
Abstract
Background: There is a need for a prosthetic knee joint design that is technologically and functionally appropriate for use in developing countries.
Objectives: To develop and clinically evaluate a new type of stance phase controlled prosthetic knee joint that provides stance phase stability without inhibiting swing phase flexion.
Study design: A crossover repeated measures study design comparing the new knee joint to the participant's conventional low- or high-end prosthetic knee joint.
Methods: The new knee joint was fitted to fourteen individuals aged 15 to 67 years with unilateral lower limb amputations. Walk tests were performed to measure walking speed. Energy expenditure was estimated using the physiological cost index (PCI).
Results: Walking speeds with the new knee joint were on average 0.14 m/s faster than conventional low-end knees (p < 0.0001), but 0.07 m/s slower than conventional high-end prosthetic knees (p = 0.008). The PCI was similar across all three knee joint technologies (p = 0.276).
Conclusions: Mobility function with the new knee joint, in terms of walking speed, was more closely matched to high-end than low-end prosthetic knee joints. Therefore, given its relatively simple design, the new stance phase control mechanism may offer a functional and cost effective solution for active transfemoral amputees.
Introduction
A prosthetic knee joint serves a vital role in the overall function of a transfemoral prosthesis by providing stability during stance phase and controlled flexion during the swing phase of gait. 1 Stance phase knee stability is achieved by resisting knee flexion during weight bearing, which is termed stance phase control. Sophisticated prosthetic knee joint mechanisms utilize microprocessors and hydraulics to effectively control knee resistance and enable safe and efficient gait. 2- 7 However, most individuals in low and middle income countries rely on substantially more basic knee joint technologies, such as manually locking knee joints, weight-activated braking mechanisms and polycentric knee joint mechanisms. 8 While clearly more appropriate for developing countries in terms of cost, serviceability and ease of maintenance, these low-end prosthetic knee joint technologies are not intended to facilitate a high level of mobility function.
In the case of manually locking knees in particular, knee stability is achieved at the expense of a stiff-legged gait, which can decrease walking speed and increase energy expenditure during walking. 9,10 While weight-activated knees eliminate gait deviations associated with a stiff-legged gait, they result in an unnatural and delayed initiation of swing phase, since weight must be fully removed from the prosthesis for knee flexion to occur. 11 Hence, both manually locking and weight-activated friction knees are more appropriate for elderly individuals who are inclined to walk at a slow pace. 11
For active individuals, polycentric knee joint mechanisms can offer a higher level of functionality compared with manually or weight-activated knee joints. The linkages of a four-bar polycentric knee joint can be configured to enhance stability in early stance phase without adversely affecting swing phase initiation. 12 This has limits, however, since a hyper-stabilized polycentric knee joint, which may be preferable in developed countries to accommodate walking on uneven terrains, 13 impedes swing phase initiation in late stance. 12 Due to these functional limitations and issues of durability and reliability associated with more complex mechanisms, such as four-bar linkage knees, 1,8,11 it was concluded at a recent state-of-the -science meeting on the status of prosthetic technologies for developing countries that ‘there is no appropriate (knee joint) stance phase control technology available at this time’. 14
The overarching goal of this work has been to develop and evaluate a stance phase control mechanism that is technologically simple yet more biomechanically appropriate for active individuals when compared to existing low-end technologies. The mechanism has been termed the simplified automatic stance phase lock (SASPL) since it is based on a locking mechanism that engages or disengages depending on loading of the prosthetic limb during weight bearing. In contrast to existing low-end technologies, the SASPL mechanism provides a securely locked knee in early to mid-stance phase without restricting knee flexion in pre-swing and swing phase.
The work presented here relates to the development of the SASPL technology and consists of the first two steps in the development process, 8 namely (1) design and development, and (2) a clinical (laboratory-based) evaluation to assess mobility function. Mobility function, in terms of walking speed and energy efficiency, was assessed using fixed distance and fixed time walk tests. These are not only reliable and valid outcome measures of mobility in prosthetics, 15,16 but also practically applicable in developing countries, since there is no need for complex equipment such as gait laboratories. We anticipated that the new mechanism would improve mobility function for active adults compared to the prosthetic knee joints currently used in developing countries. Moreover, it was anticipated that mobility function would be comparable to that of the high-end prosthetic knees typically used in developed countries.
Methods
Participants and procedure
To address the above objectives and compare the SASPL knee joint to both low- and high-end prosthetic knee joints, a multicentre crossover study design was applied. The study involved a convenience sample of 14 individuals with unilateral lower limb amputations. Participants who possessed conventional (CONV) high-end prostheses were recruited from two sites in Canada (n = 9) and those with low-end knee joints were recruited from an institution in El Salvador (n = 5). Participants were included in the study if they were over 15 years of age and used their prostheses in the community on a daily basis, based on self-report. For seven participants, test prostheses for the SASPL knee joints were fabricated by duplicating the participant's socket and other prosthetic components. For the other seven participants, testing was done by substituting the SASPL knee for the CONV knee.
The study involved a minimum of three sessions. During session 1, preparations were made for fitting of the SASPL knee and the participant executed the testing procedure once in order to limit potential learning effects. During session 2, data were collected for the CONV knee and the participant was fitted with the SASPL knee. Data for the SASPL knee were collected during session 3, which was scheduled two weeks after session 2 to allow for adequate familiarization with the new knee. 17 The study was approved by the ethics committees of the three participating institutions. All participants provided written consent prior to their involvement in the study.
Outcome measures
Fixed distance walk test (20-meter walk test)
Fixed distance walk tests have been utilized extensively in the assessment of walking ability/capacity in prosthetics and have been found to possess excellent reliability, validity and responsiveness. 15,18,19 The walk tests were performed in a straight line within the corridors of the facility. A stopwatch was used to measure elapsed time between the start and finish lines. Participants were initially instructed to walk at their comfortable, self-selected walking speed, and then at their fast walking speed.
Fixed time walk test (two-minute walk test)
The two-minute walk test (2MWT) is a tool that objectively measures walking ability/capacity and the energy efficiency of ambulation, 20 and has been found to have excellent reliability, validity and responsiveness. 18,21,22 Participants walked along a rectangular course and a stopwatch was used to time the walking trials. The average walking speed was calculated over the distance walked.
Heart rate and physiological cost index
The physiological cost index (PCI) has been shown to correlate well with measurements of oxygen uptake in amputees and is therefore useful in ascertaining the efficiency of walking. 23,24 In this study, a chest-mounted heart rate monitor (Polar T31, Polar Electro Inc) was used during the 2MWT. Prior to the 2MWT, participants were seated for approximately five minutes and their resting heart rate recorded. After completion of the 2MWT, the active heart rate was recorded within 2–3 seconds. The PCI was calculated as the difference between the resting and active heart rates divided by the average walking speed. The unit of measure is therefore the number of heartbeats per unit of distance (metres) walked, that is, heartbeats/m. Smaller PCI values indicate lower energy expenditure.
Data analysis
A repeated measures analysis of variance (ANOVA) was used to examine the effects of the knee type (SASPL versus CONV) on the outcome variables, including walking speed and PCI score, with CONV knees being categorized as either high-end or low-end based on their technological features and intended use. Knees were deemed high-end if they were fluid-based (pneumatic or hydraulic) and intended for high mobility/activity levels (grades K3 and K4). In contrast, the low-end knees included less complex and non-fluid-based mechanisms typically prescribed for patients expected to achieve lower mobility levels (grades K1 and K2). All analysis was performed using SAS software. Differences between two means were considered significant for values of p < 0.05.
Results
Knee joint design
The SASPL knee joint is composed of a thigh element that articulates about the knee body component via the knee axis (Figure 1). A control axis, strategically positioned to respond to ground reaction force vectors, allows a small relative rotation between the knee body component and a knee shin component. Directly interfaced to the shin component is a knee lock that extends toward the thigh component and engages it to prevent knee flexion when the knee is in full extension. A spring biases the knee lock into the engaged position, thus causing the knee to automatically lock in full extension. A flexion moment at the control axis, such as is normally present in early stance phase, augments lock engagement. To disengage the knee lock, an external extension moment at the control axis occurs naturally during late stance phase as a result of forefoot loading and voluntary muscle (flexor) activation at the residual hip. With this arrangement, the knee is securely locked during stance phase and unlocked at the initiation of swing phase. The detailed biomechanical arrangement of the control axis to effectively respond to ground reaction forces has been published elsewhere.
25
The simplified automatic stance phase lock (SASPL) prosthetic knee joint: (A) assembled in a prosthesis; (B) with knee lock engaged to prevent knee flexion; (C) with knee lock disengaged shown by circle; and (D) shown flexed to about 120 degrees.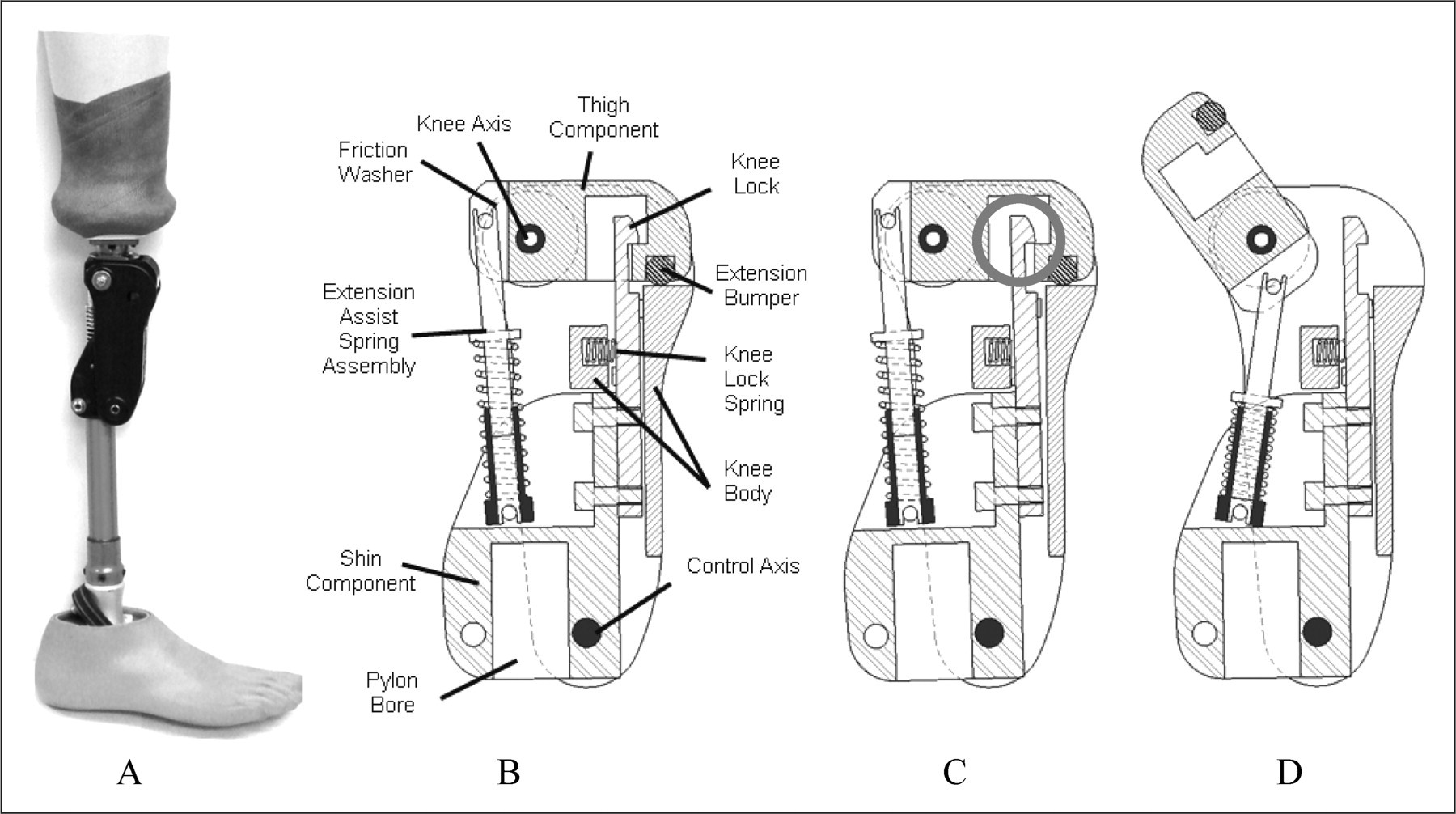
For the knee joint prototypes evaluated here, the swing phase control consisted of a compression spring (extension assist spring assembly) and an adjustable friction mechanism (friction washers). The stiffness of the spring was modified either by exchanging the spring or by adding washers to increase pre-compression of the spring. The friction mechanism was adjusted by tightening or loosening a screw and increasing/decreasing pressure on the friction washers.
Prior to commencing the clinical testing, prototypes of the SASPL knee joint were structurally tested following the International Organization for Standardization (ISO) guidelines for prosthetics 10328: structural testing of lower-limb prostheses. 26
Clinical evaluation
Characteristics of participants.
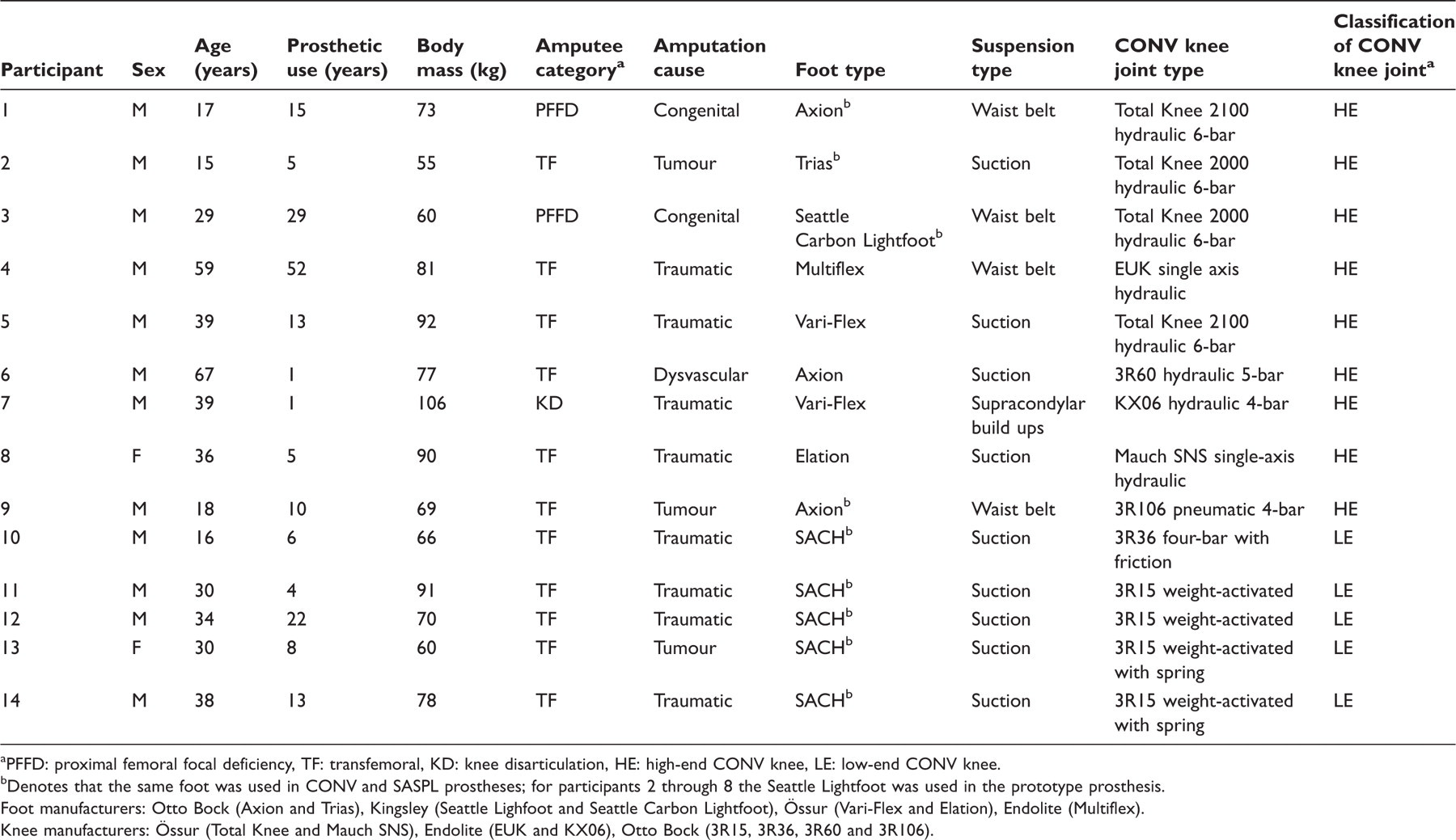
PFFD: proximal femoral focal deficiency, TF: transfemoral, KD: knee disarticulation, HE: high-end CONV knee, LE: low-end CONV knee.
Denotes that the same foot was used in CONV and SASPL prostheses; for participants 2 through 8 the Seattle Lightfoot was used in the prototype prosthesis.
Foot manufacturers: Otto Bock (Axion and Trias), Kingsley (Seattle Lighfoot and Seattle Carbon Lightfoot), Össur (Vari-Flex and Elation), Endolite (Multiflex).
Knee manufacturers: Össur (Total Knee and Mauch SNS), Endolite (EUK and KX06), Otto Bock (3R15, 3R36, 3R60 and 3R106).
Results of the 20-metre walk test and the two-minute walk test (2MWT) including the physiological cost index (PCI).
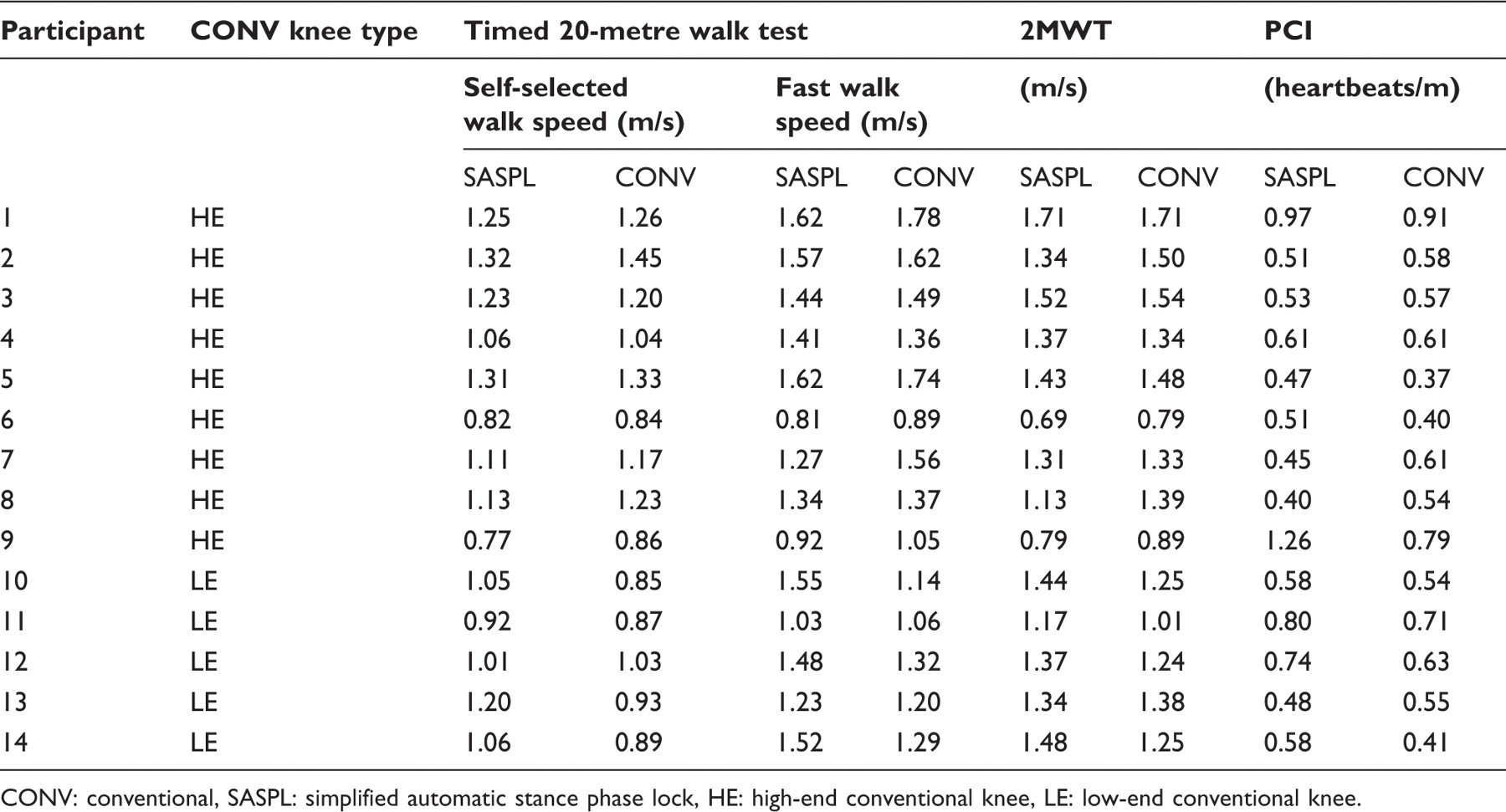
CONV: conventional, SASPL: simplified automatic stance phase lock, HE: high-end conventional knee, LE: low-end conventional knee.
Discussion
This work represents the initial steps in the development and assessment of a new type of stance phase controlled prosthetic knee joint intended to be functionally and technologically appropriate for use in developing countries. Similarly to manually locking knees, the SASPL mechanism provides a completely locked knee joint in early and mid-stance phase, which is especially important when negotiating rough and uneven terrains, a common occurrence in rural areas of developing countries. However, in contrast to manually locking, weight-activated and hyper-stabilized four-bar linkage knees, the SASPL mechanism facilitates an unencumbered transition into swing phase. Based on these functional characteristics, the SASPL knee joint was anticipated to enable improved mobility compared to conventional low-end technologies.
Our findings suggest that the SASPL technology improves mobility compared to low-end prosthetic knee joints, increasing average walking speeds by 13.6 %, 10.2% and 12.3%, respectively, for self-selected walking, fast walking and the 2MWT. Moreover, although the SASPL knee was also found to produce slower walking speeds than the high-end knees, these differences were smaller in magnitude, averaging 3.7% for self-selected walking, 5.9% for fast walking and 6.9 % for 2MWT. These findings provide preliminary evidence that the SASPL mechanism may be functionally more closely matched to high-end rather than low-end knees.
To estimate walking efficiency, the PCI was determined from the 2MWT. The average PCI values obtained (≈0.60 heartbeats/m, range 0.40–1.26) for the SASPL knee correspond closely to those reported for high-end prosthetic knee joints. 16 For a microprocessor knee joint, Chin et al. (1999) reported PCI values ranging from 0.25 to 1.20 heartbeats/m (average ≈ 0.60) for walking speeds which closely match those obtained in the current study during the 2MWT. Furthermore, average PCI values amongst the various knees (SASPL, low- and high-end CONV) in the current study were closely matched, but velocities differed. These findings coincide with previous work showing that amputees modify their walking speed to keep relative energy costs within normal limits. 27 Therefore, the improved functionality of the SASPL knee joint over conventional low-end knees may enable the user to adopt faster walking speeds due to lower energy demands.
Although instrumented gait analysis is needed to confirm this, a potential explanation for the differences in walking speeds observed for SASPL and low-end CONV knees may relate to stance phase function in late stance. Four of the low-end CONV knees in this study were weight-activated friction knees, which restrict pre-swing phase flexion because they remain locked until all weight is removed from the prosthesis. This introduces gait compensations that hinder natural forward progression during gait, an effect which is accentuated at faster walking speeds. 11 The SASPL knee is designed to be more biomechanically effective in this regard, a potential contributing factor in the higher SASPL walking speeds obtained in this study.
Four-bar linkage knees are very effective stance phase control mechanisms, however, a highly stable arrangement of the four-bar linkage knee is not ideal due to increased effort and compensation during swing phase initiation. 12 This may have been a factor in the slower walking speeds measured in this study with the low-end CONV four-bar linkage knee, the 3R36, which is specifically designed for low voluntary control. Conversely, a four-bar linkage knee can be configured to allow greater voluntary control in late stance phase, but this unfavourably decreases stability in early stance phase. 12 Geometrically locking five and six-bar linkage knees alleviate these compromises, offering concomitantly high levels of stability in early stance phase and low resistance to flexion in late stance. 28 However, these complex mechanisms are not considered an appropriate technology for developing countries. 8 The SASPL knee on the other hand, with similar functional benefits but a simpler 3-linkage system, offers a potential stance phase solution.
Limitations of this study include non-randomization of the tests and non-blinding. Furthermore, given the relatively small sample size, there are potential limitations associated with the statistical analysis and results. Finally, seven of the nine participants with the high-end CONV knees continued to have access to their conventional knees during the familiarization period with the SASPL knee, and while the level of compliance was not formally assessed, anecdotal feedback from participants suggests that some did not use the SASPL knee for the full two weeks, as instructed. Hence noncompliance leading to poor familiarization with the SASPL knee is a potential confounding factor in the results obtained here.
As part of future work, gait analysis may provide a deeper understanding of the gait biomechanics of the SASPL knee and its effects on mobility. In terms of design and development, work is ongoing to further simplify the mechanism. During the final step of this work, field testing involving a larger sample of users should provide a comprehensive picture of the SASPL technology and its appropriateness for use in developing countries.
Conclusion
Prosthetic knee joints used in developing countries are primarily founded on technologies that were developed over half a century ago and which in developed countries are primarily prescribed for individuals expected to achieve limited mobility. The SASPL technology offers a unique approach to facilitating stance phase control, which may be more suitable for young and active individuals. The findings of this study indicate that the SASPL technology may be beneficial in enabling faster and more normal walking speeds without additional energy costs. Future work is needed to more finely examine the mechanisms behind this. Conversely, future work is needed to more broadly examine the functionality, utility and appropriateness of SASPL technology in developing countries.
Footnotes
Funding
This work was supported by the Canadian Institutes of Health Research [grant number 200704PPP], Ontario Centers of Excellence [grant number MR40095-09] and the Ministry of Research and Innovation.
Acknowledgements
We would like to thank Gilberto Abarca, Evelin Mena, Monica Castaneda and Carlos Zelaya at Don Bosco University in El Salvador, and RJ Clemens and Marcus Weber at the Sunnybrook Center for Independent Living in Toronto, Canada, for their assistance in collecting data. We would also like to thank the students that participated in the various aspects of the project including Alex Furse, Jennifer Irwin, James Christensen and Alyssa Randal, as well as, Bill Johnson for his technical expertise in the development of the SASPL prototypes. Finally, we thank Andy Dondorff and the team at DuPont Canada for their support.