
Abstract
In this pilot cross-sectional study, the effectiveness of rigid spinal orthoses in the correction of spinal curvature of 14 patients with moderate adolescent idiopathic scoliosis (AIS) at different recumbent positions (supine, prone, right and left decubitus) was investigated. Using magnetic resonance (MR) imaging and multi-planar reconstruction technique, evaluation of the scoliotic spine in the coronal, sagittal and axial planes and the effect of spinal orthosis on AIS at different recumbent positions was studied. There was significant reduction of coronal Cobb's angle (p < 0.05) with bracing at all four recumbent positions and the maximal reduction was found in the prone position (18% reduction). The sagittal Cobb's angle was only significantly reduced at the supine position while the axial rotation did not change significantly in all positions.
Introduction
Orthoses have been demonstrated to be effective for a significant proportion of patients with mild to moderate adolescent idiopathic scoliosis (AIS), provided that treatment is started early enough and the orthosis worn with good compliance (Wong and Evans 1998; Wong et al. 2000; Wright 1997; Lonstein and Winter 1994; Willers et al. 1993; Rudicel and Renshaw 1983; Blount and Moe 1980; Edmonson and Morris 1977; Keiser Shufflebarger 1976).
The most commonly recommended treatment protocol is for the AIS patients to wear the orthoses for up to 23 h per day including bedtime. In assessing the compliance, history taking and physical examination to look for signs of wear are often used. Other more sophisticated and objective methods have been tested including the application of thermal sensors to reflect the time spent in the orthosis (Lavelle et al. 1996; 1997) and force sensor by Lou et al. (2002a; 2002b). Besides assessment of the compliance, the effectiveness of bracing on curve correction can be assessed by standing X-ray films. The effect of nocturnal bracing and different recumbent positions on curve correction was, however, only poorly studied with simple x-ray techniques. The introduction of MR imaging makes it possible to conduct such studies non-invasively.
Material and methods
Subjects
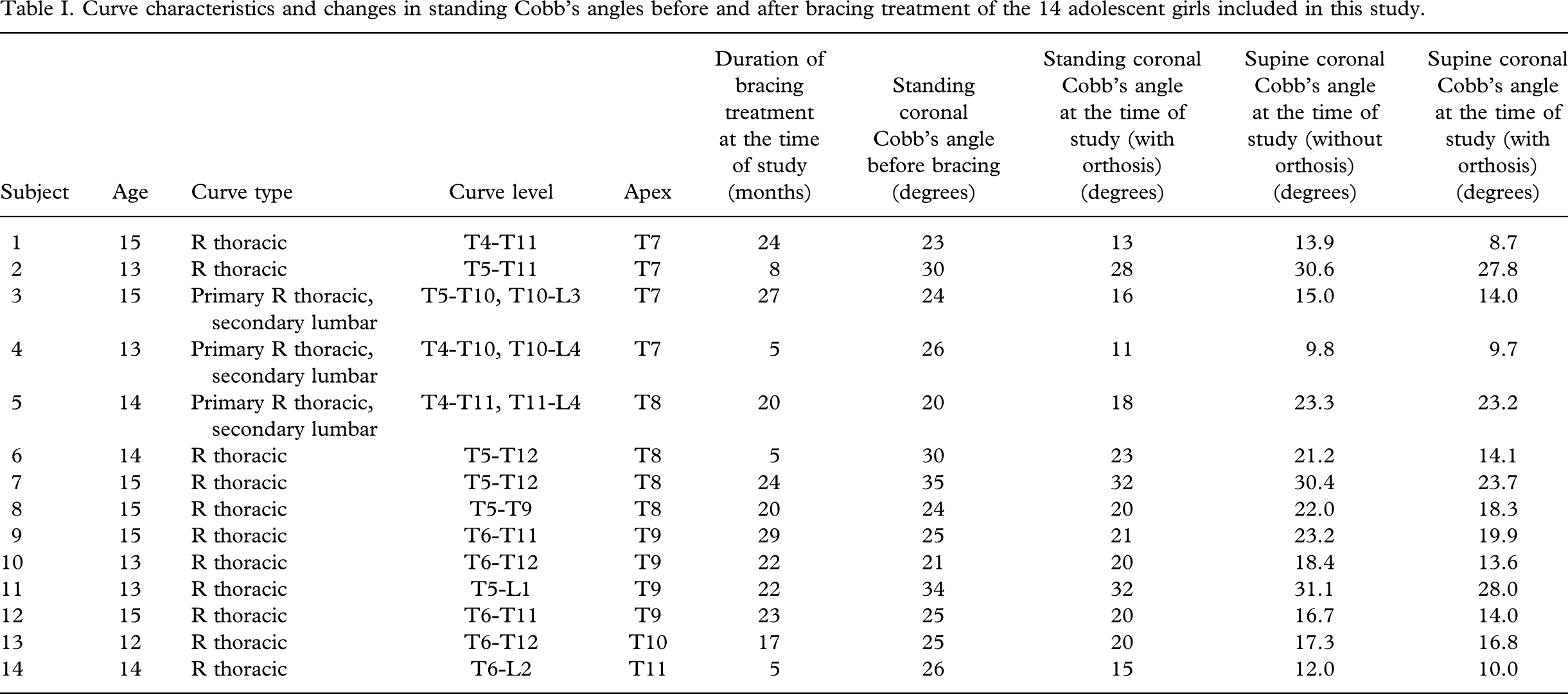
Fourteen adolescent girls with idiopathic scoliosis and orthotic treatment (underarm thoraco-lumbar-sacral orthosis, TLSO) were recruited. Eleven patients had a single right thoracic curve and three patients had a primary right thoracic curve and a secondary lumbar curve. Their age ranged from 12 – 15 years (mean 14 ± SD 1.0 years). The duration of bracing treatment ranged from 5 – 29 months (mean 17.9 ± SD 8.5 months). The conventional standing AP Cobb's angles ranged from 20 – 35° (mean 26.3 ± SD 4.4°) at initial presentation before orthotic treatment, which changed to 11 – 32° (mean 20.6 ± SD 6.4°) at the time of the study with rigid spinal orthosis in situ. Table I summarizes the curve characteristics and details of the bracing treatment of the 14 patients. Ethical approval for the study was obtained from the hospital research ethics committee. Informed written consent was obtained from all patients and/or their parents.
Curve characteristics and changes in standing Cobb's angles before and after bracing treatment of the 14 adolescent girls included in this study.
MR imaging and measurement
Immediately before the MR scanning, all subjects were assessed by an experienced prosthetist-orthotist specialized in AIS orthotics. The tension of the straps was optimized and a mark was made on the strap to ensure correct fitting of the orthosis during the MR scanning. The orthoses were specially constructed without ferromagnetic parts. Metallic rivets on the orthoses were replaced by plastic ones so that the subjects could be safely assessed with MR imaging in their orthoses.
Each subject was examined in the MR scanner at four different positions: supine, prone, right and left decubitus, first with the spinal orthosis in situ, followed by without wearing the orthosis. Soft cushions and pads were used to support the subjects during scanning to ensure the pelvis and shoulders were in parallel with the scanner table while the subjects were at either supine or prone positions. The same manoeuvre was employed to keep the body plane of the subjects perpendicular to the scanner table while they were in either right or left decubitus positions. The positioning of the subjects was carried out by the same experienced MR radiographer throughout the study (Figure 1).

Positioning of the subject within the MR scanner. (A) Subject with spinal orthosis in situ. Soft cushions and pads are placed underneath the subject to ensure the pelvis and shoulders are parallel with the scanner table while the subject is in the supine position. (B) Subject is now in a right decubitus position. Soft cushions and pads are put underneath and at the back of the subject to keep her body plane perpendicular to the scanner table.
The MRI examination of the spine was performed in all subjects using a 1.5T MR scanner (Sonata, Siemens, Erlanger, Germany) and a spine array coil. Sagittal scans of the whole spine from foramen magnum to sacrum were performed using two-dimensional (2D) Turbo spin-echo T2-weighted sequence (Repetition time, TR = 6500 ms; Echo time, TE = 118 ms; 3 mm thickness with no gap, 256×256 matrix, field of view 40 cm). A three-dimensional Tubo spin-echo T2-weighted sequence (Repetition time, TR = 9960 ms; Echo time, TE = 93 ms; 2 mm thickness with no gap, image matrix of 256×256, field of view 18 cm; number of excitations = 3, bandwidth 305 Hz/pixel) was performed covering the apical five vertebrae (which included the apical vertebra, the two vertebrae above and the two vertebrae below).
Using the multi-planar reconstruction facility on a workstation (EasyVision, Philips Medical Systems, Best, the Netherlands), the MRI images were reformatted into the best coronal and sagittal planes for the scoliotic curve. Sections passing through the endplates of the apical vertebra were then recognized in the sagittal and coronal planes, allowing the best axial reconstruction to be obtained at the apical vertebra in order to visualize the laminae of the vertebra clearly and symmetrically. The AP Cobb's angles were measured using Cobb's method described in radiographic assessment (Cobb 1948) (Figure 2).

Reconstructed image in the coronal plane indicating the measurement of Cobb's angle.
The sagittal Cobb's angles (thoracic kyphosis) were calculated between T1 and T12 (Figure 3). The apical vertebral rotation was measured by identifying three datum points as follows: one at the junction of the inner surfaces of the two laminae, and one each on the inner surfaces of the laminae as close as possible to the pedicle. These datum points have been established in CT and MR studies as reliable landmarks with least inter-observer and intra-observer variation (Ho et al. 1992; Birchall et al. 1997).

Reconstructed image in the sagittal plane indicating the measurement of the sagittal Cobb's angle.
The angle subtended by these points was measured and the degree of axial rotation was calculated by drawing a line bisecting this angle and comparing it with a vertical line drawn perpendicular to the scanner table (Figure 4). The measurement of the angle was taken as positive if the vertebral rotation was clockwise from the perpendicular line and vice versa.
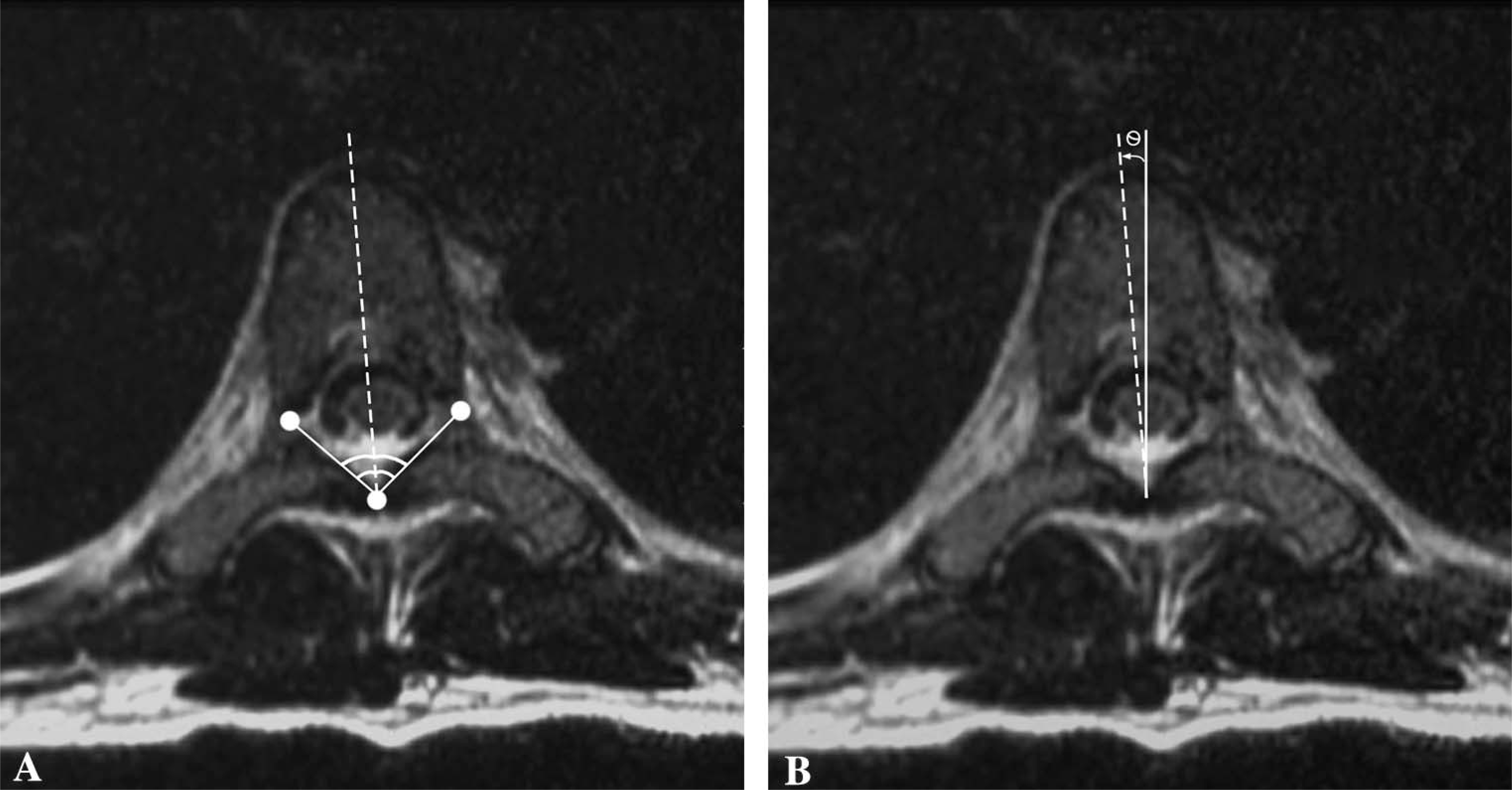
(A) Reconstructed image in an axial plane parallel to the vertebral endplate with the best visualization of the laminae. The angle subtended by datum points on the inner aspects and the junction of the laminas is shown. (B) The same reconstructed axial image indicating measurement of the angle of axial rotation as defined by the angle subtended by a line bisecting the angle in Figure A and comparing it with a vertical line drawn perpendicular to the scanner table.
The change in spinal curvature in different planes (coronal, sagittal and axial) was assessed in the four different positions in each subject with and without the orthosis. Each measurement was taken in two separate occasions by two independent observers. The mean of all readings was used as the measurement of spinal curvature. The inter-observer and intra-observer variations were evaluated.
The data were analysed using the Statistical Package for Social Sciences (SPSS) (Version 12). All the MRI measurements were expressed as mean with standard deviation. Statistical analysis was performed using two-sided Wilcoxon-signed rank test. Statistical significance was considered with p < 0.05.
Results
The mean, standard deviation and range of coronal Cobb's angles, sagittal curvature, apical vertebral rotation, with and without bracing, at different recumbent positions are summarized in Tables II, III and IV respectively.
Mean AP Cobb's angles with and without orthosis at the four different recumbent positions.
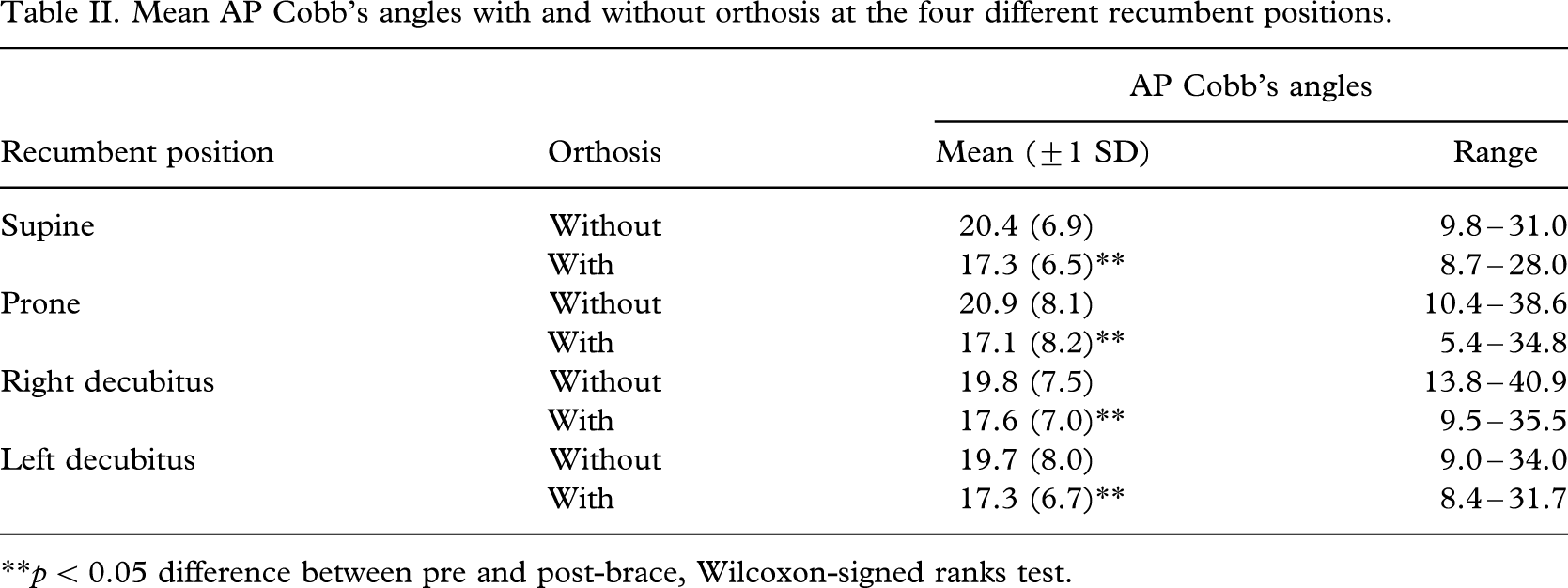
∗∗p < 0.05 difference between pre and post-brace, Wilcoxon-signed ranks test.
Mean lateral Cobb's angles (thoracic kyphosis) with and without orthosis at the four different recumbent positions.
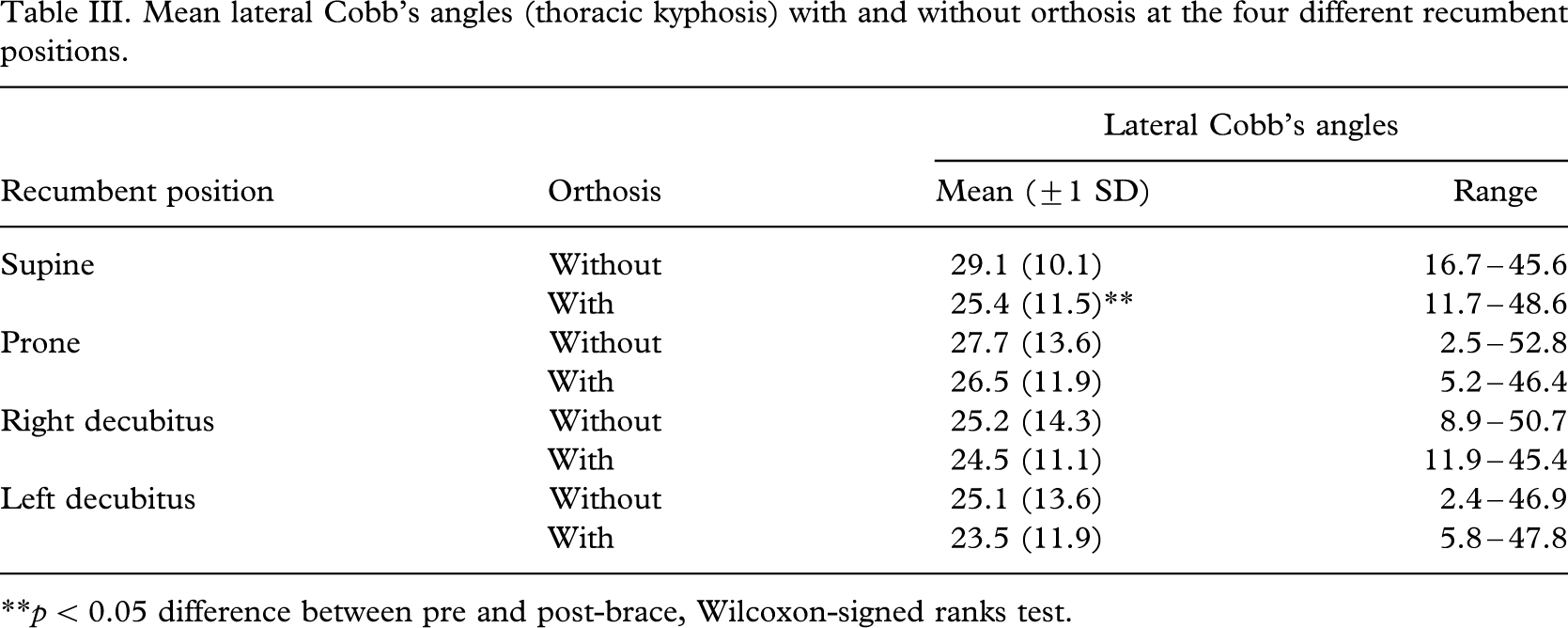
∗∗p < 0.05 difference between pre and post-brace, Wilcoxon-signed ranks test.
Mean apical vertebral rotation with and without orthosis at the four different positions.
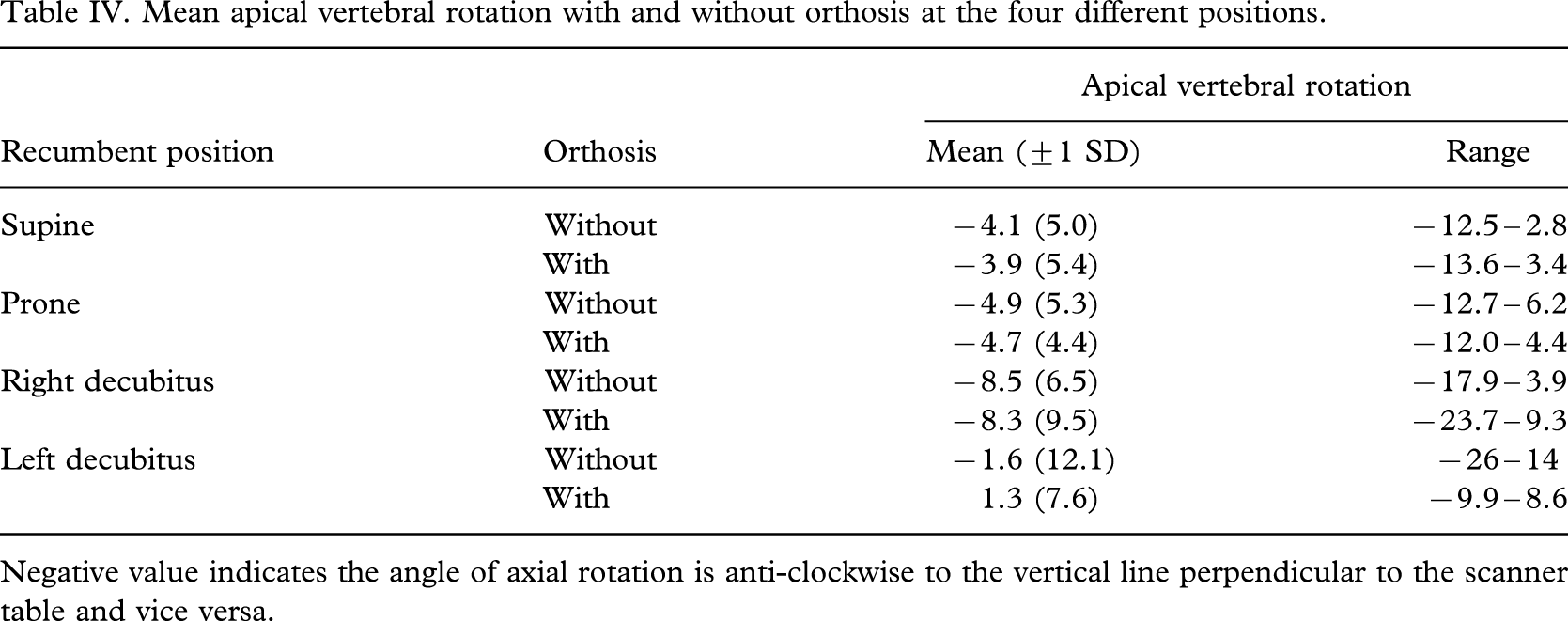
Negative value indicates the angle of axial rotation is anti-clockwise to the vertical line perpendicular to the scanner table and vice versa.
The intra-class correlation coefficient of observer 1 was 0.96 and that of observer 2 was 0.99 while the inter-class correlation coefficient between the two observers was 0.91.
There was significant reduction in the coronal Cobb's angle (p < 0.05) after bracing in all recumbent positions. The largest reduction in mean Cobb's angle was observed in the prone position (18% reduction), followed by supine (15%), left decubitus (12%) and right decubitus position (11%) (Table II).
Sagittal Cobb's angle (thoracic kyphosis) was only significantly reduced (p < 0.05, with a 13% reduction) in the supine position after bracing. In the remaining positions, though the sagittal Cobb's angles were slightly reduced but they had not reached significant levels (Table III).
The changes in apical vertebral rotation before and after bracing were not significant in all positions. The pattern of changes was also inconsistent at different recumbent positions (Table IV).
Discussion
Spinal orthoses have been demonstrated to be effective in preventing curve progression. Nachemson and Peterson (1995) postulated that orthotic treatment exerts its effect by modifying biomechanically the morphology of the scoliotic spine and control the progression of the spinal curvature through applying pressures to the trunk over a prolonged period. The most commonly recommended treatment protocol is for the AIS patients to wear the orthoses for up to 23 h/day including bedtime. However, there is a lack of evidence to estimate the bracing effect in different lying postures.
With the multi-planar reconstruction technique of MR imaging, the degrees of spinal curvature can be accurately measured in three planes before, during and after bracing. By comparing the degree of curve correction after bracing in different recumbent positions, this study could provide better and more objective understanding of the mechanical action and effect of orthotic treatment in AIS.
Though the conventional assessment of vertebral deformity in the sagittal and coronal planes can be determined by plain radiographs, the measurement of vertebral rotation in the axial plane is, however, more complex. Several techniques have been described using plain radiographs to estimate the axial vertebral rotation (Nash and Moe 1969; Perdriolle and Vidal 1985; Gunzberg et al. 1991) but they are generally limited by difficulty in landmark definition with resulting wide variations of measurements and inherent inaccuracies. Computed tomography (CT) has been used in the assessment of axial rotation (Kojima and Kurokawa 1992), but the associated high radiation dose precludes its regular use in scientific research studies of adolescent patients, in particular, in the predominantly female population. In contrast, MR does not involve any ionizing radiation, which makes it an ideal method of repeated assessment in this group of patients. Previous studies also showed high reproducibility and reliability of MR in measurement of spinal curvatures (Birchall et al., 1997; Schmitz et al. 2001a).
From the literature, only limited MR studies have been performed to evaluate the orthotic effect on AIS patients (Schmitz et al. 2001b). This study is the first one to assess in details how bracing can correct the spinal curvature of AIS patients in the three anatomical planes in different recumbent positions.
The results of this pilot study provided useful clinical evidence that rigid spinal orthosis can provide significant correction of coronal Cobb's angle in all recumbent positions with maximum effect at the prone position. From this finding, it can be estimated that the posteriorly directed forces on the thoracic and abdominal regions being increased in the prone position so as to enhance the control of the lateral curvature via the coupling effect. However, the corrective effect of the spinal orthosis on the associated sagittal plane and axial rotation was not shown as effective as that on the coronal plane. A further biomechanical evaluation of the spinal orthosis is suggested.
There are limitations in this study. First of all, the duration of the orthotic treatment in this study group was not standardized. The MR examination was carried out after a mean duration of orthotic treatment of 18 months; therefore the orthotic effect of the primary correction on spinal curvature may be different from the findings obtained immediately after bracing. Wong et al. (2000) found that the maximum reduction of the coronal, sagittal and axial Cobb's angle occurred in the first 12 months after bracing. The timing of examination in the present study's patients might not reflect the maximum corrective effect of bracing. However, significant decreases were still observed in coronal Cobb's angles from this study. Ideally, a prospective study of orthotic treatment to scoliotic patients using MR imaging at regular intervals might provide more insight on the efficacy of the orthosis at different time frames and comparison of the performance of different orthoses would be useful. The results might help to further improve the design of spinal orthosis and determine the optimal duration of orthotic treatment in the future.
In this study, no attempt was made to evaluate the difference of corrective forces of spinal orthosis in upright and recumbent positions since our centre does not have an open-configured magnet scanner. MR study is expensive and may not be applicable for routine clinical assessment of every patient with AIS having orthotic treatment. However, in view of the three dimensional imaging and multi-planar reconstruction capacities, the accuracy and great reproducibility of measurements in the evaluation of complex deformities involved in AIS, as well as lack of ionizing radiation, MR imaging is an ideal method for repeated evaluation of orthotic treatment of adolescent spine.
Conclusion
Multi-planar reconstruction of MR imaging enables the accurate assessment of orthosis performance in different recumbent positions in a non-invasive fashion. The spinal orthosis continues its corrective effects on the scoliosis curve in different recumbent positions with the maximal corrections found at the prone position.