
Abstract
Background:
The great toe helps in maintaining body balance during standing, walking, running, dancing, and so on.
Case Description and Methods:
A 22 year-old female patient reported to the department, one month after losing her left hallux in a road accident. Anatomical reconstruction was performed with distraction osteogenesis. The prosthesis was constructed using a wax pattern of the normal hallux to create a silicone prosthesis. The residual limb mold was altered to increase prosthesis retention.
Findings and Outcomes:
The procedure was economical, conserved materials, and produced lifelike anatomy without requiring artistic expertise.
Conclusion:
Distraction osteogenesis helped in improving function and retention of the prosthesis. Satisfactory esthetic and functional results were observed at the one-year follow-up.
Clinical relevance
Distraction osteogenesis of the amputated hallux improved prosthetic prognosis by aiding retention. Modifications were made in the conventional prosthesis fabrication technique to increase retention, as the hallux is in constant movement and/or friction.
Background
The great toe seems to play an important role in the function of the foot. Its role in balance of the foot, propulsion, (particularly running), and pedal appearance is well accepted. 1 The hallux supports 40% of the body weight during gait. Though normal gait is possible without the big toe, it is necessary for activities such as dancing or running, for maintaining balance, and beginning different gait movements. 2 In standing, the big toe exerts more pressure than the heel, with a pressure twice that of the combined pressure of the other four toes. 3
The great toe may be affected by many conditions varying from congenital absence to diseases such as diabetes, but the greatest cause of functional impairment is trauma. Great toe amputation affects foot bone stress distribution and significantly alters the weight distribution pattern within the foot. This would inevitably affect a subject’s balance. 3
Currently, even a severely injured and traumatically amputated toe can be saved by microsurgical replantation.2,4 In certain cases where this may not be possible for psychological, financial, functional, or rehabilitative reasons, a prosthesis may be provided to restore esthetics and offer psychological help. By restoring natural appearance, the prosthesis eliminates constant reminder of the disability and offers true psychological therapy.
Retention is the primary determinant of success of a prosthesis for any part of the body and is important for esthetics, function, and comfort. Digit prostheses are normally retained by a vacuum effect on the stump. To improve the appearance and add retention on short stumps, patients may wear a ring at the junction of the prosthesis and stump. Osteointegrated implants are also an option for increasing support and retention for a prosthesis. 5 Alongside this, size of amputated stump can be increased by distraction osteogenesis. This procedure not only improves retention but also enhances function.6,7 Distraction osteogenesis was started in 1905, when Codivilla introduced surgical practices for lengthening of the lower limbs. Early techniques had a high number of complications, particularly during healing, and often resulted in failure to achieve the surgical goal. 8
The breakthrough came with a technique introduced by Gavril Ilizarov, who developed a procedure based on the ability of surrounding soft tissues to regenerate under tension, involving an external fixator. The Ilizarov technique made this surgery safer and allowed the goal of lengthening limbs to be achieved. 8 This clinical report describes the use of distraction osteogenesis to increase the stump size, followed by construction of prosthesis, to restore the traumatized hallux functionally and esthetically.
Case description and methods
A 22 year-old female patient reported to the Department of Prosthodontics, 1 month after losing her left hallux in a road accident. Surgical replantation had not been performed as the patient belonged to a remote area where the facility was not available. The remaining stump was a little dark in color compared to other digits (probably due to extravasation of blood at the time of trauma) but otherwise asymptomatic. 7 Since the size of the remaining stump was very small (7–8 mm), advice was taken from the Department of Plastic Surgery for further course of action.
Osteogenesis
Distraction osteogenesis was planned to increase the size of the remaining stump. After a latency period of 7 days, a unidirectional bone distractor with external fixator was used to distract the proximal phalange at the rate of 1 mm/day, till a total distraction of 18–20 mm was achieved (Figure 1). A 5-week consolidation period was given before removing the distractor. 6 The patient was examined about 1.5 months after distraction. Stump dimension was determined to be suitable for prosthetic rehabilitation (Figures 2 and 3).
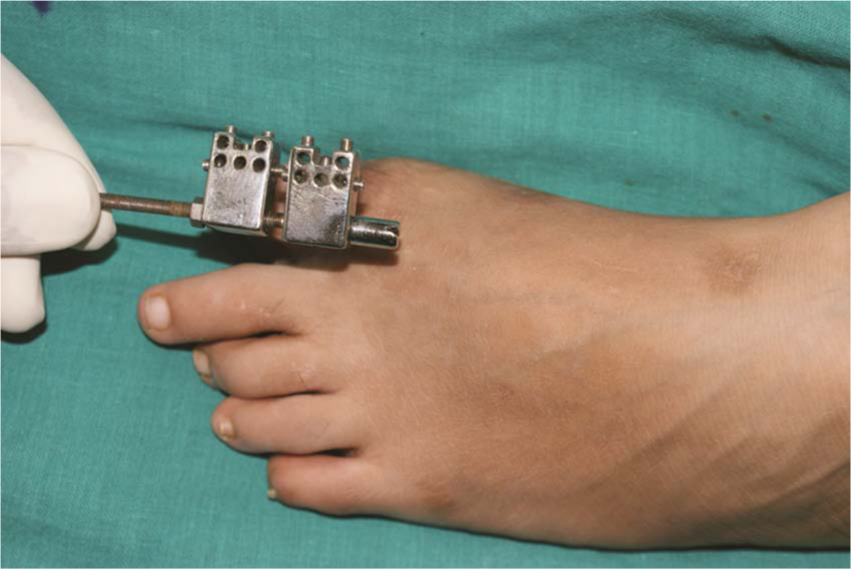
External fixator distractor in situ.

Size of residual toe after distraction, compared to the counter toe.

Radiographic comparison of great toe phalange predistraction (left) and postdistraction (right).
Prosthesis construction
Impressions of both feet were made with a thin mix of irreversible hydrocolloid (Zelgan 2002; Dentsply Pvt. Ltd, Gurgaon, Haryana, India) and poured in dental stone (Type 3 Labstone; Kalabhai, Karson Pvt. Ltd, Mumbai, Maharashtra, India) (Figure 4). Then, the residual hallux was lubricated with a thin layer of petroleum jelly (Vaseline; Hindustan Unilever Ltd, Mumbai, India ) to facilitate the removal of impression without tearing. A cylinder of modeling wax (Modeling wax no 2; Hindustan Dental Products, Hyderabad, India) providing a uniform 4-mm space for the impression material was made and used to make an impression of the residual stump with putty consistency by the addition of silicone (3M ESPE AG, Seefeld, Germany). This was poured in dental stone (Type 3 Labstone; Kalabhai, Karson Pvt. Ltd). The residual stump cast was reduced uniformly by 1 mm in the area designated for contact with the prosthesis. Markings were made on the residual stump cast to differentiate dorsal and ventral aspects, which would help in orientation of the wax pattern.

Impression of affected foot in a relaxed natural position.
An impression of the patient’s counterpart hallux was also made in a similar cylinder of modeling wax, in the natural, slightly flexed position and poured in molten wax. This pattern was gradually hollowed with a carver while still soft, from the internal side and slowly adapted on the modified residual stump cast to achieve a natural position. The pattern was then transferred to the stone cast of the affected foot. Carving was done to obtain normal curvature, size, and length of the great toe in relation to the other four toes using the stone cast of the unaffected foot as a guide, saving valuable clinical time.
The pattern was then transferred to the patient’s foot and evaluated for size, shape, retention, and minute details such as creases (Figure 5). On achieving satisfactory results, the pattern was flasked, so that the dorsal and ventral halves of the toe were obtained in separate parts of the flask to achieve better characterization (Multisil Epithetic; bredent GmbH & Co.KG, Seden, Germany). Separating medium was applied between the two pours of dental stone for easy separation, and dewaxing was done routinely. Suitable quantity of the transparent silicone was poured onto a mixing pad. Intrinsic stains were mixed into the transparent epithetic, and a direct color comparison with ventral and dorsal surfaces of the toe was carried out in natural daylight. Shade selection was performed with the patient’s approval. After all stains had been added, a thickener was used to modify the consistency of the silicone to avoid running of stains after adding them in the flask.

Wax pattern try-in.
The appropriately matched silicone was layered into its location. Even the fingernail was created with silicone at the time of processing the rest of the toe and pigmented to match the natural nails, as problems have been encountered with artificial nails in adaptation to tissue bed. Once overnight room temperature curing was complete, the final prosthesis was retrieved, excess material was trimmed using a sharp blade, and final finishing was accomplished using fine sandpaper (Figure 6). The fit and shade of the prosthesis were evaluated on the residual digit and extrinsic coloration was applied on required areas. An adjustable split ring was used to better the retention by its compressible nature. The patient was instructed to avoid prolonged contact of the prosthesis with water, sunlight, and corrosives (Figure 7).

Silicone prosthesis after curing.

Final rehabilitation (after one year).
Findings and outcomes
The distraction procedure partially restored function, while the prosthesis helped in improving esthetics. After a follow-up period of one year, the patient rated function and esthetics as 60 and 70 mm, respectively, on a visual analog scale (0- to 100-mm scale). The prosthesis was stable during normal walking, but during dancing and running, she complained of occasional dislodgement. Also, the color of the prosthesis faded slightly and had to be redone extrinsically after 8 months of fabrication. The distracted bone is being followed up radiographically till date, at 2-month intervals. Regular follow-up and compliance is the key to the management of such patients.
In Thebes, the capital of ancient Egypt, a mummy of a 50 to 60 year-old woman wearing a wooden prosthesis of the right big toe, made up of three separate components, was found. This prosthesis was skillfully crafted and at one time carried a false nail. Several areas showed clear signs of wear and rubbing, indicating that the person used it in her lifetime. 9 Hence, the importance of the big toe is evident.
In this report, bone was distracted before prosthesis construction. The advantages lay in the achievement of greater final bone length, avoidance of bone grafting, suitability for multiple lengthening procedures, shorter delay after metatarsal lengthening before the patient could put weight on the affected limb, and lower incidence of neurovascular damage. However, when the distraction osteogenesis method is used (also known as callus distraction, callotasis, and osteodistraction), some morbidities such as pin-tract infection, limitation of range of motion, stiffness, and angulation may occur. 6 Distraction osteogenesis is a surgical process in which a corticotomy is used to fracture bone into two segments, and the two ends are gradually moved apart during the distraction phase, allowing new bone to form in the gap. When the desired or possible length is reached, a consolidation phase follows in which the bone is allowed to keep healing. Distraction osteogenesis has the benefit of simultaneously increasing bone length and the volume of surrounding soft tissues. 8
Thus, this procedure helped in restoring some function and increasing both support and retention of the prosthesis. Though osteointegrated implants could have been used as in hand digit amputation cases, proprioceptive responses are poor for the big toe. This poor acuity arises because the anatomy of the foot and ankle results in poor coupling between the toe and muscles that operate it, requiring comparatively greater movement for detection by the subject.5,10 Therefore, there are chances of loading during walking and standing leading to micromotion at implant–bone interface. Such motion may cause doubtful osteointegration of implant at this site.
The mold was reduced by 1 mm to take advantage of the compressibility of the residual stump and to create a prosthesis with better retention and fit, combining the superb elasticity of silicone with suctional retention. Care should be taken that this arbitrary reduction is not excessive, to avoid creating a constricting prosthesis that may cause ischemia and associated complications. A split finger ring was placed at the margin of the prosthesis to divert attention from the junction and to improve retention by its compressible nature. The impression of the normal counterpart helped in duplicating minute details in a simple manner, saving time without requiring great skill. Because an adhesive was not required, problems of compliance were reduced. Hollowing out the solid wax toe was cumbersome and needed multiple alterations during adaptation to the residual stump, as the overlapping part had to be kept very thin.
Various materials such as acrylic resins and polyvinyl chloride may be used to fabricate toe prosthesis but have been rejected as these can be uncomfortable because of lack of flexibility. The overall durability and resistance of silicone is superior to any other material currently available for this restoration, with the benefit of gentle constant pressure applied by the elastomer helping to desensitize and protect the residual stump. Over time, scar tissue contained within the silicone prosthesis becomes more compliant and comfortable. 11 This is probably due to the massaging action of the silicone that breaks down the cement or matrix holding the scar. Such therapy appears most beneficial in preventing contractures. 12
Conclusion
In reviewing the literature, no reference was found for toe prosthesis as such. This case was an attempt to restore an amputated hallux functionally and esthetically, by combining distraction osteogenesis with prosthesis fabrication.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.