
Abstract
Background:
The International Committee of the Red Cross supports a worldwide program of prosthetic fitting and rehabilitation. In this context, a prosthetic foot was developed and widely distributed in least developed countries.
Study design:
Prospective, randomized, double-blind, controlled study.
Objective:
To compare patient satisfaction and energy expenditure during ambulation between a low-cost prosthetic foot designed with a polypropylene keel (CR-Equipements™ solid ankle cushion heel, International Committee of the Red Cross) to a well-recognized solid ankle cushion heel foot with a wooden keel (solid ankle cushion heel foot, Otto Bock).
Methods:
A total of 15 participants with unilateral transtibial amputation were evaluated using the two prosthetic feet in a randomized prospective double-blind crossover study. Main outcomes were patient satisfaction questionnaires (Satisfaction with Prosthesis Questionnaire and prosthetic foot satisfaction) and energy expenditure (oxygen consumption—mL/kg/min, oxygen cost—mL/kg/m, and heart rate—bpm).
Results:
There were no significant differences between the two prosthetic feet for satisfaction and energy expenditure.
Conclusion:
The low-cost solid ankle cushion heel foot with polypropylene keel provides comparable satisfaction and similar energy expenditure as the solid ankle cushion heel foot with wooden keel.
Clinical relevance
The results of this study support the application and widespread use of the CR-Equipements™ solid ankle cushion heel foot. From a cost-effectiveness standpoint, patients are well satisfied and exhibit similar outcomes at a substantially lower cost.
Keywords
Background
Since 1998, the International Committee of the Red Cross (ICRC) has been supporting a worldwide program of prosthetic fitting and rehabilitation. This has been carried out using an ICRC designed solid ankle cushion heel (SACH) foot produced at low cost by CR-Equipements™ (CRE) and known as CRE SACH foot. The CRE SACH foot is available in all orthopedic centers supported by the ICRC. Approximately 45,000 units are produced per year which makes this prosthetic foot the most widely distributed foot in the world.
Despite the worldwide distribution of the CRE SACH, only a few studies have evaluated its performance. The durability of the CRE SACH foot has been studied in the field by the ICRC leading to an improvement in the durability of this prosthetic foot.1–3 The biomechanical performance of the CRE SACH foot has been evaluated in one study. 4 This study demonstrated that the CRE SACH foot showed improved gait biomechanics as compared to the SACH foot with a higher percentage of the stance phase on the affected side, greater ankle range of motion, greater power absorption and power generation at the ankle, and a more symmetric gait. Based on these results, we can assume that the CRE SACH foot as compared to Otto Bock SACH foot has better flexibility and improved capacity for storing and returning energy. Indeed, it has been demonstrated that the use of energy storing feet improves the walking performance of transtibial amputees. 5 Although the CRE SACH is not an energy storage and return (ESAR) foot, the polypropylene keel could improve the capacity to flex, to adapt to different surfaces (slopes), and return energy as compared to the Otto Bock SACH foot where the keel is made of wood. Therefore, CRE SACH might require less energy to walk and could improve patient satisfaction as compared with the Otto Bock SACH foot.
To the best of our knowledge, there are no studies comparing the CRE SACH foot with other prosthetic feet with regard to patient satisfaction and energy expenditure. To evaluate prosthetic feet, numerous studies have used the Otto Bock SACH foot as a reference4,6–18 because the SACH foot is the most frequently used and evaluated. Energy expenditure is considered as an important outcome to evaluate and compare prosthetic feet.19,20 Moreover, Rietman et al. 19 stated that in addition to assessing impairments with instrumented gait analysis, a subjective opinion from the patient remains crucial.
Thus, our objective was to compare patient satisfaction and energy expenditure during gait with these two prosthetic feet.
Based on the results of the previously mentioned study 4 showing improved biomechanics of gait with the CRE SACH foot as compared to the SACH foot, our hypothesis was that there would be less energy expenditure and better satisfaction with the use of the CRE SACH foot.
Materials and methods
Patients
A total of 15 participants were recruited for the study at the Geneva University Hospitals between April 2010 and March 2012. All patients who had undergone an amputation following a traumatic episode and living in the cantons of Geneva or Valais (Switzerland) were first asked by letter and then by telephone to participate in this study. To be included in the study, participants had to be older than 18 years of age with a traumatic unilateral transtibial amputation. They also had to be ambulating for more than 1 year with a prosthesis without an assistive device. Only those with traumatic unilateral transtibial amputations were selected for this study because most amputees supported by the ICRC are war victims, and the main cause of amputation is antipersonnel mines. 21 Those individuals with an amputation related to vascular disease or those having co-morbidities affecting their gait and/or balance were excluded.
This study was approved by the Cantonal Human Research Ethics Commission of Geneva University Hospitals. All of the study participants completed an informed consent procedure before participating in this investigation.
Protocol
The protocol has already been described in a previous study, 4 and the main aspects are repeated here. All study participants first had a familiarization session. Then, a sequence order of using the CRE SACH and Otto Bock SACH were allocated to each participant in a randomized way. The randomization sequence was generated using MATLAB 2008b (MathWorks, Natick, MA, USA) (randomizing with balance permutation) and was concealed until interventions were assigned. The research coordinator held this sequence independently, enrolled participants, and randomized them to one of the two sequences. The participants were evaluated in two evaluations, one involving the use of the Otto Bock SACH foot and one involving the use of the CRE SACH according the randomized sequence. The timeline of evaluations is summarized in Figure 1. The time period between each evaluation was 1 week.22,23 At the end of the familiarization session, patients received the first allocated foot. Following a 1-week acclimatization and subsequent testing, the second prosthetic foot was provided. A further week of acclimatization and another testing session concluded the protocol. Two qualified prosthetists performed all of the static and dynamic alignments of the prostheses, although each study participant consistently interacted with the same prosthetist. The study participants were blinded throughout the execution of the study protocols, and the evaluators were blinded until the end of the data analyses. To ensure that neither the participants nor the evaluators could recognize the types of foot prostheses that were used at a particular time, the study’s prosthetists created a cosmetic covering used to cover both of the experimental foot types. Moreover, to avoid the confounding influences of shoes during the gait evaluations, all of the study participants wore the same standardized flat shoes throughout the study.
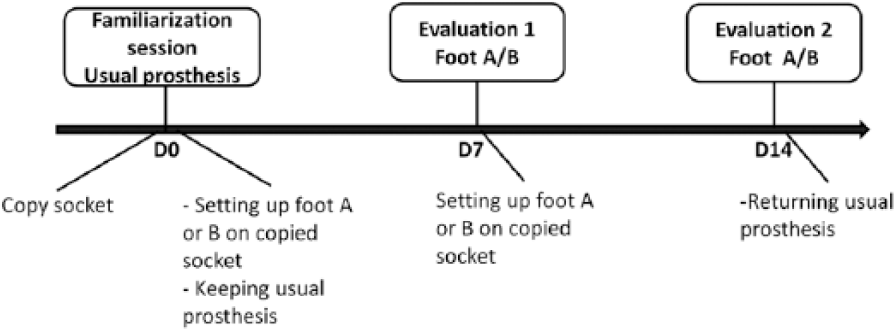
Timeline of the protocol.
Description of prosthetic feet
The newly made prosthesis retained the usual polyethylene foam soft socket or the silicone or polyurethane liner, but the hard socket was a copy of the usual one made by Orthochoc, Proteor™ (Dijon, France).
The Otto Bock SACH foot used was the 1S90 = side size with the same cushion heel (all patients weighed less than 100 kg). It is a combination of a contoured core and functional foam with a wooden keel. It is light, durable, and can support up to 125 kg of load. The CRE SACH foot was the CRE 595.size.side. These two feet are the same type of prosthetic foot, except that the keel of the CRE SACH foot is made of polypropylene and can support up to 135 kg of load. For the same size (28 cm), Otto Bock SACH foot is lighter than CRE SACH foot (609 vs 772 g).
Evaluation of patient satisfaction
Participant satisfaction was evaluated with (1) Satis-faction with Prosthesis Questionnaire (SAT-PRO), a self-administrated questionnaire validated in French, 24 and (2) a specific questionnaire concerning participant satisfaction with the prosthetic foot itself.
The SAT-PRO is a 15-item questionnaire designed to evaluate global satisfaction with the prosthesis. As described in the original publication, 25 a score in percentages can be computed for each participant who answers 10 of 14 items, where the item concerning walking aids was not used because patients using aids for ambulation were excluded from participation in the study.
The specific questionnaire, called “prosthetic foot satisfaction questionnaire”, was developed to specifically address participant satisfaction with the prosthetic foot itself (Table 1). The questionnaire was developed based on the orthotics technician’s experience in his daily activity with patients. Questions were chosen to reflect satisfaction with comfort in different situations of daily life and were based upon the Prosthesis Evaluation Questionnaire (PEQ). 26 Since only the foot was replaced in the prosthesis, we focused on the prosthetic foot and on the comfort it provided. For this separate seven-item questionnaire, each item was rated between 1 (“very satisfied”) and 4 (“very dissatisfied”). In the same fashion as with the SAT-PRO, a score in percentages was computed for the prosthetic foot satisfaction questionnaire. The scores were respectively transformed in percentages: 1–0%, 2–33.3%, 3–66.6%, and 4–100%. An average score, representing the mean of the seven items, was computed for each participant. The internal consistency of the prosthetic foot satisfaction questionnaire was good, estimated with Cronbach’s coefficient 27 at 0.89.
Prosthetic foot satisfaction questionnaire.
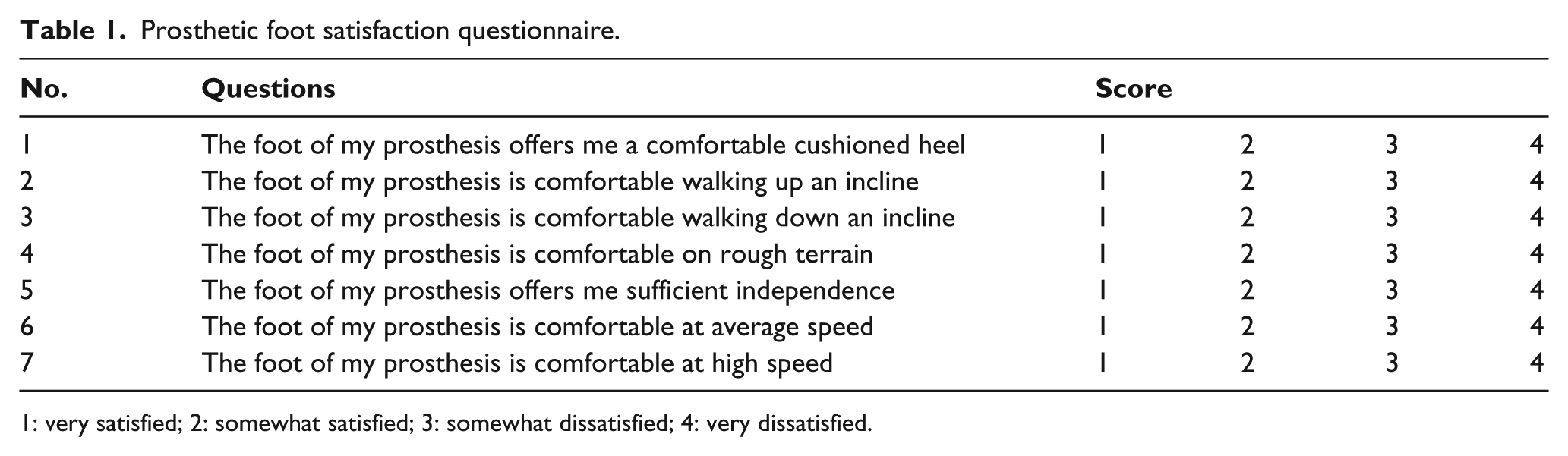
1: very satisfied; 2: somewhat satisfied; 3: somewhat dissatisfied; 4: very dissatisfied.
Evaluation of energy expenditure
Energy expenditure was recorded during a treadmill walking test using the Medgraphics CPX metabolic cart (St. Paul, MN, USA). Prior to testing, the metabolic cart was calibrated according to manufacturer guidelines including flow transducer calibration with a 3-L syringe and gas analyzer of known concentration. Participants were instructed to avoid coffee, energy beverages, or alcohol during the 24 h prior to the evaluations. The protocol was similar to a previous study, 28 except that the walking time was increased to 10 min in order to be sure that the participants reached a steady state. Thus, the protocol included 5 min of rest in a sitting position, 10 min of walking, and 5 min of cooling down, for a total of 20 min. The protocol was repeated at the same hour (±1 h) of the day and under the same conditions for all sessions. The first session was for accommodation where the participants learned to walk on a treadmill and establish a comfortable gait pattern. The walking speed was fixed for each participant and for the three sessions, as was established during the first session at a self-selected comfortable speed. The most relevant parameters to describe energy expenditure in participants with lower-limb amputation were selected from a systematic review 20 and utilized for data analysis as follows: oxygen consumption (VO2), oxygen cost (OC), and heart rate (HR). 28 VO2 is expressed in milliliters per minute per kilogram of body weight (mL/min/kg). OC is expressed in milliliters of oxygen consumed per kilogram of body weight per meter walked (mL/kg/m) and was calculated using the formula: “oxygen consumption (mL/min/kg)/speed (m/min).” For a given task (e.g. walking), lower values of VO2, OC (considering the walking speed), and HR indicate greater movement efficiency. HR was recorded simultaneously using the Polar® monitoring system (Polar Electro Oy, Kempele, Finland).
All breath-by-breath gas exchange data were filtered using a moving average filter, keeping five of seven values and removing the highest and the lowest ones. 29 The average of the 13th and 14th min of the testing protocol (i.e. corresponding to the two penultimate minute walks) was calculated for each parameter and compared between the CRE and Otto Bock SACH feet.
Statistical analysis
Since the sample size was small and the HR parameter was not distributed normally (Kolmogorov–Smirnov test), we decided to use non-parametric tests. Performance achieved for both feet regarding participant satisfaction and energy expenditure were assessed using the Wilcoxon matched-pairs test. Median and interquartile range were reported throughout the results. To reduce the risk of Type I error, a Bonferroni corrected alpha level of p = 0.01 (alpha divided by number of tests per) was used to determine a significant difference between prosthetic feet.
Results
A total of 15 participants (12 men and 3 women) with a mean age of 46.3 ± 12.7 years (range, 26.9–73.4 years) completed all evaluations and composed the study group. Participant characteristics are presented in Table 2.
Participant characteristics.
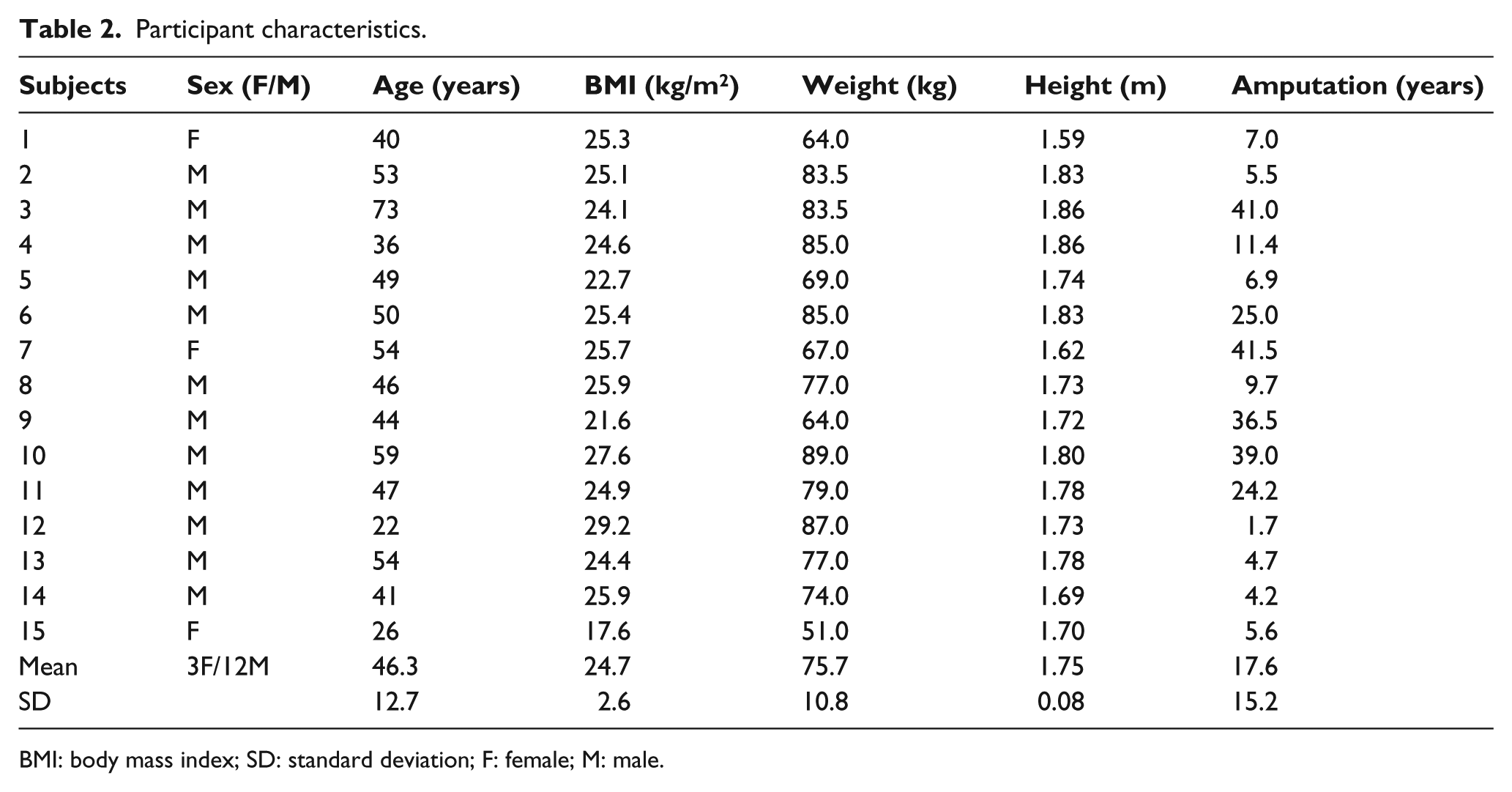
BMI: body mass index; SD: standard deviation; F: female; M: male.
Satisfaction
The SAT-PRO revealed satisfaction greater than 70% for both prostheses (CRE SACH foot: 76% (64%–85%), Otto Bock SACH foot: 71% (58%–84%)), with no significant difference between the two prosthetic feet (Figure 1) (p = 0.64, Z = −0.471).
The results of the prosthetic foot satisfaction questionnaire showed no significant differences between the two prosthetic feet (Figure 1) (p = 0.117, Z = −1.570).
Energy expenditure
One participant had data missing for the assessment of the CRE SACH foot due to problems during recording, thus leaving 14 participants for evaluation of energy expenditure.
Participants selected comfortable walking speeds ranging from 3.6 to 5.5 km/h (average, 4.62 ± 0.48 km/h). The walking speed selected at the familiarization session was retained for the assessment of the two different feet. The results are detailed in Figure 2. No significant differences were observed between feet for the VO2 (p = 0.64, Z = −0.471), OC (p = 0.59, Z = −0.534), and the HR (p = 0.31, Z = −1.022) (Figure 3).
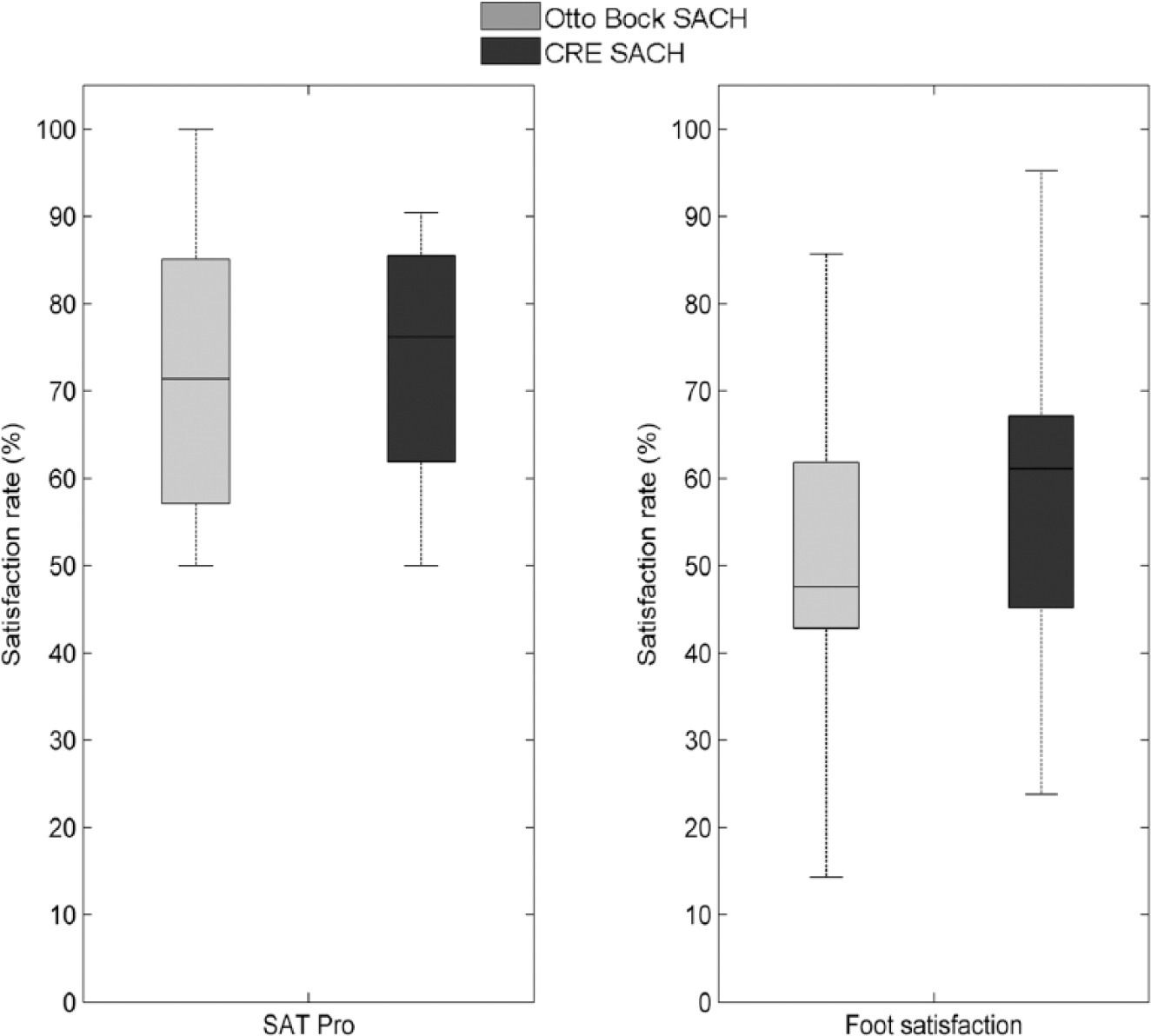
Satisfaction rate according to each foot.
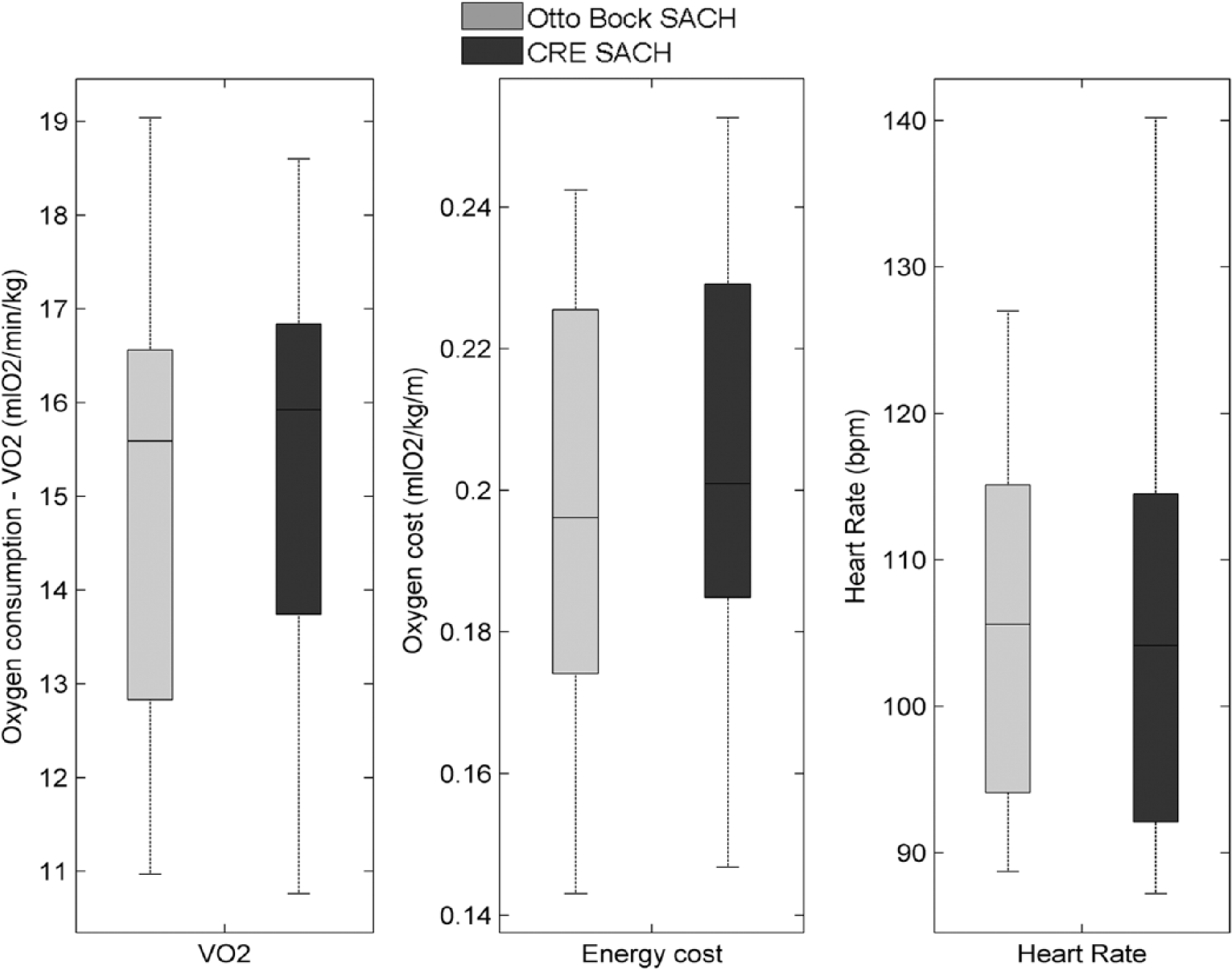
Energy expenditure during walking.
Discussion
Our objective was to compare the CRE SACH foot with the Otto Bock SACH foot. To the best of our knowledge, this is the first study assessing these feet with regard to satisfaction and energy expenditure during ambulation.
The SAT-PRO questionnaire showed that patients had an overall satisfaction rate greater than 70% with both feet analyzed, with no difference between the two feet. These results could be due to an equivalence between the two feet or the differences between the two feet are too small to be detected by the participants and/or the questionnaire.
It is well accepted that metabolic energy expenditure during ambulation for lower-limb amputees depends upon the level of amputation and the different prosthetic components. 30 In our study, during comfortable walking speed, the differences between the two prosthetic feet for transtibial amputees were not statistically significant. In other studies comparing prosthetic feet, energy expenditure was rarely significantly different between feet, even between conventional prosthetic feet and ESAR feet.20,31,32 Therefore, our hypothesis that the CRE SACH foot might require less energy to walk was certainly too optimistic. Given that there were no differences in satisfaction and energy expenditure between the Otto Bock and CRE SACH feet, the decision between the two can be based on other considerations such as cost and durability of the prosthetic feet. In our country, the Otto Bock SACH foot costs CHF 272, while the price of the CRE SACH foot is CHF 54. This is a very substantial consideration in light of the fact that the ICRC particularly supports a worldwide program of prosthetic fitting and rehabilitation in Least Developed Countries. The life span of the prosthetic components is also an important aspect that was not considered in this study. The life span of the CRE SACH foot has been studied and improved by the ICRC 2 but has not been compared to the Otto Bock SACH foot. A future study is needed to compare the durability of the prostheses.
We are aware that this study has some limitations. First is the recruitment of participants in a more economically developed country, whereas the main destination for use of the CRE SACH foot is least developed countries. We can speculate that the use of these feet and the expectations of the traumatic amputees differ as to the type of country. However, this choice was made to facilitate the evaluation process and ethical procedures. We acknowledge that a further study should be performed in least developed countries to validate these findings. Another limitation is the low number of participants (n = 15) due to the difficulty to locating traumatic amputees in more economically developed countries. Again, this drawback could be eliminated by a further study performed in least developed countries.
The use of a non-validated specific questionnaire to estimate the satisfaction of the prosthetic foot can also be a limitation. However, we found a good internal consistency.
The strengths of this study include the protocol we developed using a familiarization session, randomization of the order of the feet, the duration of wearing the prosthetic foot (7 days, as recommended to evaluate prosthetic foot22,23), and the blinding of participants, assessors, and statistician. Lack of these points is reported to be a bias one must avoid when reviewing and evaluating amputees.20,23 Another strength of this study was the inclusion of only post-traumatic below knee amputees. We believe that this population is able to assess prosthetic feet with greater precision than persons with a dysvascular amputation because they have different health-related profiles. 33 Persons with a traumatic amputation are more active (they walk longer periods 34 ), have better physical function, 33 and have less sensory alterations. 35 Moreover, patients who benefit from the prosthetic feet provided by the ICRC are mostly traumatic amputees living in least developed countries and are mainly causalities of war. As recommended in a Cochrane review, 23 function comparisons between different prosthetic components should be tested according to the level of activity, intended use of patients (traumatic or dysvascular), and level of amputation (below or through-knee amputation).
The results of this study highlight that the CRE SACH foot provides comparable outcomes in terms of satisfaction and energy expenditure at a lower cost.
Conclusion
This study demonstrated that the CRE SACH foot designed with a polypropylene keel provides comparable satisfaction and similar energy expenditure as the Otto Bock SACH foot designed with a wooden keel. In addition, this foot is considerably less expensive than the Otto Bock SACH foot, an important ethical issue in the context of humanitarian aid provided by the ICRC.
Footnotes
Author contribution
Concept and design of study: AL, AS, MA.
Recruitment of the participants: AL, OB.
Acquisition of data: AL, AS, KT.
Analysis and interpretation of data: AL, AS, KT.
Drafting the article: AL, KT, AS.
Revision of the article: AL, AS, MA, RS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Clinical Research Center University Hospital and Faculty of Medicine (grant/award number: PRD 09-I-15).