
Abstract
Background:
Flat foot in children is a common deformity in which the medial longitudinal arch is reduced or eliminated.
Objectives:
The objective of this article was to compare flat foot and healthy children on the displacement of the center of pressure and walking parameters in children with two common orthoses (functional foot orthosis and medical shoe).
Study design:
Comparative study.
Methods:
This study included 30 children with flat foot and 20 healthy children as a control group. The step length and width, walking velocity, symmetry, and center of pressure (CoP) displacements were recorded and compared for three conditions: functional foot orthosis and regular shoe, a medical shoe and barefoot.
Results:
The results from the CoP displacements showed that the regular shoe with functional foot orthosis caused a significant decrease in the level of displacement of the CoP in flat foot children. The findings indicated a significant improvement in symmetry of steps and walking speed with the functional foot orthosis in comparison to the medical shoe in flat foot children.
Conclusion:
The CoP displacement was decreased and the percentage of gait symmetry and walking speed were increased by the use of regular shoes with a functional foot orthosis in comparison to the medical shoes.
Clinical relevance
An orthopaedic shoe can be expensive, and in particular heavy with most children reluctant to wear it. This study focussed on the CoP displacement and selected gait parameters with an orthopaedic shoe and functional foot orthosis, and showed that a combined prescription of a functional foot orthosis and with regular shoes may be a useful alternative for children with moderate flat foot.
Introduction
Flexible flat foot is a common deformity in children. Due to the abundance of adipose tissue at birth and during infancy, there is no medial longitudinal arch in the foot. When the child starts to walk, the medial plantar arch will begin to form. At the age of 2–6 years, the development of the medial longitudinal arch is rapid. 1 If it is present when the patient is sitting, but disappears when the patient stands, the deformity is called a flexible flat foot.2,3 At the age of 6, the advancement of the medial longitudinal arch of the foot becomes more critical, therefore assessment of the deformity prior to this age may be useful. 4 People with flexible flat foot feel pain during prolonged standing. 5 Initial symptoms of flexible flat foot are as follows: plantar fasciitis, ligament laxity, fatigue, and instability of the internal structure of the foot.6,7 Over time, this excessive mechanical force on the medial longitudinal arch is transmitted to the more proximal structures of the knee, hip, and spine. 5 Pronation is considered an essential movement in gait, an adapter on uneven surfaces and a shock absorber. 8 Excessive pronation develops in flat foot. 9 Hyperpronation together with internal rotation applies critical forces to the lower extremities. 10 Flat foot may be associated with muscle disorders such as Achilles tendinopathy,7,11 stress fracture, 11 patellofemoral joint pain, 12 and back ache. 13 Flat foot in children is often identified by parents who are concerned about structural problems and pain in their children. Due to the effect of medical shoes to treat this deformity, the approach is embedded within the culture of many families with most parents choosing a medical shoe for the child to treat this deformity. Additionally, doctors conventionally prescribe medical shoes for children.2,14
Management of flat foot varies from observation and surgery to physiotherapy and orthotic treatments. 15 Orthotic treatment involves a variety of custom-made orthoses, prefabricated orthoses, arch supports, heel modifications, and medical shoes. 16 McCulloch et al. 9 described orthotics as a means to control the amount and rate of subtalar joint motion and also to restore normal biomechanical movements in the subtalar joint and the other joints of the lower extremities. Although orthoses are widely used in the treatment of flexible flat foot, limited research is available on the kinematic effect of orthoses, particularly on the rearfoot. 17 In order to establish a better understanding of the role of foot orthoses on gait in children with flexible flat feet, temporal and spatial parameters, and the centre of pressure (CoP) displacement may provide useful information in terms of stability and foot function. Research in a standing position shows that anterior–posterior CoP displacement in patients with severe pronation is more than that of medial–lateral displacement. While persons with excessive supination have more mediolateral displacement of CoP, 19 evidence shows that medial displacement is caused by orthosis. 20 A study pertaining to the movement of the CoP during barefoot walking in healthy persons and individuals with a low medial longitudinal arch showed that displacement and the velocity of the CoP were mainly concentrated on the medial longitudinal arch. Yet in individuals with a high medial longitudinal arch, the CoP was more on the lateral side. 21 According to Redmond et al. and Chen et al., orthoses can increase walking speed.22,23 Yet a study by Selby-Silverstein et al. 24 showed that walking speed can be reduced by wearing orthoses in persons with flat foot. However, what remains unclear is that whether the administration of medical shoes in children with flat foot is essential and if foot orthoses with regular shoes has a similar effect in children with flexible flat feet.
Shoes can change the displacement of the CoP path, so that it will shift the ground reaction force and change the torque and forces applied to the body. 25 Despite the high prescription of medical shoes for children with flat foot, evidence shows that medical shoes are not necessary at a very young age.7,26 Determining the effect of an orthosis on CoP displacement in flat feet may aid in better understanding of the body’s compensatory mechanisms. Currently, the existing literature is unclear on the displacement of the CoP and velocity of walking. Therefore, this study aimed to investigate the CoP displacement and various gait parameters while wearing functional foot orthosis with a regular shoes and medical shoes in children with flat foot. Our hypothesis was that the functional foot orthosis in combination with a regular shoe will have no significant effect on the CoP displacement compared to the orthopedic shoe. We also surmised that the functional foot orthosis will improve gait parameters such as gait symmetry and velocity.
Methods
Subjects
A total of 62 children were examined, of which 30 were selected as the flat foot group, 20 were selected as healthy children, and 12 were excluded. Children were matched for height and weight. For the flat foot group, children were required to present with bilateral flat foot without any other structural deformity. Prior to the test, foot posture was determined using the Foot Posture Index (version 6). According to this index, children with a score of +6 to +9 were considered as having an average flat foot and +10 to +12 as having a severe flat foot. Following this, children in the range of +6 to +12 feet of postural parameters were selected for this study. A randomized method was used for the sampling from the flat footed children who were referred for a new pair of shoes. Those children whose medical shoes had corrective wedges were excluded from the study. Following examination and medical evaluation, a consent form was signed by parents of children. This was then followed by each group (flat foot and healthy) performing the tests. Both groups walked with the new medical shoes on the testing day to become accustomed to the shoes. Ethical approval was granted from the Ethics Committee at Tehran University of Medical Sciences before the study commenced.
Six main criteria used for the Foot Posture Index are as follows: 27 (1) Palpation of the talus (2) curvature of the upper and lower lateral malleoli, (3) calcaneal position in the frontal plane, (4) talonavicular joint, (5) medial longitudinal arch of the feet, and (6) adduction and abduction of the forefoot on the rearfoot.
Children were assessed prior to the test and were excluded from the study if any of the following was observed:
Contracture of soft tissue;
Genu varum or valgum;
Structural congenital deformity;
Lower extremity fracture;
Neurological problems such as cerebral palsy, polio, and spina bifida;
History of foot and ankle surgery or trauma in the past 6 months;
Leg length discrepancy.
Orthotic devices
Design characteristics and structure of the medical shoes were required to be equal for all the subjects. Therefore, all the shoes were custom made at the Iranian Red cressent in Tehran. All the medical high-top shoes were made of leather and had a wide toe box, with internal counter in the heel area. The orthosis in the medical shoe was made from polyethylene (PE) shore 55. All the functional foot orthoses were manufactured using thermoplastic low-density PE (Figure 1). In addition, the height of the medical arch support in the medical shoe and the functional foot orthosis were identical.

Orthotic devices used in this study: (a) medical shoe and (b) functional foot orthosis.
Apparatus and test procedure
Gait parameters and CoP displacement were obtained using the Balance Master, Neurocom. The system had a 2-m force plate (Figure 2). All the tests were performed in three conditions: walking with the medical shoe, walking with the regular shoe and functional foot orthosis, and barefoot. This test procedure was the same for the healthy children.

Neurocom system.
Prior to the test, the child was informed of the test procedure and was required to practice before the main test. For each of the three conditions, three trials were collected using a mid-gait protocol. If any child, hesitated or stumbled, the process was repeated. Data were collected from both feet, but only the right was analyzed. All data was recorded at 100Hz. Step length, step width, step symmetry, and the displacement of the CoP were recorded. The CoP displacement was defined as the summation of all ground reaction forces on the force plate representing the change of center of gravity (COG) above the force plate. The displacement of CoP can be measured in the antero- posterior and the medio- lateral directions. For this study however, the instantaneous changes of CoP displacement were measured in the medial–lateral direction. All data were collected on the same day. The children were allowed 5 minutes of rest between each test. The test order was randomized for each child to minimize learning effect.
Statistical analysis
The mean and standard deviation (SD) of variables were calculated for each subject. Repeated measures analysis of variance (ANOVA) was used to compare the three conditions. If significant, paired t-tests were further used as a post hoc. Regression coefficient tests were conducted to examine the correlation of underlying index with other variables. Data analysis was performed using the SPSS 17 and level of significance was considered less than 0.05.
Results
In this study, 30 children with flat foot (18 males and 12 females) and 20 healthy children (12 males and 8 females) (average age of 7.76 ± 1.4 years) participated as the control group. The average height and weight of the children with flat foot were 123.06 cm and 31.40 kg, respectively. In the healthy children, the average height and weight were 127.91 cm and 32.81 kg, respectively (Table 1). The mean and standard deviation (SD) of CoP for the two groups are presented in Table 2. In children with flexible flat foot, mean displacement of the CoP with the medical shoe decreased in comparison to the barefoot condition (P < 0.05). Although less displacement was observed in the CoP with the functional foot orthosis in comparison to the orthopedic shoe, the difference was not statistically significant (P > 0.05). Healthy children showed no significant difference between the three conditions; however, the average displacement of the CoP in the regular shoe with functional foot orthosis reduced compared to the other two conditions.
The demographic data (mean ± SD) of the participants with flat foot and healthy participants.

SD: standard deviation.
Comparison of three conditions of CoP in the participants with flat foot and healthy participants (mean ± SD).
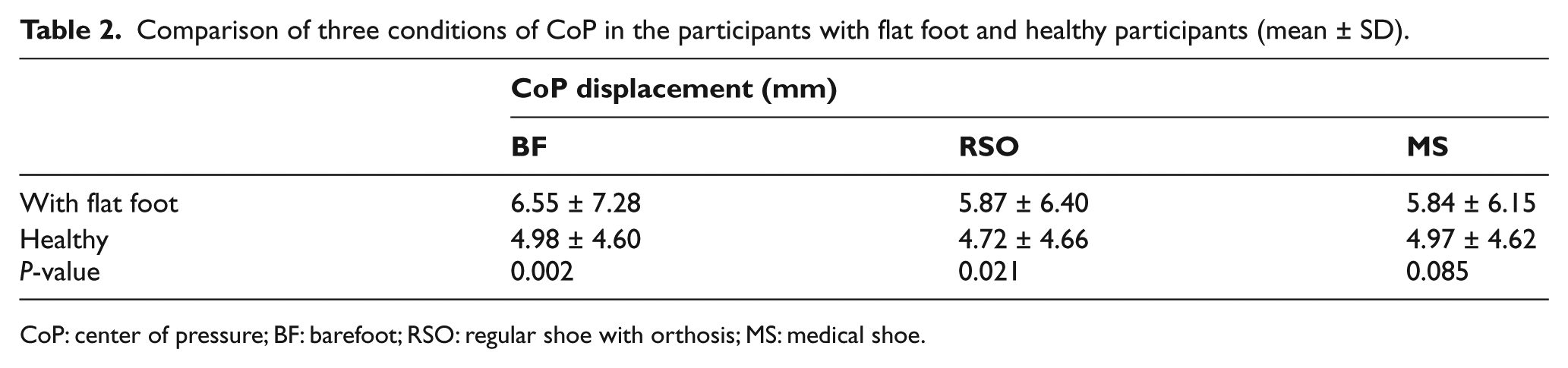
CoP: center of pressure; BF: barefoot; RSO: regular shoe with orthosis; MS: medical shoe.
Gait parameters including the mean and SD of the step length and width, step velocity, and symmetry are mentioned in Table 3. In the subjects with flexible flat foot, the step length increased when wearing functional foot orthosis and medical shoes compared to the barefoot condition. Despite the higher step length observed with the regular shoe with functional foot orthosis compared to the medical shoe, the difference was not statistically significant. The step width of the subjects with flat foot was lower when wearing the regular shoe with functional foot orthosis, but the difference between the conditions with the regular and medical shoes was not significant. In the healthy subjects, the length and width of the steps were higher when wearing the regular shoe with orthosis than the barefoot condition and with medical shoes.
Comparison of three conditions of gait parameters in participants with flat foot and healthy participants.
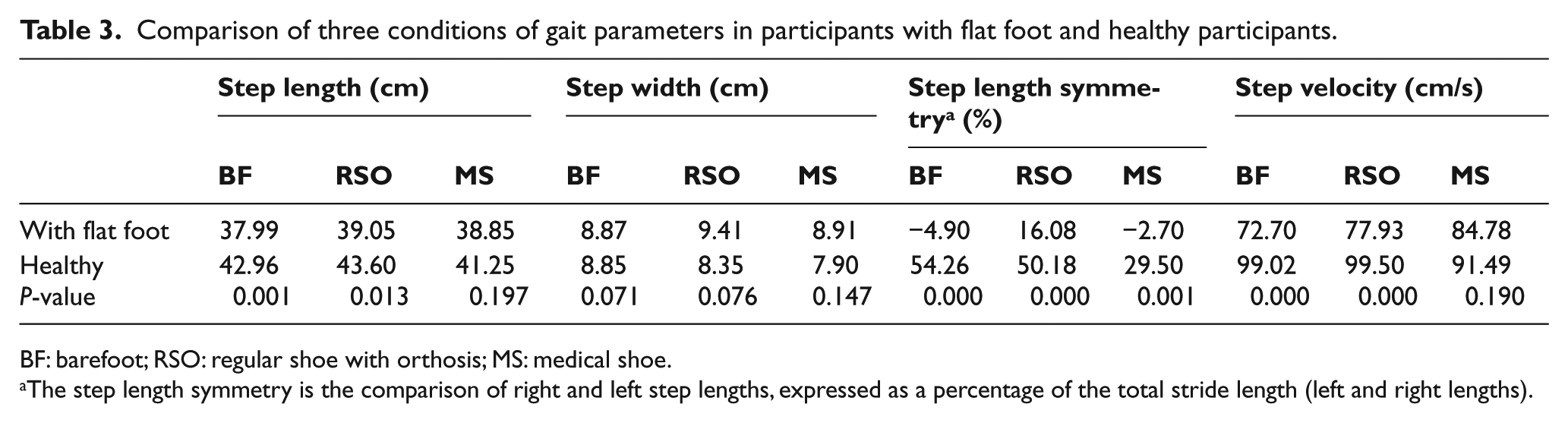
BF: barefoot; RSO: regular shoe with orthosis; MS: medical shoe.
The step length symmetry is the comparison of right and left step lengths, expressed as a percentage of the total stride length (left and right lengths).
In analyzing the parameters of step symmetry in children with flat foot, there was no significant difference between walking barefoot and wearing the medical shoes. Nevertheless, the step symmetry was greatly improved from 4% with the medical shoe to 16% by wearing the regular shoe with functional foot orthosis (P < 0.05). There was no significant difference evident in the symmetry of the steps while barefoot and when wearing the regular shoe. Yet the symmetry of steps decreased with the medical shoes in the healthy children (P < 0.005) (Table 4).
Comparison of three conditions in participants with flat foot (mean ± SD).
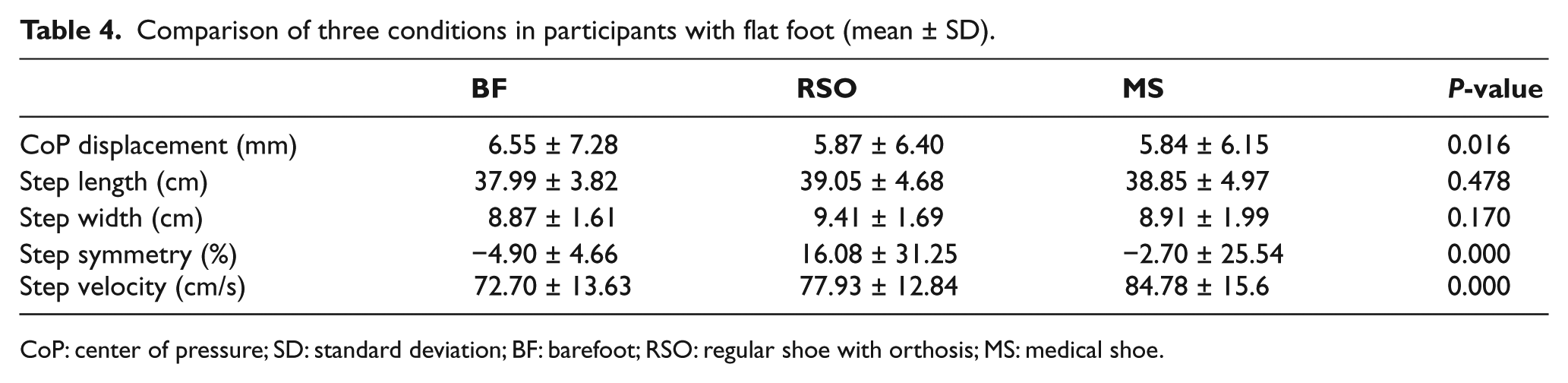
CoP: center of pressure; SD: standard deviation; BF: barefoot; RSO: regular shoe with orthosis; MS: medical shoe.
Discussion
Our basic assumption in this study was that CoP displacement in an orthopedic shoe was similar to a functional foot orthosis with regular shoe, and we assumed that parameters such as step velocity, step length and width, and step symmetry increase with an orthopedic shoe and functional foot orthosis with regular shoe.
In children with flat foot, the average displacement of the CoP in the barefoot condition was 6.5 ± 7.28, and it was decreased by wearing regular shoe with functional foot orthosis and the medical shoes. Both the medical shoes and regular shoe with orthosis significantly reduced the CoP displacement compared to the barefoot condition (P < 0.05). This is in contrast to the findings of Chen et al. 22 that the orthosis had no effect on the CoP displacement in children with flat foot.
Results for the CoP displacement showed that in children with flat foot, wearing the medical shoe or regular shoe with a functional foot orthosis limits the CoP displacement of the feet. However, such effect was not seen in the healthy children (Table 2). The results of the present study are similar to the study by Dixon, 28 whereby an increase in foot pronation resulted in a higher displacement of the CoP whilst walking barefoot. In addition, the average rate of CoP displacement in children with severe flat foot was more than those with mild and moderate flat foot.
Analyzing the gait parameters revealed that the mean step length (39.05 ± 4.6) and step width (9.41 ± 1.6) were not significantly different whilst wearing regular shoe with functional foot orthosis compared to the barefoot condition (Table 3). The mean values of step length and step width were similar for the healthy subjects and the children with flat foot. It might be concluded that the orthosis had no significant effect on the step length and step width. In contrast, Oeffinger et al. and Lythgo et al. had concluded that medical footwear could help children take a longer step.29,30
Moreno-Hernández and Rodríguez-Reyes and Wenger et al. showed that walking speed could be increased by wearing shoes.31,32 Our findings for the children with flat foot comply with their results. Both the medical shoe and regular shoe with orthosis significantly increased the walking speed (P < 0.05) compared to the barefoot condition (P < 0.05). Najafi et al. 33 compared the walking shoes and prefabricated orthoses and observed no significant difference in the walking speed. The study by Redmond et al., 23 on the contrary, was indicative of increase in walking speed with orthoses. In contrast, Selby-Silverstein et al. 24 reported a reduction in the walking speed by wearing orthoses. In our study, healthy children walked slower when wearing the orthoses (mean: 91.49 ± 4.3) as compared to barefoot (mean: 99.02 ± 5.9). Unlike children with flat foot, wearing a regular shoe with functional foot orthosis could not increase the walking speed in the healthy children (Table 3).
In children with flexible flat foot, step symmetry was disrupted by medical shoes. Perhaps, one reason is the mass of medical shoes. However, a regular shoe with a functional foot orthosis improved the symmetry of steps (P < 0.005). The symmetry index was not significantly different in the healthy children with a regular shoe as compared to the barefoot condition. In fact, it might be deduced that walking with insoles did not result in improvement in the healthy children. In both the healthy subjects and the children with flat foot, the symmetry index was severely disrupted (P < 0.005).
The Neurocom system can only identify the rate of CoP displacement, and the CoP trajectory is unclear. Therefore, future studies should employ other measurement tools or systems.
There were limited studies on the dynamic CoP displacement and step symmetry, particularly in the flat foot children, to compare with our results. It was good to compare the results in long term; however, ethically, we were not allowed to impel healthy children to wear medical shoe for longer time.
Conclusion
In general, this article showed that although medical shoes decrease the CoP displacement and increase the walking speed, the step symmetry would reduce. Since the medical shoes are heavy, expensive, and do not have a good appearance, regular shoes with the functional foot orthosis can be suitably replaced for children with flat foot. In addition, to decrease the CoP displacement, a functional foot orthosis can increase the symmetry of steps, step length, and step width.
Footnotes
Acknowledgements
The authors wish to thank all the participants and their parents.
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.