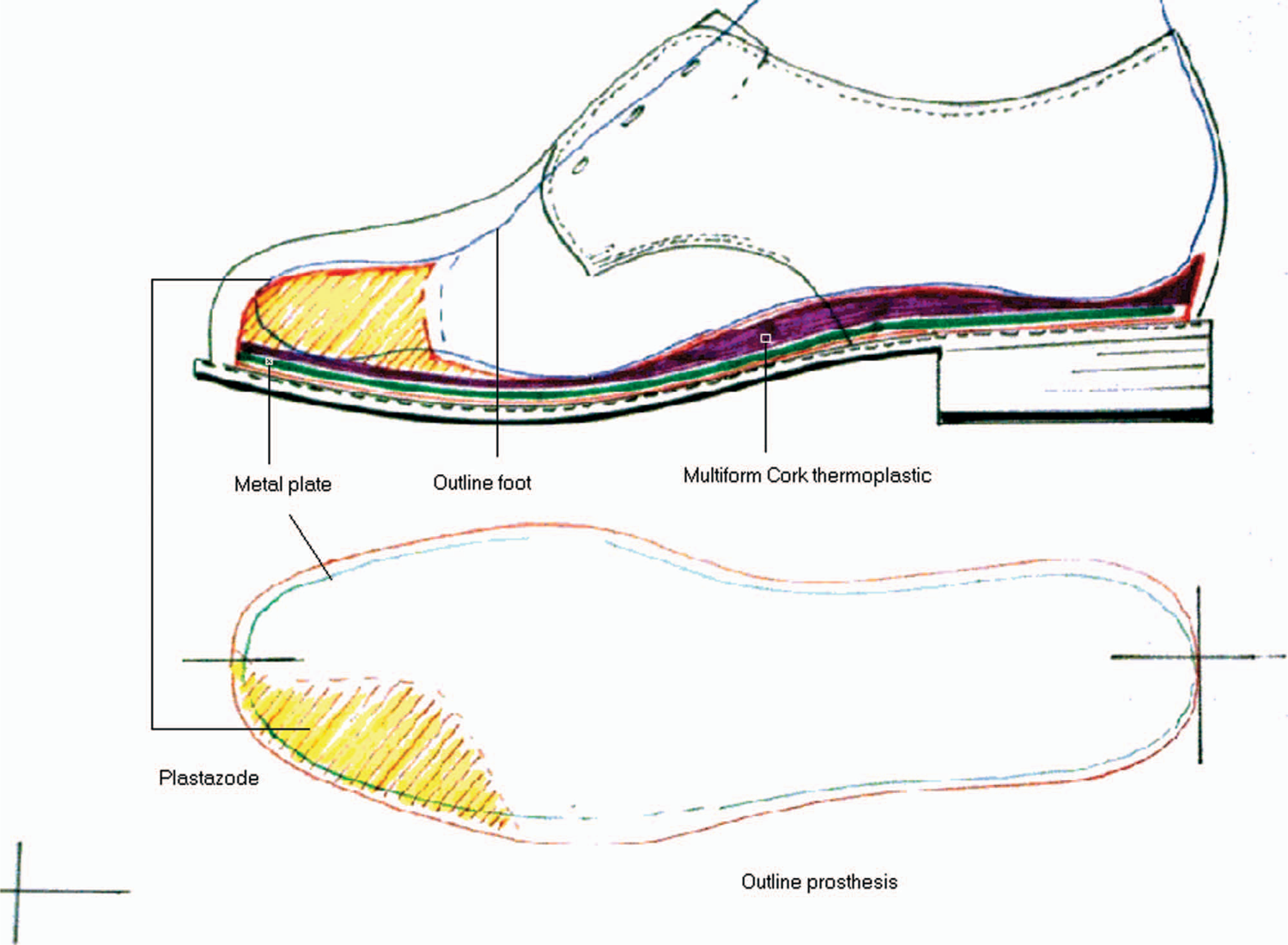
Drawing of prosthesis: Sagittal view of the insole and orthosis.
Advantage of this insole is the thin orthosis with flexible characteristics that can be used in normal walking and diverse shoes, including safety shoes without further adaptations. See Figure 5. (# 14/50) See Figure 6.

Inlay with on top plastozote top layer.

Custom-made shoes with inlay.
Two years of extensive use of the special insole in the shoe did not show any technical failure of the material. During clinical follow up there were no reports of extra callus formation or other painful changes in the foot.
Discussion
In the literature (Recal and PubMed databases) there is ample evidence for the treatment of traumatic toe amputations with shoe adaptations. Limb salvage is the main concern of the surgeon and a good pressure resistant foot. The relation towards functional shoe-ware has not been published. Adequate pressure distribution and reduction of shear forces are eminent. The authors have presented a solution to the shoe fabrication without a rocker bar by a metal plate for enforcement of the sole and improvement of walking.
The normal adaptation for forefoot amputations is stiffening of the sole of the shoe and a rocker bar to improve the toe off phase with load reduction of the forefoot (Postema et al. 1998; Hsi et al. 2004). In normal shoe adaptation this leads to a thicker sole with less comfort during stair climbing and descending. For this purpose we constructed this inlay to give comfortable walking possibilities and safe stair climbing.
Psychological impact of foot trauma can be of major importance towards acceptance of the shoe adaptations. Cosmetic disfigurement can cause post-traumatic stress disorders and depression in about 20% of cases (Fukunishi 1999). During the medical treatment this aspect should be well focused and encountered.
To encourage use of adapted shoes cosmetic appearance is important. The authors' insole guarantees optimal cosmetics in the production of the adapted shoe.
To improve shoe adaptation more research and case reports have to be published in order to inform doctors and shoe technicians about everyday solutions to partial foot amputations.
Footnotes
Acknowledgements
The authors thank the patient for his generous co-operation. They thank H. J. M. Diepstraten, orthopaedic shoe technician, for the photographs and drawings and Professor Dr K. Postema for the comments to the manuscript.