
Abstract
Background:
The purpose of this article is to describe a technique which helps in fabrication of glove-type hollow thumb prosthesis using three-part mould technique.
Case description and methods:
Patient reported to the Department of Private dental clinic, Delhi, India with a chief complaint of missing partial left thumb and wanted to get it replaced. A complete clinical hand examination was carried out, which revealed a residual stump of 1 cm length. After ensuring the medical conditions to be normal, fabrication of hollow thumb prosthesis was planned using three-part mould technique.
Findings and outcomes:
The prosthesis delivered to the patient was highly retentive because of its glove-type retention and lighter weight; feedback from the patient regarding retention was excellent. The prosthesis was aesthetically pleasing because of its excellent colour matching with the skin, and each and every part of the prosthesis could be colour customized because of easy retrieval of the third part of the mould, as well.
Conclusion:
A technique of hollow thumb prosthesis has been described in this article which helps in reduction in weight, easy packing of silicone material into the mould and easy colour customization at the knuckles area of the dorsal and ventral aspect of the prosthesis.
Clinical relevance
This three-part mould technique helps to fabricate hollow prosthesis which increases retainability and at the same time allows easy packing of silicone material and easy colour customization at the knuckles area of the prosthesis.
Background
‘Amputation’, derived from the Latin word ‘amputare’ (to excise, to cut out), has been defined as the ‘removal of part or all of a body part enclosed by skin’ (Online Medical Dictionary). There are various types of amputations like self-amputation, congenital amputation and traumatic amputation. Irrespective of the indication of an amputation, the result is a limb stump, 1 and treat-ment may be either reconstructive surgery or prosthetic rehabilitation.
Prosthesis refers to artificial replacement of an absent part of the human body 2 and serves primarily to improve the patient’s appearance as well as to support them psychologically. A prosthesis can restore aesthetics as much rather than reconstructive surgery and thus has a major role in case of lost body parts. They play an immense role in making the patient more socially acceptable. 3 Maxillofacial prosthodontists and anaplastologists play a major role in rehabilitating the patients. One of the major problems associated with prosthetic replacement is inadequate retention of the prosthesis. This may stem from the weight of the prosthesis, inadequate tissue support and/or the particular area of the body to be replaced. 4 The purpose of this article is to describe a technique which helps in the fabrication of a glove-type hollow thumb prosthesis using three-part mould technique.
Case description and methods
A 25-year-old male patient reported to the Department of Private dental clinic, at Delhi, India, with the chief complaint of partial loss of his left thumb (Figure 1). The history behind this loss presented a road traffic accident at the age of 5 years. A complete clinical examination of the hand was carried out, which revealed the loss of left thumb at the level of middle phalanx with residual stump of 1 cm in length. The area around the residual stump was found to be clear with no signs of inflammation. After ensuring the medical conditions to be normal, prosthetic rehabilitation of the amputated part was planned and the complete protocol was discussed and ethical clearance in consent form for the treatment was obtained from the patient. The prosthesis was fabricated keeping in mind the primary requirements and basic expectations of the patient.

Amputated left partial hand.
Primary impression and working model
Fabrication of the prosthesis was initiated with the first step being the making of the impression of the amputated thumb. The patient’s left hand was lubricated with a thin layer of petroleum jelly and an impression was taken using irreversible hydrocolloid (Alginate, Zelgan; Dentsply, Delhi, India) in a custom-made modelling wax (Modelling wax no 2; Hindustan Dental Products, New Delhi, India) conformer (Figure 2(a)). A working master cast was obtained from the impression using Die stone, Type IV plaster (Ultrarock; Kalabhai, Mumbai, India).
(a) Alginate impression of the defect made using wax conformer, (b) alginate impression made from the donor and (c) molten wax poured into the donor impression.
Wax pattern fabrication
The next step was to form a wax sculpture of the amputated part. A donor whose finger dimensions and contours closely matched the fingers of the patient was chosen to form the pattern. As compared to freehand sculpting, the donor technique was less time-consuming and more reliable. An alginate impression of the donor finger was taken (Figure 2(b)), and wax was then poured and removed four to five times into the impression to fabricate a hollow wax pattern (Figure 2(c)).
Stump preparation
In order to provide a snug fit of the prosthesis, 0.5–1 mm of the stump on the working model was reduced (Figure 3(a)). This allows the final silicone prosthesis to flex and stretch over the stump on insertion and removal, giving it a snug fit and a glove-like construction. With a suitable instrument such as cleoid–discoid carver, two parallel horizontal indentations approximately 0.75 mm deep and 1.0 mm wide are inscribed into the working cast around its entire circumference (Figure 3(b)) to provide a snug fit of the prosthesis. 4 A die pin with plastic sleeve (Crosspin; Nordin, Swiss Dental Products of Distinction, Chailly/Montreux, Switzerland) was placed along the long axis of the amputated end of the model to provide easy retrieval and placement of the third part of the mould that has to be casted using wax pattern (Figure 3(c)).
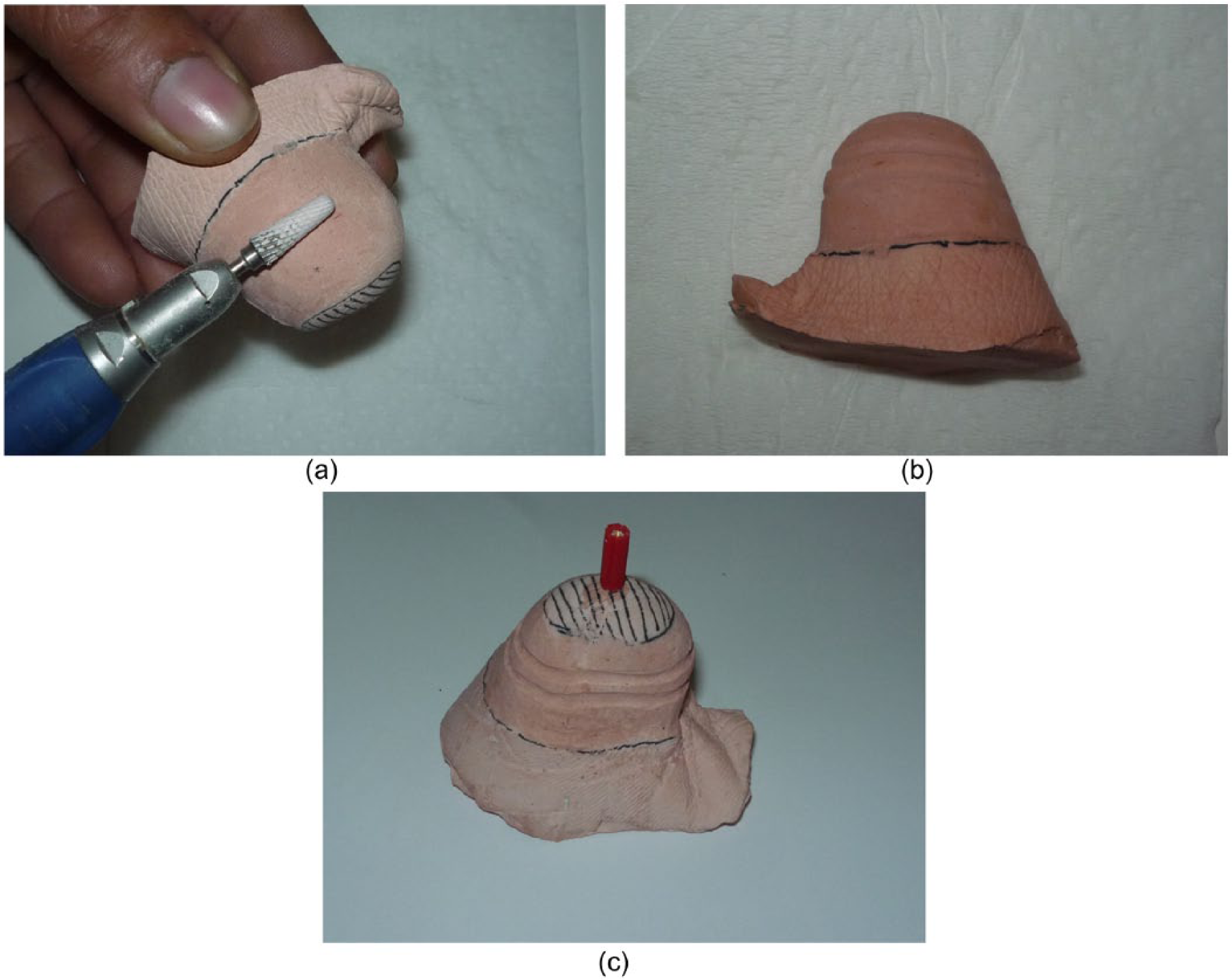
(a) Stump preparation: reducing 0.5–1 mm, (b) two parallel horizontal grooves and (c) placement of die pin.
Fabrication of model/third part from the wax sculpture
The wax pattern was then placed on the working model and modifications in sculpting were carried out to resemble the digit of the other hand (Figure 4(a)). A hole was created on the ventral aspect of the wax pattern to inject die stone for the making of the third part of the mould (Figure 4(b)). Die stone was injected through the hole (Figure 5(a)), and after complete pouring, the hole was sealed with wax (Figure 5(b)). Wax was scraped in the region of the nail and metal screw was attached to provide mechanical retention for the nail which was to be constructed using acrylic resin (Figure 5(c)). The three parts of the mould consisted of (1) base part (with attached stump), (2) counter-part and (3) detachable bullet-shaped part (in between the base and the counter-part fabricated from die stone).
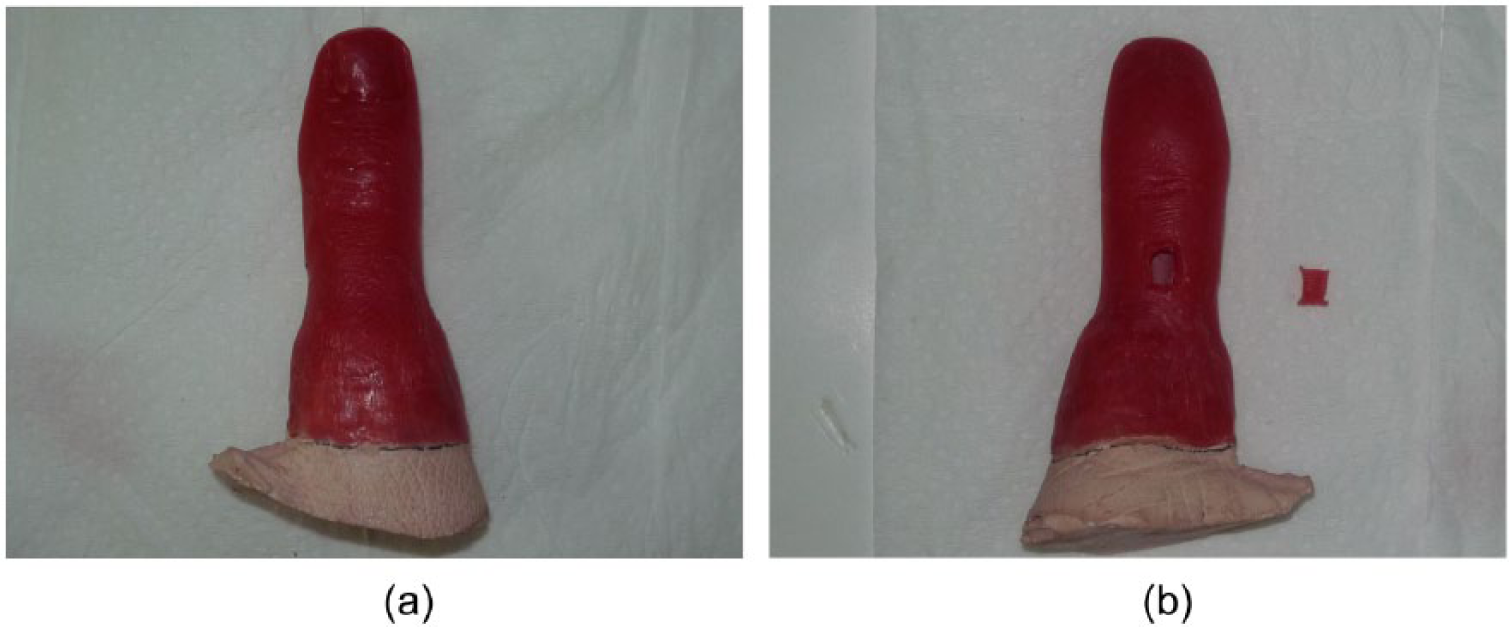
(a) Seating of wax pattern and (b) window created onto the ventral aspect of wax pattern.
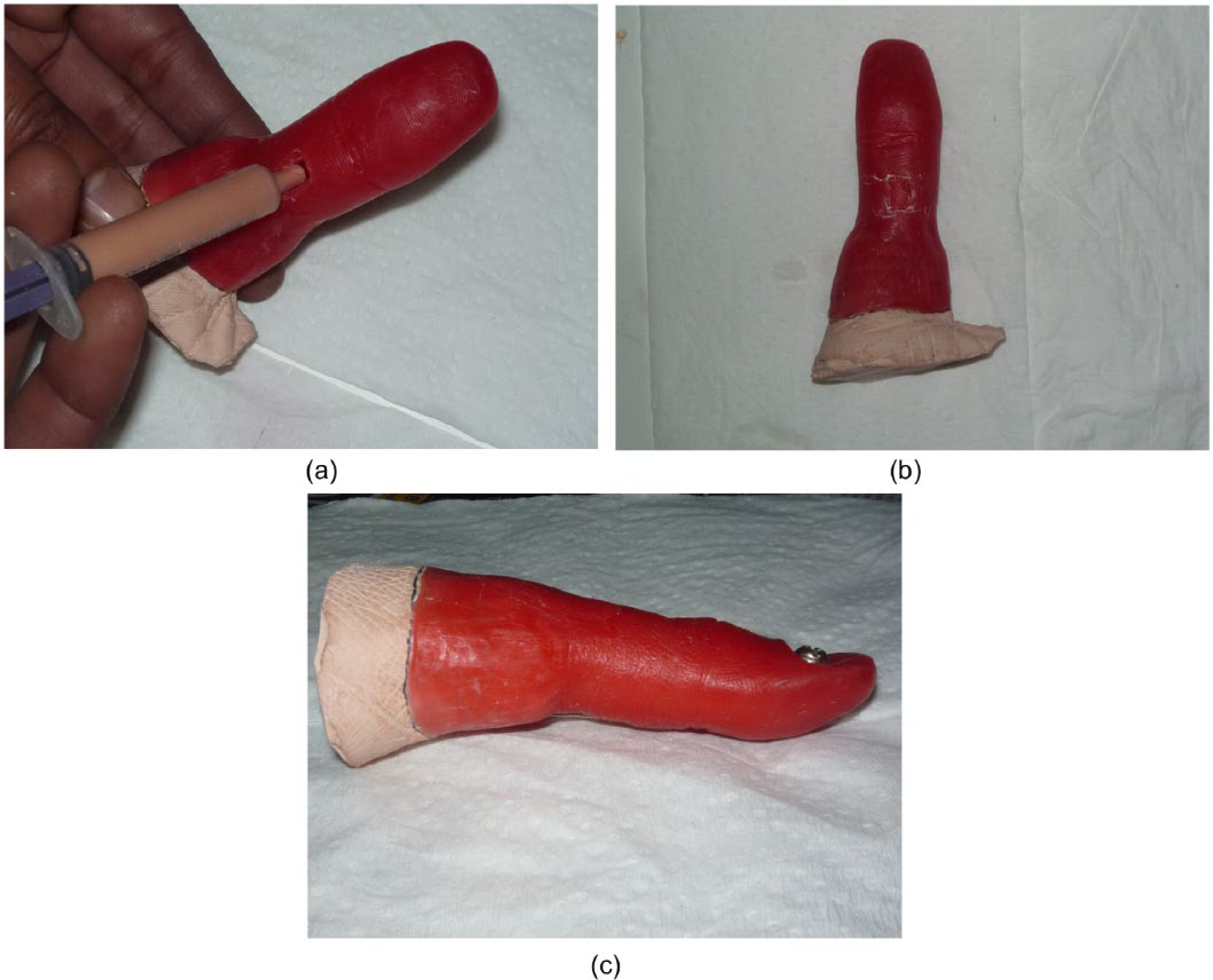
(a) Injection of die stone, (b) placement of wax window back onto the position and (c) placement of screw in the region of nail.
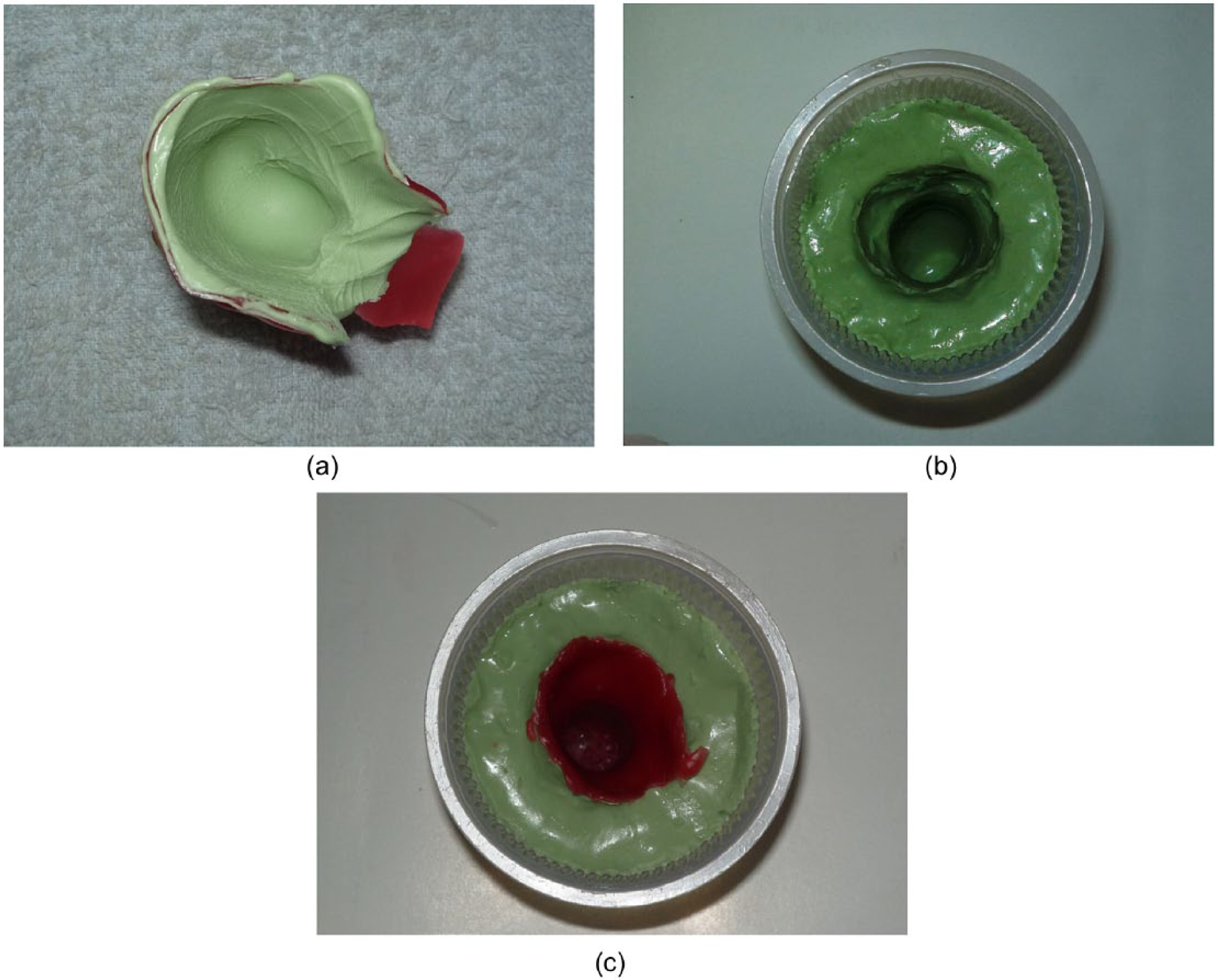
Fabrication of final prosthesis
The pattern and the stone model thus obtained were flasked using the conventional technique for heat cure acrylic resin (Figure 6(a)). Dewaxing was done and the wax was completely eliminated (Figure 6(b)). It can be appreciated that after dewaxing, there is the third part of the mould, which is detachable through the die pin (Figure 7). This helps for easy packing of silicone and precise placement of third part back into the mould. Room temperature vulcanizing silicone (Multisil-Epithetic set; Bredent, Senden, Germany) was manipulated according to the manufacturer’s instructions and packed into the mould (Figure 8). After the specific curing time, the final prosthesis obtained was checked on the patient, finished and polished. The final prosthesis which met all the basic requirements of the patient was delivered (Figure 9).
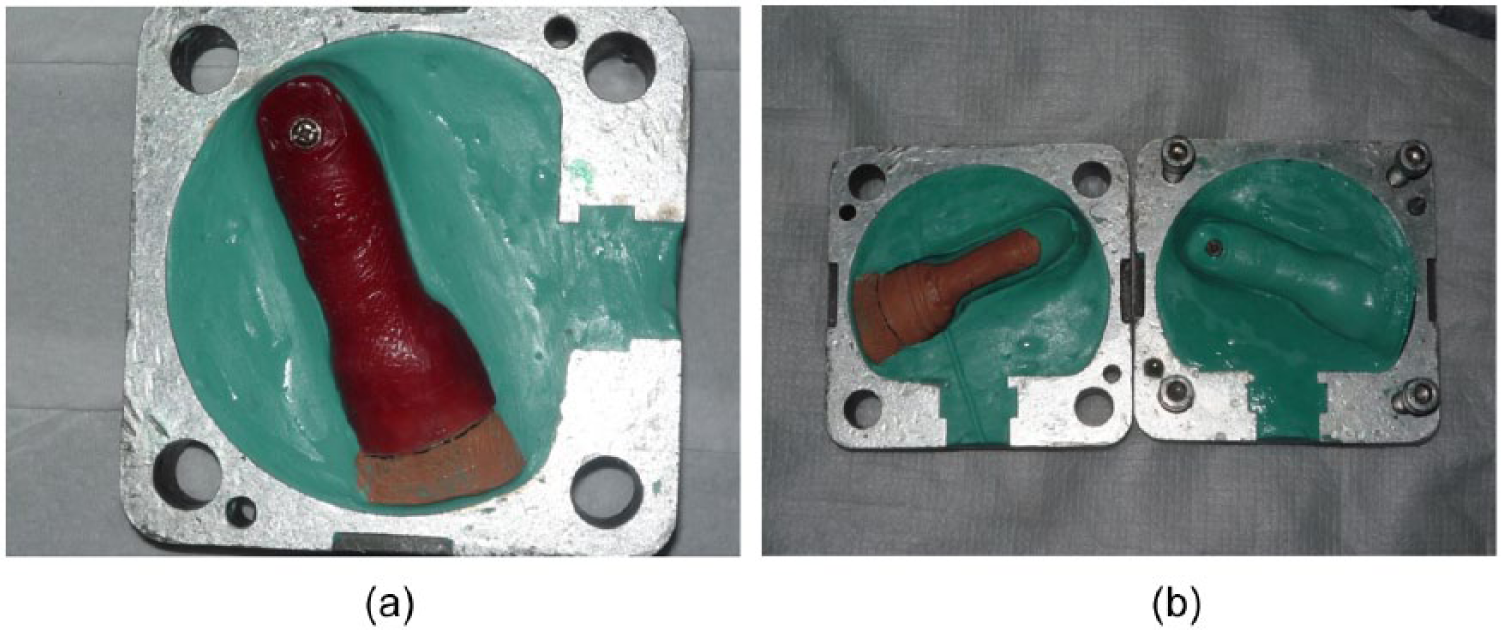
(a) Investment of the wax pattern and (b) mould after dewaxing.
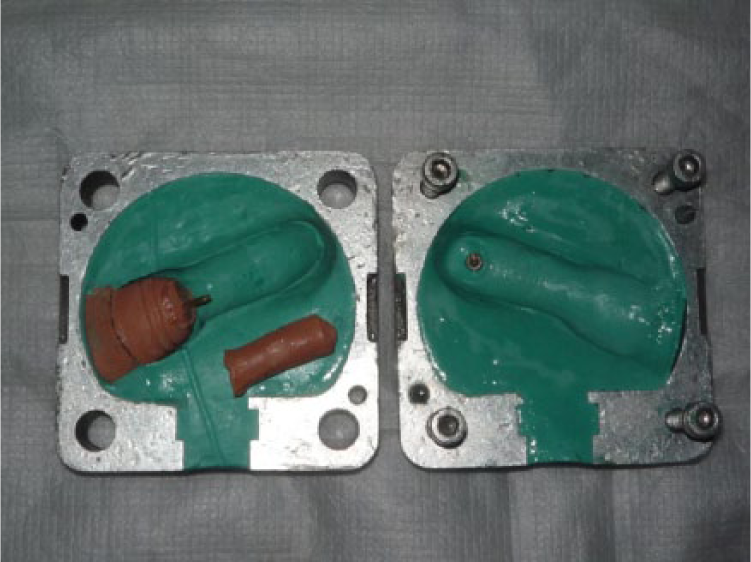
Three-part mould.

Silicone packing.

Final prosthesis.
Findings and outcomes
The prosthesis delivered to the patient was highly retentive because of its lighter weight and glove-type retention; feedback from the patient regarding retention was excellent and there was reduced risk of prosthesis detachment by itself. The prosthesis was aesthetically pleasing because of its excellent colour matching with the skin, and each and every part of the prosthesis could be colour customized because of easy retrieval of the third part of the mould, as well.
Discussion
Basic goals of prosthetic rehabilitation include preservation of the functional length, useful sensitivity, adjacent joint contractures, achieving short duration of morbidity and enabling the patient to perform tasks of daily life as quickly as possible. 5 Acceptance rate of individually sculpted custom-made silicone prosthesis has been much higher as stated by Buckner. 6
The most commonly used impression material in most of the cases is irreversible hydrocolloid – alginate7,8 using either wax 9 or plastic conformer. 10 The fabrication of wax pattern can be done by two methods: (1) by selection of an appropriate donor and (2) by the impression of the unaffected side. 7 impression of donor’s fingers is made with either condensation silicone in putty consistency or alginate and then molten wax is poured into the impression. This technique allows the avoidance of laborious task of sculpting. 11 The present technique used a donor impression to fabricate the hollow wax pattern by pouring molten wax four to five times. The limitation of this technique might be to find the similar donor. Hollowing of the prosthesis helps in reducing the weight by 40%–50%, as well as reducing the effect of gravity and preventing dislodging of the prosthesis.
The technique of mould fabrication for hollow finger prosthesis is a two-part mould technique.8–10 This case report used three-part mould technique using die pin that provides easy orientation of the third part of mould into the position after packing of silicone and at the same time helps in easy colour customization of the knuckles during the packing of silicone. The present technique makes the colour customization an easy task because the third part of the mould can be detached easily.
Retention in finger prosthesis is generally achieved by a vacuum effect on the stump, 12 medical adhesives, 13 placement of finger ring, 14 osseointegrated implant 15 and the use of separate vacuum chambers formed from the Biostar clear acrylic of 1.5 mm thickness to get the suction and to enhance retention. 16 The present technique modified the stump cast to achieve retention, the circumference of the finger stump is reduced accurately by 0.5–1 mm and two horizontal grooves are created to create vacuum chambers in order to provide a snug fit and vacuum retention. The prosthesis was highly retentive and the patient’s feedback regarding retention was excellent.
Attachment of acrylic nails on silicone prostheses is not a simple task. Silicone rubber has extremely good stain resistance which is attributed to its highly inert property.17,18 This quality of silicone rubber also makes its bonding to most materials by the commonly used adhesives a difficult challenge. Silicone sealant 14 and single part silicone 8 for the attachment of the nail to the silicone prosthesis have been used by various authors. This present technique used metal screw along with the silicone sealant for the attachment of the nail to the silicone rubber that added mechanical retention for the prosthesis.
Conclusion
This three-part mould technique presented in this article allows fabrication of hollow thumb prosthesis which allows good retention, easy packing of silicone material into the mould and easy colour customization at the knuckles area of the dorsal and ventral aspect of the prosthesis.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.