
Abstract
In a prospective, controlled study, 186 prosthetic rubber feet of different designs were fitted to amputees with trans-tibial prostheses. There were 158 amputees available for follow-up. The amputee compliance was good and 89% were satisfied with their device. After 18 months of use one VI-Solid rubber foot from VVAF in Cambodia had failed, as compared to 11% failures with the same foot with a heel cavity, 3% with the EB-1 sandwich construction from POF in Vietnam, all performing significantly better than the 62% encountered with the vulcanized rubber foot from ICRC in Cambodia; the latter representing half of the feet failing in amputees walking bare-footed. Nearly all failures were located at the foot-sole or the keel. The failure rate was 20% for the HI-Cambodia foot after 12 months. After 24 months of use, still only one VI-Solid rubber foot had failed and this foot design was found superior to the others in regard of durability.
Introduction
According to Cummings (1996), who scrutinized 30 years of publications, no relevant publications were found about the rubber Jaipur foot apart from those coming from the group at the SMS Hospital in Jaipur, India. Verhoeff et al. (1999) published the ICRC experience with 43 polypropylene (PP) prostheses in Vietnam and found that 40 rubber feet fabricated locally needed exchange because of wear after 7 – 12 months depending on hours of daily use. Jensen and Heim (1999) found that none out of 10 rubber feet from Veterans International in Cambodia had failed after 19 months. The purpose of this study was to investigate the failure rate of different rubber feet in a prospective, controlled study.
Materials and methods
In five series of trans-tibial amputees the prosthesis provided was the modular PP system developed and marketed by the International Committee of the Red Cross (ICRC), consisting of a drape wrapped PP socket, two alignment discs and a tubular shank part.
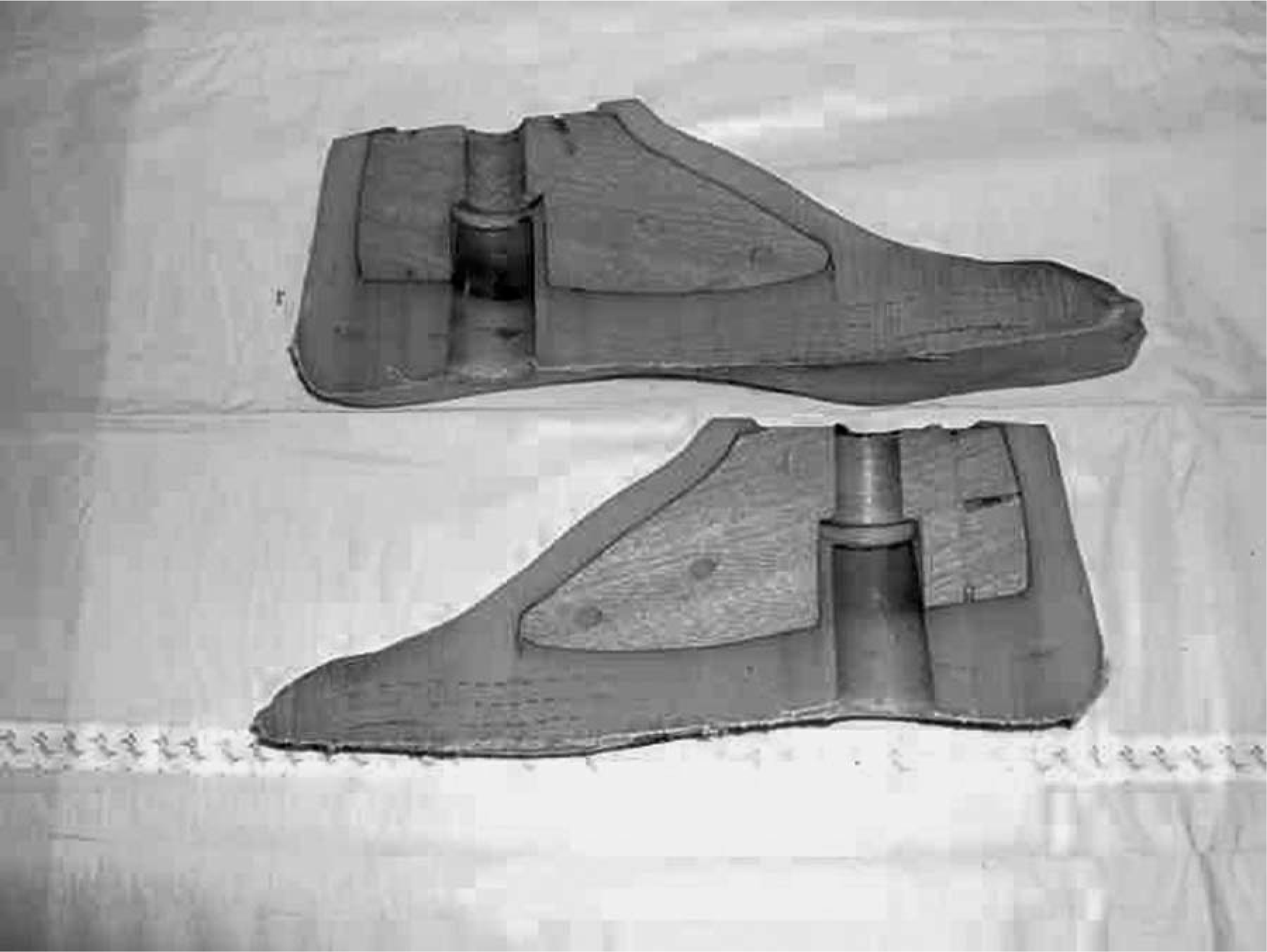
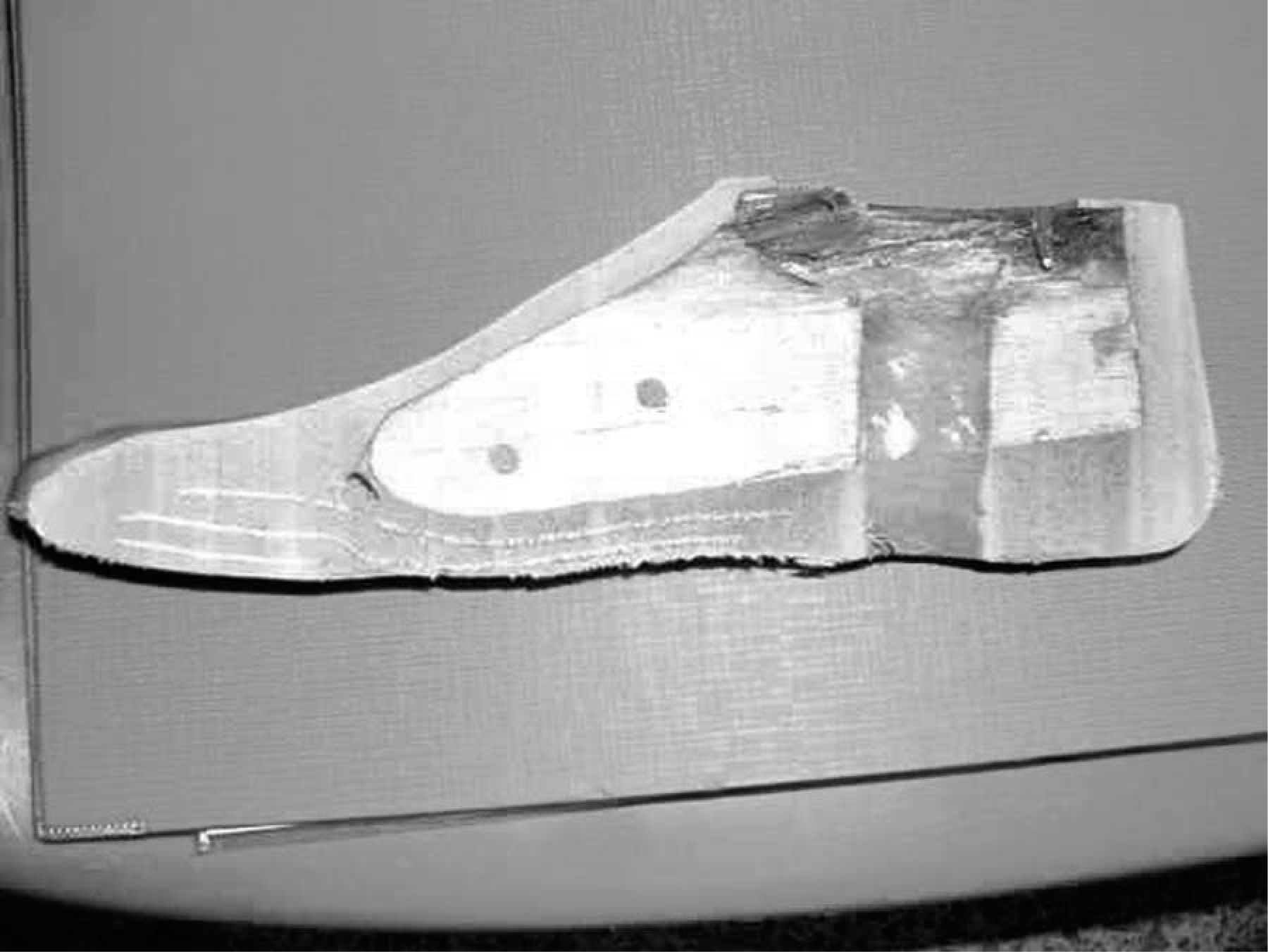
At the Vietnamese Training Centre for Orthopaedic Technology (VIETCOT) in 41 cases the terminal device was a SACH-foot design developed by Prosthetics Outreach Foundation, Hanoi, Vietnam. It consists of a wedge formed wooden keel with a vulcanized textile-rubber sandwich construction for the heel cushion, mid- and fore-foot (Figures 1 and 2).

EB-1 Foot. A sandwich construction of cotton and natural rubber with a wooden keel.
EB-1 Foot. Cross-section.
The VI-Solid foot from Vietnam Veterans of America Foundation (VVAF), Kien Khleang, Cambodia was tested in a further 37 cases at VIETCOT. The internal construction of the foot is a large tooth-shaped PP keel with anchoring holes, tyre-rubber sole and rubber foam heel cushion (Figure 3), and textile reinforcement of heel, mid-foot and dorsum. In 40 amputees another foot from VVAF, Cambodia was tested at the Cambodian School for Prosthetics and Orthotics (CSPO), Cambodia. The difference is that a cavity was formed in the heel cushion to act as a shock absorber (Figure 4). A series of 38 SACH rubber-feet from ICRC, Phnom Penh, Cambodia was tested at CSPO. The PP keel is dog tail formed with multiple anchoring holes and wound with rubber bands. The sole is reinforced with tyre rubber (Figure 5). Finally 30 feet from Handicap International, Phnom Penh, Cambodia supplied to amputees with an early breakdown of an experimental foot (not included in this evaluation) were tested at CSPO. The big tooth PP keel has anchoring holes and is wound with rubber bands. The heel cushion is of PP (Figure 6).

VI-Solid Foot, cross-section. Polypropylene keel rubber foam heel cushion, tyre-rubber reinforced foot-sole and dorsum.
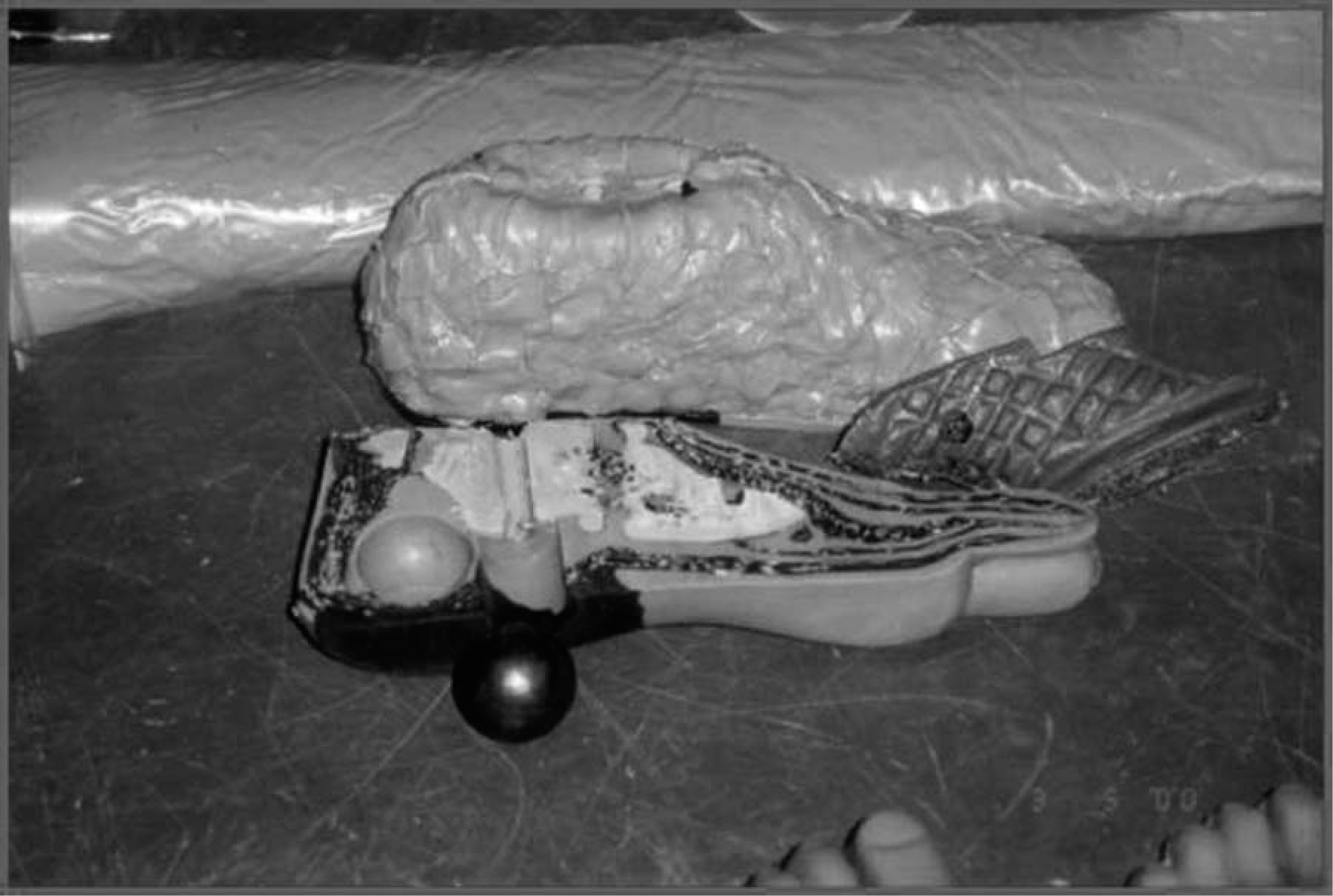
VI-Cavity Foot. A cavity is formed in the heel section by a steel ball during vulcanization.
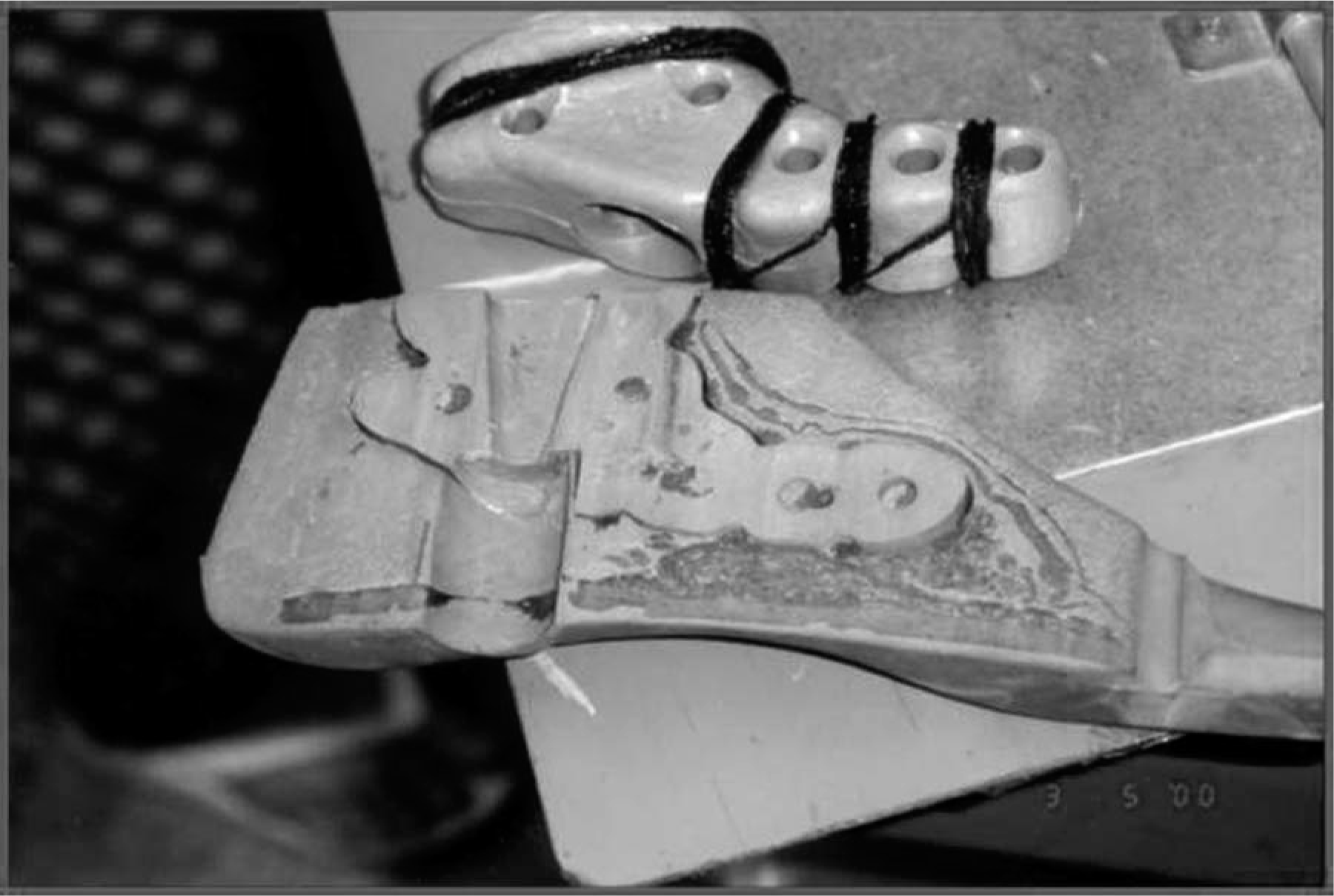
PP-Rubber Foot. The polypropylene keel is dog tail formed with multiple anchoring holes and wound with rubber bands. Tyre-rubber reinforcement of sole.
HI-Cambodia Foot. The big tooth formed polypropylene keel has anchoring holes and is wound with rubber bands. Textile reinforcement of sole and dorsum. Heel cushion made from polyurethane.
The studies were conducted at the ISPO/WHO recognized Category-II schools for prosthetics and orthotics in Vietnam and Cambodia. The surveys were undertaken by teams of a Category-I prosthetist and an orthopaedic surgeon experienced with prosthetic performance studies. The amputees were recruited among cohorts of well-known users of prostheses, who all had availability of at least one more prosthesis at home. Consequently, they did not seek repair of a failed prosthesis but awaited the call for follow-up. The plan was to see the amputees at 9 and 18 months after prosthesis provision, but a half-year delay in delivery of one foot tested in Vietnam, and the need for replacing missing subjects after demilitarization in Cambodia and adding the model used for replacement in Cambodia made it impossible to keep the proposed follow-up schedule. That eliminated the application of rigorous Kaplan-Meier survival statistics. Instead it was necessary to combine such analyses with crude comparisons at 12 and 18 months applying Student's t-test (unpaired, two-tailed, two sample, unequal variance). The follow-up rate was 85% (158/186), varying from 76% (29/38) to 100% (30/30). The study was completed either at failure or at the latest follow-up.
The clinical field testing was conducted in accordance with the system developed by the International Society for Prosthetics and Orthotics (ISPO) (Jensen and Heim 1999; Jensen and Raab 2002).
Demographics and patient characteristics
The median follow-up was 20 (6 – 32) months (Table I), and there was no difference in follow-up between those who failed and those not failing (p = 0.34) in the overall group.
Demographics, trans-tibial amputees with rubber feet.
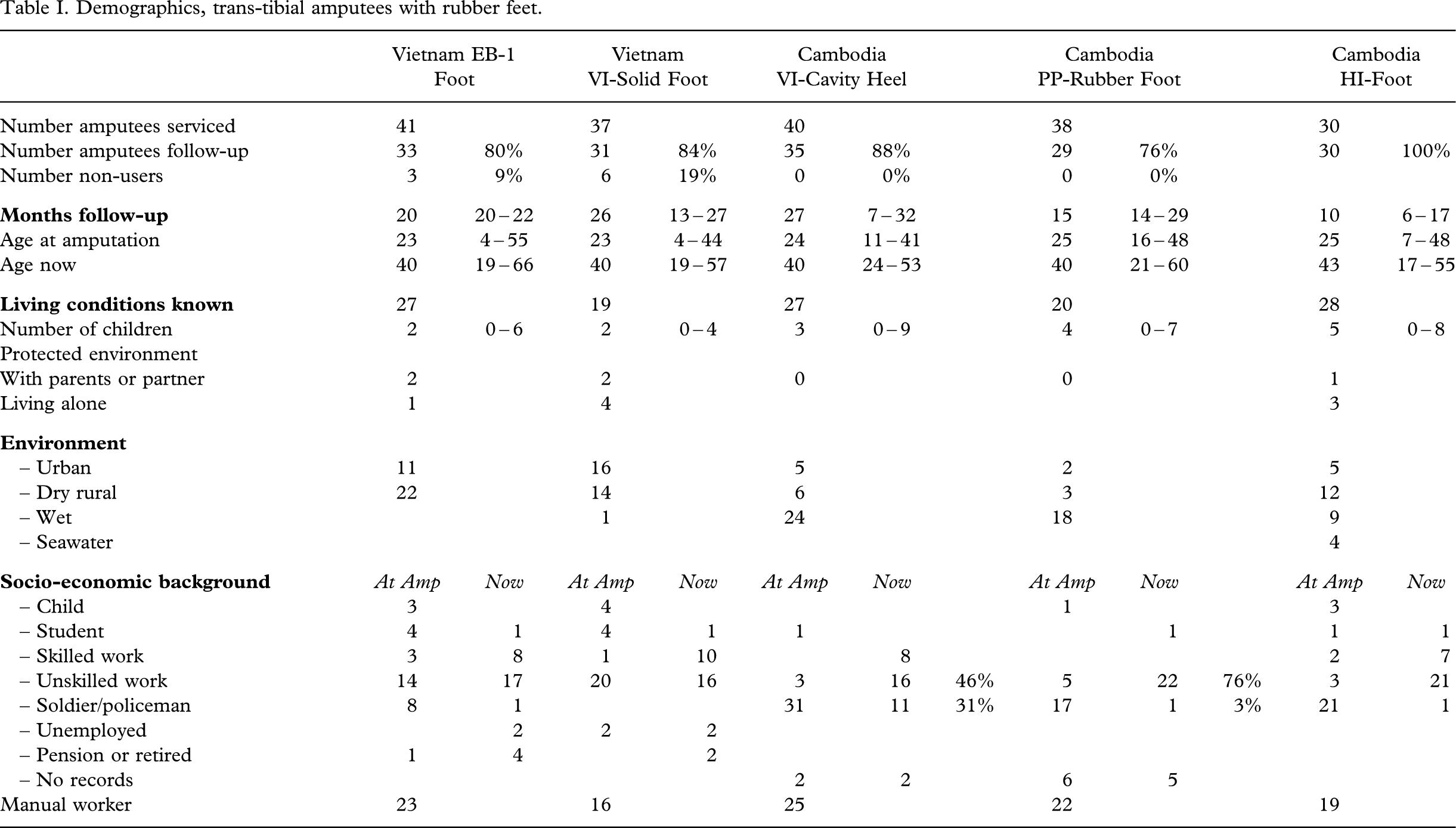
Harold Wood Stanmore assessment system:
Household ambulators Disability-Mobility 1 – 2.
Community ambulators Disability-Mobility 3 – 5.
The amputees had a median age of 24 (4 – 55) years at the time of amputation and 40 (17 – 66) years at the time of follow-up. A total of 61% (96/158) lived in urban or dry rural areas; however, one third lived in wet areas. The majority were now employed in unskilled work, but 49% (77/158) were soldiers at the time of amputation, and in 59% (94/158) war ordnance was the cause of amputation. Nine amputees did not use the prosthesis under investigation, but 94% (149/158) were community ambulators.
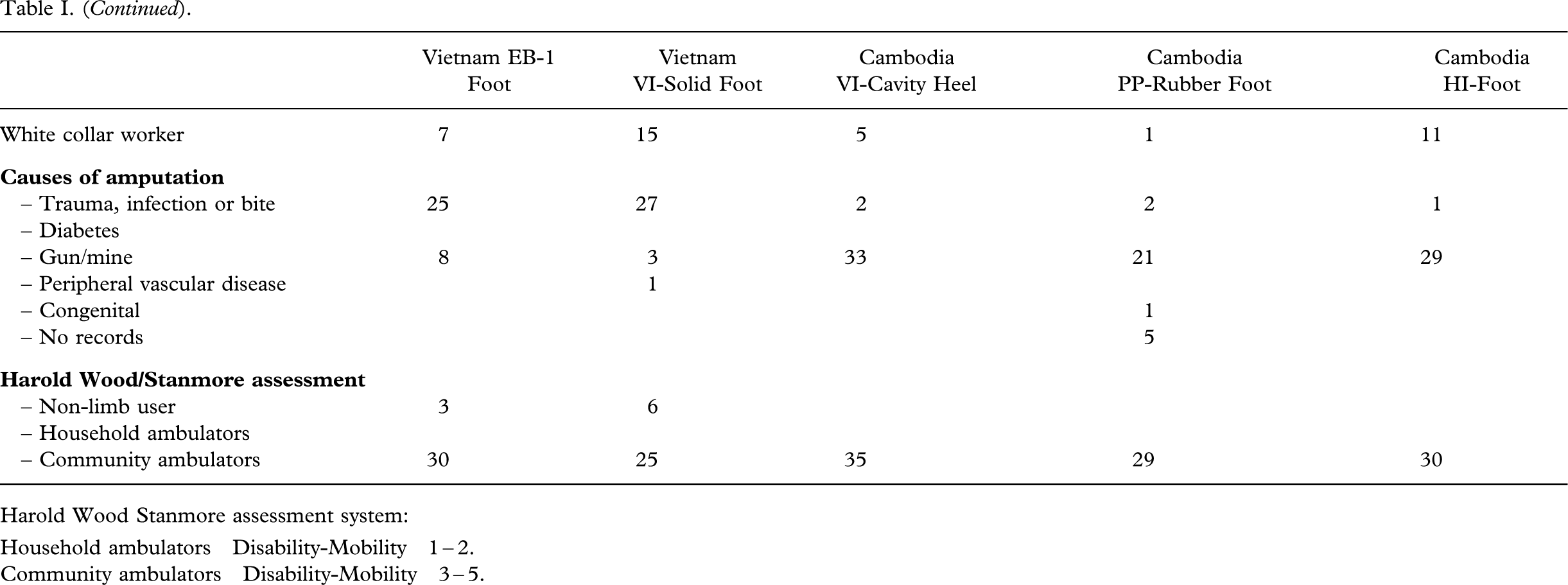
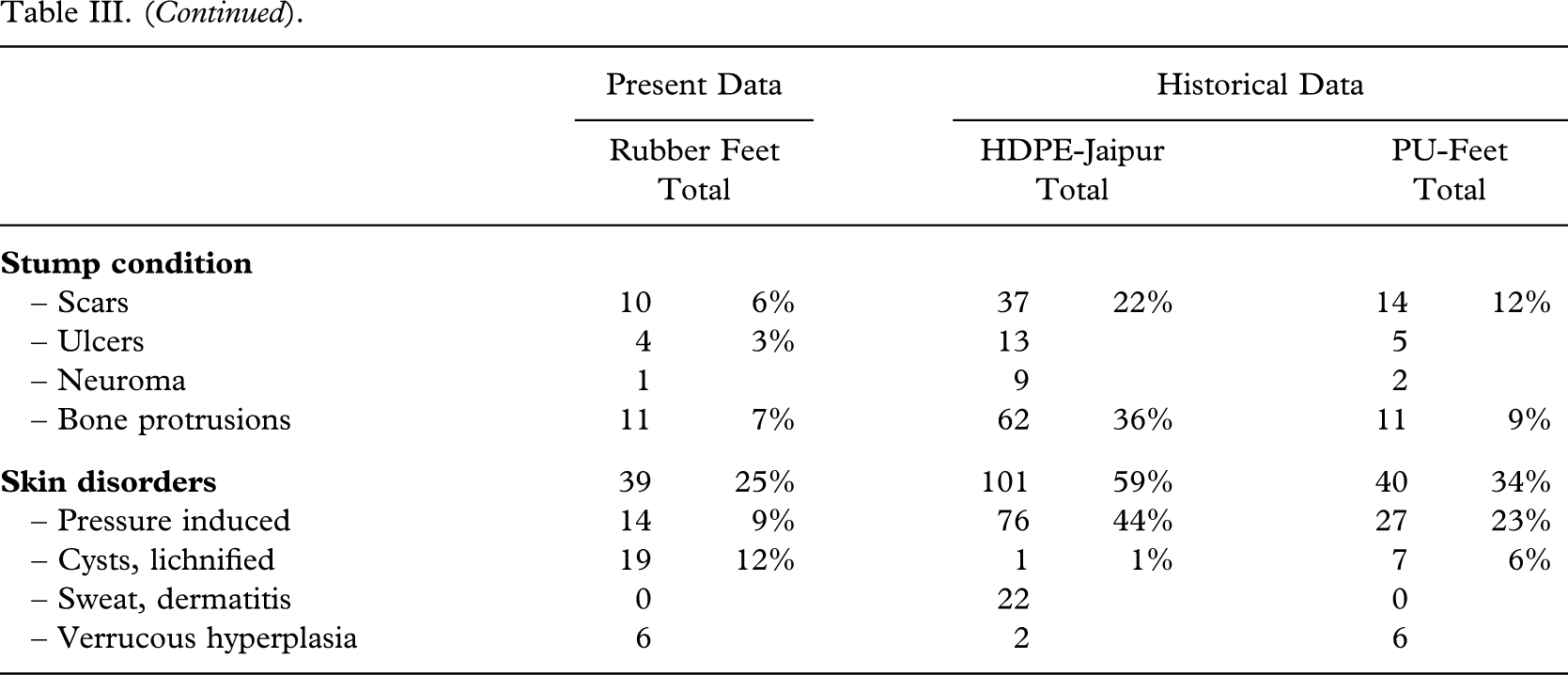
The stumps were straight-forward for fitting (Table II); 72% (104/145) being of medium length or long; only 3% (4/158) having ulcers, and 7% (11/158) bone protrusions. Scars were encountered in 6% (10/158) and 21% (33/158) had pressure induced skin disorders, lichnified skin or cysts. There were no significant differences in relation to demographics or patient characteristics in this series as compared to historical series (Table III).
Patient characteristics, trans-tibial amputees with rubber feet.
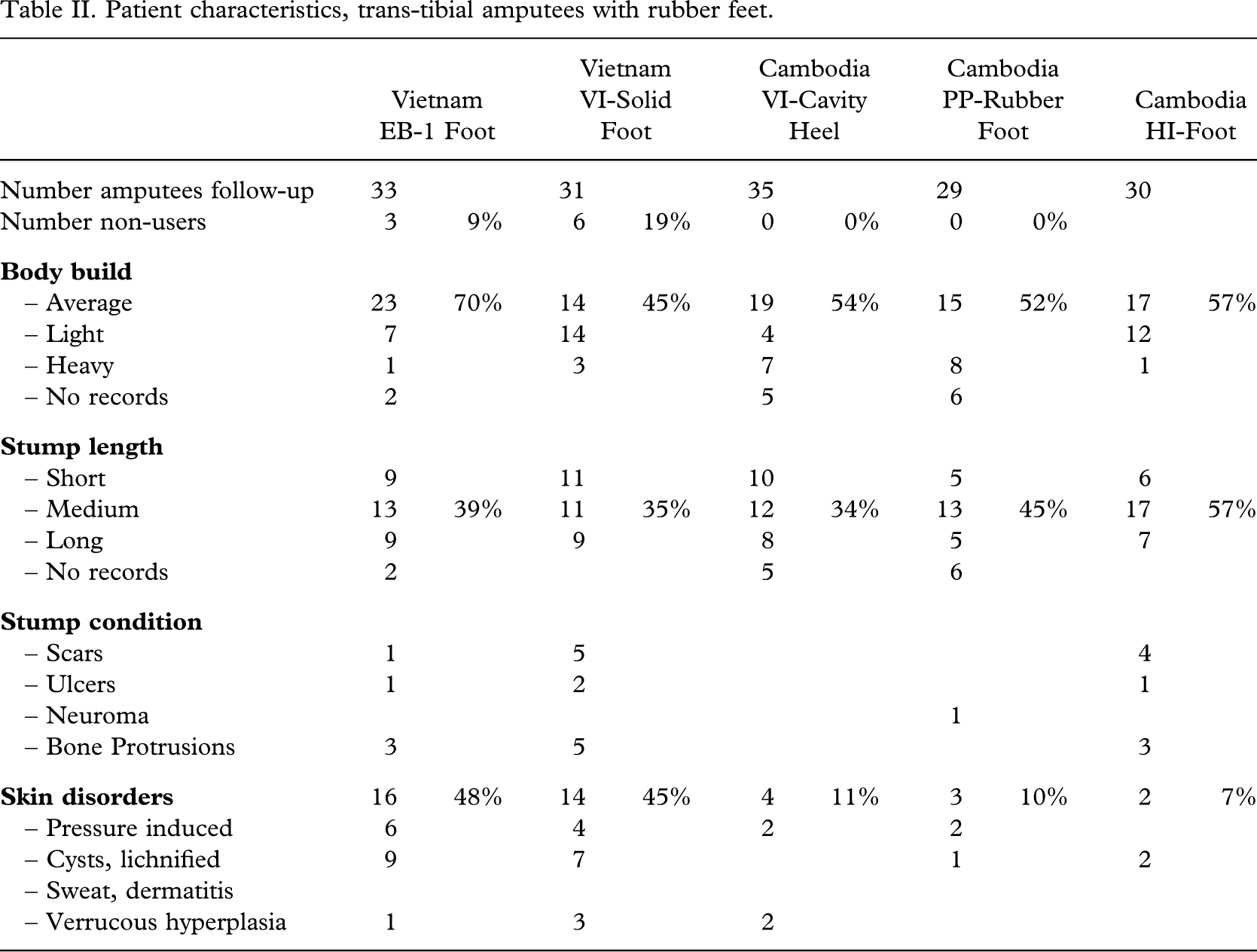
Demographics and patient characteristics, present and historical series.
Patient compliance and craftsmanship
The amputees were wearing their prosthesis for 14 (5 – 16) h daily, and 91% (143/158) walked more than 1 km (Table IV). Some 26% (41/158) walked bare-footed; all being in Cambodia. Intensive use of the prosthesis was recorded in 85% (134/158). Only 16%(25/158) complained about discomfort or pain, and 89% (141/158) were satisfied with the device.
Patient compliance and prosthetic fitting.
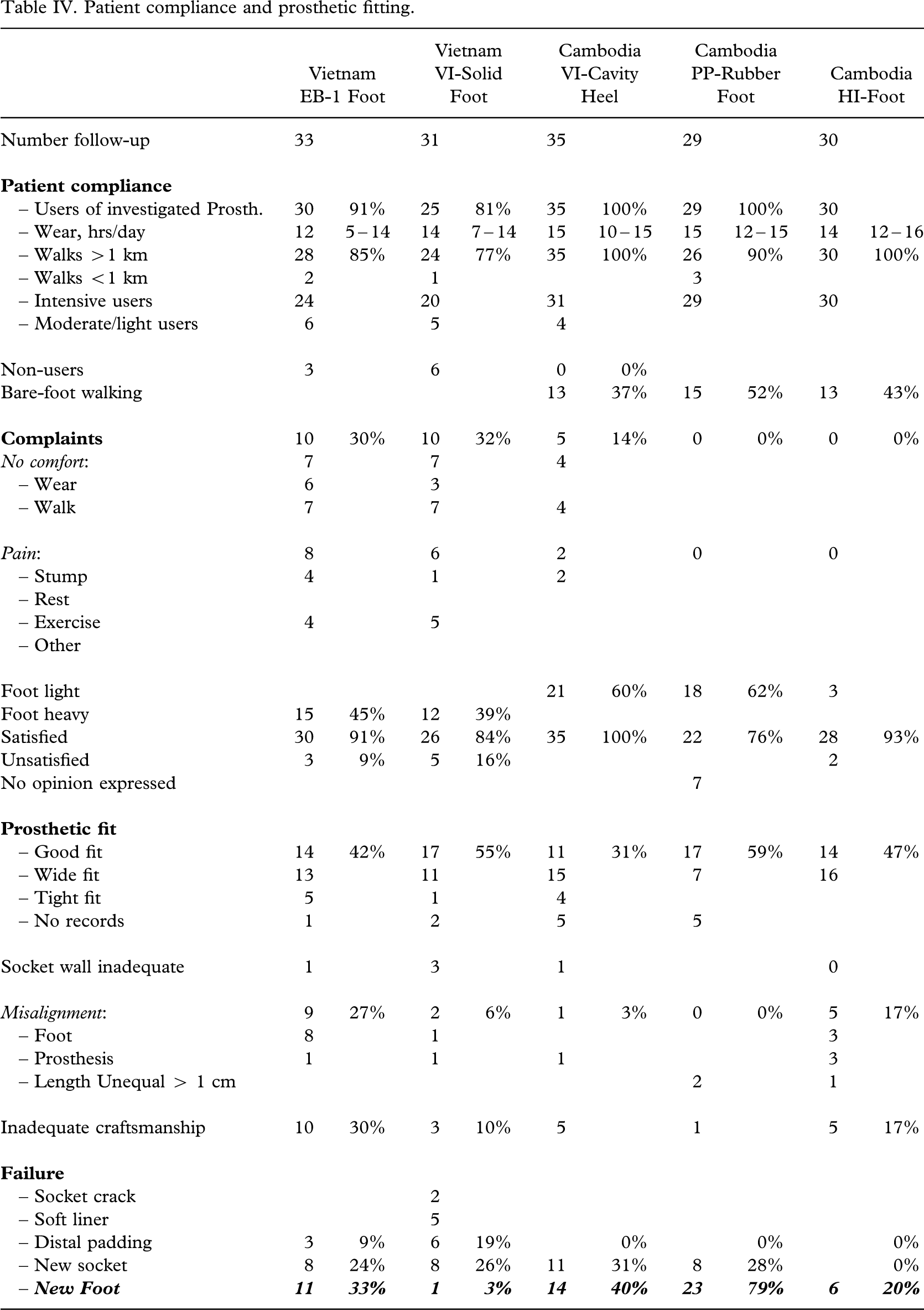
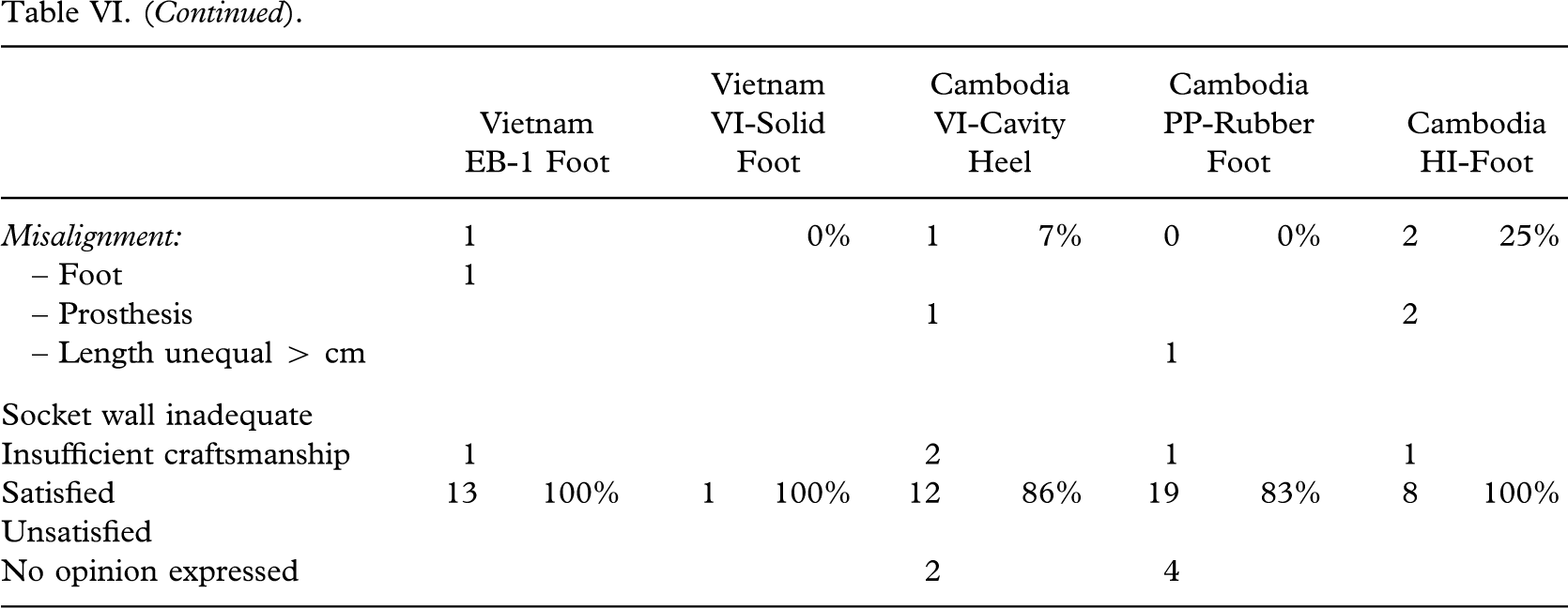
A tight socket fit was found in 6% (10/158), inadequate socket wall in 3% (5/158) and misalignment in 11% (17/158). In 15% (23/158), the craftsmanship was found to be inadequate.
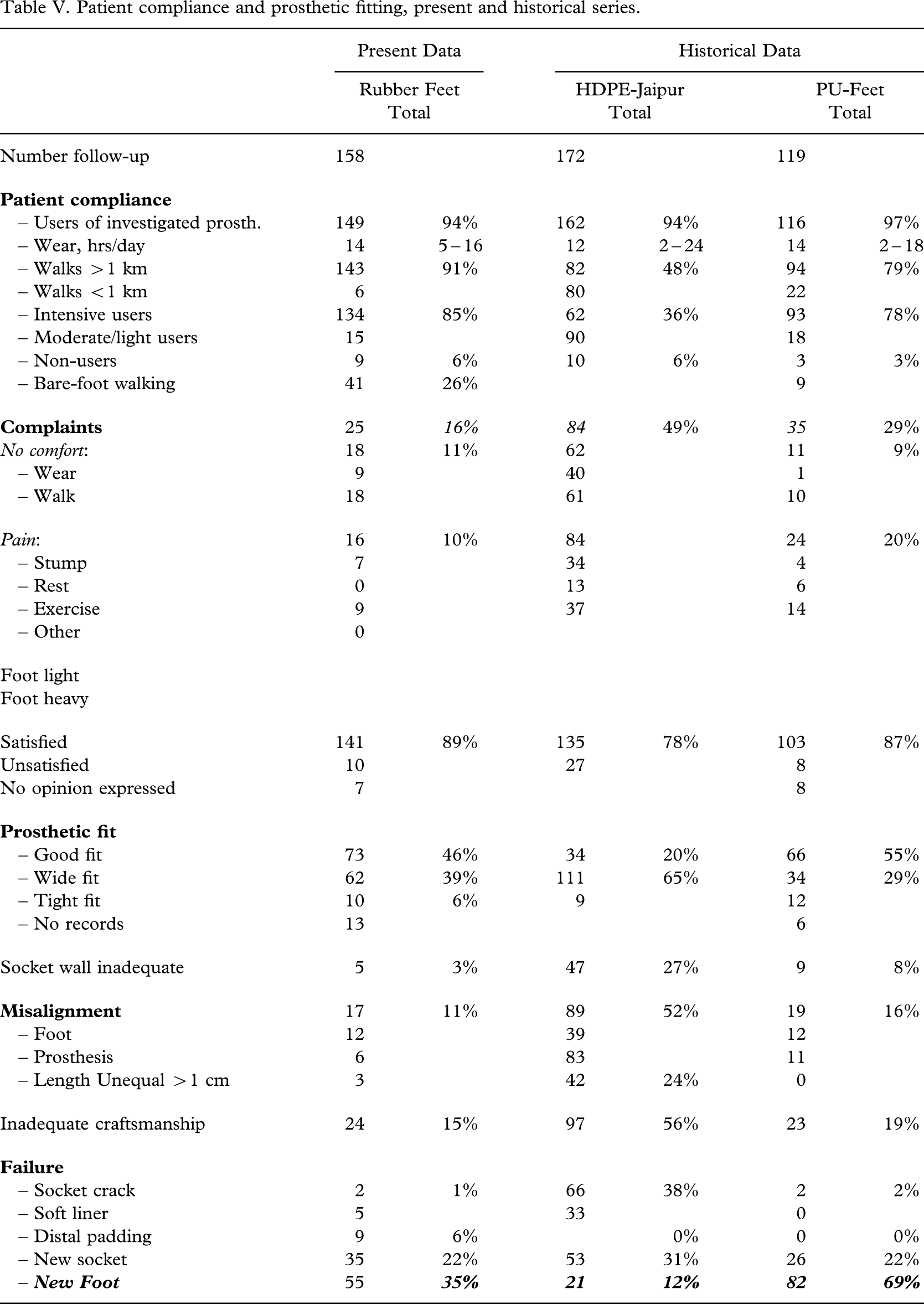
In comparison with four series of amputees supplied with PP feet at the same kind of institutions (Jensen et al. 2006) there were no differences of significance regarding patient satisfaction and craftsmanship (Table V). In comparison with high density polyethylene (HDPE) Jaipur prostheses (Jensen et al. 2004) the present results were better both with regard to patient compliance and not least in respect of adequate craftsmanship (p < 0.000001).
Patient compliance and prosthetic fitting, present and historical series.
Failures of the prosthetic foot
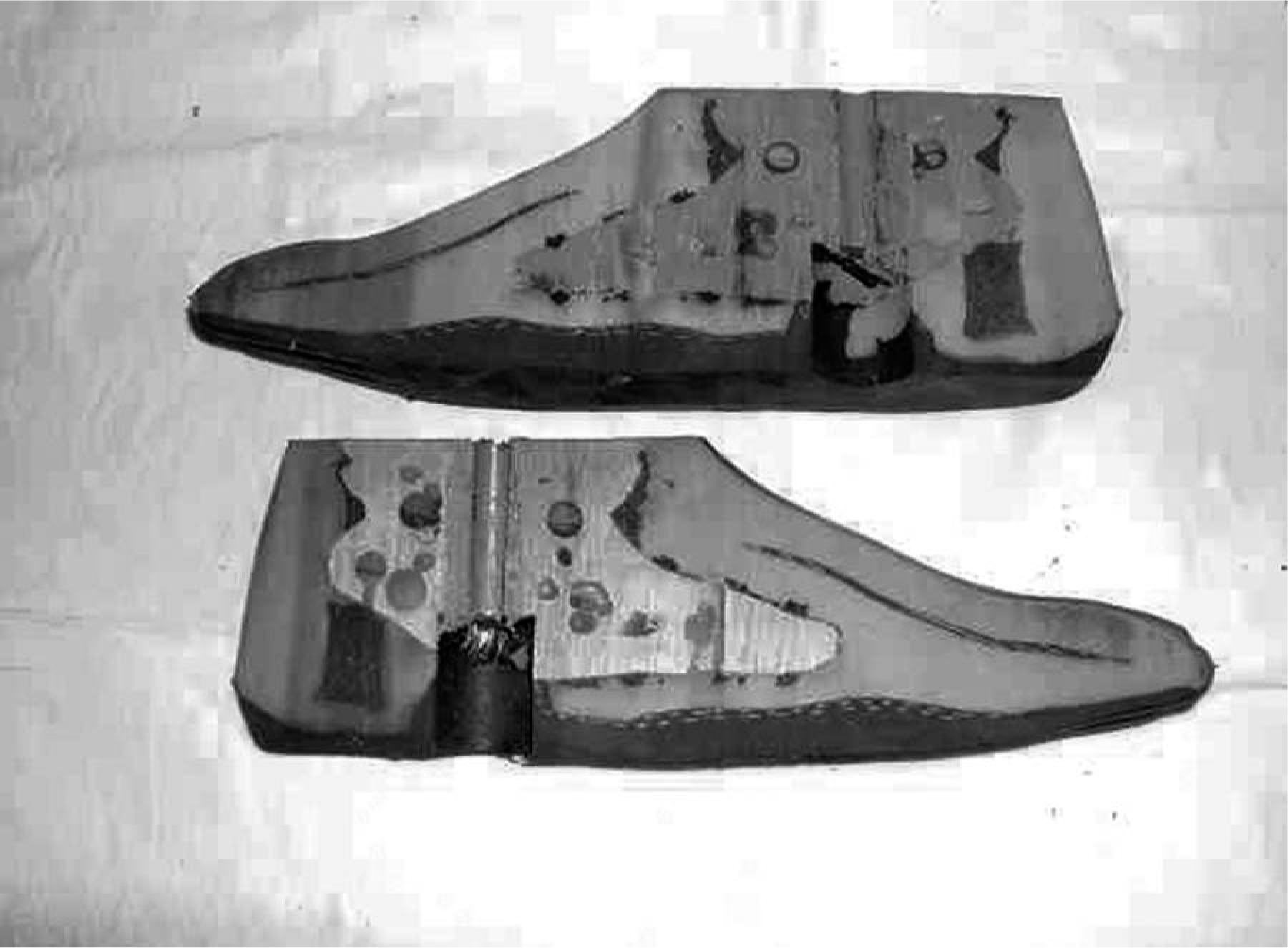
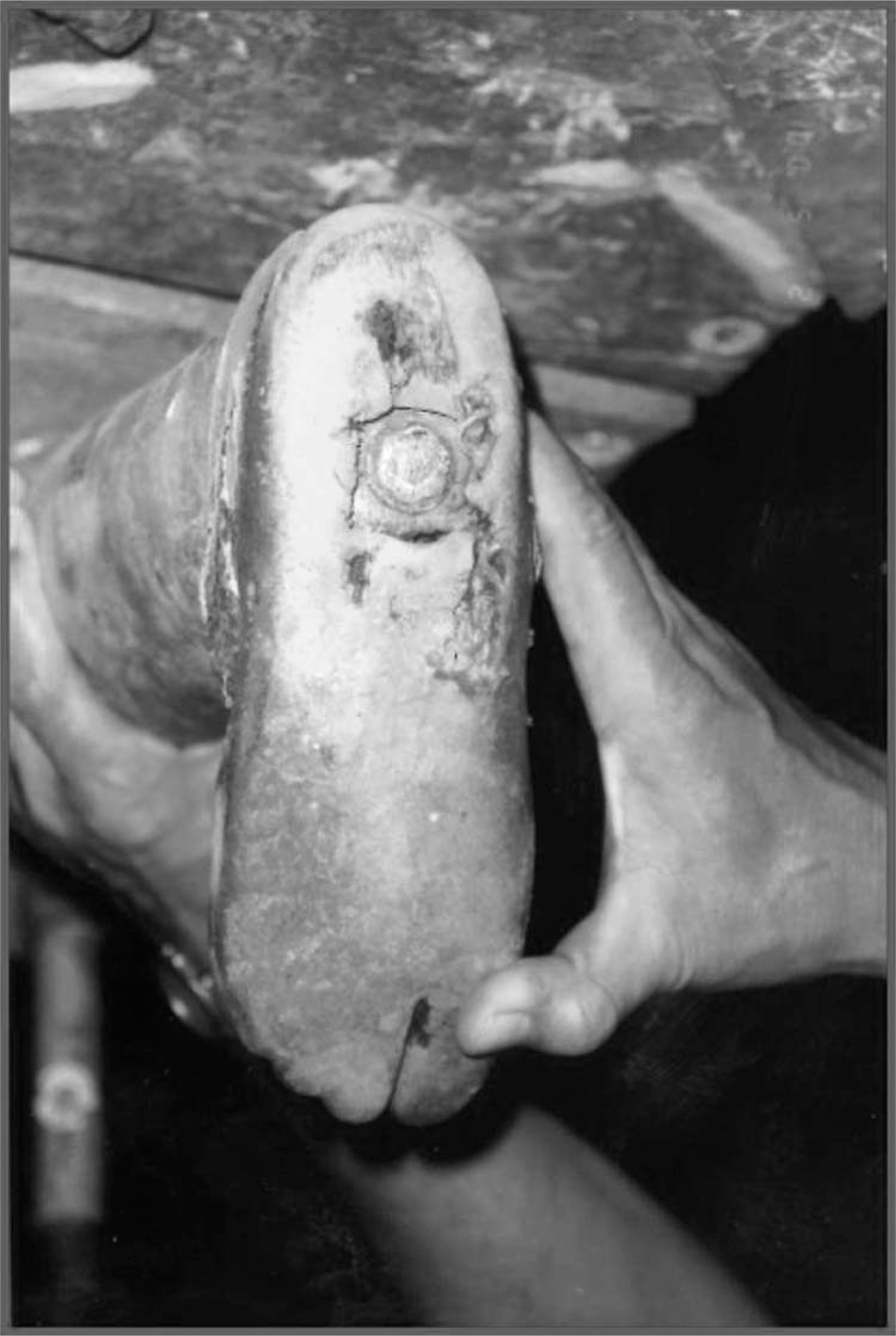
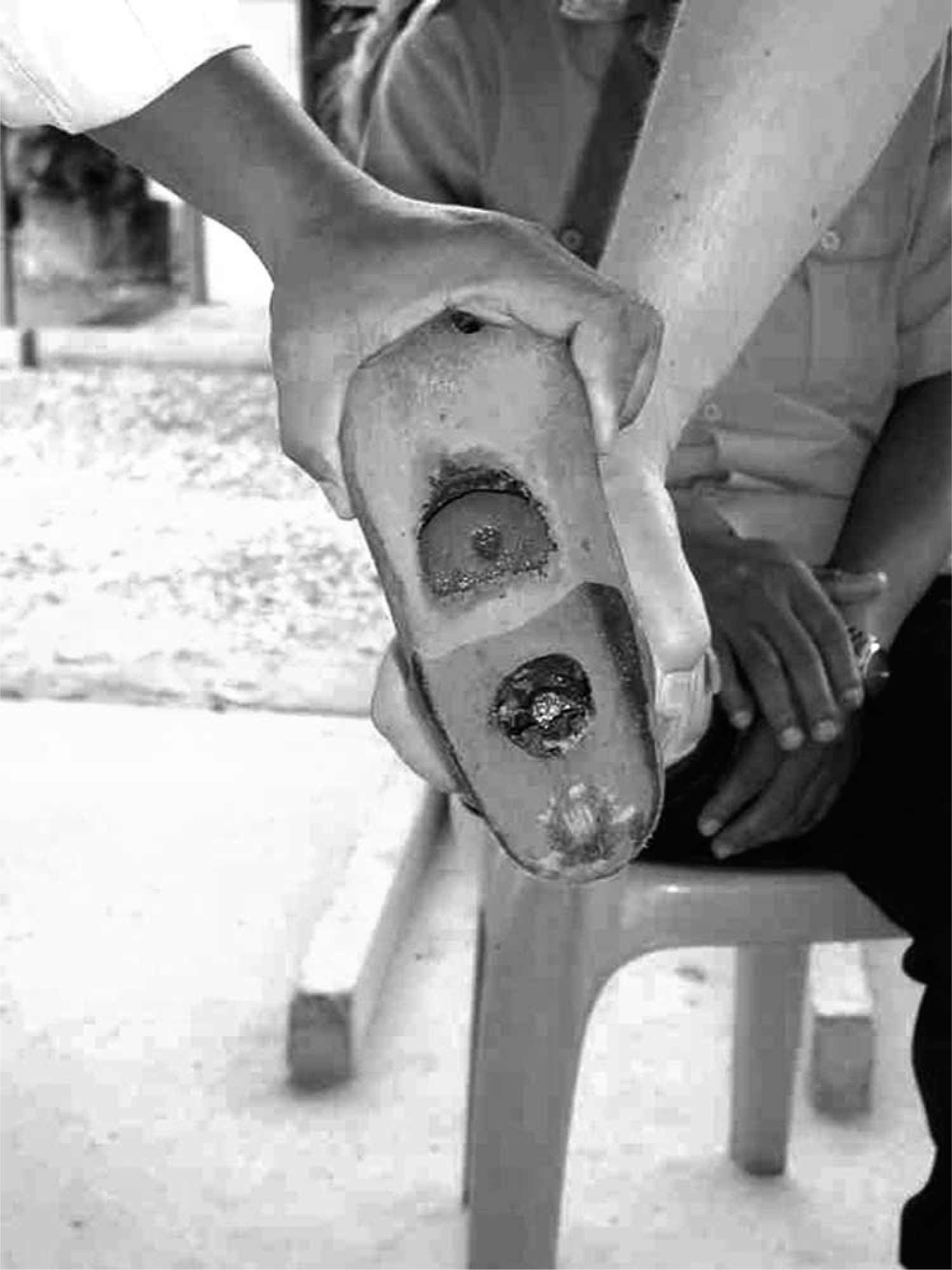
Fracture of the sole (Figure 7), worn foot sole with or without penetration of the keel (Figures 8 and 9), or wear of the keel (Figure 10) were the most frequent failures, which occurred in 36% (57/158) of feet provided and leading to exchange of the foot in 93% (55/59) of cases.

VI-Cavity Foot. Fracture of sole.
PP-Rubber Foot. Badly worn sole.
VI-Cavity Foot. Penetration of keel.

EB-1 Foot. Wear of wooden keel with separation.
After 12 months, one each of the VI-Solid and the VI-Cavity feet had been replaced, but none of the EB-1 feet (Table VI). The HI-foot needed replacement in 20% (6/30), which is not significantly different from the 7% (2/29) encountered with the PP-Rubber foot (p = 0.14). Only four (4) HI-Cambodia feet were seen for more than 12 months.
Failure of prosthetic foot.
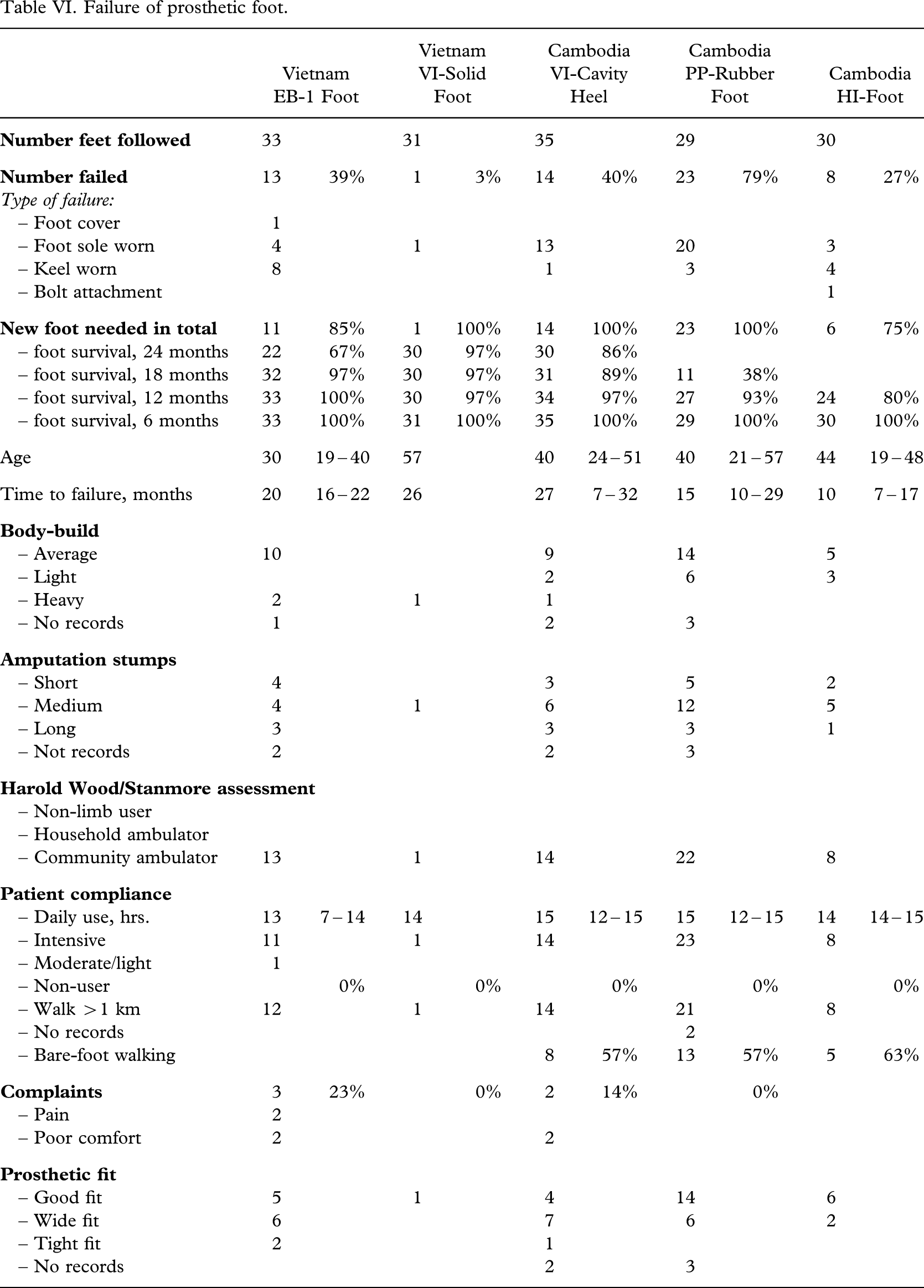
At 18 months, one VI-Solid foot, one EB-1 foot and 11% (4/35) of VI-Cavity feet had failed. This difference is not significant (p = 0.13), but only 20% (7/35) of VI-Cavity feet had been seen before 26 months. Only half of the PP-Rubber feet were followed for more than 15 months, but the failure rate of 62% (18/29), was significantly poorer than the VI-Solid foot (p < 0.0000001), the VI-Cavity foot (p < 0.0002), and the EB-1 foot (p < 0.03).
If the end results of these two foot models from VVAF are compared, the VI-Solid foot did perform better (p < 0.0002). The results with the EB-1 foot was poorer (p < 0.02) with a failure rate of 33% (11/33), all followed 20 – 21 months.
The overall time of follow-up had significant influence in all comparisons (p < 0.01).
The influence of different factors on the overall failure rates of the prosthetic feet was analysed. The amputees with EB-1 feet were younger than the other groups (p < 0.03). The median time of daily wear was a significant factor (p < 0.03), and so also was the intensity of use (p < 0.03) and body weight (p < 0.01). Bare foot walking was recorded in 41 Cambodian amputees, and in 63% (26/41) their foot failed (p < 0.0001).
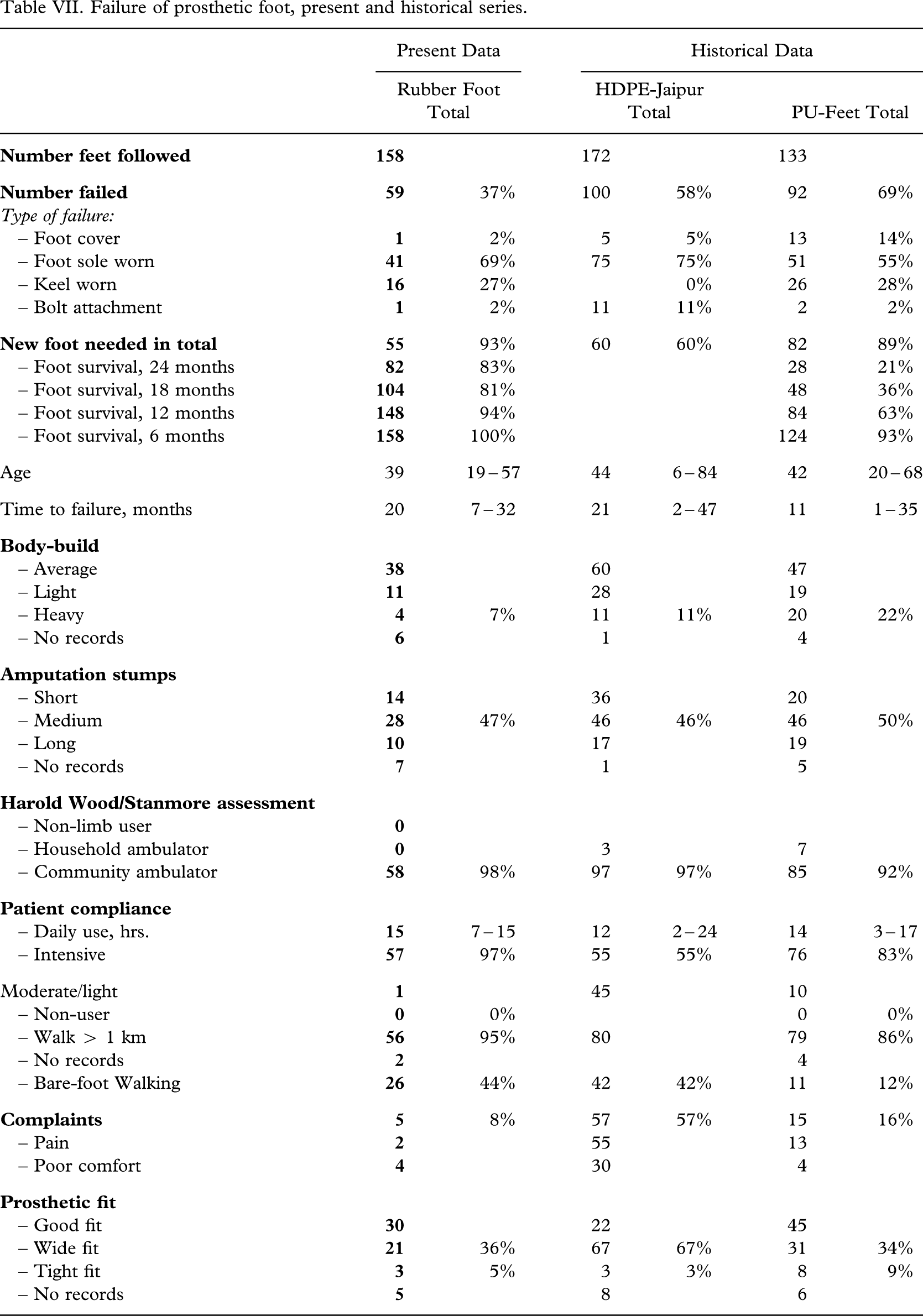
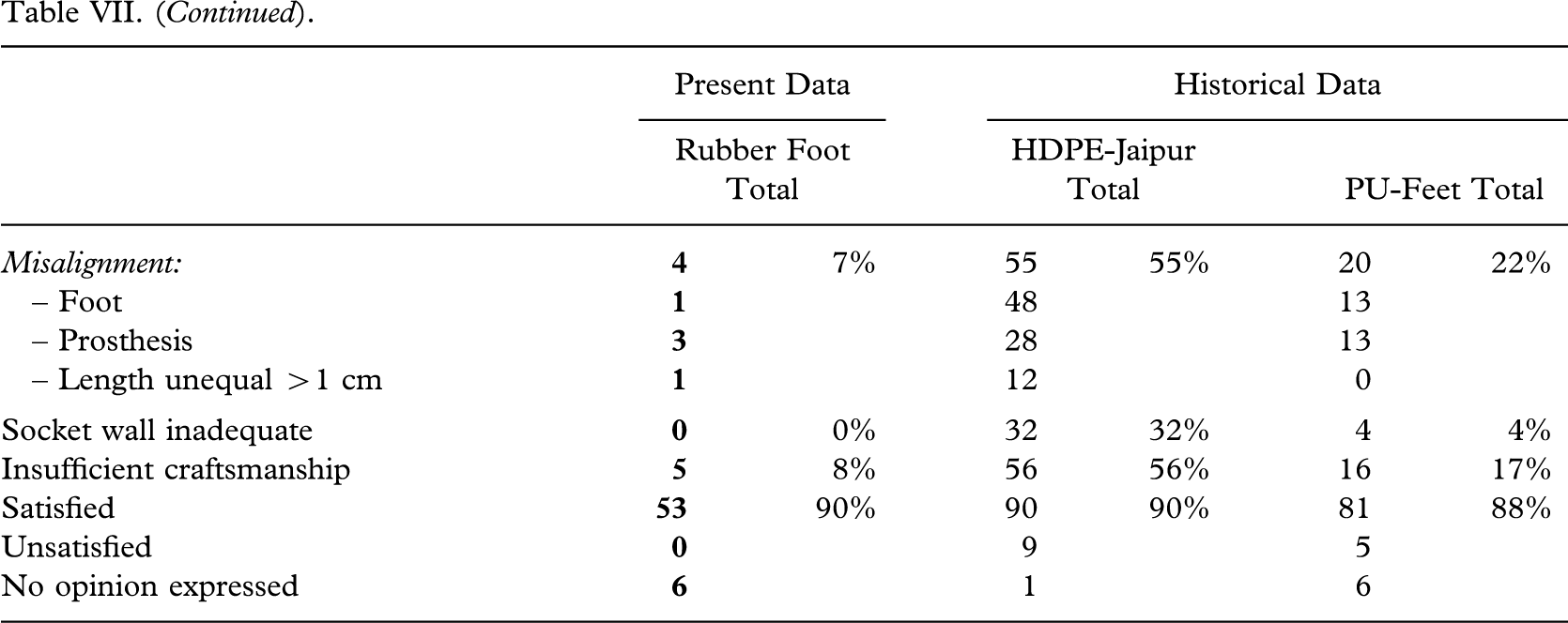
The results were compared with a clinical field testing series of polyurethane feet (Jensen et al. 2006) and it was found that at 12 months all the tested rubber feet performed better (p < 0.01) than the CR-SACH foot from CR Instruments SA, Switzerland and the Fujian-foot from Endolite-Asia, Hanoi, Vietnam (Table VII). Further it was observed that the VI-Solid and VI-Cavity feet performed better than the Kingsley Strider-08 foot from the Kingsley Manufacturing Company, Costa Mesa, California, USA (p < 0.02).
Failure of prosthetic foot, present and historical series.
Discussion
Little has been published about the results with vulcanized prosthetic rubber feet in tropical areas, being manufactured by local NGO prosthetic workshops. Jensen and Heim (1999) did find in a small clinical testing series of 18 months follow-up that 10 VI-Solid rubber feet all survived, but 4/10 HI-feet failed (bolt 1, keel 1, sole 2). The feet were subjected to intensive use, mostly in a dry rural area.
It was already at that time pointed out that sustainability of local manufacturers should be secured because of financial constraints limiting the import of finished goods like feet (Kijkusol 1986). Cummings (1996) scrutinized three decades technical publications for the 1995 ISPO consensus conference on appropriate prosthetic technology (ISPO 1996) and found that outcome studies were few and that there appeared to be a significant need for durable prosthetic feet that can be produced in-country.
The vulcanized rubber feet tested in these series represent attempts to meet these goals. The HI-foot has for long been the standard foot among the NGOs in Cambodia together with the PP modular system from ICRC (ISPO 1996; Simon 1996). The 12-month results with a failure rate of 20% were acceptable, but few feet were followed for more than a year. The failures were located at sole and keel. At one year also the PP-Rubber foot performed well, but for logistic reasons only half of the subjects were followed for more than 15 months, and the failure rate increased to 62% at 18 months. The failures were mostly located at the sole (Figures 7, 8, and 9). The failure of the sole was usually located at the tip of the keel where the material is thin (Figure 11) and push-off forces concentrated during walking.

PP-Rubber Foot. Keel penetration at push-off area.
The best performing was the VI-Solid foot, but 39% found the foot heavy resulting in non-use in 9% and dissatisfaction in 9%. The only failure observed was a rocker-foot (Figure 12), which was exchanged at 26 months.

VI-Solid Foot. Rocker-bottom shape.
In an attempt to make the foot lighter and more comfortable, a cavity was added to the heel for a damping effect. All could walk more than 1 km and all were satisfied; 37% walking bare-footed. This had no detrimental effect on the short time survival, but only a few subjects were seen before 26 months. As follow-up and repair service is not a part of the normal service provision system, amputees having access to more than the device under testing, will rarely attend when the device fails. This means, that the 37% failure rate could have occurred any unknown time before the subject was called in for control. The delay in follow-up was a result of demilitarization, as the majority of the subjects were veterans, who were sent home directly from the rehabilitation hospital.
The final vulcanized rubber foot tested was the EB-1 foot, which is based on a sandwich construction of rubber and textile layers and a wooden keel. That foot was considered heavy by 45% of the amputees. The main problem was failure of the wooden keel due to rot (Figure 13), which led to an unacceptably high failure rate.
EB-1 Foot. Rot of wooden keel.
In conclusion, it was found that the best results were achieved with the two feet from VVAF, Cambodia in accordance with previous experiences (Jensen and Heim 1999). These results did not only exceed any of the other rubber feet tested, but also the polyurethane feet tested in another series (Jensen et al. 2006), including the commercial Kingsley Strider-08 foot. The authors consider that Cummings (1996) request for a low cost, durable and locally manufactured foot has been fulfilled.
Footnotes
Acknowledgements
The following feet were supplied at no cost by the manufacturers, EB-1 (Prosthetics Outreach Foundation, Hanoi, Vietnam); VI-Solid and VI-Cavity (Vietnam Veterans of America Foundation, Kien Khleang, Cambodia); and PP-Rubber (International Committee of the Red Cross, Phnom Penh, Cambodia). The study was supported by the Leahy War Victims Fund, United States Agency for International Development (grant no. HRN-G-00-00-00015-00). The opinions expressed in this paper are those of the authors and ISPO, and do not necessarily reflect the views of USAID.