
Abstract
Based on six series of patients (n = 198) participating in clinical field testing of prosthetic feet and all provided with trans-tibial prostheses in accordance with the polypropylene component and assembly system developed by the International Committee of the Red Cross (ICRC) follow-up studies by teams consisting of an orthopaedic surgeon and a Category-I prosthetist-orthotist were conducted. A series of quality measures were tested against previously published quality benchmarks. The polypropylene system gives a consistent product and allows for increased demands on quality benchmarks. The acceptance of discomfort and pain could be reduced to 5 ± 5%. The technical performance demands were reduced for misalignment to 10 ± 5%. In general for all quality measures the range could be reduced to ±5%. These new demands reflect what an orthopaedic workshop outside of a teaching system should be able to attain.
Introduction
Polypropylene is the most commonly used material for socket fabrication as introduced by the ICRC (Verhoeff et al. 1999). Recently ISPO published quality benchmarks for trans-tibial prosthetics in low-income countries based on experiences in schools training and educating Category-II orthopaedic technologists. The prostheses were supplied by the teachers and their students. It was felt, that the results of these series should be considered as being at the lower end of the acceptance level for quality (Jensen et al. 2005a). ISPO has continued clinical field testing utilizing the polypropylene system, and has now collected data from three other centres. One series was fitted by Category-II graduated teachers and their students at University Don Bosco (UDB), El Salvador; one other series from Cambodia fitted by Category-II graduates from the Cambodian School of Prosthetics and Orthotics (CSPO) at their satellite workshops; and one last series from the ICRC workshop in Ho Chi Minh City, Vietnam, where the work was done by technicians with long experience, but check-out supervised by a local Category-II graduate or expatriate Category-I prosthetist-orthotist.
Patients and methods
The ISPO systematic follow-up programme was carried out as normal by a team of an orthopaedic surgeon and a Category-I prosthetist-orthotist. The feet utilized in Cambodia were both of SACH design with internal keel and vulcanized rubber skin from ICRC, Phnom Penh or the Vietnam Veterans of America Foundation (VVAF), Kien Khleang, Cambodia; the latter with a hollow cavity in the heel pad. In El Salvador, a commercially available polyurethane foot, Strider-08, from the Kingsley Manufacturing Company, USA, was tested together with a spring-blade design, polyurethane foot from Fundacio Pro Chirurgica Reconstructive (CIREC), Colombia. Finally, two rubber feet of Jaipur design were utilized in Vietnam (MUKTI, NISHA).
Although the follow-up was planned after approximately 9 months and 18 months, respectively, considerable variation occurs because of difficulties relating to implementation of the series and arrangements and coordination of evaluation team visits. The study was considered completed, if the foot had broken down and required replacement. The follow-up focused on patient compliance based on direct interviews; the basis for prosthetic supply, i.e. stump descriptors and amputee characteristics as based on the examination by the follow-up team; the craftsmanship, i.e. fit, alignment (<20° deviation), socket wall adequacy (<2 cm short), length (<2 cm difference), as assessed by the follow-up team; and finally recording of failures. The results were compared with the quality benchmarks previously suggested by ISPO (Jensen et al. 2005a).
For statistical analysis Student's t-test (unpaired, two-tailed, two-sample, unequal variance) was applied.
Demographics
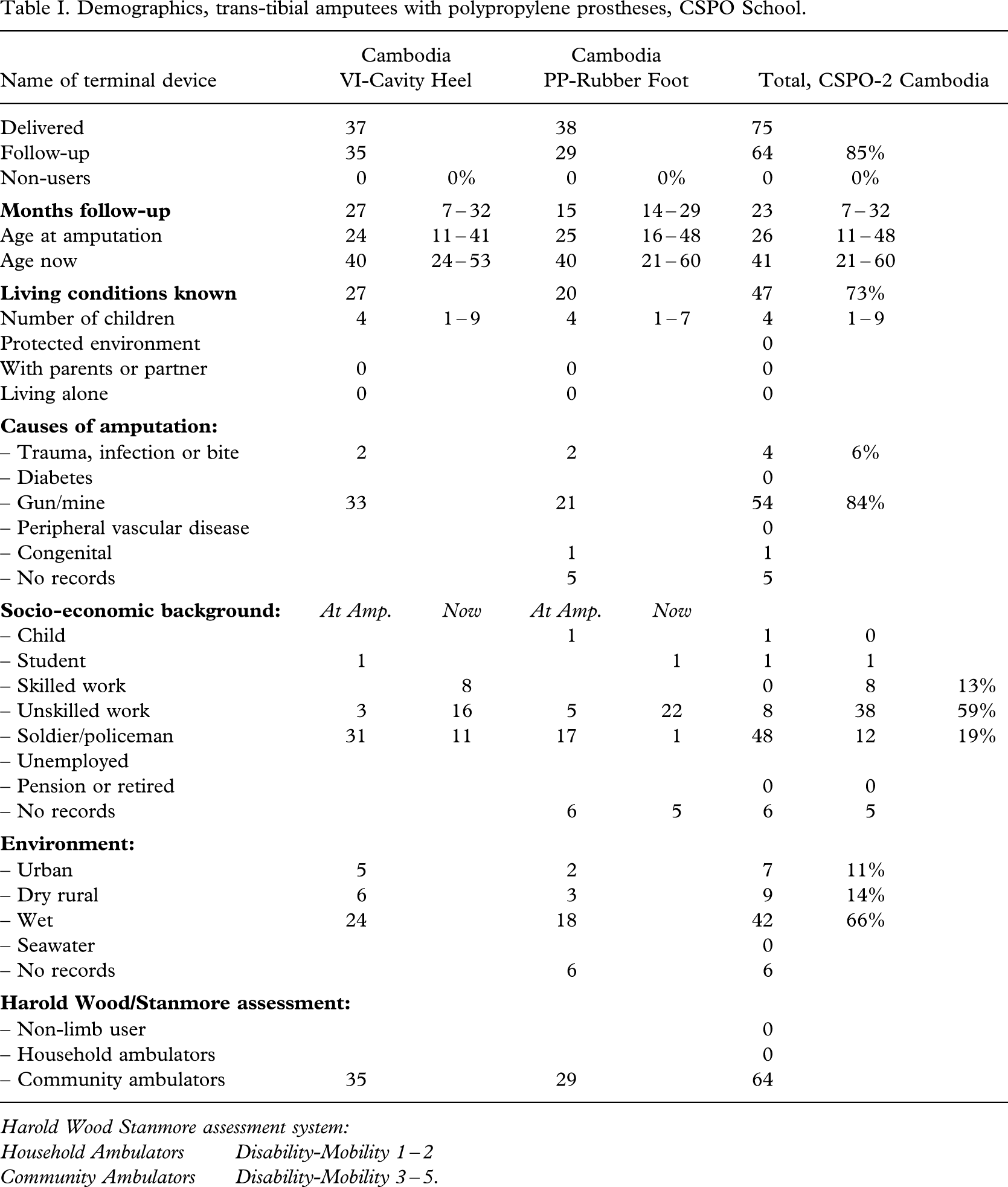
Altogether 83% (198 out of 240) prostheses were followed for 7 months or more, depending on the time of delivery of a given foot, but also on some amputees not showing up for the second follow-up examination.
The amputees were, as in the former series, aged in their 20s at the time of amputation and in their 40s by the time of follow-up (Table I).
Demographics, trans-tibial amputees with polypropylene prostheses, CSPO School.
| Name of terminal device | Cambodia VI-Cavity Heel | Cambodia PP-Rubber Foot | Total, CSPO-2 Cambodia | ||||
|---|---|---|---|---|---|---|---|
| Delivered | 37 | 38 | 75 | ||||
| Follow-up | 35 | 29 | 64 | 85% | |||
| Non-users | 0 | 0% | 0 | 0% | 0 | 0% | |
|
|
27 | 7 – 32 | 15 | 14 – 29 | 23 | 7 – 32 | |
| Age at amputation | 24 | 11 – 41 | 25 | 16 – 48 | 26 | 11 – 48 | |
| Age now | 40 | 24 – 53 | 40 | 21 – 60 | 41 | 21 – 60 | |
|
|
27 | 20 | 47 | 73% | |||
| Number of children | 4 | 1 – 9 | 4 | 1 – 7 | 4 | 1 – 9 | |
| Protected environment | 0 | ||||||
| With parents or partner | 0 | 0 | 0 | ||||
| Living alone | 0 | 0 | 0 | ||||
|
|
|||||||
| – Trauma, infection or bite | 2 | 2 | 4 | 6% | |||
| – Diabetes | 0 | ||||||
| – Gun/mine | 33 | 21 | 54 | 84% | |||
| – Peripheral vascular disease | 0 | ||||||
| – Congenital | 1 | 1 | |||||
| – No records | 5 | 5 | |||||
|
|
At Amp. | Now | At Amp. | Now | |||
| – Child | 1 | 1 | 0 | ||||
| – Student | 1 | 1 | 1 | 1 | |||
| – Skilled work | 8 | 0 | 8 | 13% | |||
| – Unskilled work | 3 | 16 | 5 | 22 | 8 | 38 | 59% |
| – Soldier/policeman | 31 | 11 | 17 | 1 | 48 | 12 | 19% |
| – Unemployed | |||||||
| – Pension or retired | 0 | 0 | |||||
| – No records | 6 | 5 | 6 | 5 | |||
|
|
|||||||
| – Urban | 5 | 2 | 7 | 11% | |||
| – Dry rural | 6 | 3 | 9 | 14% | |||
| – Wet | 24 | 18 | 42 | 66% | |||
| – Seawater | 0 | ||||||
| – No records | 6 | 6 | |||||
|
|
|||||||
| – Non-limb user | 0 | ||||||
| – Household ambulators | 0 | ||||||
| – Community ambulators | 35 | 29 | 64 |
Harold Wood Stanmore assessment system:
Household Ambulators Disability-Mobility 1 – 2
Community Ambulators Disability-Mobility 3 – 5.
The living conditions were recorded in 78% (155 out of 198). Mostly they lived in partnership with a small number of children; only 5% (9 out of 198) living alone.
The cause of amputation was predominantly injuries from war ordnance or other trauma, infection or bites (91%, 181 out of 198).
A minimum of 79% (154 out of 198) were in work at the time of follow-up.
All but one were community ambulators (Davies and Datta 2003).
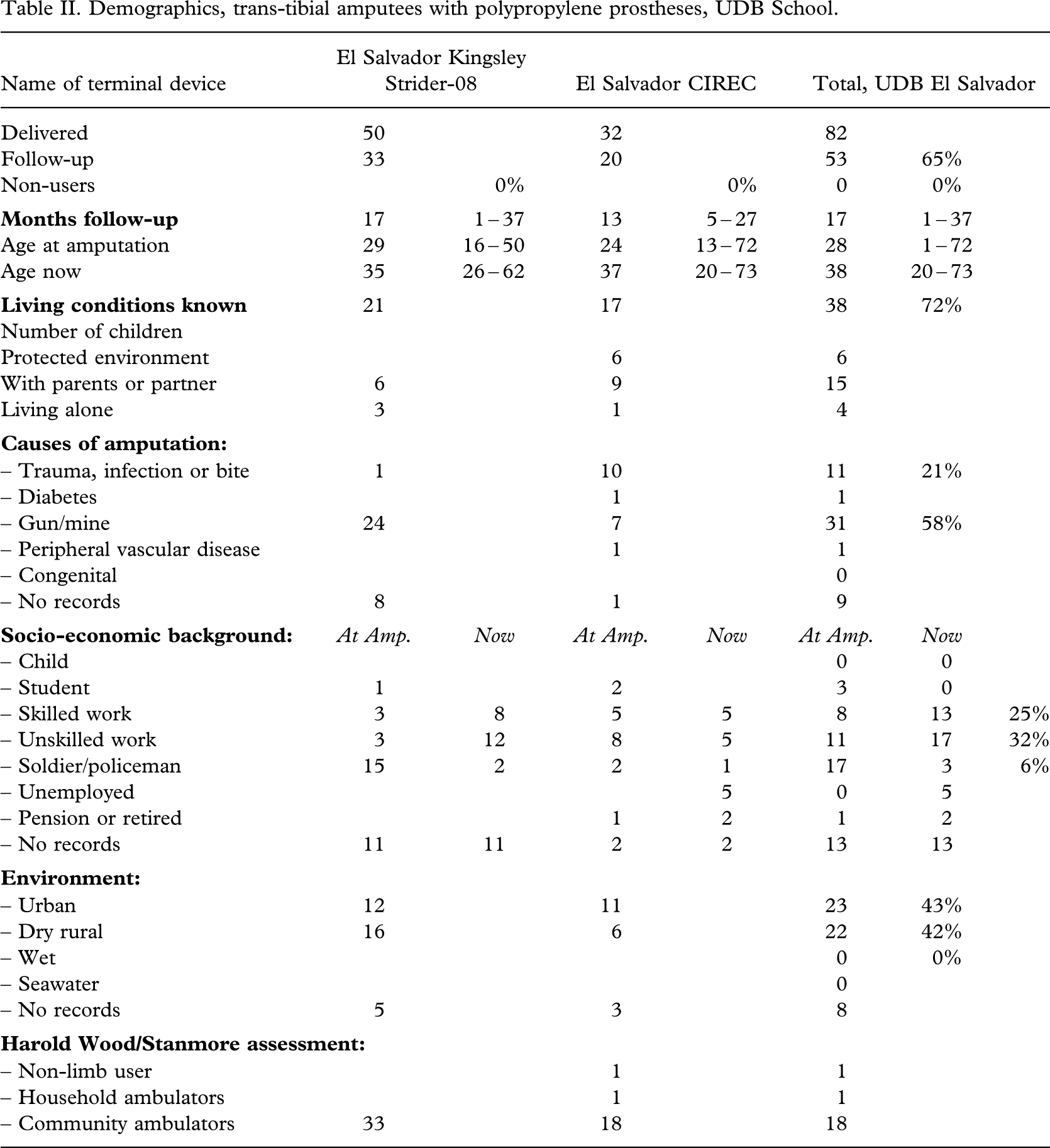
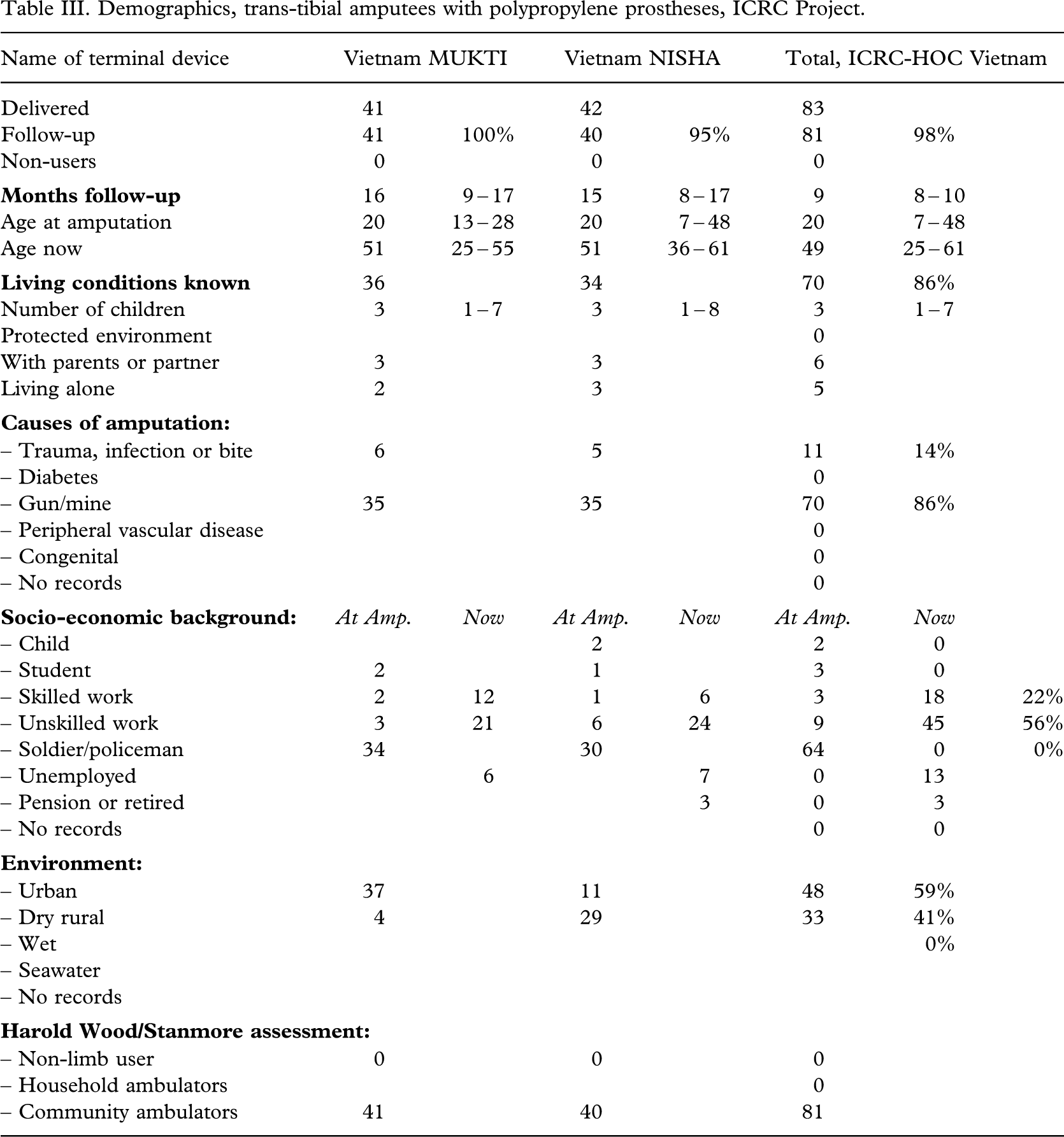
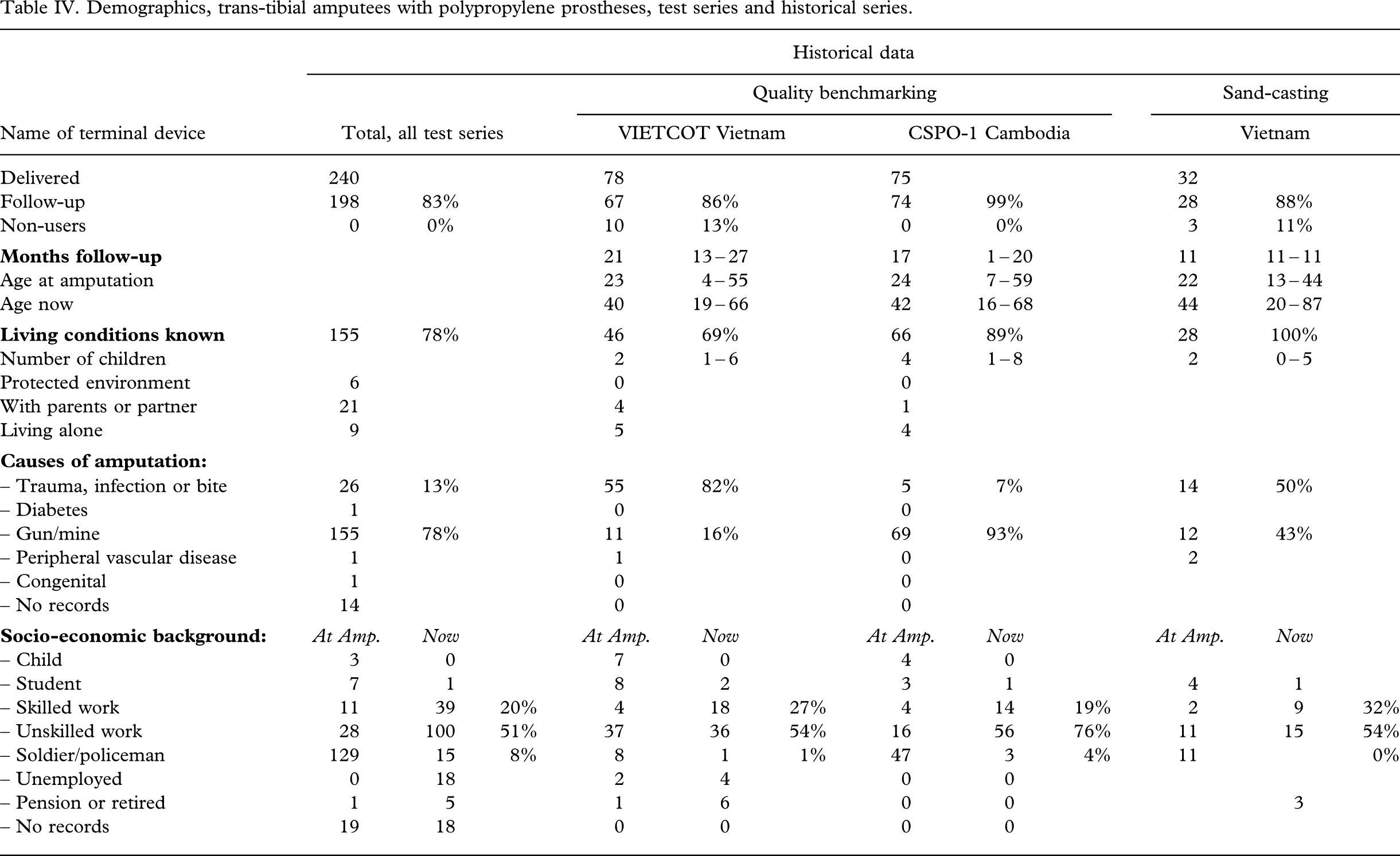
Two other series (Jensen et al. 2005a; 2005b) are displayed for comparative purposes (Tables I–II III IV). The demographics of these series were similar to the present ones.
Demographics, trans-tibial amputees with polypropylene prostheses, UDB School.
| Name of terminal device | El Salvador Kingsley Strider-08 | El Salvador CIREC | Total, UDB El Salvador | ||||
|---|---|---|---|---|---|---|---|
| Delivered | 50 | 32 | 82 | ||||
| Follow-up | 33 | 20 | 53 | 65% | |||
| Non-users | 0% | 0% | 0 | 0% | |||
|
|
17 | 1 – 37 | 13 | 5 – 27 | 17 | 1 – 37 | |
| Age at amputation | 29 | 16 – 50 | 24 | 13 – 72 | 28 | 1 – 72 | |
| Age now | 35 | 26 – 62 | 37 | 20 – 73 | 38 | 20 – 73 | |
|
|
21 | 17 | 38 | 72% | |||
| Number of children | |||||||
| Protected environment | 6 | 6 | |||||
| With parents or partner | 6 | 9 | 15 | ||||
| Living alone | 3 | 1 | 4 | ||||
|
|
|||||||
| – Trauma, infection or bite | 1 | 10 | 11 | 21% | |||
| – Diabetes | 1 | 1 | |||||
| – Gun/mine | 24 | 7 | 31 | 58% | |||
| – Peripheral vascular disease | 1 | 1 | |||||
| – Congenital | 0 | ||||||
| – No records | 8 | 1 | 9 | ||||
|
|
At Amp. | Now | At Amp. | Now | At Amp. | Now | |
| – Child | 0 | 0 | |||||
| – Student | 1 | 2 | 3 | 0 | |||
| – Skilled work | 3 | 8 | 5 | 5 | 8 | 13 | 25% |
| – Unskilled work | 3 | 12 | 8 | 5 | 11 | 17 | 32% |
| – Soldier/policeman | 15 | 2 | 2 | 1 | 17 | 3 | 6% |
| – Unemployed | 5 | 0 | 5 | ||||
| – Pension or retired | 1 | 2 | 1 | 2 | |||
| – No records | 11 | 11 | 2 | 2 | 13 | 13 | |
|
|
|||||||
| – Urban | 12 | 11 | 23 | 43% | |||
| – Dry rural | 16 | 6 | 22 | 42% | |||
| – Wet | 0 | 0% | |||||
| – Seawater | 0 | ||||||
| – No records | 5 | 3 | 8 | ||||
|
|
|||||||
| – Non-limb user | 1 | 1 | |||||
| – Household ambulators | 1 | 1 | |||||
| – Community ambulators | 33 | 18 | 18 |
Demographics, trans-tibial amputees with polypropylene prostheses, ICRC Project.
| Name of terminal device | Vietnam MUKTI | Vietnam NISHA | Total, ICRC-HOC Vietnam | ||||
|---|---|---|---|---|---|---|---|
| Delivered | 41 | 42 | 83 | ||||
| Follow-up | 41 | 100% | 40 | 95% | 81 | 98% | |
| Non-users | 0 | 0 | 0 | ||||
|
|
16 | 9 – 17 | 15 | 8 – 17 | 9 | 8 – 10 | |
| Age at amputation | 20 | 13 – 28 | 20 | 7 – 48 | 20 | 7 – 48 | |
| Age now | 51 | 25 – 55 | 51 | 36 – 61 | 49 | 25 – 61 | |
|
|
36 | 34 | 70 | 86% | |||
| Number of children | 3 | 1 – 7 | 3 | 1 – 8 | 3 | 1 – 7 | |
| Protected environment | 0 | ||||||
| With parents or partner | 3 | 3 | 6 | ||||
| Living alone | 2 | 3 | 5 | ||||
|
|
|||||||
| – Trauma, infection or bite | 6 | 5 | 11 | 14% | |||
| – Diabetes | 0 | ||||||
| – Gun/mine | 35 | 35 | 70 | 86% | |||
| – Peripheral vascular disease | 0 | ||||||
| – Congenital | 0 | ||||||
| – No records | 0 | ||||||
|
|
At Amp. | Now | At Amp. | Now | At Amp. | Now | |
| – Child | 2 | 2 | 0 | ||||
| – Student | 2 | 1 | 3 | 0 | |||
| – Skilled work | 2 | 12 | 1 | 6 | 3 | 18 | 22% |
| – Unskilled work | 3 | 21 | 6 | 24 | 9 | 45 | 56% |
| – Soldier/policeman | 34 | 30 | 64 | 0 | 0% | ||
| – Unemployed | 6 | 7 | 0 | 13 | |||
| – Pension or retired | 3 | 0 | 3 | ||||
| – No records | 0 | 0 | |||||
|
|
|||||||
| – Urban | 37 | 11 | 48 | 59% | |||
| – Dry rural | 4 | 29 | 33 | 41% | |||
| – Wet | 0% | ||||||
| – Seawater | |||||||
| – No records | |||||||
|
|
|||||||
| – Non-limb user | 0 | 0 | 0 | ||||
| – Household ambulators | 0 | ||||||
| – Community ambulators | 41 | 40 | 81 |
Demographics, trans-tibial amputees with polypropylene prostheses, test series and historical series.
| Historical data | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quality benchmarking | Sand-casting | |||||||||||
| Name of terminal device | Total, all test series | VIETCOT Vietnam | CSPO-1 Cambodia | Vietnam | ||||||||
| Delivered | 240 | 78 | 75 | 32 | ||||||||
| Follow-up | 198 | 83% | 67 | 86% | 74 | 99% | 28 | 88% | ||||
| Non-users | 0 | 0% | 10 | 13% | 0 | 0% | 3 | 11% | ||||
|
|
21 | 13 – 27 | 17 | 1 – 20 | 11 | 11 – 11 | ||||||
| Age at amputation | 23 | 4 – 55 | 24 | 7 – 59 | 22 | 13 – 44 | ||||||
| Age now | 40 | 19 – 66 | 42 | 16 – 68 | 44 | 20 – 87 | ||||||
|
|
155 | 78% | 46 | 69% | 66 | 89% | 28 | 100% | ||||
| Number of children | 2 | 1 – 6 | 4 | 1 – 8 | 2 | 0 – 5 | ||||||
| Protected environment | 6 | 0 | 0 | |||||||||
| With parents or partner | 21 | 4 | 1 | |||||||||
| Living alone | 9 | 5 | 4 | |||||||||
|
|
||||||||||||
| – Trauma, infection or bite | 26 | 13% | 55 | 82% | 5 | 7% | 14 | 50% | ||||
| – Diabetes | 1 | 0 | 0 | |||||||||
| – Gun/mine | 155 | 78% | 11 | 16% | 69 | 93% | 12 | 43% | ||||
| – Peripheral vascular disease | 1 | 1 | 0 | 2 | ||||||||
| – Congenital | 1 | 0 | 0 | |||||||||
| – No records | 14 | 0 | 0 | |||||||||
|
|
At Amp. | Now | At Amp. | Now | At Amp. | Now | At Amp. | Now | ||||
| – Child | 3 | 0 | 7 | 0 | 4 | 0 | ||||||
| – Student | 7 | 1 | 8 | 2 | 3 | 1 | 4 | 1 | ||||
| – Skilled work | 11 | 39 | 20% | 4 | 18 | 27% | 4 | 14 | 19% | 2 | 9 | 32% |
| – Unskilled work | 28 | 100 | 51% | 37 | 36 | 54% | 16 | 56 | 76% | 11 | 15 | 54% |
| – Soldier/policeman | 129 | 15 | 8% | 8 | 1 | 1% | 47 | 3 | 4% | 11 | 0% | |
| – Unemployed | 0 | 18 | 2 | 4 | 0 | 0 | ||||||
| – Pension or retired | 1 | 5 | 1 | 6 | 0 | 0 | 3 | |||||
| – No records | 19 | 18 | 0 | 0 | 0 | 0 | ||||||
|
|
||||||||||||
| – Urban | 78 | 39% | 27 | 40% | 17 | 23% | 6 | 21% | ||||
| – Dry rural | 64 | 32% | 39 | 58% | 27 | 36% | 18 | 64% | ||||
| – Wet | 42 | 21% | 1 | 1% | 6 | 8% | 4 | 14% | ||||
| – Seawater | 0 | 0 | 24 | 32% | ||||||||
| – No records | 14 | 0 | 0 | |||||||||
|
|
||||||||||||
| – Non-limb user | 1 | 10 | 0 | 3 | ||||||||
| – Household ambulators | 1 | 0 | 0 | |||||||||
| – Community ambulators | 196 | 99% | 57 | 85% | 74 | 100% | 28 | 100% |
Characteristics of amputees and stumps
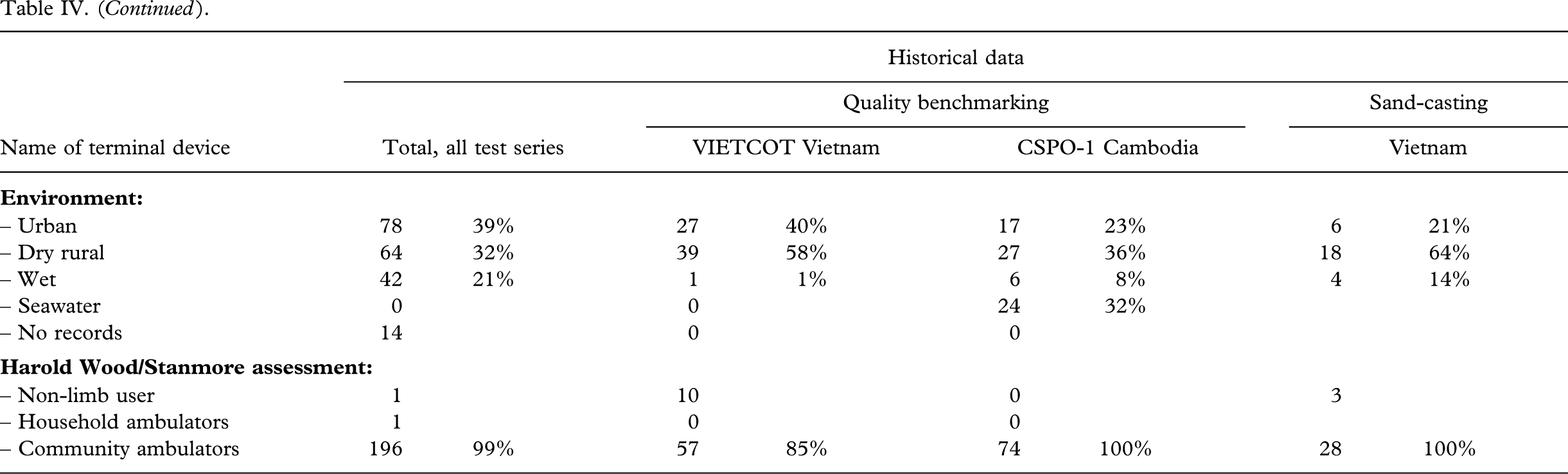
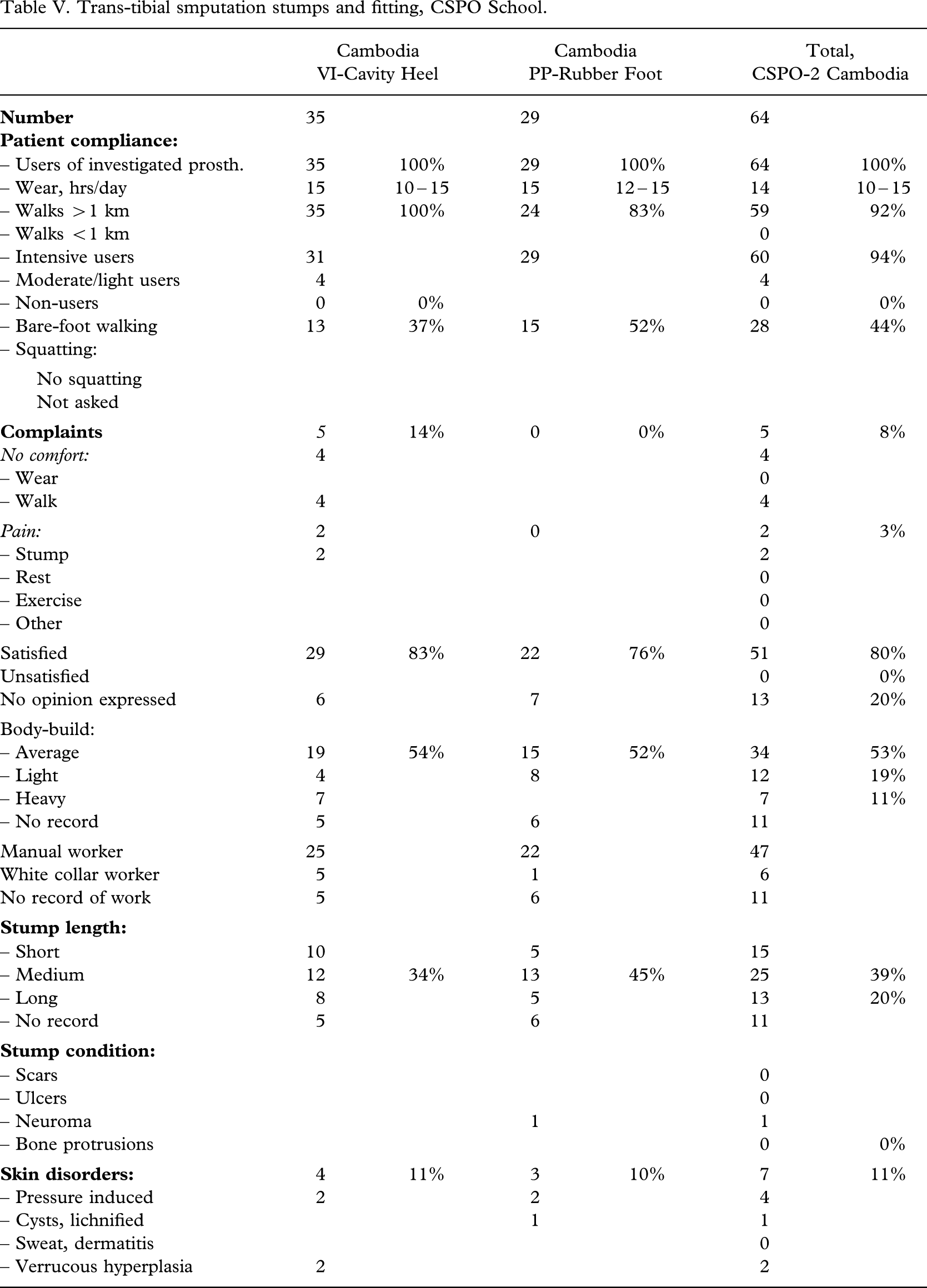
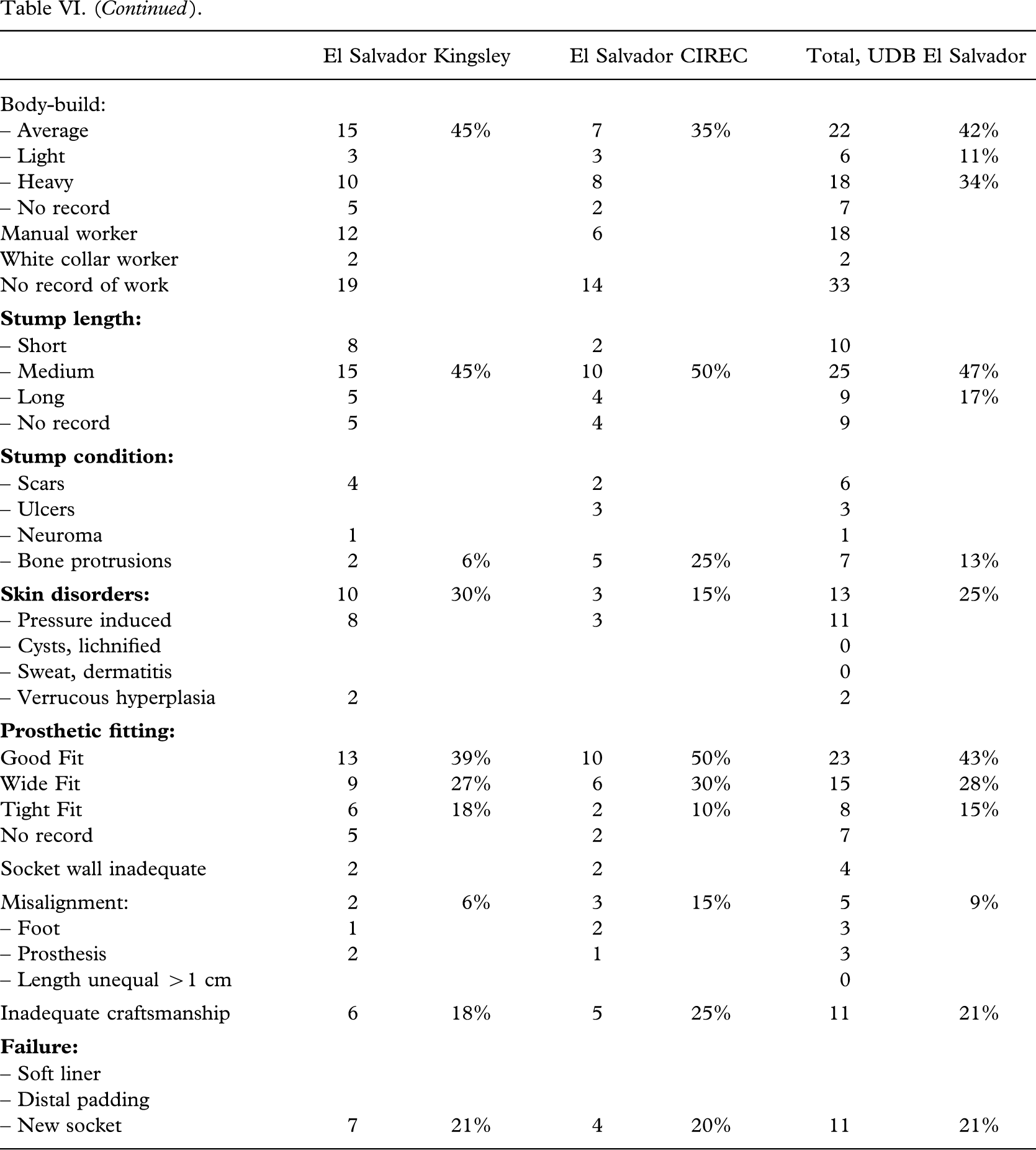
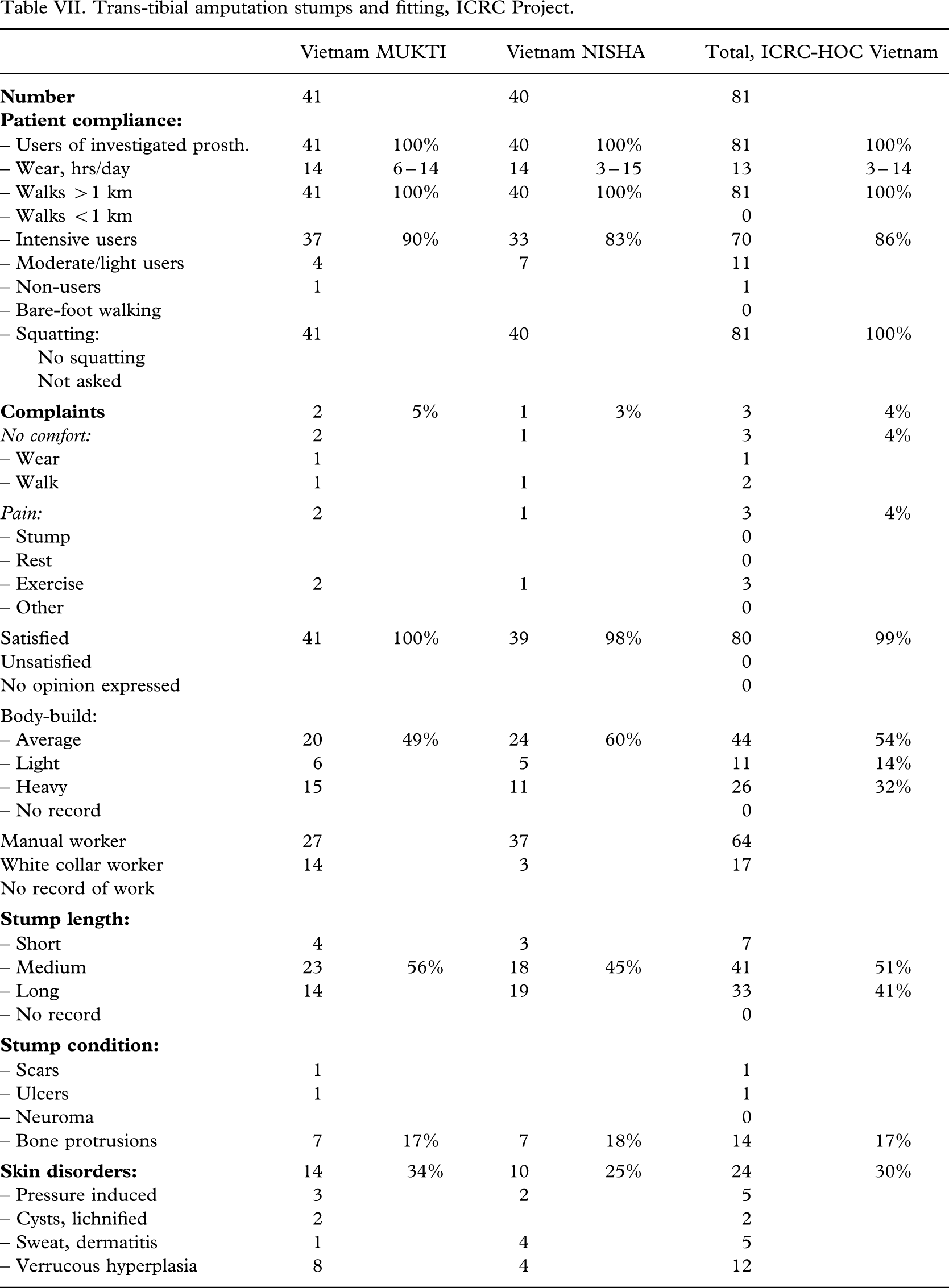
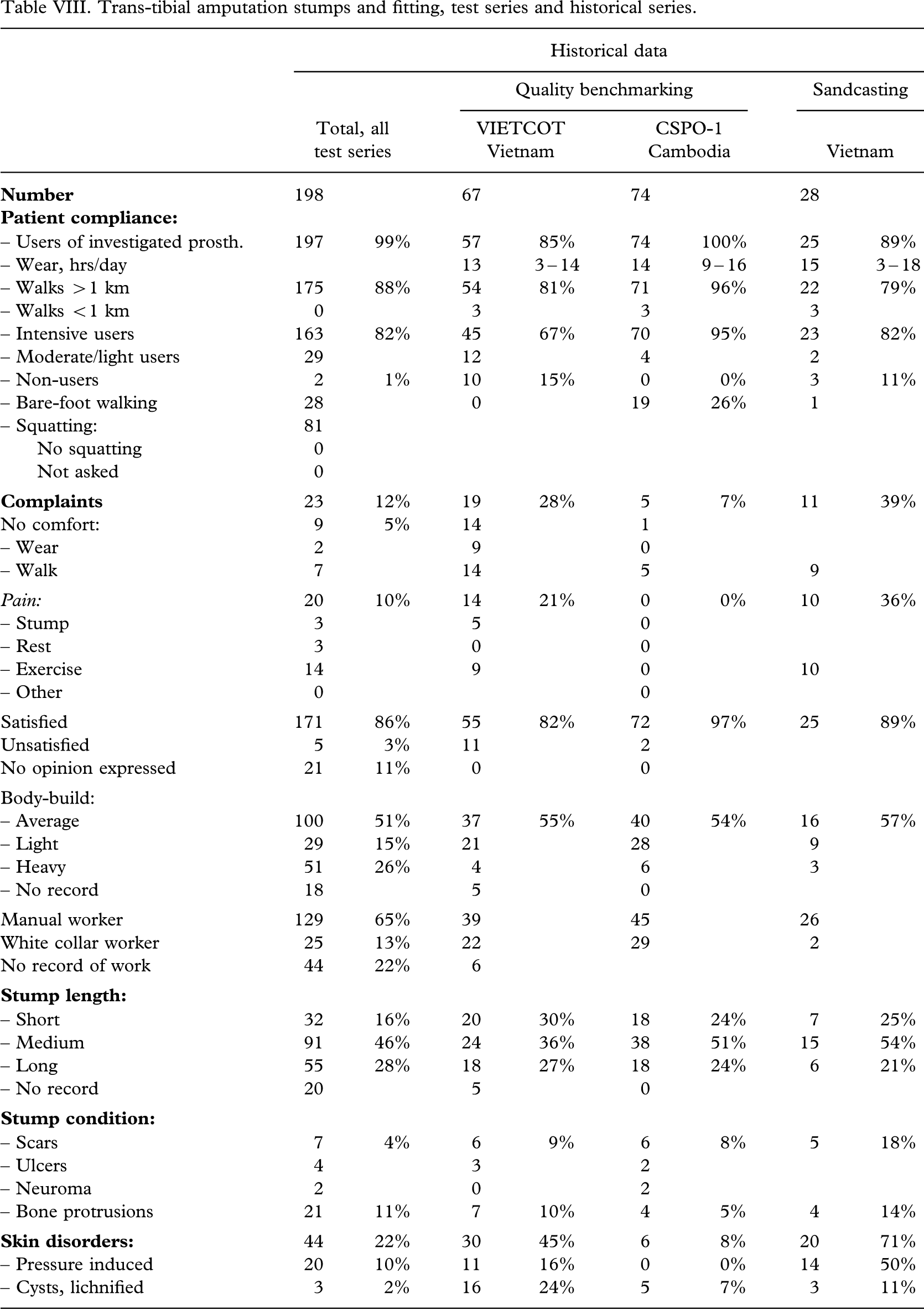
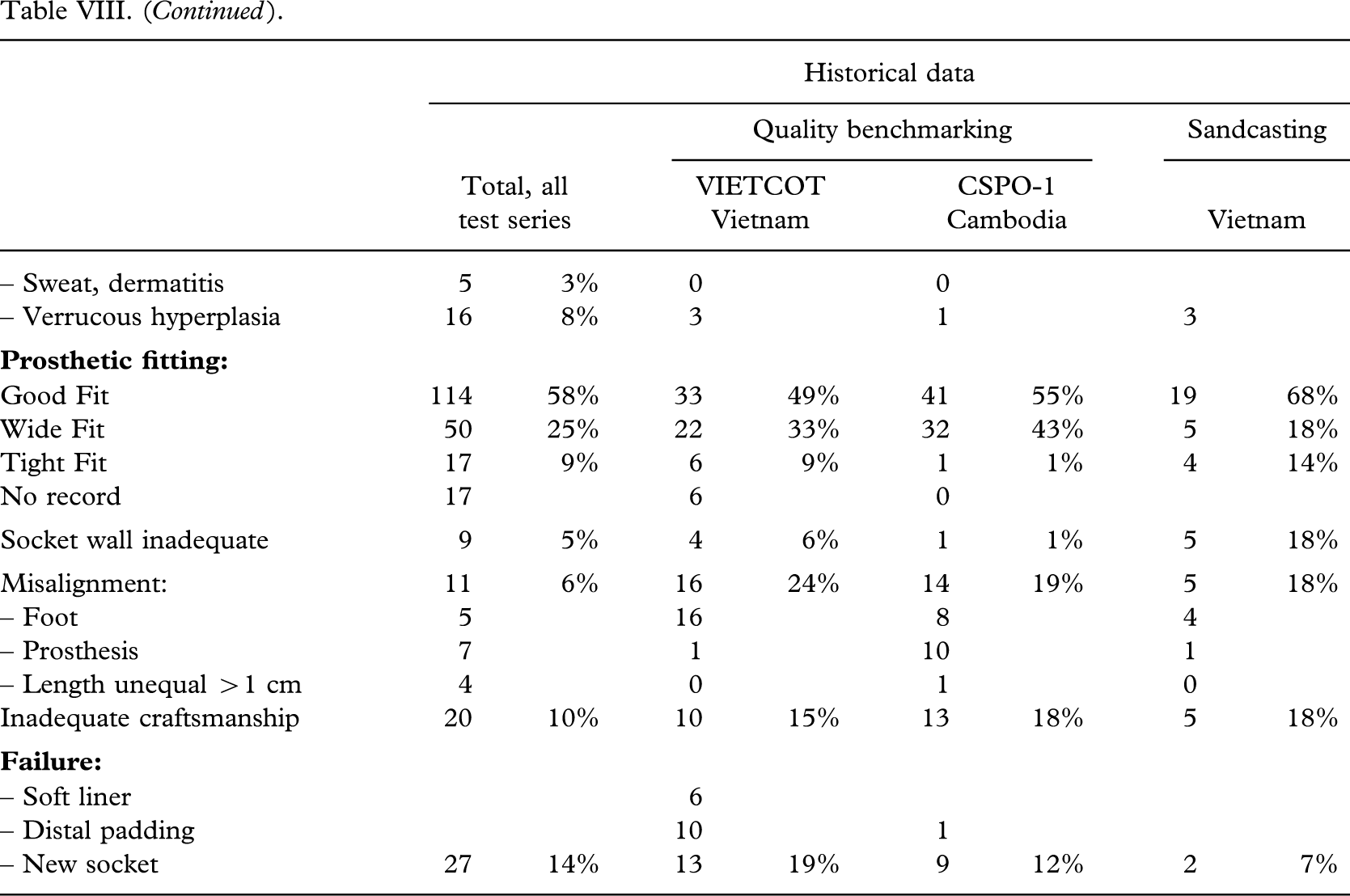
Average body-build was recorded in 51% (100 out of 198), and 65% (129 out of 198) were assessed as manual workers (Tables V–VI VII VIII). The stumps were found to be short in 16% (32 out of 198). Only a limited number had scars (4%, 7 out of 198) and bone protrusions (11%, 21 out of 198). Pressure induced skin disorders, cysts and lichnified skin was encountered in 12% (23 out of 198). The CSPO-2 series from the satellite workshops was without bone protrusions (P < 0.04) and had less skin disorders (P < 0.03). In the ICRC-HOC series the stumps were longer (P < 0.02).
Trans-tibial smputation stumps and fitting, CSPO School.
| Cambodia VI-Cavity Heel | Cambodia PP-Rubber Foot | Total, CSPO-2 Cambodia | ||||
|---|---|---|---|---|---|---|
|
|
35 | 29 | 64 | |||
|
|
||||||
| – Users of investigated prosth. | 35 | 100% | 29 | 100% | 64 | 100% |
| – Wear, hrs/day | 15 | 10 – 15 | 15 | 12 – 15 | 14 | 10 – 15 |
| – Walks >1 km | 35 | 100% | 24 | 83% | 59 | 92% |
| – Walks <1 km | 0 | |||||
| – Intensive users | 31 | 29 | 60 | 94% | ||
| – Moderate/light users | 4 | 4 | ||||
| – Non-users | 0 | 0% | 0 | 0% | ||
| – Bare-foot walking | 13 | 37% | 15 | 52% | 28 | 44% |
| – Squatting: | ||||||
| No squatting | ||||||
| Not asked | ||||||
|
|
5 | 14% | 0 | 0% | 5 | 8% |
| No comfort: | 4 | 4 | ||||
| – Wear | 0 | |||||
| – Walk | 4 | 4 | ||||
| Pain: | 2 | 0 | 2 | 3% | ||
| – Stump | 2 | 2 | ||||
| – Rest | 0 | |||||
| – Exercise | 0 | |||||
| – Other | 0 | |||||
| Satisfied | 29 | 83% | 22 | 76% | 51 | 80% |
| Unsatisfied | 0 | 0% | ||||
| No opinion expressed | 6 | 7 | 13 | 20% | ||
| Body-build: | ||||||
| – Average | 19 | 54% | 15 | 52% | 34 | 53% |
| – Light | 4 | 8 | 12 | 19% | ||
| – Heavy | 7 | 7 | 11% | |||
| – No record | 5 | 6 | 11 | |||
| Manual worker | 25 | 22 | 47 | |||
| White collar worker | 5 | 1 | 6 | |||
| No record of work | 5 | 6 | 11 | |||
|
|
||||||
| – Short | 10 | 5 | 15 | |||
| – Medium | 12 | 34% | 13 | 45% | 25 | 39% |
| – Long | 8 | 5 | 13 | 20% | ||
| – No record | 5 | 6 | 11 | |||
|
|
||||||
| – Scars | 0 | |||||
| – Ulcers | 0 | |||||
| – Neuroma | 1 | 1 | ||||
| – Bone protrusions | 0 | 0% | ||||
|
|
4 | 11% | 3 | 10% | 7 | 11% |
| – Pressure induced | 2 | 2 | 4 | |||
| – Cysts, lichnified | 1 | 1 | ||||
| – Sweat, dermatitis | 0 | |||||
| – Verrucous hyperplasia | 2 | 2 | ||||
|
|
||||||
| Good Fit | 11 | 31% | 17 | 59% | 28 | 44% |
| Wide Fit | 15 | 43% | 7 | 24% | 22 | 34% |
| Tight Fit | 4 | 11% | 0% | 4 | 6% | |
| No record | 5 | 5 | 10 | |||
| Socket wall inadequate | 1 | 1 | ||||
| Misalignment: | 1 | 3% | 0 | 0% | 1 | 2% |
| – Foot | 0 | |||||
| – Prosthesis | 1 | 1 | ||||
| – Length unequal >1 cm | 2 | 2 | ||||
| Inadequate craftsmanship | 5 | 1 | 6 | 9% | ||
|
|
||||||
| – Soft liner | ||||||
| – Distal padding | ||||||
| – New socket | 9 | 26% | 5 | 17% | 14 | 22% |
Trans-tibial amputation stumps and fitting, UDB School.
| El Salvador Kingsley | El Salvador CIREC | Total, UDB El Salvador | ||||
|---|---|---|---|---|---|---|
|
|
33 | 20 | 53 | |||
|
|
||||||
| – Users of investigated prosth. | 33 | 100% | 19 | 95% | 52 | 98% |
| – Wear, hrs/day | 15 | 3 – 16 | 15 | 2 – 16 | 15 | 2 – 16 |
| – Walks >1 km | 24 | 73% | 11 | 55% | 35 | 66% |
| – Walks <1 km | 6 | |||||
| – Intensive users | 23 | 10 | 33 | 62% | ||
| – Moderate/light users | 5 | 9 | 14 | |||
| – Non-users | 0 | 1 | 1 | 2% | ||
| – Bare-foot walking | 0 | |||||
| – Squatting: | ||||||
| No squatting | ||||||
| Not asked | ||||||
|
|
8 | 24% | 7 | 35% | 15 | 28% |
| No comfort: | 2 | 2 | ||||
| – Wear | 1 | 1 | ||||
| – Walk | 1 | 1 | ||||
| Pain: | 8 | 7 | 15 | 28% | ||
| – Stump | 1 | 1 | ||||
| – Rest | 3 | 3 | ||||
| – Exercise | 8 | 3 | 11 | |||
| – Other | 0 | |||||
| Satisfied | 26 | 79% | 14 | 70% | 40 | 75% |
| Unsatisfied | 2 | 3 | 5 | 9% | ||
| No opinion expressed | 5 | 3 | 8 | 15% | ||
| Body-build: | ||||||
| – Average | 15 | 45% | 7 | 35% | 22 | 42% |
| – Light | 3 | 3 | 6 | 11% | ||
| – Heavy | 10 | 8 | 18 | 34% | ||
| – No record | 5 | 2 | 7 | |||
| Manual worker | 12 | 6 | 18 | |||
| White collar worker | 2 | 2 | ||||
| No record of work | 19 | 14 | 33 | |||
|
|
||||||
| – Short | 8 | 2 | 10 | |||
| – Medium | 15 | 45% | 10 | 50% | 25 | 47% |
| – Long | 5 | 4 | 9 | 17% | ||
| – No record | 5 | 4 | 9 | |||
|
|
||||||
| – Scars | 4 | 2 | 6 | |||
| – Ulcers | 3 | 3 | ||||
| – Neuroma | 1 | 1 | ||||
| – Bone protrusions | 2 | 6% | 5 | 25% | 7 | 13% |
|
|
10 | 30% | 3 | 15% | 13 | 25% |
| – Pressure induced | 8 | 3 | 11 | |||
| – Cysts, lichnified | 0 | |||||
| – Sweat, dermatitis | 0 | |||||
| – Verrucous hyperplasia | 2 | 2 | ||||
|
|
||||||
| Good Fit | 13 | 39% | 10 | 50% | 23 | 43% |
| Wide Fit | 9 | 27% | 6 | 30% | 15 | 28% |
| Tight Fit | 6 | 18% | 2 | 10% | 8 | 15% |
| No record | 5 | 2 | 7 | |||
| Socket wall inadequate | 2 | 2 | 4 | |||
| Misalignment: | 2 | 6% | 3 | 15% | 5 | 9% |
| – Foot | 1 | 2 | 3 | |||
| – Prosthesis | 2 | 1 | 3 | |||
| – Length unequal >1 cm | 0 | |||||
| Inadequate craftsmanship | 6 | 18% | 5 | 25% | 11 | 21% |
|
|
||||||
| – Soft liner | ||||||
| – Distal padding | ||||||
| – New socket | 7 | 21% | 4 | 20% | 11 | 21% |
Trans-tibial amputation stumps and fitting, ICRC Project.
| Vietnam MUKTI | Vietnam NISHA | Total, ICRC-HOC Vietnam | ||||
|---|---|---|---|---|---|---|
|
|
41 | 40 | 81 | |||
|
|
||||||
| – Users of investigated prosth. | 41 | 100% | 40 | 100% | 81 | 100% |
| – Wear, hrs/day | 14 | 6 – 14 | 14 | 3 – 15 | 13 | 3 – 14 |
| – Walks >1 km | 41 | 100% | 40 | 100% | 81 | 100% |
| – Walks <1 km | 0 | |||||
| – Intensive users | 37 | 90% | 33 | 83% | 70 | 86% |
| – Moderate/light users | 4 | 7 | 11 | |||
| – Non-users | 1 | 1 | ||||
| – Bare-foot walking | 0 | |||||
| – Squatting: | 41 | 40 | 81 | 100% | ||
| No squatting | ||||||
| Not asked | ||||||
|
|
2 | 5% | 1 | 3% | 3 | 4% |
| No comfort: | 2 | 1 | 3 | 4% | ||
| – Wear | 1 | 1 | ||||
| – Walk | 1 | 1 | 2 | |||
| Pain: | 2 | 1 | 3 | 4% | ||
| – Stump | 0 | |||||
| – Rest | 0 | |||||
| – Exercise | 2 | 1 | 3 | |||
| – Other | 0 | |||||
| Satisfied | 41 | 100% | 39 | 98% | 80 | 99% |
| Unsatisfied | 0 | |||||
| No opinion expressed | 0 | |||||
| Body-build: | ||||||
| – Average | 20 | 49% | 24 | 60% | 44 | 54% |
| – Light | 6 | 5 | 11 | 14% | ||
| – Heavy | 15 | 11 | 26 | 32% | ||
| – No record | 0 | |||||
| Manual worker | 27 | 37 | 64 | |||
| White collar worker | 14 | 3 | 17 | |||
| No record of work | ||||||
|
|
||||||
| – Short | 4 | 3 | 7 | |||
| – Medium | 23 | 56% | 18 | 45% | 41 | 51% |
| – Long | 14 | 19 | 33 | 41% | ||
| – No record | 0 | |||||
|
|
||||||
| – Scars | 1 | 1 | ||||
| – Ulcers | 1 | 1 | ||||
| – Neuroma | 0 | |||||
| – Bone protrusions | 7 | 17% | 7 | 18% | 14 | 17% |
|
|
14 | 34% | 10 | 25% | 24 | 30% |
| – Pressure induced | 3 | 2 | 5 | |||
| – Cysts, lichnified | 2 | 2 | ||||
| – Sweat, dermatitis | 1 | 4 | 5 | |||
| – Verrucous hyperplasia | 8 | 4 | 12 | |||
|
|
||||||
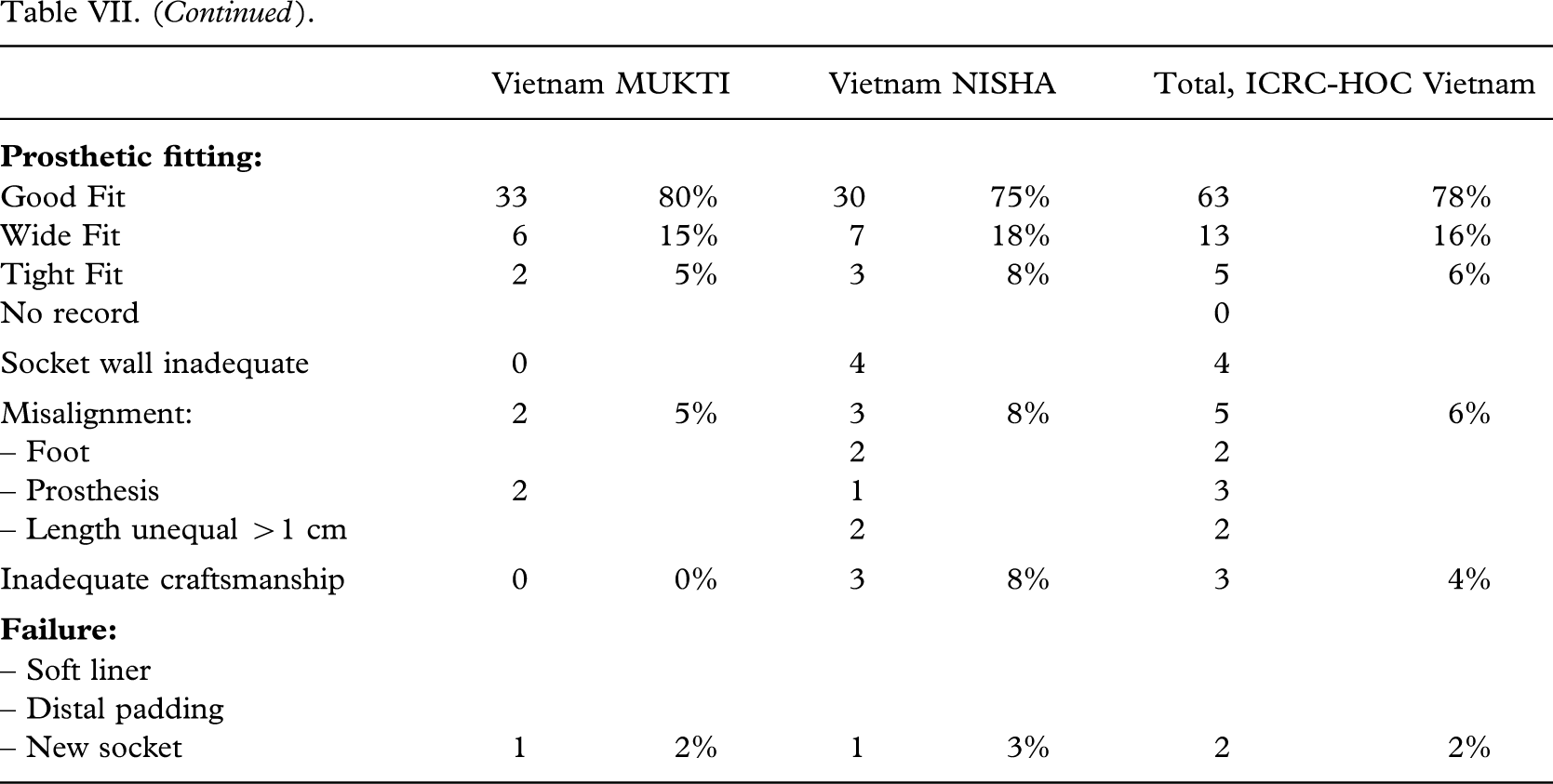
| Good Fit | 33 | 80% | 30 | 75% | 63 | 78% |
| Wide Fit | 6 | 15% | 7 | 18% | 13 | 16% |
| Tight Fit | 2 | 5% | 3 | 8% | 5 | 6% |
| No record | 0 | |||||
| Socket wall inadequate | 0 | 4 | 4 | |||
| Misalignment: | 2 | 5% | 3 | 8% | 5 | 6% |
| – Foot | 2 | 2 | ||||
| – Prosthesis | 2 | 1 | 3 | |||
| – Length unequal >1 cm | 2 | 2 | ||||
| Inadequate craftsmanship | 0 | 0% | 3 | 8% | 3 | 4% |
|
|
||||||
| – Soft liner | ||||||
| – Distal padding | ||||||
| – New socket | 1 | 2% | 1 | 3% | 2 | 2% |
Trans-tibial amputation stumps and fitting, test series and historical series.
| Historical data | ||||||||
|---|---|---|---|---|---|---|---|---|
| Quality benchmarking | Sandcasting | |||||||
| Total, all test series | VIETCOT Vietnam | CSPO-1 Cambodia | Vietnam | |||||
|
|
198 | 67 | 74 | 28 | ||||
|
|
||||||||
| – Users of investigated prosth. | 197 | 99% | 57 | 85% | 74 | 100% | 25 | 89% |
| – Wear, hrs/day | 13 | 3 – 14 | 14 | 9 – 16 | 15 | 3 – 18 | ||
| – Walks >1 km | 175 | 88% | 54 | 81% | 71 | 96% | 22 | 79% |
| – Walks <1 km | 0 | 3 | 3 | 3 | ||||
| – Intensive users | 163 | 82% | 45 | 67% | 70 | 95% | 23 | 82% |
| – Moderate/light users | 29 | 12 | 4 | 2 | ||||
| – Non-users | 2 | 1% | 10 | 15% | 0 | 0% | 3 | 11% |
| – Bare-foot walking | 28 | 0 | 19 | 26% | 1 | |||
| – Squatting: | 81 | |||||||
| No squatting | 0 | |||||||
| Not asked | 0 | |||||||
|
|
23 | 12% | 19 | 28% | 5 | 7% | 11 | 39% |
| No comfort: | 9 | 5% | 14 | 1 | ||||
| – Wear | 2 | 9 | 0 | |||||
| – Walk | 7 | 14 | 5 | 9 | ||||
| Pain: | 20 | 10% | 14 | 21% | 0 | 0% | 10 | 36% |
| – Stump | 3 | 5 | 0 | |||||
| – Rest | 3 | 0 | 0 | |||||
| – Exercise | 14 | 9 | 0 | 10 | ||||
| – Other | 0 | 0 | ||||||
| Satisfied | 171 | 86% | 55 | 82% | 72 | 97% | 25 | 89% |
| Unsatisfied | 5 | 3% | 11 | 2 | ||||
| No opinion expressed | 21 | 11% | 0 | 0 | ||||
| Body-build: | ||||||||
| – Average | 100 | 51% | 37 | 55% | 40 | 54% | 16 | 57% |
| – Light | 29 | 15% | 21 | 28 | 9 | |||
| – Heavy | 51 | 26% | 4 | 6 | 3 | |||
| – No record | 18 | 5 | 0 | |||||
| Manual worker | 129 | 65% | 39 | 45 | 26 | |||
| White collar worker | 25 | 13% | 22 | 29 | 2 | |||
| No record of work | 44 | 22% | 6 | |||||
|
|
||||||||
| – Short | 32 | 16% | 20 | 30% | 18 | 24% | 7 | 25% |
| – Medium | 91 | 46% | 24 | 36% | 38 | 51% | 15 | 54% |
| – Long | 55 | 28% | 18 | 27% | 18 | 24% | 6 | 21% |
| – No record | 20 | 5 | 0 | |||||
|
|
||||||||
| – Scars | 7 | 4% | 6 | 9% | 6 | 8% | 5 | 18% |
| – Ulcers | 4 | 3 | 2 | |||||
| – Neuroma | 2 | 0 | 2 | |||||
| – Bone protrusions | 21 | 11% | 7 | 10% | 4 | 5% | 4 | 14% |
|
|
44 | 22% | 30 | 45% | 6 | 8% | 20 | 71% |
| – Pressure induced | 20 | 10% | 11 | 16% | 0 | 0% | 14 | 50% |
| – Cysts, lichnified | 3 | 2% | 16 | 24% | 5 | 7% | 3 | 11% |
| – Sweat, dermatitis | 5 | 3% | 0 | 0 | ||||
| – Verrucous hyperplasia | 16 | 8% | 3 | 1 | 3 | |||
|
|
||||||||
| Good Fit | 114 | 58% | 33 | 49% | 41 | 55% | 19 | 68% |
| Wide Fit | 50 | 25% | 22 | 33% | 32 | 43% | 5 | 18% |
| Tight Fit | 17 | 9% | 6 | 9% | 1 | 1% | 4 | 14% |
| No record | 17 | 6 | 0 | |||||
| Socket wall inadequate | 9 | 5% | 4 | 6% | 1 | 1% | 5 | 18% |
| Misalignment: | 11 | 6% | 16 | 24% | 14 | 19% | 5 | 18% |
| – Foot | 5 | 16 | 8 | 4 | ||||
| – Prosthesis | 7 | 1 | 10 | 1 | ||||
| – Length unequal >1 cm | 4 | 0 | 1 | 0 | ||||
| Inadequate craftsmanship | 20 | 10% | 10 | 15% | 13 | 18% | 5 | 18% |
|
|
||||||||
| – Soft liner | 6 | |||||||
| – Distal padding | 10 | 1 | ||||||
| – New socket | 27 | 14% | 13 | 19% | 9 | 12% | 2 | 7% |
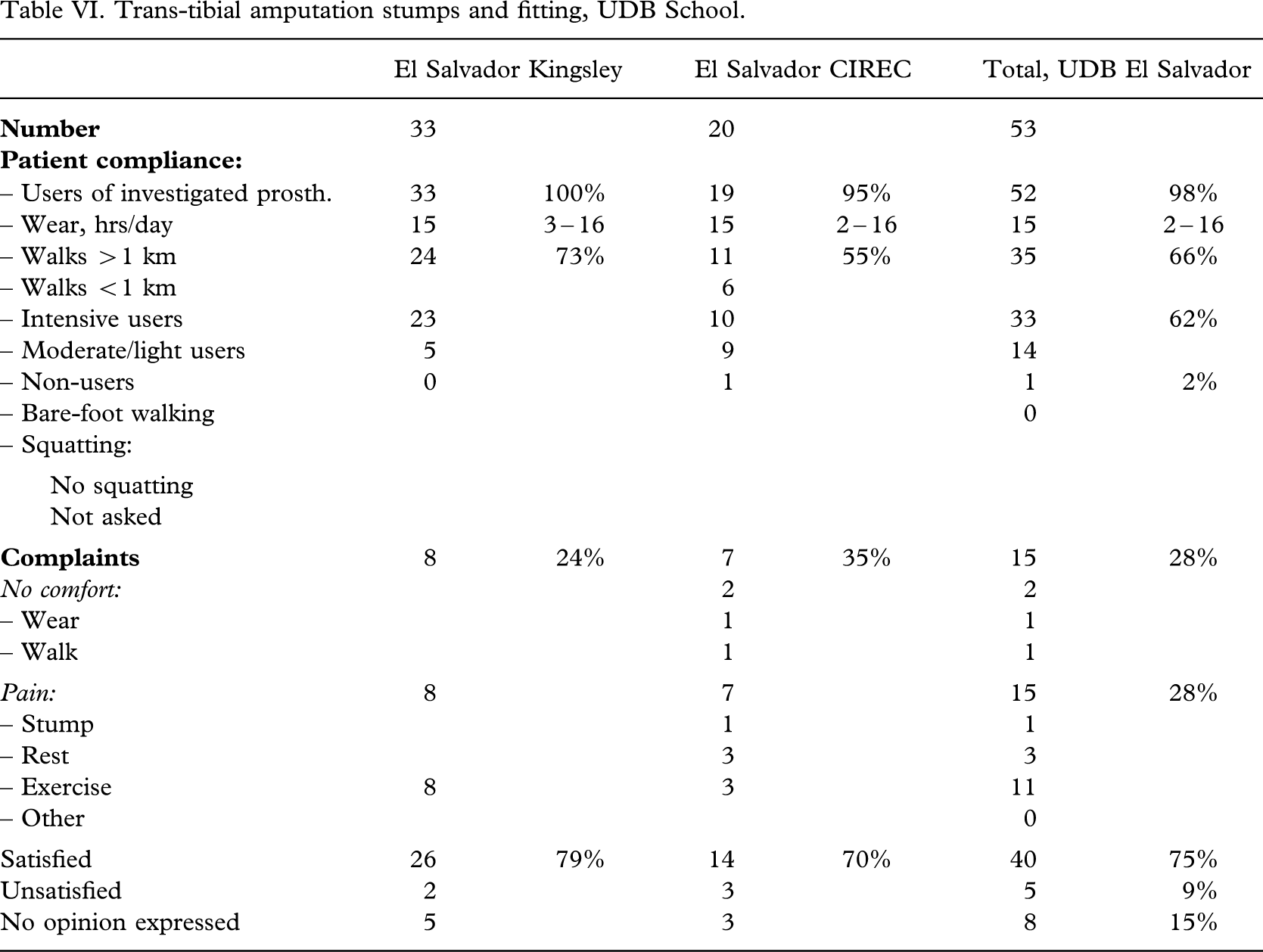
Patient compliance
The patient compliance (Tables V – VI VII VIII) was high; 99% (197 out of 198) being users of the investigated prosthesis with a median wearing period of 15(2 – 16) h/day. Intensive use was recorded for 82% (163 out of 198) on average, but being higher for the CSPO-2 and ICRC-HOC series (P < 0.01). Eighty-eight per cent (175 out of 198) could walk >1 km.
Complaints were noted in 12% (23 out of 198) on average, but being lower in the CSPO-2 and ICRC-HOC series (P < 0.04). Discomfort was recorded in 5% (9 out of 198), and pain in 10% (20 out of 198) solely or in combination. Altogether a minimum of 86% (171 out of 198) were satisfied with the prosthesis, but in 11% (21 out of 194) no opinion was expressed, or recorded. There was a significantly higher percentage of satisfied users in the CSPO-2 group and the ICRC-HOC group (P < 0.0002).
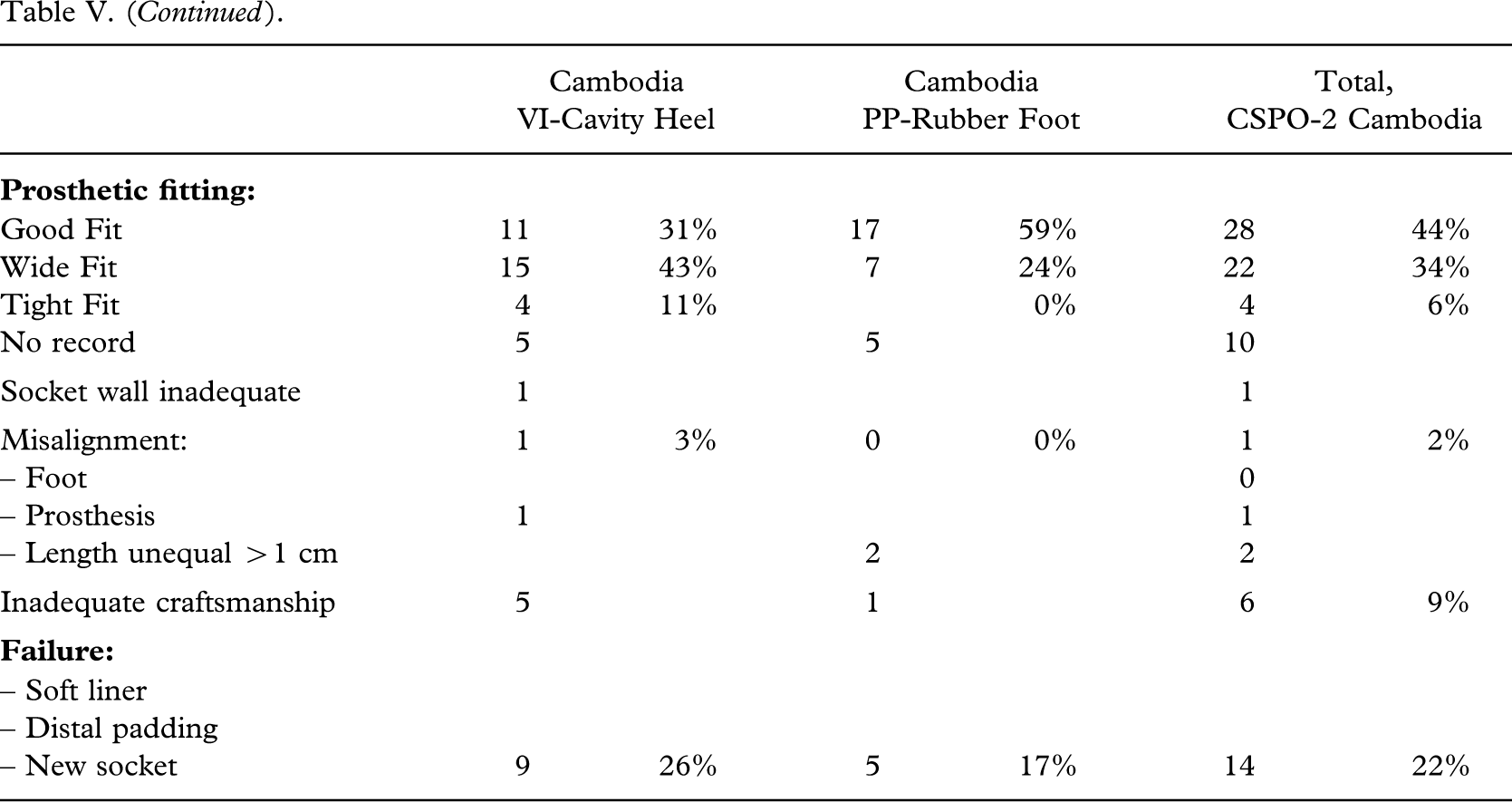
Craftsmanship
A good fit was attained in 58% (114 out of 198), however, ranging from 43% (23 out of 53) to 78% (63 out of 81); the highest figure being achieved by the ICRC-HOC group (P < 0.0003). A wide fit was seen in every fourth patient (25%, 50 out of 198), ranging from 16% (13 out of 81) to 34% (22 out of 64) (P < 0.0003).
An inadequate socket wall height (>2 cm) was recorded in 5% (9 out of 198). Misalignment (>20°) was encountered in 6% (11 out of 198), which is better than both former series (Jensen et al. 2005a; 2005b) with the CSPO-2 group (P < 0.05), and better than the benchmark series (Jensen et al. 2005a) with the ICRC-HOC group (P < 0.0001). Inadequate craftsmanship, which was defined as two errors or more in respect of fit, socket wall, alignment and length (±2 cm), was encountered in 10% (20 out of 198), ranging from 4% (3 out of 81) in the ICRC-HOC group (P < 0.0003) to 21% (11 out of 53).
Failure of the socket resulted in a new socket in 14% (27 out of 198), ranging from 2% (2 out of 81) in the ICRC-HOC group (P < 0.002) to 21% (25 out of 117) for the others (P < 0.0008).
Discussion
ISPO has now conducted clinical field tests of trans-tibial prostheses in eight series from low-income countries in tropical areas of the world (Jensen and Heim 2000; Jensen and Raab 2002; Jensen et al. 2005a; 2005b). All these series have in common the use of the ICRC developed system for polypropylene socket forming over a positive stump model (Verhoeff et al. 1999). The results have been fairly consistent.
ISPO published quality benchmarks based on records from two Category-II schools for training and education of orthopaedic technologists, but was concerned that the benchmarks were not rigorous enough (Jensen et al. 2005a).
In the present series a third Category-II school in El Salvador has been added. It is noted that the products from this school being supplied to amputees do not meet the previously recommended benchmarks (Jensen et al. 2005a) on patient compliance and technical demands. There is no obvious explanation to be found in the records. It is noted, however, that the follow-up rate was the lowest yet seen. It seems evident that the school needs improvement in their check-out procedures. A higher engagement by the teachers in this process is required, as it is in the fit and alignment that the school falls short. This same engagement is of course necessary in all schools (Jensen et al. 2005a).
The satellite workshops to CSPO performed better than the recommended benchmarks apart from the socket fit. That was found good in 44%, but wide in 34%, which is not an unusual finding in tropical areas (Jensen and Heim 2000). That does indeed lead to an unacceptably high number of new sockets. The staff manning these workshops consists of Category-II graduates from CSPO, who seem to have developed a good sense for quality.
The ICRC-HOC project scored the highest marks. They do have two Category-I professionals and one local Category-II professional on their staff. The Category-I expatriates are not directly involved in the fabrication of prostheses, but do supervise all final check-out procedures which is obviously the most effective, as technical errors or need for socket change were rarely encountered.
Against the background of the findings from workshops that have implemented check-out procedures, it is considered justifiable to make the benchmarks more rigorous. As seen from Table IX the authors suggest limiting the range for all measures to ±5% and reducing acceptance of discomfort and pain to 5 ± 5% each and for misalignment to 10 ± 5%.
Quality benchmarks for TT-prosthetics.
| Before | Recommended now | |||
|---|---|---|---|---|
|
|
95% | ±5% | 95% | ±5% |
| – Non-users | 5% | ±5% | 5% | ±5% |
| – Walks >1 km | 90% | ±10% | 90% | ±5% |
| – Discomfort | 10% | ±10% | 5% | ±5% |
| – Pain | 10% | ±10% | 5% | ±5% |
| – Satisfaction | 90% | ±10% | 90% | ±5% |
|
|
||||
| – Good socket fit | 60% | ±10% | 60% | ±5% |
| – Misalignment | 15% | ±10% | 10% | ±5% |
| – Insufficient craftsmanship | 10% | ±10% | 10% | ±5% |
| – Socket change needed | 10% | ±10% | 10% | ±5% |
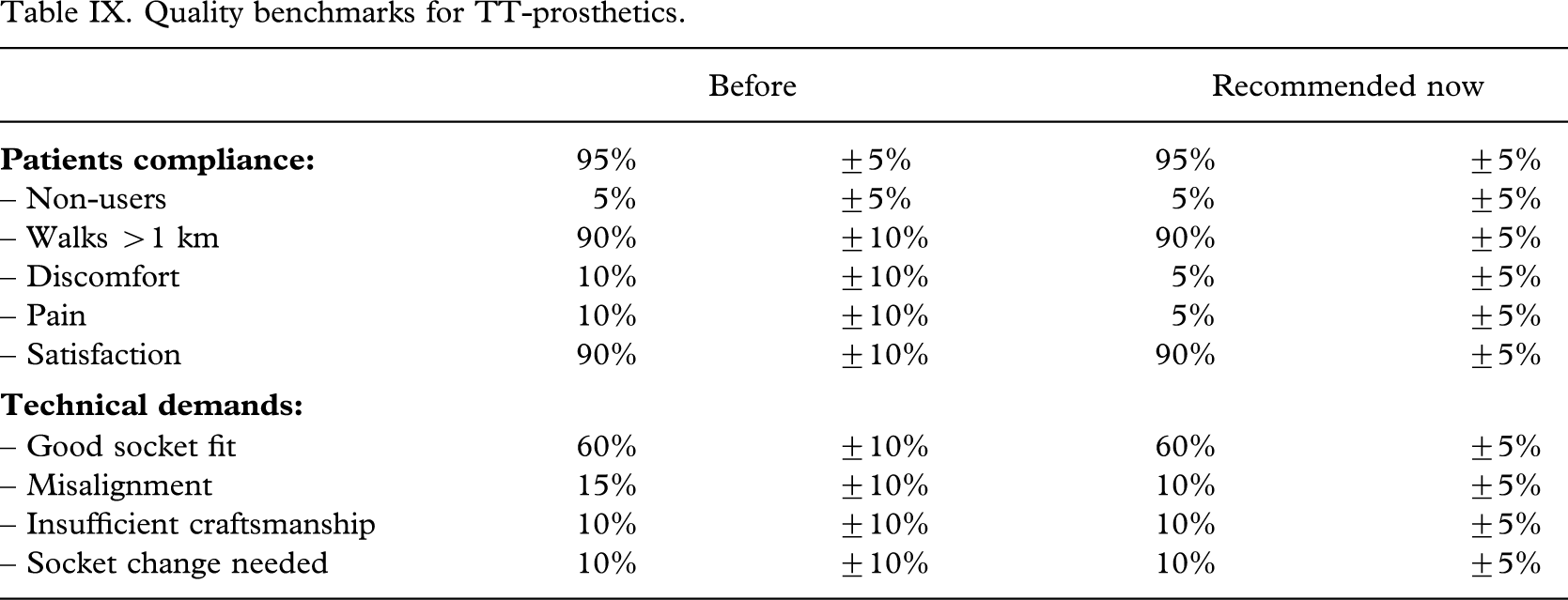
In conclusion, the previously suggested quality benchmarks for polypropylene trans-tibial prostheses can be made more rigorous and should be easily attainable provided the check-out procedures are improved. For the Category-II schools providing patient service it is emphasized that supervision of the check-out procedures is crucial to minimize technical errors.
Footnotes
Acknowledgements
The study was sponsored by the Leahy War Victims Fund, United States Agency for International Development (grant no. HRN-G-00-00-00015-00). The opinions expressed in this paper are those of the authors and ISPO, and do not necessarily reflect the views of the USAID.