
Abstract
The purpose of this study was to check out the performance and durability of vulcanized Jaipur rubber feet in tropical areas of the developing world. Forty-one MUKTI and 40 NISHA feet were followed for 16 (8 – 17) months. The user compliance was high and nearly all were satisfied. Failure of the prosthetic foot with the need for exchange at the end of the study amounted to 27% (22/81), which is equivalent to a mixed series of rubber feet previously reported (Jensen et al. 2006b). Failures were mostly related to skin fracture and gliding between sponge rubber layers of the heel block.
Introduction
In the 1970s, Dr. P. K. Sethi initiated the development of a prosthetic foot being an alternative to the conventional SACH foot, but which allowed barefoot walking, squatting and cross-legged sitting (Sethi et al. 1978). The foot was originally designed with a high ankle block of wood facilitating fixation to the aluminium shank of the prosthesis with wooden screws; a block of sponge rubber layers glued together to resemble the mobility of the normal ankle, subtalar and mid-tarsal joints. Originally the tarsus and metatarsals were replicated by a wooden wedge with plantar reinforcement by cord lining. Each block was enclosed in a shell of hard rubber, covered with natural rubber and vulcanized. In later models the fore-foot was replaced by a hard rubber block or sponge rubber layers.
That the sponge rubber parts allowed for dorsiflexion, plantarflexion, supination, pronation, internal and external rotation has been shown in the laboratory (Kabra and Narayanan 1991) likewise it provided a more natural gait closer to the performance of the normal foot (Arya et al. 1995).
The purpose of the present study was to check out the performance and the durability of Jaipur rubber feet in urban and dry rural tropical areas in the developing world.
Materials and methods
In two series of trans-tibial amputees Jaipur rubber feet produced by two different manufacturers (MUKTI, Chennai and NISHA Foot Centre, Kartarpura, Jaipur, India) were tested. The constructions are in essence identical to the original design of the Jaipur foot (Sethi et al. 1978) with a wedge formed block of sponge rubber layers, separated by a wall of natural rubber from the cubical, compressible heel block of sponge rubber layers, separated from the wooden ankle block. The whole construction is wrapped with natural rubber and vulcanized (Figures 1 and 2).

Sagittal cut of MUKTI foot.

Sagittal cut of NISHA foot.
In order to allow results to be compared to previous field tests performed by ISPO, the authors used the modular polypropylene (PP) system designed and marketed by the International Committee of the Red Cross (ICRC), consisting of a drape wrapped polypropylene socket, two alignment discs, and a tubular shank part. The NISHA foot has a bolt going centrally through the ankle wooden block making fixation to the shank possible in the fashion conventional to the PP technology. The MUKTI foot is normally fixed by wooden screws through the distal portion of the aluminium or polyethylene shank pipe, which is wrapped down over the ankle piece. As the PP technology with its distal alignment disc does not allow for such fixture a distal ankle cap was welded to the shank part and fixed to the block with wooden screws.
The studies were conducted at the ICRC project in Ho Chi Minh City, Vietnam. The prostheses were produced by prosthetic technicians, but check-out carried out by one of two expatriate Category-I prosthetists. The surveys were conducted by a team of the two authors, who both have been involved in previous studies. The amputees were recruited among well-known users and seen for follow-up at 8 – 9 months and 15 – 17 months. The study was completed either at failure or at the latest follow-up.
The clinical field testing was conducted in accordance with the system developed by ISPO (Jensen and Heim 2000; Jensen and Raab 2002).
Demographics and patient characteristics
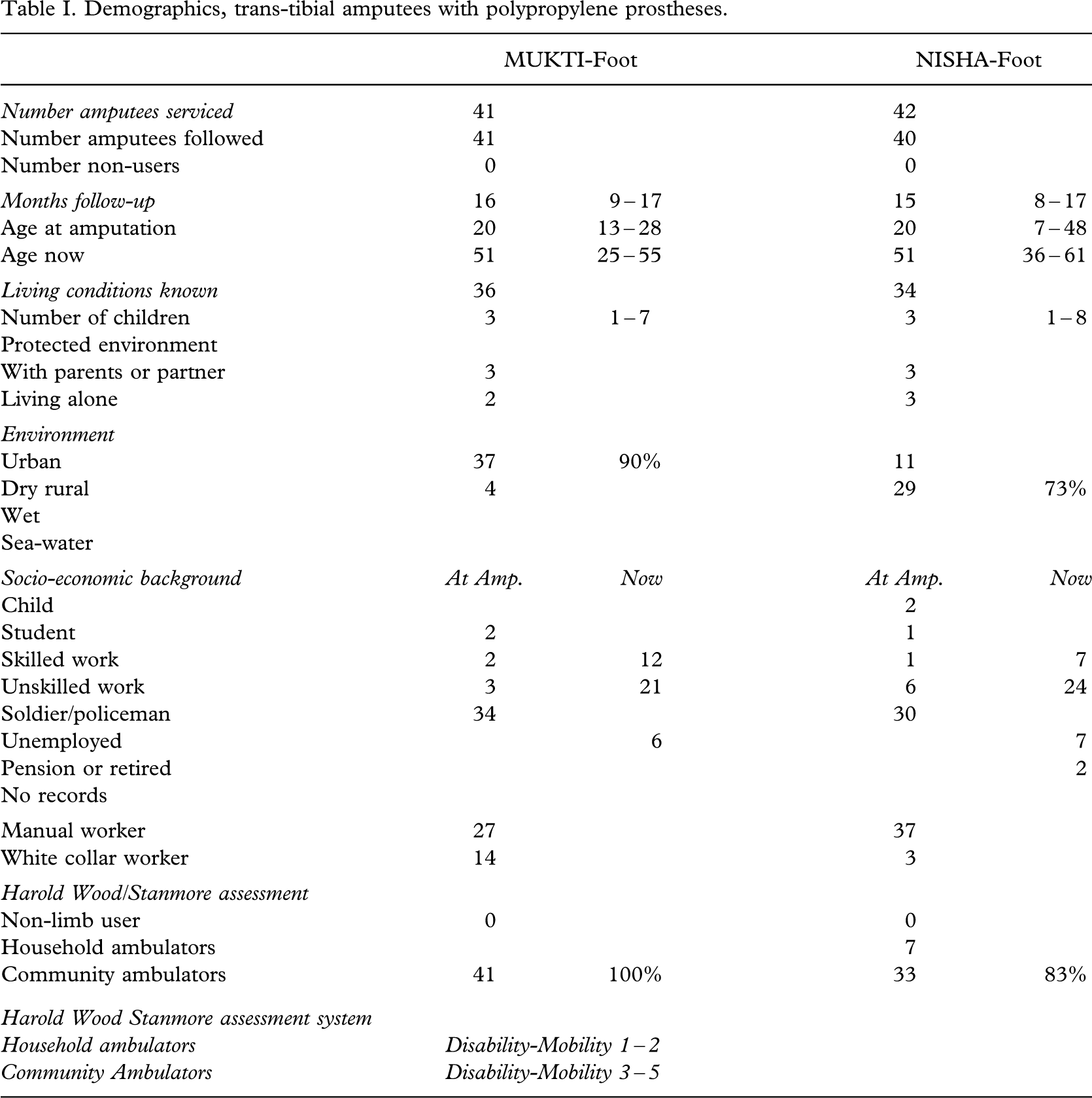
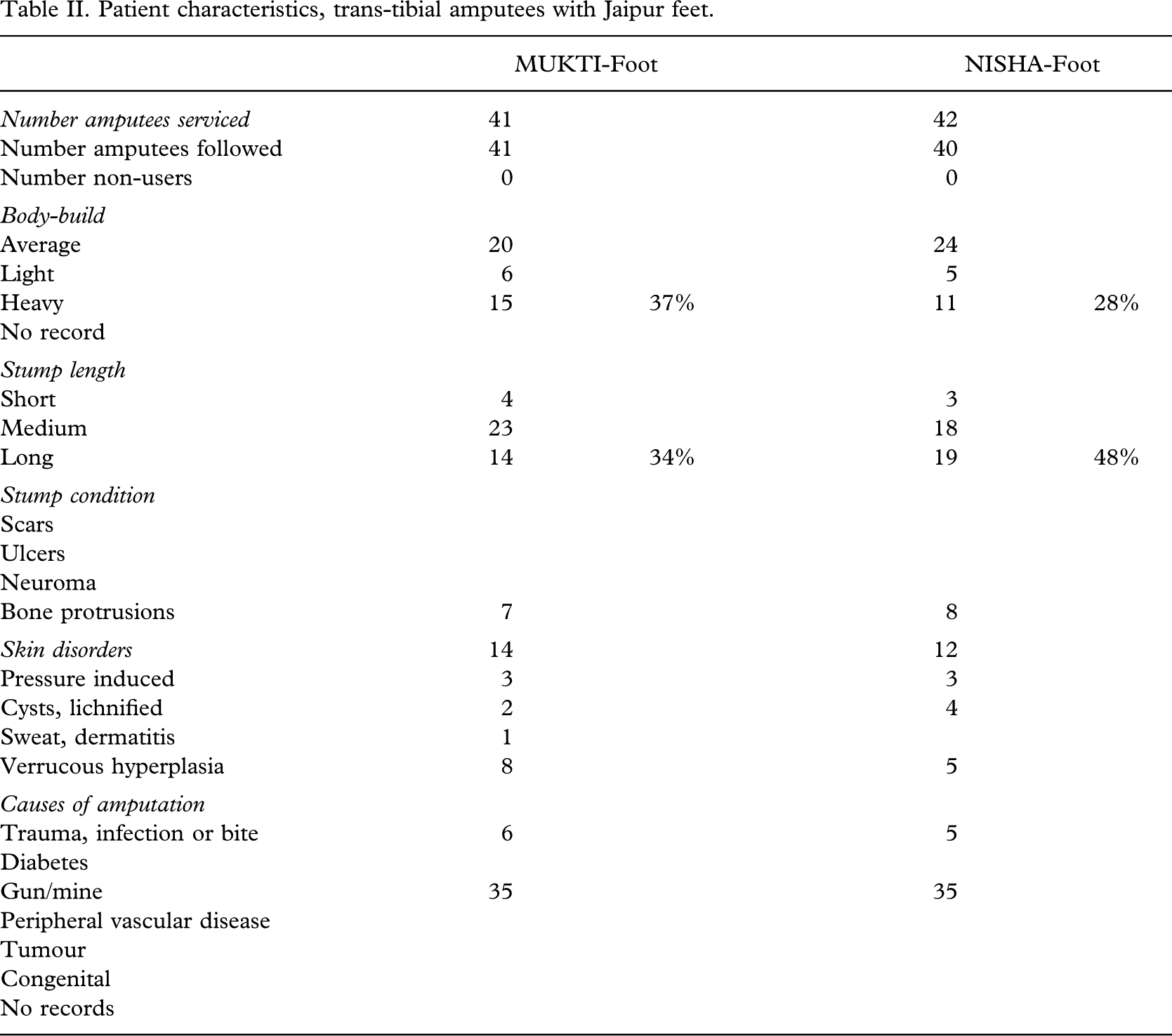
The follow-up rate amounted to 98% (81/83) with a median time of 16 (8 – 17) months (Table I). The amputees were 20 (7 – 48) years of age at the time of amputation and 51 (25 – 61) years at the time of the study. The MUKTI foot was in the main given to urban dwellers, and the NISHA foot to those from nearby rural districts. There were no differences in socio-economical background, but there was a higher proportion of community ambulators in the MUKTI group (p < 0.006). There were no significant differences in respect of weight, stump length and skin disorders (Table II).
Demographics, trans-tibial amputees with polypropylene prostheses.
Patient characteristics, trans-tibial amputees with Jaipur feet.
Patient compliance and prosthetic fitting
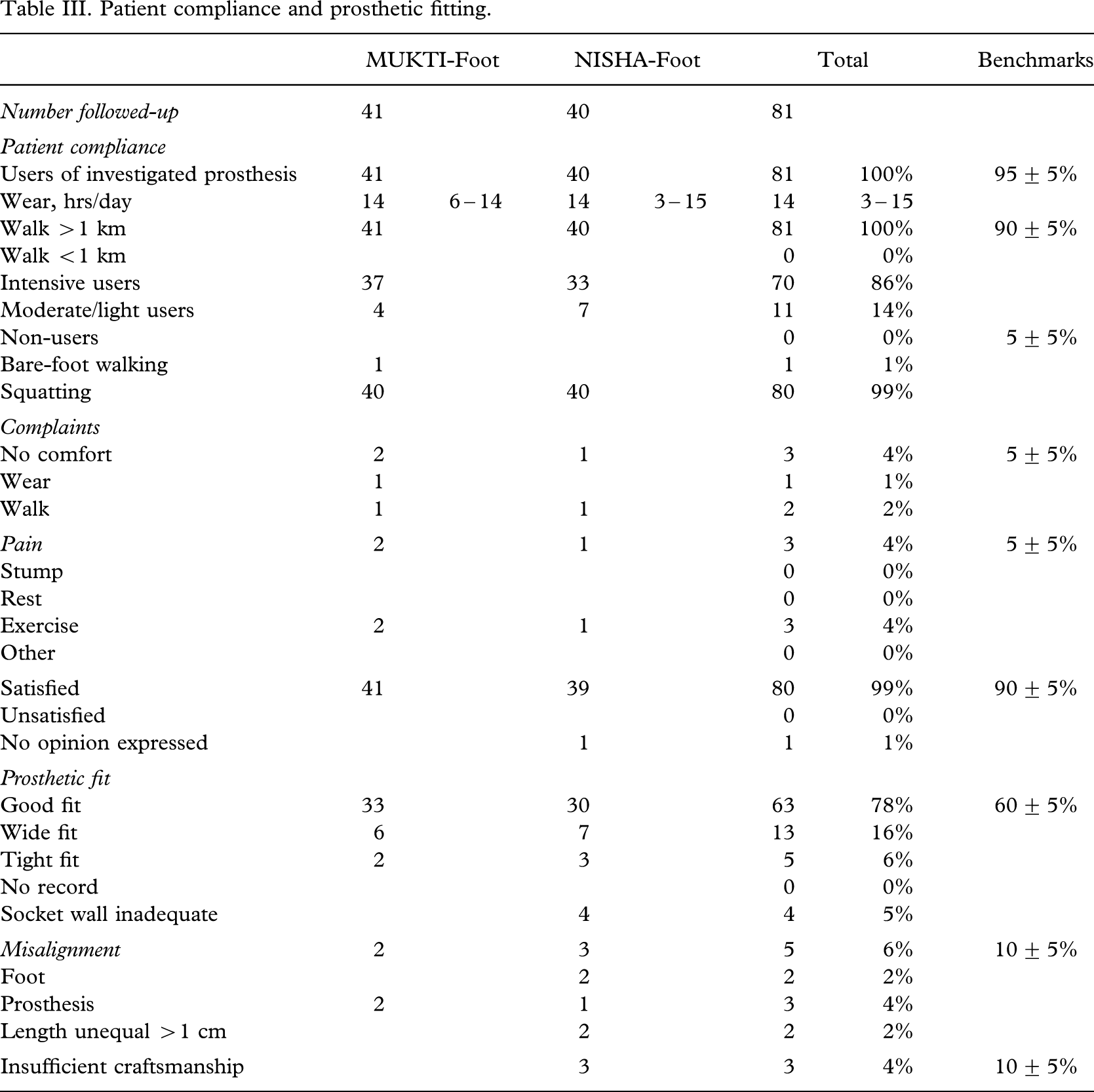
Amputees compliance was high (Table III) and the study group were in general heavy users with walking distances exceeding one kilometre and a median daily use of 14 hours. The complaints were few and the satisfaction rate high. The results satisfied the bench marks recently published (Jensen et al. 2006c).
Patient compliance and prosthetic fitting.
Failure of the prosthetic foot
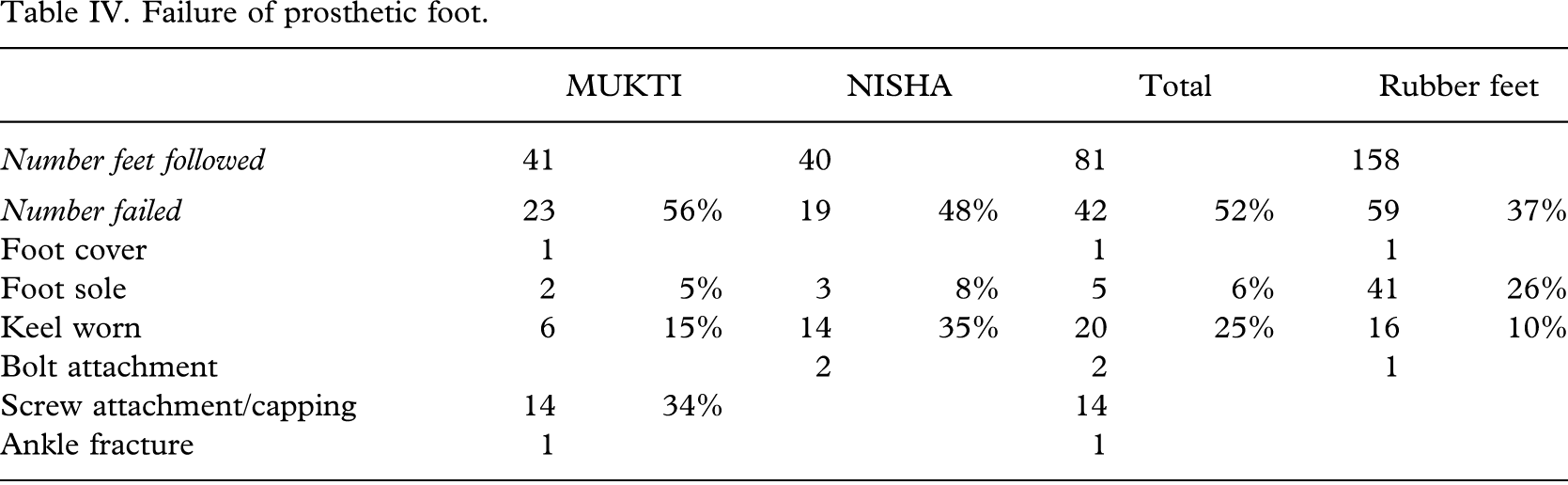
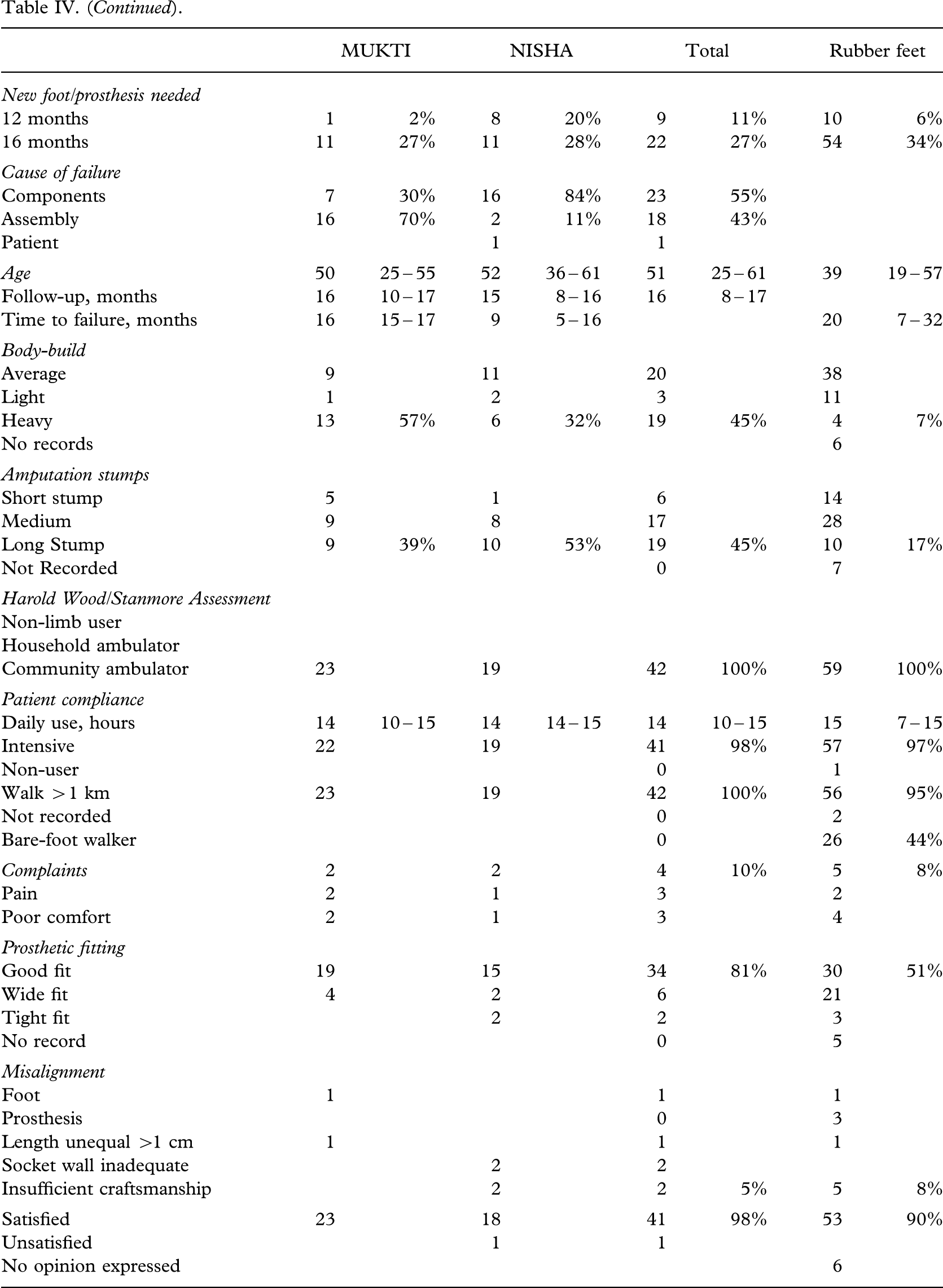
The MUKTI foot needed intervention for loosening of the distal fixation screws in 34% (14/41) already at the first follow-up (Table IV). This was caused by the capping being too short preventing a solid grip in the wooden block. An extra ring of PP was welded to the cap and fixed to the ankle block with screws (Figures 3 and 4). The failure was the result of the choice of the method of fixation and not of the foot construction.
Failure of prosthetic foot.

Polypropylene ring added to ankle cap.

Ankle block fixed to polypropylene ring with wooden screws.
The most frequent failure was related to the heel block with fracture of the skin (Figure 5) and internal separation of the sponge layers (Figure 6), occurring in 25% (20/81) of cases. This failure happened more often (p < 0.03) with the NISHA foot, and resulted in 20% needing exchange of the foot at 12 months, but the different load and wear conditions between urban and rural application should be borne to mind. However, there was no significant difference between the two models by the end of the study, and neither did the need for exchange differ (p = 0.69) from a previous study on rubber feet (Jensen et al. 2006b).

Fracture of skin over ankle block.

Skin fracture extending in between sponge layers of heel block.
Another failure is fracture of the sole and the foot along the septum between heel block and mid-foot (Figures 7 and 8).

Fracture of sole extending along septum between heel block and mid-foot.

Total separation of fore-foot from heel block.
It was not possible to identify any risk factors for failure of the foot among those records listed in Table IV.
Discussion
It has been nearly impossible to find references to clinical performance of Jaipur feet. A web search with 590 references had none concerning clinical results, but numerous descriptions of charity-based projects or camp fitting of large quantities of high density polyethylene (drain-pipe) or aluminium prostheses with Jaipur feet. It was quoted (www.i4donline.net) that by March 2003 the non-government organization, Bhagwan Mahaveer Viklang Sahayata Samiti (BMVSS) had provided 690,480 limbs in India and 15,169 in 19 foreign countries.
One advantage that is constantly brought forward is the possibility of producing the foot from locally available materials, another that the foot can be purchased at a price of less than 30 USD. Nevertheless development work is undertaken under the Indian space research programme to find durable composites in the polyurethane foams (Karunakaran 2006).
It has been claimed (Sethi et al. 1978) that the Jaipur foot is more user-friendly because it allows cross-legged sitting and squatting. That the latter is the case can be confirmed by this study, but it has not been systematically recorded in the other ISPO field studies.
That the durability of the Jaipur feet is much higher than that of the polyurethane feet is beyond doubt (Jensen et al. 2006a).
The results of this series was slightly poorer than previously reported with Jaipur feet (Jensen et al. 2004), but the types of failure were virtually the same. The difference between the MUKTI and NISHA feet with spongy rubber plates for the tarsal and mid-tarsal portion vs. a solid rubber block in the former study made no difference. The previously identified risk factors such as young age and high level of activity could not be confirmed.
The problems associated with the capping technique to fix the MUKTI foot were related to an assembly problem introduced with the study and cannot be blamed on the construction. It did not require any exchange of feet.
The two standard Jaipur feet available in India did not perform any better than the mixed series of rubber feet recently reported (Jensen et al. 2006b) with regard to durability. Among the tested rubber feet there are constructions with a 90% survival or more after 18 months, such as the VI-Solid and VI-Cavity Heel feet from Vietnamese Veterans of America Foundation, Kien Khleang, Cambodia and the EB-1 foot from Prosthetics Outreach Foundation, Vietnam even when exposed to barefoot walking.
The high number of heel block related failures with the Jaipur feet indicates that the problem is of technical nature, and that the separation and sliding between the sponge rubber plates does not have the advantage praised by Sethi et al. (1978).
In conclusion, the authors find that the groups with Jaipur feet tested in this series matched well with the other ISPO test series with regard to patient characteristics, use and compliance with the devices. However, it does show that the two tested Jaipur feet of traditional construction were not superior in respect of durability as compared to other rubber feet constructions from developing countries in South-East Asia.
Footnotes
Acknowledgements
The study was sponsored by the Leahy War Victims Fund, United States Agency for International Development (grant no. HRN-G-00-00-00015-00). The opinions expressed in this paper are those of the authors and ISPO and do not necessarily reflect the views of the USAID.