
Abstract
This study investigated energy expenditure and obstacle course negotiation between the C-leg® and various non-microprocessor control (NMC) prosthetic knees and compared a quality of life survey (SF-36v2™) of use of the C-leg® to national norms. Thirteen subjects with unilateral limb loss (12 with trans-femoral and one with a knee disarticulation amputation) participated in the study. The mean age was 46 years, range 30 – 75. Energy expenditure using both the NMC and C-leg® prostheses was measured at self-selected typical and fast walking paces on a motorized treadmill. Subjects were also asked to walk through a standardized walking obstacle course carrying a 4.5 kg (10 lb) basket and with hands free. Finally, the SF-36v2™ was completed for subjects while using the C-leg®. Statistically significant differences were found in oxygen consumption between prostheses at both typical and fast paces with the C-leg® showing decreased values. Use of the C-leg® resulted in a statistically significant decrease in the number of steps and time to complete the obstacle course. Scores on a quality of life index for subjects using the C-leg® were above the mean for norms for limitation in the use of an arm or leg, equal to the mean for the general United States population for the physical component score and were above this mean for the mental component score. Based on oxygen consumption and obstacle course findings, the C-leg® when compared to the NMC prostheses may provide increased functional mobility and ease of performance in the home and community environment. Questionnaire results suggest a minimal quality of life impairment when using a C-leg® for this cohort of individuals with amputation.
Introduction
The Otto Bock 3C100 C-leg® has been recommended to a broad spectrum of individuals with amputation who seek a prosthesis with better control of stance and swing, from the highly functional individual to those who are limited in independent ambulation (Otto Bock 1999). However, the C-leg® and other microprocessor prostheses have created enthusiasm as well as debate regarding indications, contraindications, and cost effectiveness (Berry 2004). Objective information comparing these prostheses will assist in answering these important clinical issues.
The high-energy cost of ambulation is a major concern for wearers of trans-femoral prostheses. Jaegers et al. (1993) found the mean heart rate of 11 subjects with unilateral trans-femoral amputation was significantly higher than the mean heart rate of able bodied subjects at rest and at all walking paces; the mean heart rate in a group of subjects with use of a trans-femoral prosthesis at 50 m/min was 116 bpm which is 48% higher than able bodied controls and at 75 m/min was 134 bpm which is 61% higher than able bodied controls. Chin et al. (2003) in a study of 8 physically fit individuals fitted with an Intelligent Prosthesis (a microprocessor-controlled pneumatic swing phase control knee) found that, while the most efficient walking speed was approximately the same as that of an able-bodied group, energy expenditure as reflected by oxygen consumption was 31.1% and 24.1% higher than controls at speeds of 50 and 70 m/min respectively. The differences between able bodied and those with a trans-femoral amputation persist when energy expenditure is expressed as oxygen cost per metre walked (ml/kg.m). Energy expenditure also differs depending on the cause of trans-femoral amputation. Waters et al. (1976) found an oxygen consumption of 0.35 ml/kg.m in a group of individuals with a trans-femoral amputation due to vascular causes at a pace of 36m/min compared to 0.25 ml/kg.m for those with a traumatic cause at a pace of 52 m/min. The ambulation of subjects with lower limb amputations show higher than normal energy costs (Waters and Mulroy 1999). The authors are not aware of any investigations of energy expenditure of the C-leg® published in the English language except a single case study design of an individual with bilateral knee disarticulations. Perry et al. (2004) showed the C-leg® resulted in a lower rate of energy cost compared to two other prostheses (a ‘stubby’ design and a Mauch SNS). In a related study, three subjects with a unilateral hip disarticulation, the Intelligent Prosthesis had a decreased oxygen uptake of between 10.3 and 39.6% compared to the Otto Bock 3R15 mechanical controlled stance phase control knee (Chin et al. 2005).
The application of functional tests of mobility specifically for individuals with lower limb amputations has not been widely studied. One way to measure functional abilities is to use an obstacle course (Schrodt et al. 2004). The Standard Walking Obstacle Course (SWOC) is a 12.2 m carpeted path with turns and obstacles at standardized locations. The SWOC was found to be reliable, valid, and a useful clinical tool for functional measurement of ambulatory status in a study involving two groups of subjects, able bodied and older adults with arthritis; the SWOC scores for able-bodied adults averaged 10.2 sec without carrying a weighted basket and 12.4 sec for carrying a weighted basket (Taylor and Gunther 1998). The authors are not aware of any obstacle course studies showing comparison between prostheses.
Quality of life surveys that are specific to those with amputation are available but have not been widely used or have limited validity or reliability studies (Legro et al. 1998; Miller et al. 2003). For this investigation, it was chosen to use the SF-36v2™ (SF-36v2™, Quality Metrics, Lincoln, RI). The SF-36v2™ is a widely published survey for both able-bodied subjects and those with impairments. In addition, the SF-36 is easy to use, acceptable to patients, and has established reliability and validity for many populations with impairments (Brazier et al. 1992; Jenkinson et al. 1994; Jenkinson et al. 1996). The reliability coefficient of the SF-36 ranged from 0.60 – 0.94 and the test-retest reliabilities ranged from 0.60 – 0.81 (Coons et al. 2000). Smith et al. (1995) stated the use of newer functional outcome tools such as the SF-36 provides insight into many areas of functioning and well being. In their study of 24 individuals with traumatic trans-tibial amputations found significantly decreased SF-36 scores in bodily pain, role physical and physical functioning compared to able bodied age matched controls (Smith et al. 1995). Dougherty (2003), in a survey of 46 patients an average of 28 years after unilateral trans-femoral amputation secondary to injury from the Vietnam War, found responses to the SF-36 significantly lower compared to historical controls in all areas except vitality and mental health. He stated these lower scores suggest an impaired quality of life. Hagberg and Branemark (2001), in a survey of 97 Swedish individuals with non-vascular trans-femoral amputation, found significantly lower scores in all dimensions of the SF-36 compared to age and gender matched norms.
Since there have been few studies comparing the C-leg® to a NMC prosthesis, we investigated the use of the C-leg® and the NMC knees with respect to energy expenditure and obstacle course data as well as comparing the SF-36v2™ during C-leg® use to national norms for able bodied individuals and those with limitation.
Methods
Subjects
This study was approved by the authors' Institutional Review Board. Prior to participation, subjects signed an informed consent. Subjects were recruited by certified prosthetists from the Central New York, New York City, and South Carolina areas. The study included subjects who used a C-leg® after using a NMC prosthesis, were highly effective ambulators (within United States Medicare functional level four, having ‘the ability or potential for prosthetic ambulation that exceeds basic ambulation skills which is typical of the prosthetic demands of the child, active adult, or athlete’), and did not have a concurrent medical or musculoskeletal condition limiting their functional mobility. The C-leg® was the current prosthesis of choice for all subjects. As indicated in Table I, duration of C-leg® use was 2 – 44 months. Thirteen subjects with unilateral limb loss due to non-vascular causes (12 with trans-femoral and one with a knee disarticulation) participated in this study. Other demographics of the subjects are contained in Table I.
Subject demographics (n = 13).
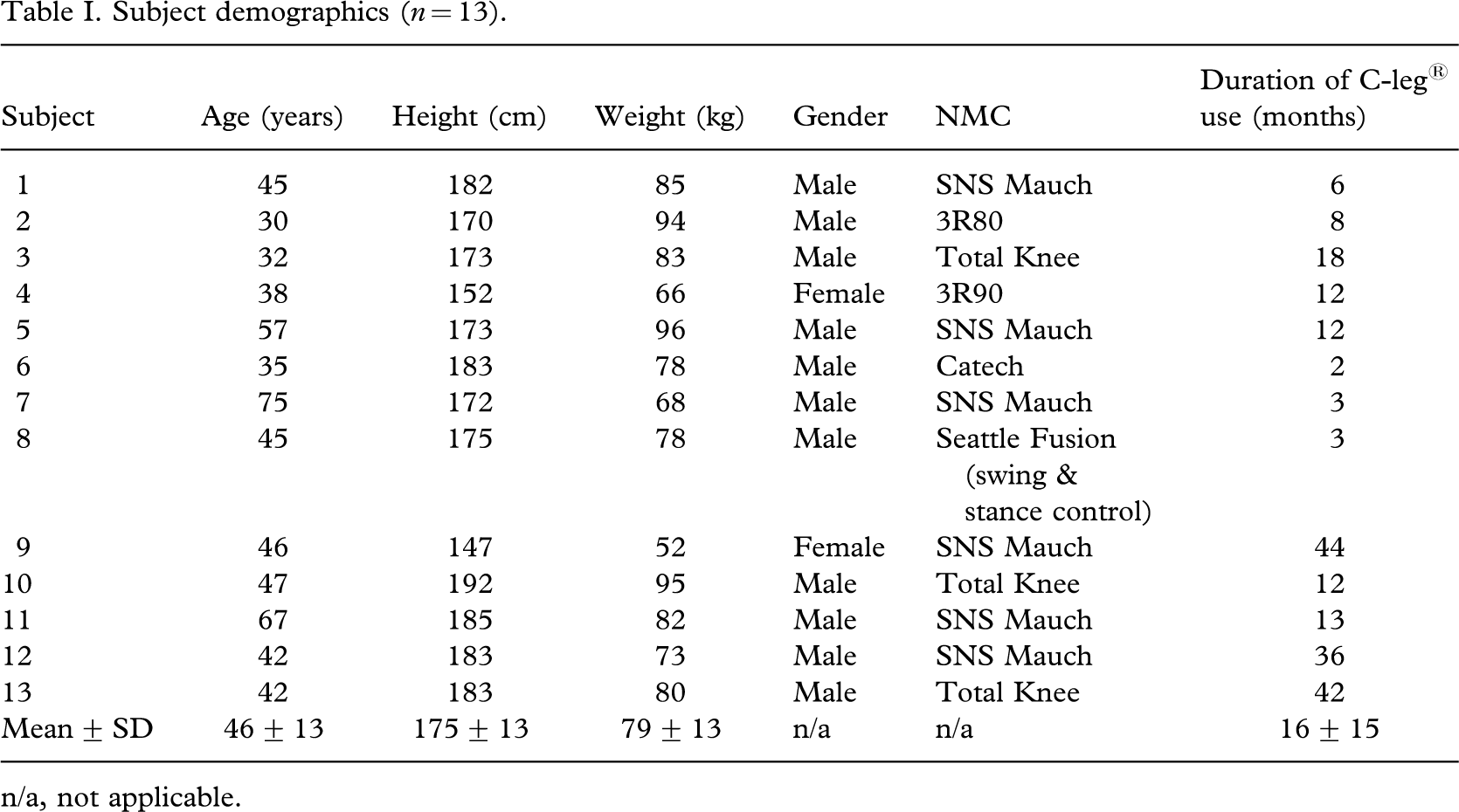
n/a, not applicable.
Energy expenditure
Prior to data collection, subjects were allowed to walk for approximately 5 min at zero per cent grade on a motorized treadmill to determine their self-selected typical and fast walking paces. To obtain oxygen consumption data, subjects wore a mouthpiece and nose plug to collect gases during ventilation and a Polar heart rate monitor was used throughout testing. Testing consisted of ambulating on the treadmill for 8 min. One minute was a warm-up, 3 min were at a self-selected typical pace, 3 min were at a self-selected fast pace and 1 min was a cool down. After a 10-min rest, the subject completed the same procedure with the other prosthesis with the same self-selected walking paces. Oxygen consumption was determined using a Medical Graphics CardioO2/ECG Exercise System (Medical Graphics Corporation, St Paul, Mn) and BREEZE EX v 3.05 software.
One subject did not perform the energy expenditure test due to scheduling conflicts. Two additional subjects did not perform the self-selected fast walking portion due to pain caused by the NMC prosthesis and their perceived risk of falling. These two subjects felt that they could have walked at a fast pace with the C-leg®. Therefore, ten subjects participated in this portion of the study.
Standardized Walking Obstacle Course (SWOC)
A functional obstacle course component was included in the study in order to determine if there was a difference in ambulation characteristics between use of the C-leg® and the NMC prostheses. Similar to the energy expenditure testing, ten subjects participated in this portion of the study. The SWOC consists of a 12.2 m walkway that includes a low profile rug with a 30° turn to the right, a 90° turn to the left, and then a 70° turn to the right (Figure 1). Each subject began the obstacle course by rising from a seated position in a chair with armrests and completed the course by sitting in a chair without armrests at the other end of the walkway. The subject encountered obstacles such as an axillary crutch to step over, a trashcan to manoeuvre around, and shag and multi-coloured rugs to walk over (Taylor and Gunther 1998). Step-offs were defined as an instance when any part of the subject's foot was outside the designated walkway. Stumbles were defined as a loss of balance or contact with obstacles in the course. Subjects were given a thorough description of the SWOC and were instructed to ambulate as they would in their normal environment while attempting to maintain both feet on the walkway at all times. Each subject completed the obstacle course under two conditions: hands free and carrying a 4.5 kg (10 lb) weighted laundry basket. Four trials for each prosthesis and each condition were collected. Similar to the procedures used by Taylor and Gunther (1998), total time, number of steps, number of step-offs and number of stumbles was recorded for each trial.
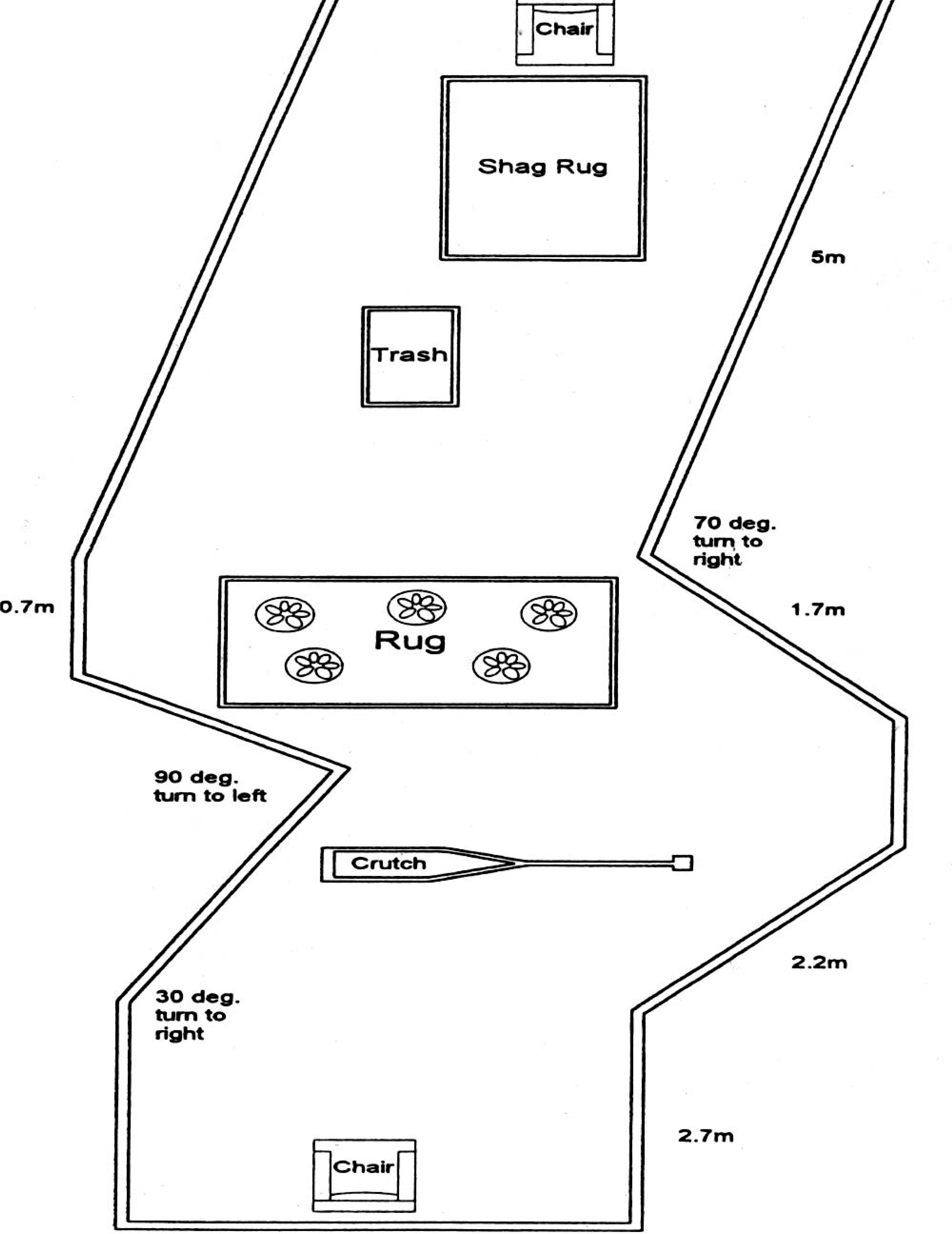
Diagram of Standardized Walking Obstacle Course (SWOC).
Quality of life survey
A licence to use the SF-36v2™ was received from QualityMetrics. The SF-36v2™ is composed of two component scores, physical component score (PCS) and the mental component score (MCS). The PCS is comprised of general health (GH), bodily pain (BP), role physical (RP), and physical functioning (PF) dimensions. The MCS is comprised of vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH) dimensions. These eight scales contain 2 to 10 items each. The SF-36v2™ is a brief 36-item self-administered general health status questionnaire, which takes approximately 5 – 10 min to complete. The SF-36v2™ uses a graded multiple level response system rather than yes or no answers. The SF-36 items are scored so that a higher score indicates a better health state (Ware and Kosinski 2004). The SF-36v2™ is generally recommended over the SF-36 for the following reasons (Coons et al. 2000). The SF-36v2™ offers increased range and precision for the role functioning scale, improved item wording, improved layout for questions and answers, increased comparability in cultural adaptations, minimizes the ambiguity and bias in wording, and has an easier to use format. The SF-36v2™ uses norm based scoring algorithms for each of the eight scales (Ware et al. 2002). These algorithms allow comparison to the population norm defined as a mean of 50 and a standard deviation of 10. Therefore, subject scores can be directly compared to a population mean. All subjects completed a quality of life survey, (SF-36v2™) based on use of the C-leg®. Since the C-leg® was the current prosthesis of choice, SF-36v2™ data were not analysed for use of the NMC prostheses. The outcomes of the questionnaire were used to compare a subject's perceived quality of life using the C-leg® to national norms. Thirteen subjects completed the SF-36v2™.
Data analysis
Administration of the testing procedures for the C-leg® and NMC prostheses were completed on the same day using a randomized testing sequence and results compared between prostheses. For each prosthesis, individual steady state heart rate and oxygen consumption were determined at a typical walking pace and fast walking pace. These determinants were averaged over the last 30 sec of the typical and fast walking paces where steady state conditions were evident. Oxygen consumption, an index of energy expenditure, was collected on all subjects and calculated in two ways (ml/kg/min and ml/kg.m). Paired t-tests were used to analyse heart rate, oxygen consumption, SWOC number of steps and time data. The number of step-offs and stumbles for the SWOC, were not normally distributed. Therefore, a non-parametric test, the Wilcoxon Signed Rank, was used to compare results from the use of each prosthesis. In addition, test re-test reliability for the number of steps and the time to complete the obstacle course was measured by Pearson Product-Moment Coefficient of Correlations. SF-36v2™ data were compared to national norms. For all tests, statistical significance was set at 0.05.
Results
Energy expenditure
Table II contains the heart rates and oxygen consumption of the subjects that were able to complete the treadmill testing at a typical and fast pace (n = 10). Statistically significant differences were found between prosthetic groups for mean oxygen consumption at both typical and fast walking paces. The mean typical pace on the treadmill was 49 ± 15 and the mean fast pace was 70 ± 20 m/min.
Mean comparisons of heart rate and oxygen consumption (n = 10).
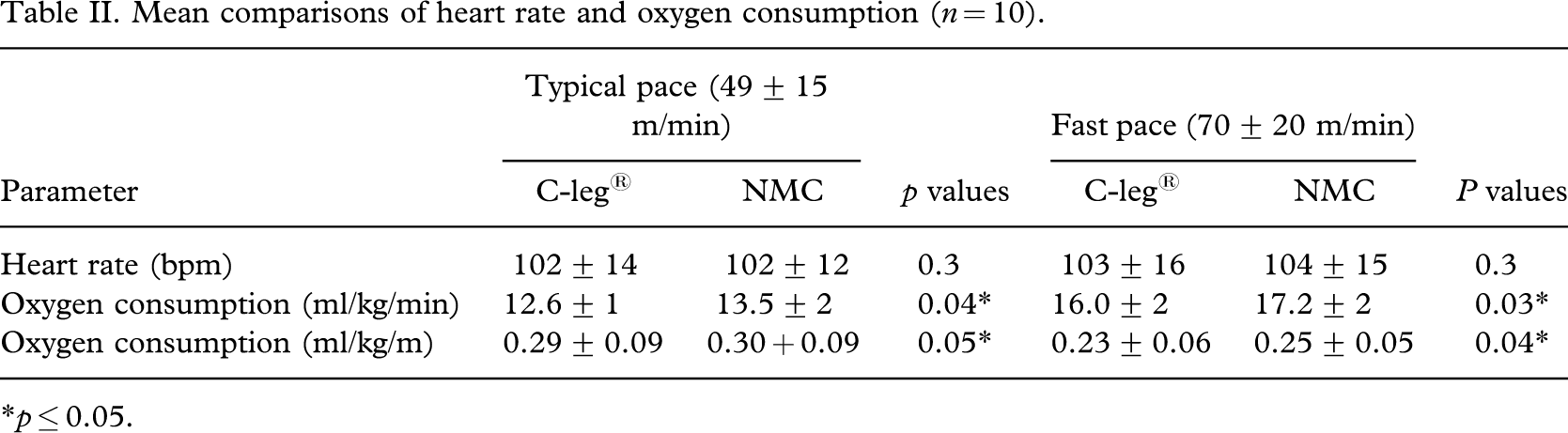
∗p ≤ 0.05.
Standardized walking obstacle course
Table III shows the mean values of various parameters measured while subjects negotiated the functional obstacle course under the conditions of hands-free and carrying a 4.5 kg (10 lb) basket. The number of steps, total time, and the number of step-offs with hands-free using the C-leg® compared to the NMC prostheses were significantly less (p ≤ 0.05). The total time while carrying the weighted basket using the C-leg® was significantly less compared to the NMC prostheses. Test re-test reliability among the four trials for number of steps and time to complete the obstacle course showed excellent correlations ranging from 0.79 – 0.93 for steps without carrying a weighted basket, 0.88 – 0.96 for steps carrying a weighted basket, 0.89 – 0.98 for time without carrying a weighted basket, and 0.88 – 0.97 for time carrying a weighted basket.
Functional obstacle course (mean of four trials) comparing the C-leg® and non-microprocessor controlled (NMC) prostheses with hands free and carrying a 4.5 kg (10 lb) basket (n = 10).
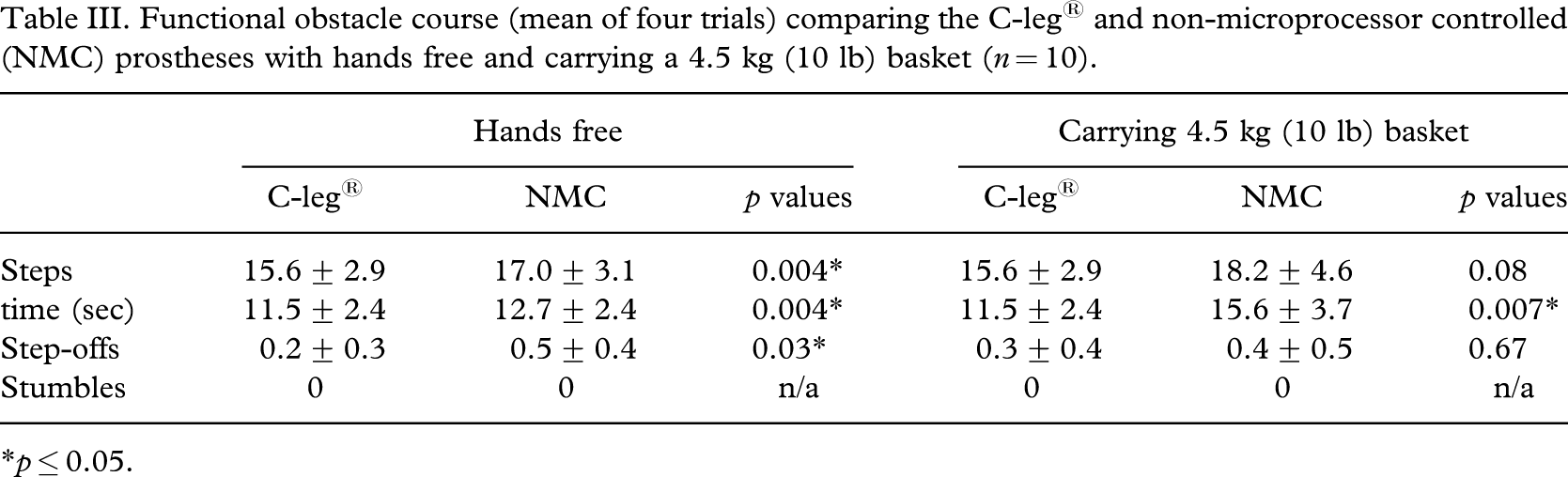
∗p ≤ 0.05.
Quality of life survey
Table IV depicts the SF-36v2™ quality of life scale values for use of the C-leg®. Scores on a quality of life index for subjects using the C-leg® were above the mean for norms for limitation in the use of an arm or leg, equaled the mean for the general United States population for the PCS and were above this mean for the MCS.
SF-36v2™ Quality of life scale values∗ associated with wearing the C-leg® (n = 13).
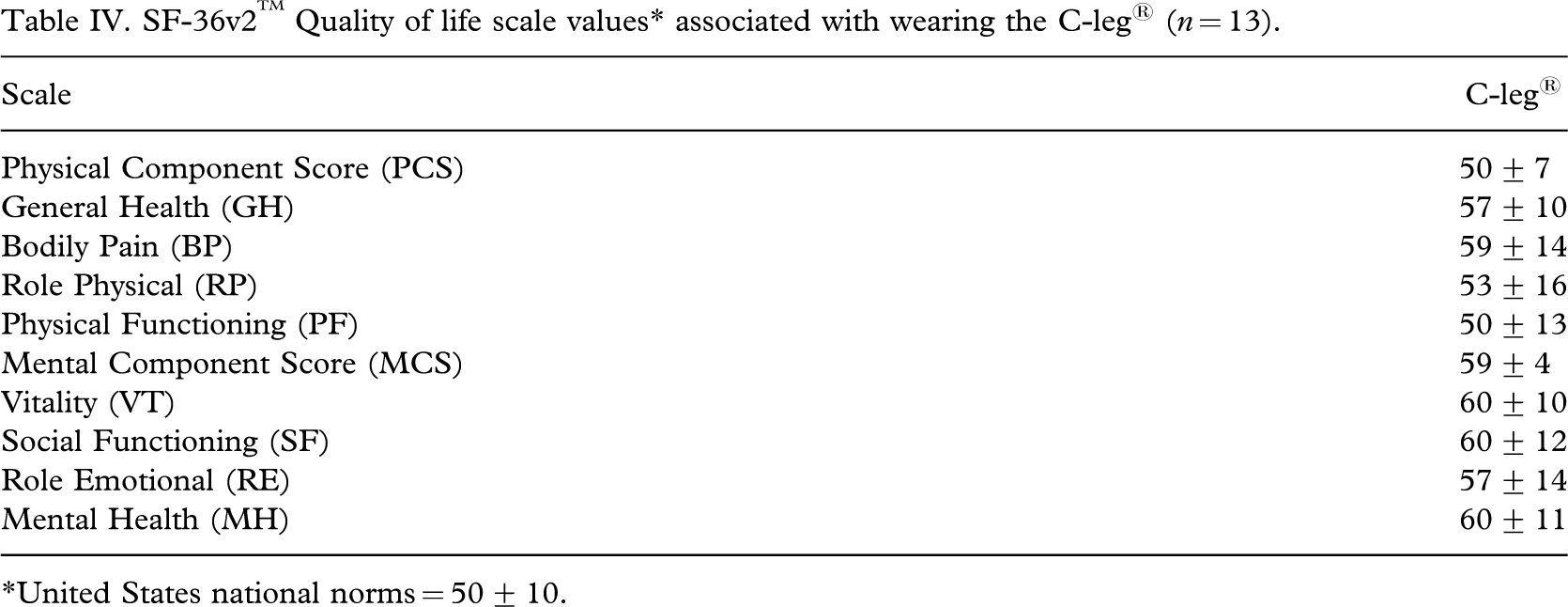
∗United States national norms = 50 ± 10.
Discussion
The authors' findings of heart rate at a typical pace of 49 ± 15 m/min of 102 bpm for both prostheses were lower than those of Jaegers et al. (1993) who found a heart rate of 116 bpm at 50 m/min. Likewise, the results at a fast pace of 70 ± 20 m/min of 103 (C-leg®) and 104 ± 15 bpm (NMC) were lower than the 134 bpm Jaegers et al. (1993) found at 75 m/min. The lower heart rate values found in the present study may reflect the high fitness level of the subjects. The lack of statistically significant differences in heart rate between prostheses was unexpected. Due to the advanced properties of the C-leg®, the authors anticipated the trend toward significantly lower heart rate with the C-leg®. The unfamiliarity and perhaps resulting anxiety of using the treadmill may have increased heart rate at a typical pace. In this study, typical pace was always measured first. At a faster pace, the subjects may have become somewhat more used to the treadmill and did not show the same increase in heart rate. This sympathetic effect was not seen when oxygen consumption was analysed since anxiety would have more of an effect on heart rate compared to oxygen consumption.
Predicted oxygen consumption (ml/kg/min) for able-bodied individuals walking at 0% grade over level ground can be calculated using the formula: VO2 = 0.1 ∗ speed + 3.5 (Franklin, 2000). Using this formula, oxygen consumption prediction for the subjects should average 8.3 ml/kg/min at a typical pace (49 ± 15 m/min) and 10.4 ml/kg/min at a fast pace (70 ± 20 m/min). The authors found an increase in oxygen consumption from these projected norms at a typical pace for the C-leg® of 55% and for the NMC prostheses of 67%. For a fast pace, the C-leg® had an oxygen consumption increase from the projected norms of 54% and for the NMC, an increase of 65%. These increases are greater than those found by Chin et al. (2003) at similar paces, a 31.1% increase at 50 m/min and 24.1% increase at 70 m/min. These differences may be due to the treadmill that was used for ambulation while Chin et al. used level walking over ground. The treadmill did not replicate the subjects' natural surroundings. In fact, several subjects stated this was their first time on a treadmill. The self-selected typical and fast paces varied widely in this study. For example, the fast pace of subject 2 was the same as the typical pace of subject 1. Some subjects felt that the treadmill was an artificial, less familiar environment resulting in a slower walking pace compared to regular level ground ambulation.
The differences in oxygen consumption between the C-leg® and NMC prostheses at both comfortable and fast paces were statistically significant but showed small differences. Nonetheless, these small differences when accumulated over a day may represent an important quantity of energy saved and result in less fatigue. The C-leg® was designed for irregular surfaces and this viewpoint was echoed by several subjects who stated the biggest advantage of the C-leg® was the stability it offered on uneven surfaces. In order to better judge whether the C-leg® decreased the energy cost of ambulation in a functional environment, future studies should include activities in which subjects traverse uneven surfaces, inclines, and stairs.
It appears from the data in Table II that walking at a typical pace (49 m/min) was somewhat inefficient while walking at a fast pace (70 m/min) was more efficient, i.e., there was lower oxygen consumption at a fast pace compared to a typical pace. The results of oxygen consumption at a fast pace of 0.23 ml/kg.m for the C-leg® and 0.25 ml/kg.m for the NMC were similar to the 0.25 ml/kg.m found by Waters et al. (1976) of individuals with trans-femoral amputation due to traumatic cause. However, subjects in the present study walked at a quicker pace of 70 m/min compared to the 52 m/min in the Waters et al. (1976) study. This difference may be due to the increased efficiency and/or higher fitness levels of subjects in the present study. Individuals with trans-femoral amputations choose slower typical walking paces as compared to able-bodied individuals (Jaegers et al. 1993). The difference in energy cost of ambulation is further amplified when energy cost is expressed as ml/kg.m. For example, the energy cost for able bodied individuals ambulating at their most efficient walking pace, which is very close to their self-selected walking pace, can be estimated to average 0.16 ml/kg.m from the data of Jaegers et al. (1993). As Table II indicates, the subjects in the authors' study consumed 0.29 ± 0.09 and 0.30 ± 0.09 ml/kg.m while walking at their typical pace with the C-leg® and NMC prostheses respectively. These values represent 81% and 88% higher values compared to able-bodied individuals.
The time necessary to complete the SWOC was higher for both prostheses compared to the mean 10.2 sec under hands free conditions and the 12.4 sec for carrying a weighted basket for able-bodied adults found by Taylor and Gunther (1998) (Table III). However, statistically significant differences were found showing fewer numbers of steps with hands free and less time under both conditions for the C-leg®. Based on these findings, the C-leg® may provide increased functional mobility and ease of performance in the home and community environment. The high test-retest reliability among the four trials for number of steps and time indicates that the SWOC is a reliable measure to use with subjects with trans-femoral amputation.
In this study, the protocol was developed to test each individual who had a functional and available C-leg® and NMC prosthesis in order to gain insight into potential differences between prosthetic designs. This protocol allowed for a repeated measure comparison which was advantageous for detecting potentially small, but clinically relevant differences. Another type of protocol could have involved two separate groups of subjects each with only one type of prosthesis. However, the two subject group protocol would require a much larger sample because of the large variability in the data that exists between individuals for these functional measures. There are additional protocols as well, but they all have inherent disadvantages with regards to this study population. Even in light of this, the protocol used in this study had limitations. The use of a variety of existing prostheses for comparison may have introduced potential confounding variables. For example, the sockets of the previous but still functional prostheses may not have fit as intimately or may not have been suspended as securely as the C-leg® prosthesis. In addition, the biomechanical differences between the various NMC knees may have affected the subjects' functional performance. Therefore, caution should be used when interpreting the apparent differences between these two groups.
The SF-36 mean for the general United States population is 50 for each category with a standard deviation of 10. The mean for norms for limitation in the use of an arm or leg for the US population is 38 for PCS and 46 for MCS (Ware 2004). The results for PCS for use of the C-leg® were 50 which are higher than the mean for individuals with limitation and equal to the general population mean. The results for MCS for use of the C-leg® were 59 which are higher than both the general US population and those with limitation means. Likewise, these results are higher than those of other studies involving individuals with amputation (Smith et al. 1995; Dougherty 2003; Hagberg and Branemark 2001). The higher scores seen for both PCS and MCS may be due to the high functional level of subjects in this study compared to the norms for individuals with limitation and the subjects with amputation of other studies (Smith et al. 1995; Dougherty 2003; Hagberg and Branemark 2001). Higher scores in every category of the SF-36v2™ compared to the general US population mean (except for an equal score for the PCS) suggest subjects, regardless of amputation, perceived a positive mental outlook and less of an impaired quality of life.
Conclusion
This study compared the C-leg® with various NMC prostheses in the areas of energy expenditure and obstacle course negotiation. In addition, a quality of life survey of use of the C-leg® was compared to national norms. Statistically significant differences were found in oxygen consumption between the use of a C-leg® and various NMC prostheses at both typical and fast paces with the C-leg® showing decreased values. Use of the C-leg® resulted in a statistically significant decrease in the number of steps and time to complete the obstacle course. Based on oxygen consumption and obstacle course findings, the C-leg® may provide increased functional mobility and ease of performance in the home and community environment. Scores on the quality of life index for use of the C-leg® were above the mean for norms for limitation in the use of an arm or leg, equal to the mean for the general US population for the PCS and were above this mean for the MCS. Questionnaire results suggest a minimal quality of life impairment for this cohort of individuals with amputation.
Footnotes
Acknowledgements
Assistance of the following former physical therapy students in data collection is appreciated: Aimee Bachand, Pattie Cannella, Felix Cheng, Molly Ferris, Adam Rufa, Stephanie Partis, Dave Wetherby, and Sarah Wolff. Appreciation is also extended to the 13 subjects involved in this study and to the New York Physical Therapy Association and Otto Bock Healthcare for partial research support for this project.