
Abstract
Background:
Individuals with unilateral lower-limb amputation (LLA) have altered structure and physiology of their lower limbs which impairs their balance, mobility, physical function and participation in physical activities. As part of (re)habilitation, focus is given to improving gait and balance in order to enhance overall mobility, function, self-efficacy, and independence. However, the relationships amongst body impairments and physical activity limitations remain unclear, particularly in the pediatric population.
Objective:
To provide an examination of the relationships among balance and mobility measures in children with unilateral lower-limb amputation and able-bodied children.
Study design:
Cross-sectional prospective comparative pilot study.
Methods:
Spatiotemporal gait parameters and standing postural control were evaluated in children with lower-limb amputation (n = 10) and age-matched able-bodied children (n = 10) in a laboratory-based setting. Clinical tests for mobility and balance consisted of the 10-m walk test, the 6-min walk test, and the Community Balance and Mobility scale. Energy expenditure was estimated during the 6-min walk test using the Physiological Cost Index. Analysis included comparing variables between able-bodied and lower-limb amputation groups, as well as examining the correlations among them.
Results:
Walking speed, distance, and functional balance (p < 0.05) were significantly diminished in children with lower-limb amputation compared to able-bodied children. For children with lower-limb amputation, reduced energy expenditure was associated with narrower step width and more symmetrical gait; better postural control and balance were associated with faster walking speeds (p < 0.05).
Conclusion:
A greater clinical understanding of gait and balance deficits in this population may help to improve rehabilitation outcomes and overall functional mobility.
Clinical relevance
Improved understanding of deficits in children with lower-limb amputation (LLA) may lead to more targeted interventions and facilitate clinical decision-making in rehabilitation settings for this population. The findings contribute to the limited literature and provide a basis to further examine suitable clinical outcome measures to be used in children with LLA.
Keywords
Background
Individuals with unilateral lower-limb amputation (LLA) experience altered structure and physiology of their lower limbs which impairs their mobility, balance, and physical function.1,2 Reduced musculature and sensory feedback in the affected limb result in decreased postural control, slower and abnormal walking patterns while using a prosthetic limb, and increased physiological energy costs.3,4 Furthermore, balance impairments in adults with LLA have been shown to lead to an increased risk of falls. 5 Thus, individuals with LLA require considerable rehabilitation to address these physical limitations and optimize function in daily life.6,7 As physical capacity can be influenced through training, 7 rehabilitation post-LLA focuses on improving range of motion, muscular strength, cardiovascular fitness, as well as re-training gait and standing balance with a prosthesis. 8 Improvements in gait and balance are important to enhance overall mobility, function, self-efficacy, and independence. However, the relationships among body impairments and physical activity limitations remain unclear, particularly in the pediatric population.
The International Classification of Functioning, Disability and Health (ICF) provides a framework for classifying the health components of functioning and disability. 9 Recent work that focused on the application of the framework in the rehabilitation of individuals with LLA comprised detailed examinations of LLA outcome measurement instruments, which provide the basis for understanding impairments in body structure and function and their influence on the execution of activities by individuals with LLA.2,10 In particular, at the body structure or function level of the ICF, measures for LLA have been categorized into mental, sensory, cardiovascular, and neuromusculoskeletal and movement; the latter category includes assessment of gait and postural control. 10 Typically measured using instrumented gait analysis, individuals with LLA, including children, demonstrate spatiotemporal, kinematic, and kinetic deviations as well as gait asymmetries such as longer stance time and increased loading of the intact limb as compared to the prosthetic limb.3,11–14 The pediatric literature has also identified higher energy cost in children with below-knee amputations when walking at a fixed speed as compared to able-bodied (AB) children. 15 Those with LLA experience slower gait speeds compared to AB individuals,6,11,16 as well as deterioration of postural control post-amputation which is associated with poor balance.10,17,18
A commonly used approach for the characterization of postural control involves the examination of center-of-pressure (COP) excursions during a quiet standing task on a force platform; higher postural sway excursions are associated with diminished postural control. 17 Studies of gait and balance in individuals with LLA further reveal compensations in balance through the sound limb and an increased base of support via greater step width when compared to AB.19,20 Therefore, assessing gait quality and postural control is central to developing an understanding of the balance and mobility deficits at the body structure and function level for individuals with LLA.
In contrast, the activity level of the ICF refers to the ability to complete whole-bodied tasks. Outcome measures used to evaluate activity include walk tests, mobility grades, and indices that involve observational, interview, questionnaire, and proxy report formats. 2 With the exception of the walk tests, including the 10-m walk test (10mWT) and the 6-min walk test (6MWT), the majority of instruments were designed for the elderly, dysvascular subgroup, comprising the majority (>80%) of the entire LLA population. 21 Consequently, many of the instruments have strong ceiling effects when applied to younger individuals with LLA who have much higher levels of physical function. 2 Children possess balance and walking strategies that are uniquely different from adults,22–24 and therefore the lack of well-evidenced pediatric-specific measurement tools, along with studies that utilize them, is a considerable barrier toward our understanding of how physical impairments impact activity performance. This may be an important factor restricting the ability to make sound clinical treatment decisions and provide effective rehabilitation for children with LLA.10,25
Given the lack of published literature to inform our understanding of the balance and mobility performance in children with LLA, as well as the tools used in their measurement, the overall goal of this study was to explore a set of standardized measures of body function and activity for use in children with LLA. Specifically, we aimed to examine the relationships among these measures to determine which aspects of mobility and balance in children with LLA are potentially related and which measures may be most useful in detecting mobility and balance deficits. Given the paucity of such information in the current literature, we undertook an exploratory rather than hypothesis-driven approach, to ultimately help guide initiatives aimed at increasing the use of these measures in clinical practice, and contribute to future research involving children with LLA.
Methods
Study design
A quantitative prospective cross-sectional study was conducted to examine gait, balance, and mobility deficits among children with unilateral LLA as compared to AB children of similar ages.
Participants
A convenience sample of children with LLA was recruited from the outpatient prosthetics department of a university-affiliated pediatric rehabilitation hospital. Inclusion criteria included age between 5 and 16 years, unilateral LLA, experience using a prosthesis for mobility for a minimum of 3 years, and wearing their current prosthesis for at least 3 months. A comparison group of AB children without any neurological, developmental, or musculoskeletal condition was also recruited. Children were excluded if they had a cognitive impairment, a behavioral issue limiting their ability to follow multi-step instructions, or a co-morbidity limiting completion of study tasks as determined by medical and parent report. The research ethics boards of the pediatric rehabilitation hospital and the affiliated university approved the study protocol. Informed consent was obtained from parents/guardians and assent from the children.
Evaluation procedures
Wearing comfortable clothing and supportive footwear, each participant completed a single assessment session of approximately 2-h duration, which comprised the tests mentioned in Table 1. Demographics and participant characteristics were also recorded.
Study measures of body function or activity.
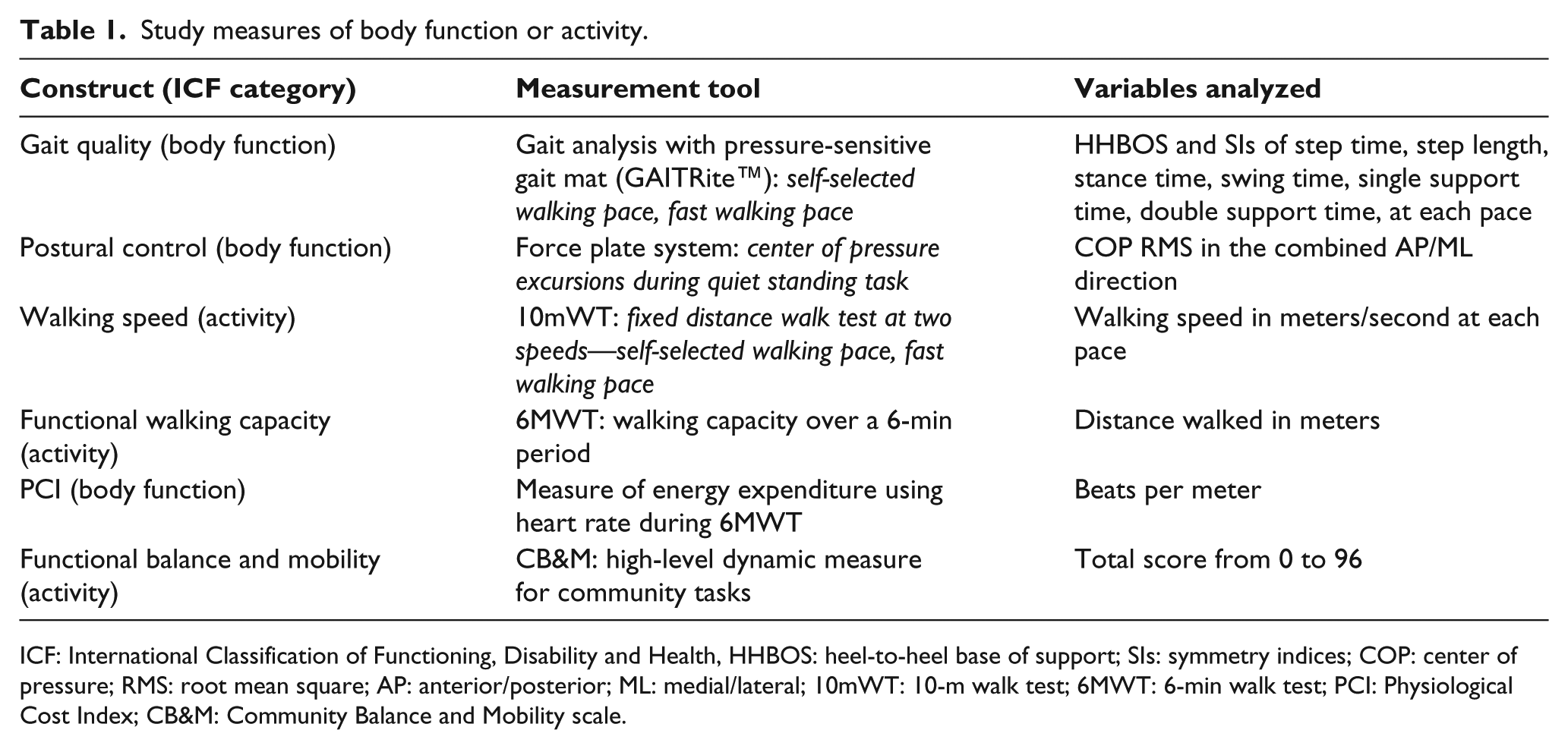
ICF: International Classification of Functioning, Disability and Health, HHBOS: heel-to-heel base of support; SIs: symmetry indices; COP: center of pressure; RMS: root mean square; AP: anterior/posterior; ML: medial/lateral; 10mWT: 10-m walk test; 6MWT: 6-min walk test; PCI: Physiological Cost Index; CB&M: Community Balance and Mobility scale.
Postural control was evaluated using a force plate system (Bertec; Nexus software Inc.; sampling frequency 1 kHz). Participants were instructed to step onto the force plate and adopt a comfortable standing position. They were free to select foot placement, including the stance width and foot angulation.17,26 Once the participants established their stance, adhesive tape was used to mark the foot position for consistency in subsequent trials. Participants were instructed to stand still with their arms by their sides and fixate on a visual target placed at eye level, 3 m straight ahead for 60 s.
17
This quiet standing task condition with eyes open was repeated three times. Force plate data were down-sampled to 120 Hz and low-pass filtered at a cut-off frequency of 12 Hz using a second-order Butterworth filter.
27
COP variables were calculated using MATLAB (The MathWorks, Inc.), and specifically the COP root mean square (RMS) was calculated by finding the resultant value (

where
Gait was then assessed using a 16-ft-long GAITRite mat system (CIR Systems, Inc.), to collect spatiotemporal gait parameters.6,29–31 Participants performed two walking conditions: (1) self-selected walking pace (SSW) and (2) fast walking pace (FW). Five trials of each walking condition were completed. Many of the parameters including step time and length, swing and stance times, and single and double support times were summarized in the form of symmetry indices (SIs), where zero values denote the greatest symmetry, calculated for amputee and AB groups, respectively, as


Walking speed was further assessed with the 10mWT, both SSW and FW. Evaluators administered the test based on a modified version of a previously documented protocol used in children. 32 Trials were timed using a standard stopwatch (Sportline, EB Sport Group©). Three trials were obtained at each pace.
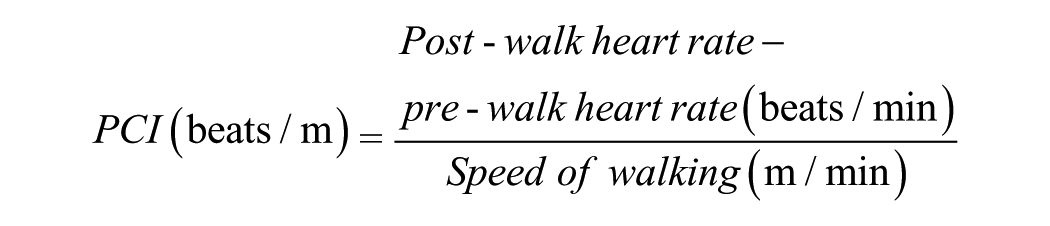
The 6MWT was used to assess functional walking capacity. 33 Evaluators followed a modified version of the protocol from the American Thoracic Society guidelines 34 and a similar protocol to the one used in children. 32 The 30-m straight walking course was set up in a corridor. Total distance walked was measured by tabulating the number of laps completed in the 6 min and using a standard measuring tape to determine the distance walked for partial lap. Trials were timed using a stopwatch, and heart rate measurements were taken pre-walking (resting heart rate) and immediately post-walk using a heart rate monitor with a chest strap and watch (Polar Electro Canada©) in standing. The Physiological Cost Index (PCI), a measure to estimate energy cost, was calculated as follows 15
The Community Balance and Mobility Scale (CB&M) was administered and scored by an experienced registered physical therapist using a pre-defined course. 35 This test includes 13 items of functional balance and mobility tasks of varying complexity, such as unilateral stance, tandem walking, hopping forward, walking and looking, and descending stairs. A summary score from 0 to 96 is computed, with a higher summary score reflecting a higher level of function. 35
Data analysis
For each participant, the average performance across trials for all variables on the GAITRite system and the speed during the 10mWT were calculated for each task condition. Variables in Table 1 were compared between children with LLA and AB children using an independent sample two-tailed t-test with statistical significance set at an alpha value of 0.05. 36 The Shapiro–Wilk test for normality determined that data were normally distributed. Relationships between variables outlined in Table 1 were analyzed using Pearson product-moment correlation coefficient since data were found to be normally distributed. The magnitude of the correlation coefficients for impairments and activities was interpreted as weak (r < 0.25), fair (r = 0.25–0.50), moderate (r = 0.50–0.75), or strong (r > 0.75). 37 SPSS software (version 19.0) was used for analysis.
Results
There were no statistically significant differences in gender, age, height, weight, or self-reported engagement in recreational activities between the groups when examining the sociodemographic and anthropometric characteristics of children with LLA and AB children (Table 2). Significant differences were found in a number of study measures between the two groups of children (Table 3). Specifically, lower walking speeds from the 10mWT, shorter distance walked during the 6MWT, and lower CB&M scores were measured for the children with LLA. Furthermore, children with LLA had significantly greater step width when walking and greater asymmetry in step length and swing time. Also, as seen in Table 3, differences exist in subgroups categorized by amputation level. Most markedly, the transfemoral group appears to perform differently (at a lower level) when compared to typically developing children for PCI and step, stance, and swing time symmetry.
Participant characteristics.
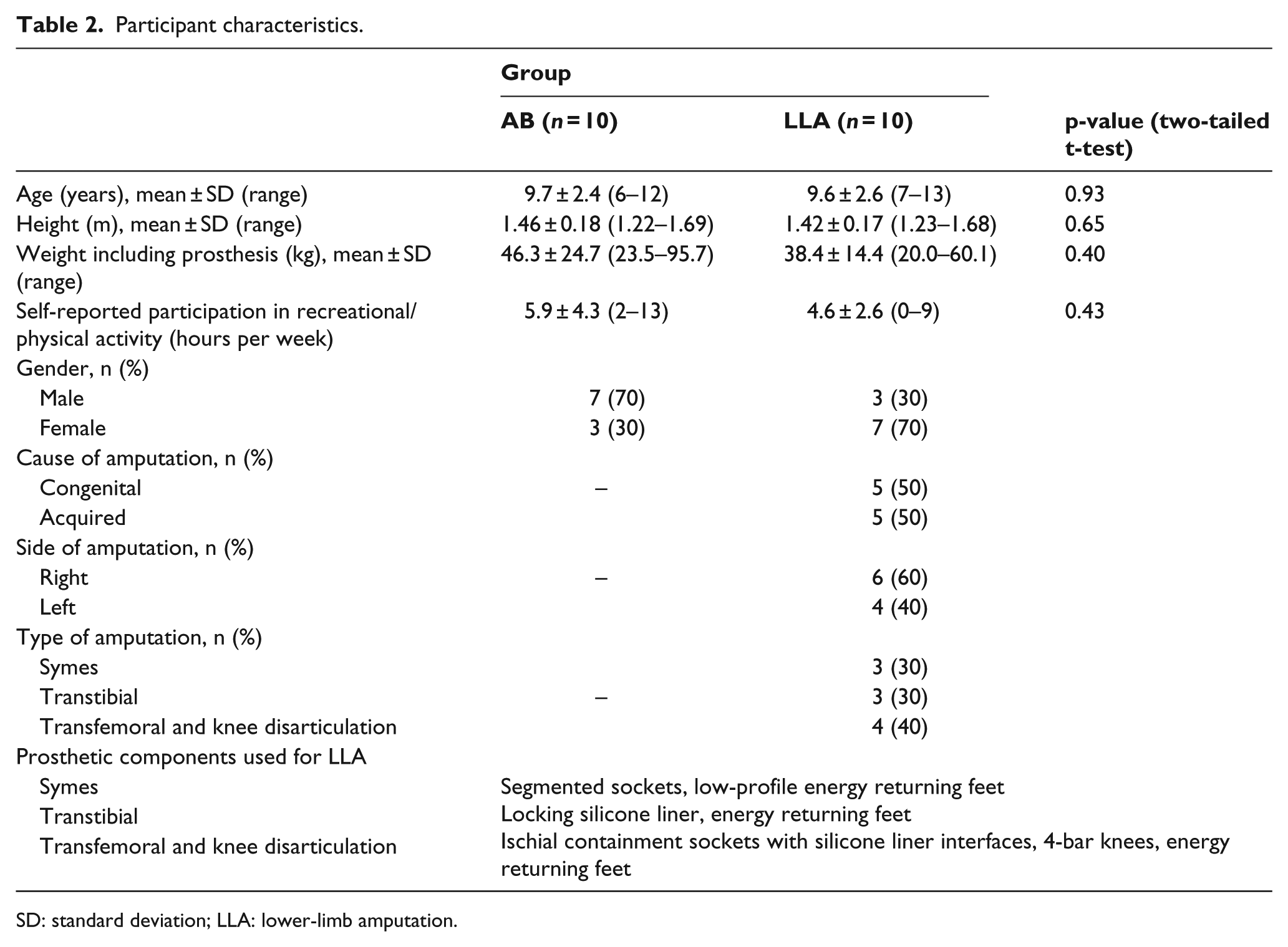
SD: standard deviation; LLA: lower-limb amputation.
Performance of AB children and children with LLA on study measures.
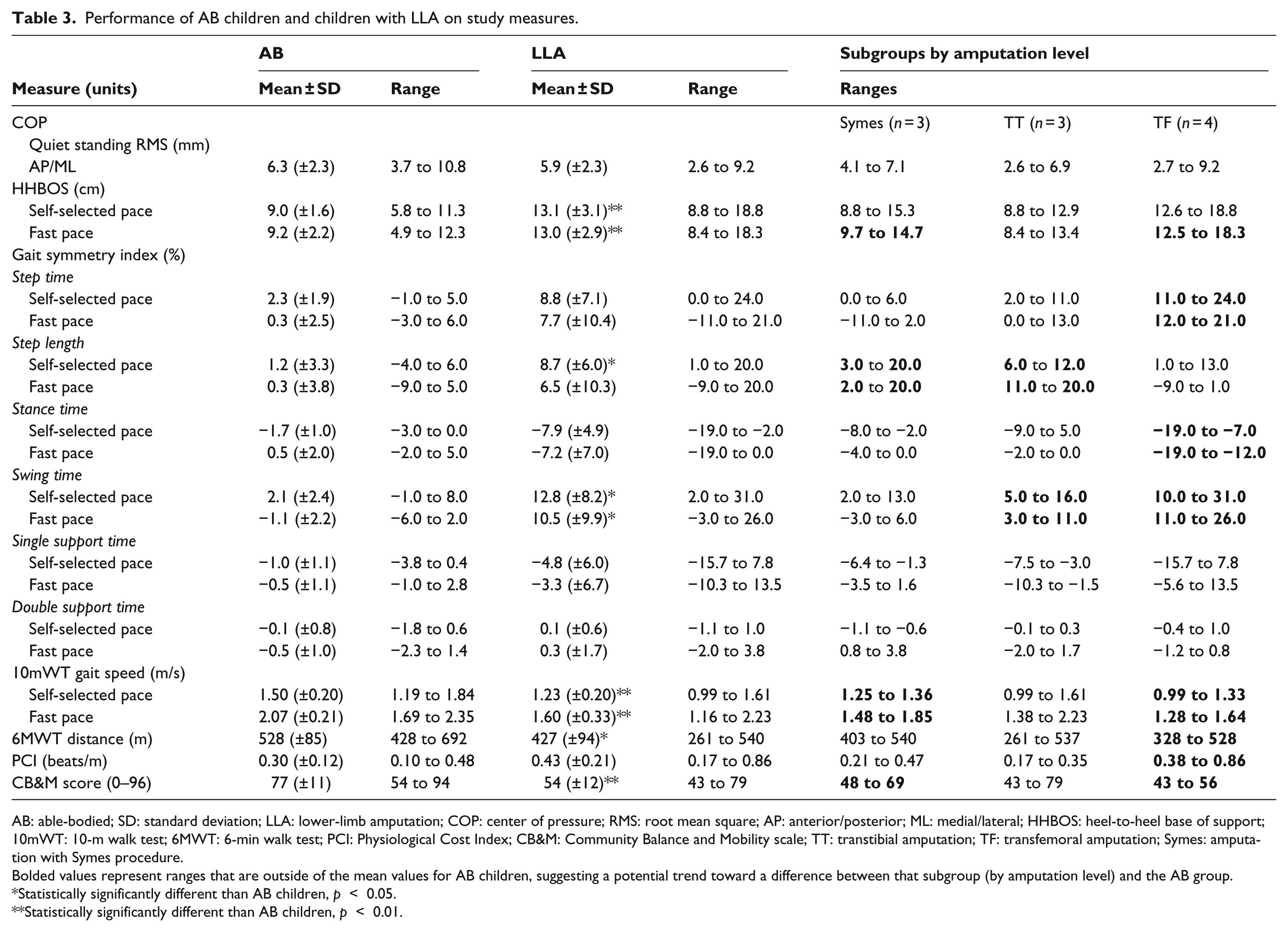
AB: able-bodied; SD: standard deviation; LLA: lower-limb amputation; COP: center of pressure; RMS: root mean square; AP: anterior/posterior; ML: medial/lateral; HHBOS: heel-to-heel base of support; 10mWT: 10-m walk test; 6MWT: 6-min walk test; PCI: Physiological Cost Index; CB&M: Community Balance and Mobility scale; TT: transtibial amputation; TF: transfemoral amputation; Symes: amputation with Symes procedure.
Bolded values represent ranges that are outside of the mean values for AB children, suggesting a potential trend toward a difference between that subgroup (by amputation level) and the AB group.
Statistically significantly different than AB children, p < 0.05.
Statistically significantly different than AB children, p < 0.01.
Figure 1 provides a summary of the correlation coefficients found in Tables 4 and 5, as well as the same data for the AB children. The figure highlights strong positive correlations between increased PCI and greater step width, and greater spatiotemporal asymmetry in children with LLA, but not AB children. A strong relationship was also found between better postural control (lower COP RMS) and increased walking speed for children with LLA, but not AB children. In children with LLA only, better postural control (lower COP RMS) was associated with better performance on the CB&M. The above represent the strongest correlations (r > 0.75), while a number of other moderate correlations (r = 0.5–0.75) were also found (Figure 1), again primarily for children with LLA. Additionally, while very strong correlations were found among the height, weight and age of the children, only a handful of correlations were found between these developmental variables and the other measures. For the amputee group, age, height, and weight were moderately positively correlated with heel-to-heel base of support (HHBOS) and negatively to single support SI and COP RMS. For the AB group, height and weight showed a positive moderate correlation with HHBOS only.
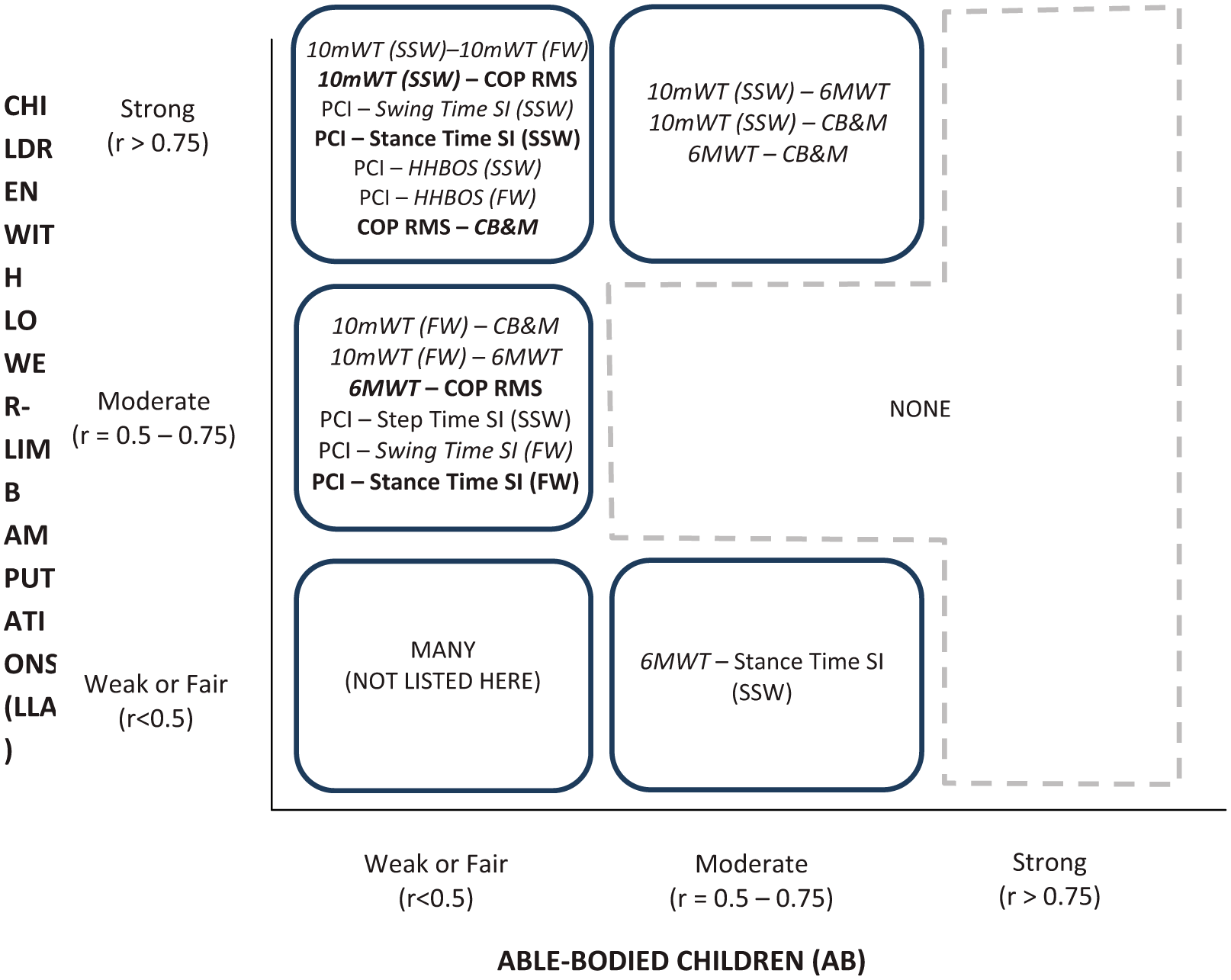
Summary of relationships from correlation analysis between measures of balance and mobility. Only items that were strongly or moderately correlated are presented. Bold items show that they are negatively correlated. Italics represent those variables for which the LLA and AB group scores were significantly different (as per Table 3).
Pearson correlations among measures of body function and activity in children with LLA.
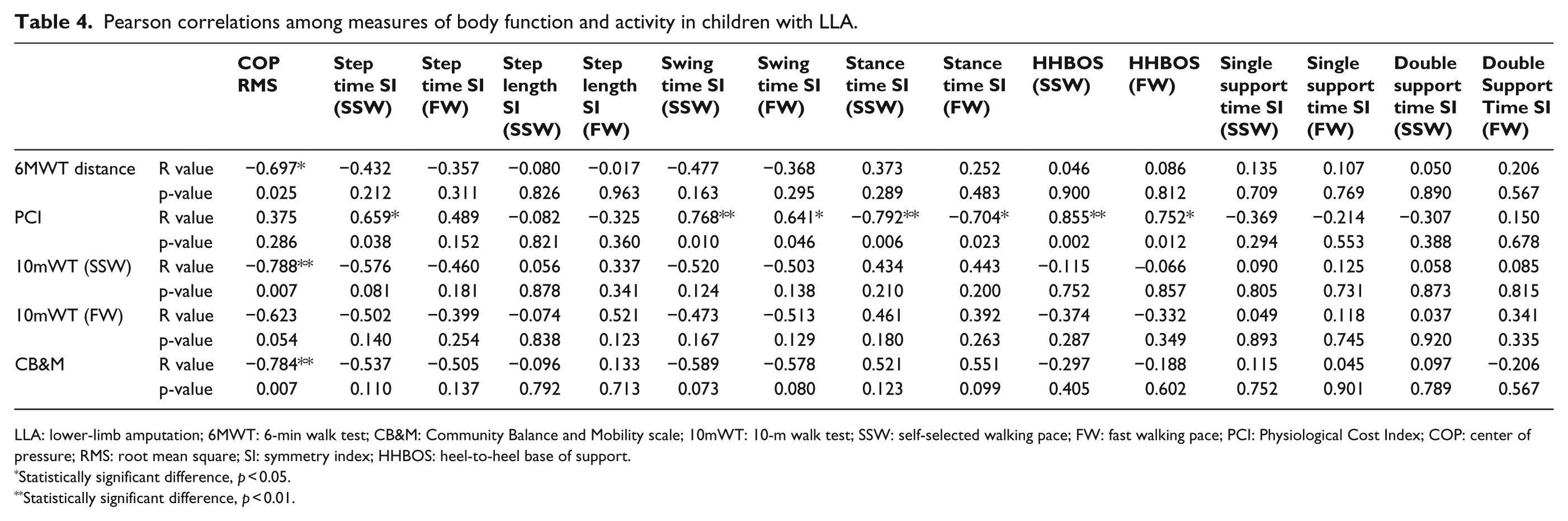
LLA: lower-limb amputation; 6MWT: 6-min walk test; CB&M: Community Balance and Mobility scale; 10mWT: 10-m walk test; SSW: self-selected walking pace; FW: fast walking pace; PCI: Physiological Cost Index; COP: center of pressure; RMS: root mean square; SI: symmetry index; HHBOS: heel-to-heel base of support.
Statistically significant difference, p < 0.05.
Statistically significant difference, p < 0.01.
Pearson correlations among measures of activity and energy expenditure for children with LLA.
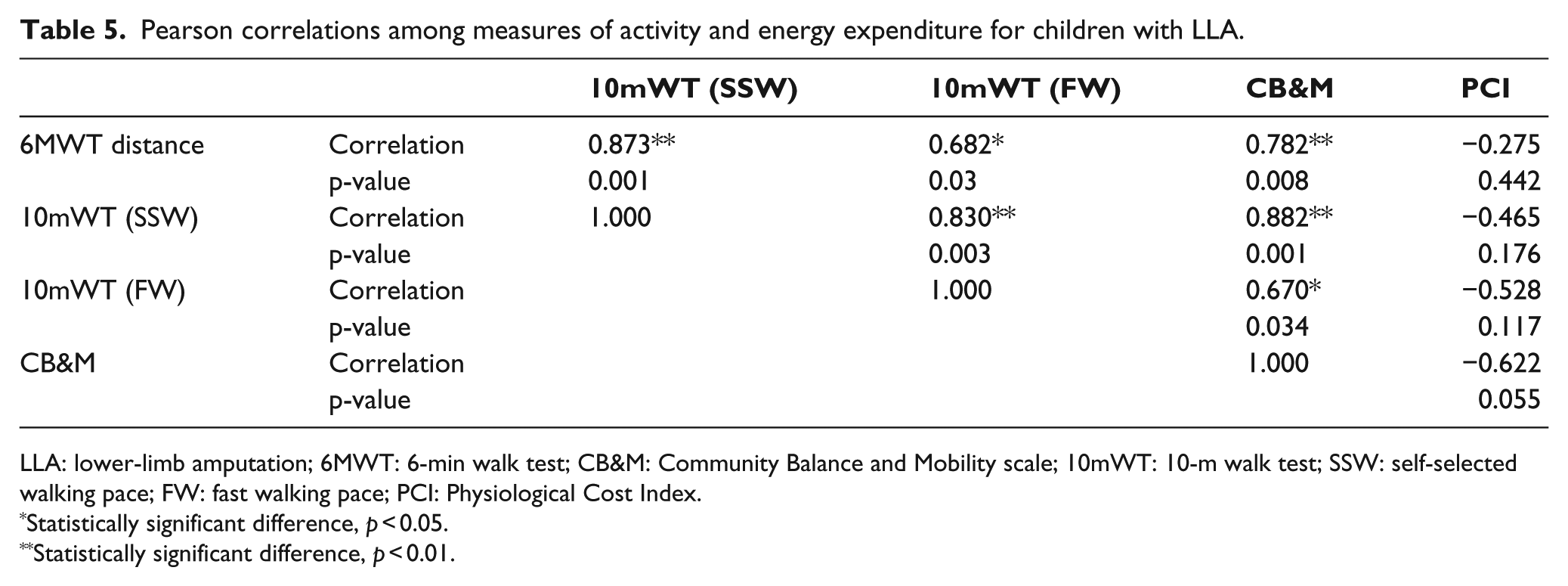
LLA: lower-limb amputation; 6MWT: 6-min walk test; CB&M: Community Balance and Mobility scale; 10mWT: 10-m walk test; SSW: self-selected walking pace; FW: fast walking pace; PCI: Physiological Cost Index.
Statistically significant difference, p < 0.05.
Statistically significant difference, p < 0.01.
Discussion
The study findings aim to address a gap in the literature with respect to the balance- and mobility-related impairments and activity limitations of children with LLA. The goal of the study was to highlight the relationships among clinically relevant balance and mobility measures and tests so as to lay a foundation to guide both the clinical use of these tools and research to further develop and evaluate them for use in children with LLA.
The two groups performed differently on most of the measures, with the AB children typically demonstrating what would be considered better performance compared to the LLA group (Table 3). One exception to this is the postural control (COP RMS) measurements, which were not found to be different between LLA and AB groups. This may in part be attributed to the fact that the AB group was on average a year younger and included more male participants. The literature shows that postural control develops in a nonlinear fashion across childhood, 22 and studies of school-aged children have shown that boys display greater postural sway than girls. 38 COP RMS was formally evaluated in this study, but it is recognized that there are numerous measures for postural sway utilizing various COP variables, which should be examined in future work.
In this study, COP measurements were found to be moderately correlated with the 6MWT distance and strongly correlated with the 10mWT speed within the LLA group. These findings coincide with the published literature (primarily for adults), indicating that the deterioration of balance, as is commonly associated with amputations, is at least moderately associated with decreased walking speed. 6 Postural control was also found to be strongly correlated with the CB&M, suggesting the association of lower quiet standing sway with better balance and mobility performance. The CB&M is much more physically challenging than a quiet standing task and appears to be able to better discriminate between LLA and AB groups, even in a highly heterogeneous sample. Although the CB&M was not developed or validated for children with LLA, based on this study’s findings and our experiences, additional work seems warranted to investigate its applicability, utility, and measurement properties in this population.
In terms of spatiotemporal gait measures, similar to studies done on adults,3,12,39 those with LLA (and especially the transfemoral subgroup) were significantly more asymmetrical and had a wider stance (HHBOS) during walking. However, a relationship between these gait deviations and limitations in functional mobility and balance, as determined via the CB&M, 6MWT, or 10mWT, was not found. The exception may be swing time, where moderate correlations may exist, but the statistical power was too low to detect them. One potential reason that correlations were generally not detected is that kinematic and spatiotemporal limb asymmetries are associated with a number of other factors, such as the performance and inertial properties of prosthetic components, 40 as well as changes in anatomy and physiology including the loss of muscle function—factors which are both dependent on the level of amputation and were not formally evaluated in this study.3,8,11
Aligned with established LLA literature, decreased energy efficiency was noted during walking as measured by PCI. Also, supporting previous findings, 41 children with LLA (and especially those with higher level amputations) clearly could not walk as far or as fast as their AB counterparts during the 6MWT, despite working harder as reflected by a trend in the PCI. Interestingly, PCI was not correlated with walking speed, possibly because this is evaluated over a much shorter duration so that energy/fatigue does not come into play or, alternatively, perhaps children with LLA adjust and reduce their walking speed to limit their energy expenditure, bringing it closer to normal levels as measured in the AB children.18,41 In terms of PCI and symmetry, moderate to strong (positive) correlations were found for step, swing, and stance times. Similarly, previous studies have also found longer swing times and shorter stance times when comparing the prosthetic and intact limbs, as well as higher metabolic cost associated with walking in individuals with LLA.3,4,42 However, the potential relationships between the two sets of variables have previously not been examined, to which the findings of this study suggest that increased energy demand may be at least partially a result of spatiotemporal asymmetries in gait. Moreover, step width (HHBOS) was found to be strongly, positively related to PCI in our study. While this has not been previously investigated for individuals with LLA, research does indicate that a higher physiological cost is associated with a wider step width in other patient populations. 43 It remains to be investigated whether focusing rehabilitation to improve gait symmetry and step width to AB population levels can help children with LLA achieve more efficient and functional mobility.
The finding of strong correlations between a number of measures across the ICF categories is positive and has useful implications in clinical and research applications. Although this study has taken the first steps in identifying potentially useful relationships between measures of balance and mobility as seen in Figure 1, it does not facilitate a deeper analysis of factors that drive these relationships. Figure 1 indicates that most of the relationships (strong and moderate correlations) were found solely in children with LLA, and not the AB children, which suggests that the correlations are likely related to impairments (as in children with LLA) rather than just developmental differences (such as age and height) in the sampled children. Future exploration of the underlying relationships should aim to isolate disability-related factors (amputation level) and developmental factors (age, height); while our sample size was too small to formally investigate these, descriptively we did see trends of improvements in measures for children with LLA who had lower levels of amputation (i.e. Symes and transtibial). It is recommended that future work control for amputation level by ensuring a sample size of at least 10 children per amputation level studied. Age appears to be less of a factor as seen by weak correlations across gait variables here (with the exception of HHBOS), and this is in agreement with other literature. 44
Finally, it is noted that not all of the selected measures have been developed for and thoroughly investigated in the pediatric LLA population, and this speaks to the need for future work to investigate measurement properties and establish suitable outcome measures, based on the ICF, for this population.25,45,46
Conclusion
This study aimed to provide a broad understanding of mobility and balance deficits in children with LLA. A number of important relationships between mobility- and balance-related impairments and activities have been identified, providing a foundation for future work geared toward generating evidence to guide clinical decision-making toward more effective rehabilitation for children with LLA. Future work should also further focus on establishing outcome measures for this population, including assessing their utility and metric properties, as well as utilizing alternate study designs to explore disability-related factors.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.