
Abstract
Study design
Retrospective cohort study.
Objectives
Wound complications and suboptimal pelvic correction remain significant challenges in posterior spinal fusion to the pelvis for neuromuscular scoliosis. We describe and evaluate the Rocket incision, a novel modification of the posterior midline approach designed to redistribute closure tension and enhance access for soft tissue release.
Methods
This retrospective cohort study included 16 paediatric patients with neuromuscular scoliosis who underwent long posterior spinal fusion to the pelvis using the Rocket incision between 2020 and 2022. Radiographic parameters included Cobb angle and pelvic obliquity, measured pre- and postoperatively. Wound complications and readmissions were documented. Surgical exposure, instrumentation, and closure were standardised. Statistical analysis was performed using paired t-tests (significance set at P < .05).
Results
The mean Cobb angle improved from 81.5° (95% CI: 72.5-90.5) to 21.0° (95% CI: 15.0-27.1), representing a 74% mean correction (P < .001). Pelvic obliquity, a primary outcome, improved from 19.8° to 3.2° (mean correction: 16.6°, P < .0001), with 81.3% of patients achieving <5° tilt. There were no early wound infections, wound breakdowns, or readmissions within 90 days. One patient (6.25%) developed a late superficial infection treated non-operatively. No patients experienced radiographic decompensation or loss of correction.
Conclusion
The Rocket incision appears to be a safe and effective modification to the posterior spinal approach in neuromuscular scoliosis, with promising early results in deformity correction and wound morbidity. These preliminary findings, derived from a small retrospective cohort, should be interpreted as hypothesis-generating and require further validation in comparative or prospective studies.
Introduction
Posterior spinal fusion to the pelvis remains a cornerstone in the surgical management of neuromuscular scoliosis, particularly in non-ambulatory patients with progressive coronal and pelvic imbalance. However, despite advances in fixation and soft tissue management, distal wound complications remain a common and serious challenge. Reported infection rates range from 10% to 20% in this population, with higher incidence in cerebral palsy and syndromic patients.1-3
The conventional midline incision terminates near the sacrum and intergluteal cleft—an area with inherently poor vascularity and soft tissue coverage. In neuromuscular patients, this location is particularly problematic due to bowel incontinence and proximity to the anus, which increases the risk of wound contamination and postoperative infection. When combined with pressure from prolonged sitting, pelvic screw prominence, and muscle atrophy, these patients are particularly vulnerable to wound dehiscence, infection, and delayed healing.4-6
Existing approaches to mitigate these risks include plastic closure techniques, muscle flaps, and negative pressure dressings. However, these are typically applied in a reactive fashion, once soft tissue damage has occurred. There is limited focus in the literature on proactive modification of the incision itself to offload tension, preserve vascularity, and redirect the wound away from high-risk anatomical zones.
In this study, we describe the Rocket incision, a novel modification to the standard midline approach designed to reduce wound tension, protect the distal closure zone, and improve access for soft tissue release. We evaluate its impact on radiographic correction and wound outcomes in a cohort of paediatric patients undergoing posterior spinal fusion to the pelvis for neuromuscular scoliosis.
Materials and Methods
This was a retrospective, single-centre cohort study conducted between January 2020 and December 2022, evaluating patients with neuromuscular scoliosis who underwent long posterior spinal fusion to the pelvis using the Rocket incision technique. All surgeries were performed by a single fellowship-trained paediatric spinal deformity surgeon using a standardised surgical protocol at a national referral centre. Our study involved a retrospective analysis of fully anonymized patients that had been previously collected during routine clinical care. All identifiers were removed prior to analysis and no patient can be reidentified from the data set. According to our institution, such research does not require formal IRB/REC approval as it does not involve identifiable data, patient contact or intervention and poses no risk to participants. The study was conducted in accordance with the principles of declaration of Helinski. A formal ethics exemption letter was not issued as our institution classifies this as research exempt from REC review.
Inclusion criteria were: • Diagnosis of neuromuscular scoliosis • Indication for long posterior spinal fusion extending to the pelvis • Availability of complete radiographic data preoperatively and at final follow-up (minimum 3 months) • No prior posterior spinal surgery Patients with incomplete imaging or follow-up data were excluded.
In our institution, fusion to the pelvis is generally reserved for non-ambulatory patients and/or those with pelvic obliquity greater than 15°, where correction is essential to optimize sitting balance and prevent long-term coronal decompensation. In contrast, constructs are typically stopped at L5 in ambulatory patients with minimal or no pelvic tilt. The Rocket incision is used exclusively in cases where fusion extends to the pelvis. When the lower instrumented vertebra is L5, we prefer the standard posterior midline approach, as the additional exposure provided by the Rocket incision is not required.
Demographic data (age, sex, diagnosis), intraoperative parameters (estimated blood loss, anaesthesia time), and clinical outcomes (length of hospital stay, wound infection, readmission) were collected. Radiographic assessments included Cobb angle and pelvic obliquity, both measured preoperatively and at final follow-up on standard sitting anteroposterior spinal radiographs. Cobb angle was measured using the standard method between the most tilted vertebrae at the apex of the main curve. Pelvic obliquity was assessed using the angle between the iliac crests and a horizontal reference line. All measurements were performed independently by two fellowship-trained spinal surgeons. The primary outcome was the change in radiographic pelvic obliquity from baseline to follow-up; Cobb angle correction was assessed as a key secondary outcome.
Surgical Technique: The Rocket Incision
The patient is positioned prone on an Allen table or equivalent, with halo–femoral traction applying approximately half the body weight to each side. A rolled gel bolster is placed under the pelvis on the concavity side of the curve to assist with rotational correction and improve access to the posterior elements.
This technique was developed by the senior author, a fellowship-trained paediatric spinal deformity surgeon, based on extensive experience with complex neuromuscular cases requiring improved pelvic exposure and wound reliability.
The posterior superior iliac crests are palpated and marked. A line is drawn between the two posterior superior iliac spines (PSISs) and measured. Bilateral attempts are made to palpate the superior gluteal artery, which is typically more accessible in slender patients. These arterial landmarks define the inferior limit of the semilunar flap and help avoid compromising its vascular supply. Figure 1 A Sketch by Medical Student Charbel Maakaroun, Demonstrating the Location of the Vascular Perforators From the Lumbar Perforating Arteries and Superior Gluteal Artery and Their Relationship With the Rocket Incision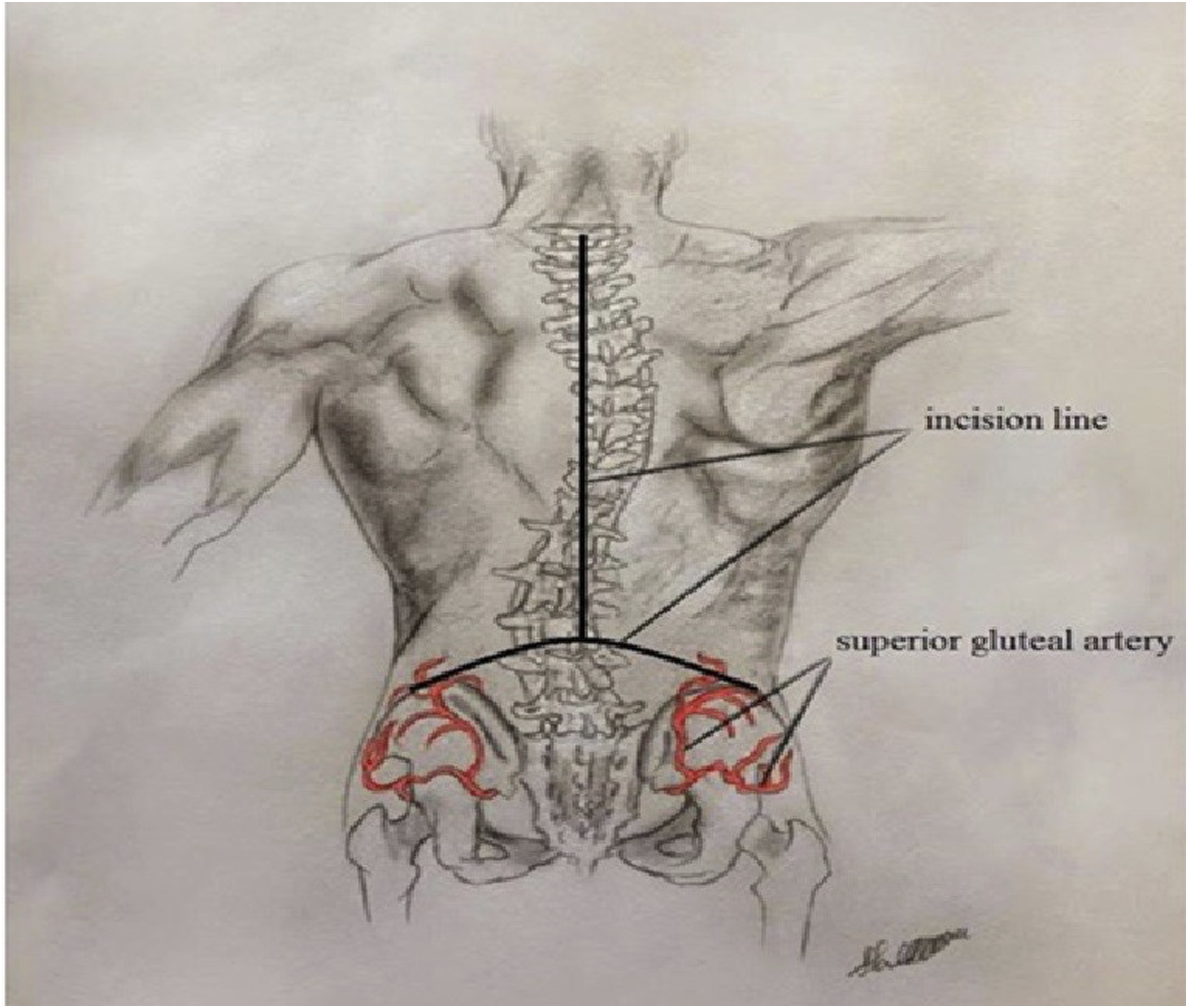
A curved semilunar line is drawn from one PSIS to the other, typically reaching the L2 or L3 level depending on the patient’s lumbar lordosis. Importantly, the length of the PSIS-to-PSIS line must exceed the vertical distance from its midpoint to the apex of the flap to preserve the vascular pedicle, including the lumbar perforators. This semilunar flap merges proximally with a standard posterior midline incision extending cranially to the planned thoracic level of instrumentation.
After incising skin and subcutaneous tissue, the lumbar fascia is opened along the semilunar flap without undermining tissue planes. The fascia is elevated off the paravertebral muscles and reflected inferiorly. In the midline, fascial attachments to the spine and interspinous ligaments are released using diathermy. Laterally, the fascia is not directly attached and can be elevated by blunt dissection, allowing the flap to advance inferiorly just short of the previously marked superior gluteal artery.
The underlying longissimus thoracis and iliocostalis lumborum muscles are then visualised and detached from the midline structures in standard fashion. Distally, these are dissected from the sacrum and iliac crest using diathermy, and reflected superolaterally to expose the sacroiliac joints and posterior iliac crest. A cuff of fascia is preserved along the iliac crest to allow reattachment of the muscle during closure.
This wide exposure also facilitates release of the iliolumbar fascia from the iliac crest on the concavity side, aiding deformity correction and pelvic rebalancing. Additionally, the elevated paravertebral muscle mass provides soft tissue coverage for pelvic instrumentation once reattached.
We acknowledge that releasing the iliolumbar fascia, particularly on the concave side, may theoretically place the superior cluneal nerves at risk. However, no patients in our cohort reported postoperative sensory disturbance in the iliac crest or buttock region.
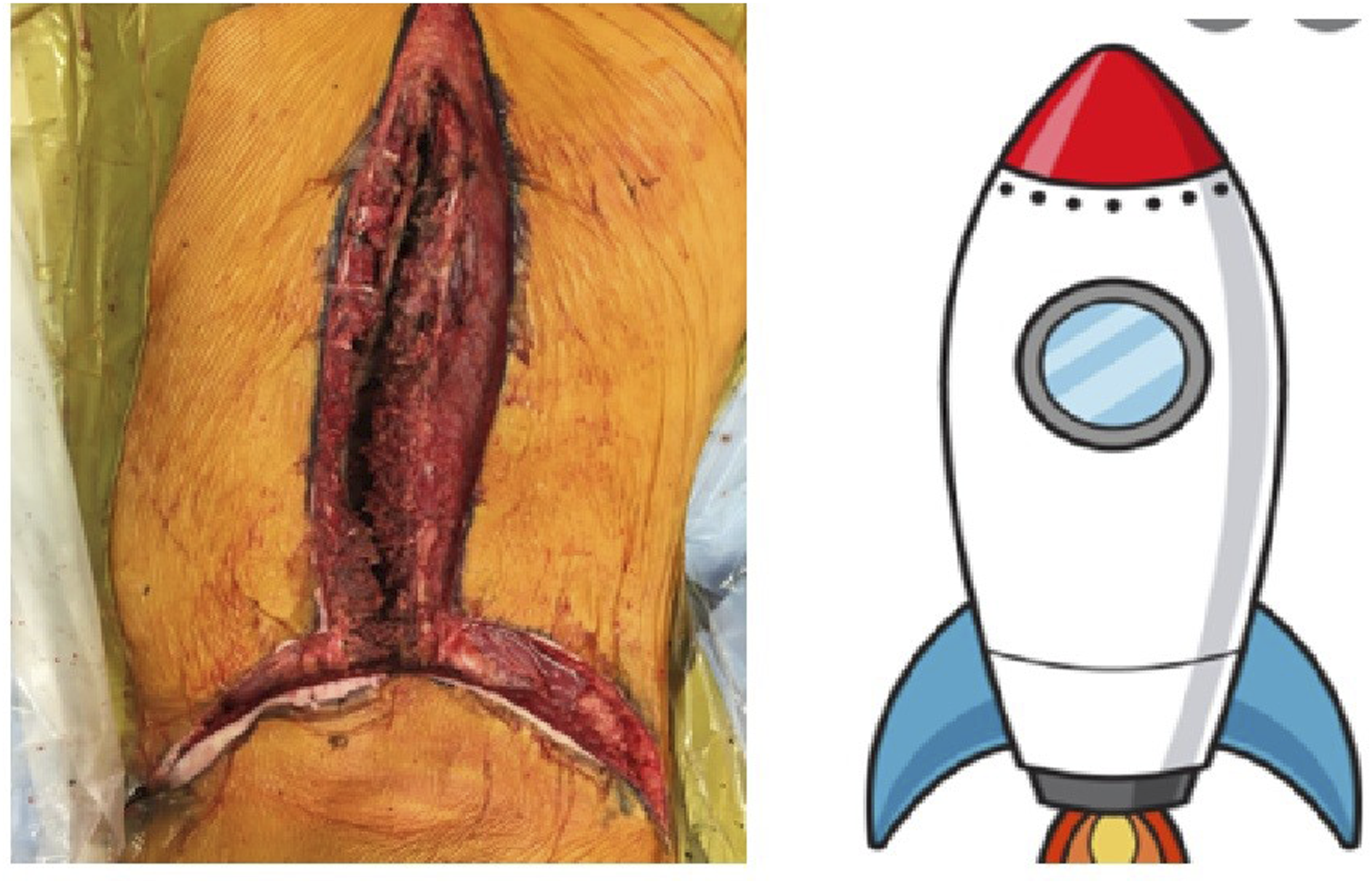
At L4–L5 and proximally, the dissection continues as per a standard posterior approach, elevating the paravertebral muscles subperiosteally. Following deformity correction and instrumentation, the paravertebral muscles are repositioned and re-sutured starting laterally on both sides using PDS sutures on sharp needles. Once midline approximation is achieved deep to the semilunar flap, one suture is tied while the other continues proximally for standard midline closure. Figures 2 and 3. Images Demonstrating Various Steps for Raising the Rocket Incision and Flap Two Corresponding Images Showing the Similarity Between Final Rocket Incision and Rocket and Hence the Name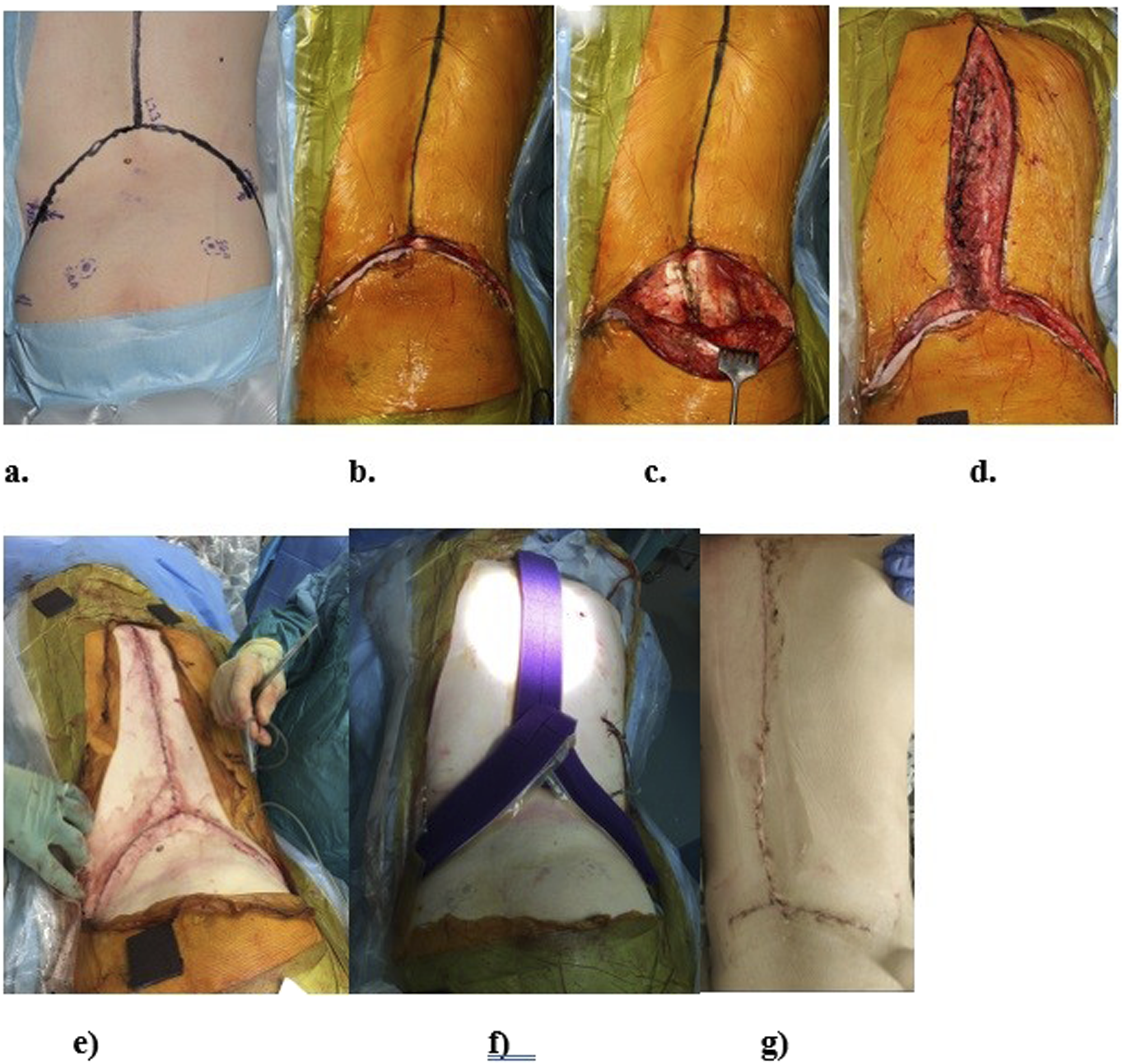
Pelvic fixation was achieved using bilateral S2 alar-iliac (S2AI) screws in most of our cases, in line with our institutional preference for low-profile constructs that minimize implant prominence and wound tension, however, we also used direct iliac screws in some cases when the S2AI was not achievable.
The deep fascia is closed with 1-0 PDS, followed by layered closure of subcutaneous tissue and skin using absorbable sutures. A suction dressing is applied and maintained for 10 days. All patients receive three perioperative doses of intravenous antibiotics.
Clinical Outcome Assessment
Wound-related complications were defined according to CDC criteria and extracted from operative notes, inpatient records, and outpatient follow-up documentation. There were no missing data points in the final cohort.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics version 29.0. Continuous variables are reported as means ± standard deviation (SD) and 95% confidence intervals (CI). A paired t-test was used to compare pre- and postoperative pelvic obliquity. Statistical significance was defined as P < 0.05.
As a retrospective study based on anonymised patient data, formal ethics committee approval was not required.
Results
A total of 16 patients underwent posterior spinal fusion to the pelvis using the Rocket incision technique. The mean age was 11.4 years (range: 5-19), with a male-to-female ratio of 6:10. Cerebral palsy was the most common underlying diagnosis (62.5%), followed by Duchenne muscular dystrophy, Rett syndrome, spinal muscular atrophy, and other syndromic conditions.
Pelvic obliquity correction, a primary outcome of this study, improved from a preoperative mean of 19.8° to 3.2° at final follow-up (mean absolute correction: 16.6°, P < 0.0001; 95% CI: 13.5-20.0). Clinically significant realignment (≤5° of obliquity) was achieved in 81.3% (13/16) of patients. Correction was maintained in all cases, with no radiographic decompensation or construct failure observed during follow-up.
Three patients in this series had previously undergone MAGEC rod insertion via the Rocket incision. All subsequently underwent successful definitive fusion through the same approach, without wound complications or technical difficulty.
Coronal deformity, measured by Cobb angle, improved from 81.5° (95% CI: 72.5-90.5) to 21.0° (95% CI: 15.0-27.1), representing a 74% mean correction in coronal alignment (P < .001). Correction was consistent across the cohort, and no loss of correction occurred at final review. Figure 4 Pre and Post-operative x Rays of 10 year old Patient Neuromuscular Scoliosis Secondary to Cerebral Palsy, GMFCS Level 5, Showing the Good Correction of the Pelvic Obliquity and Coronal Deformity Using Rocket Incision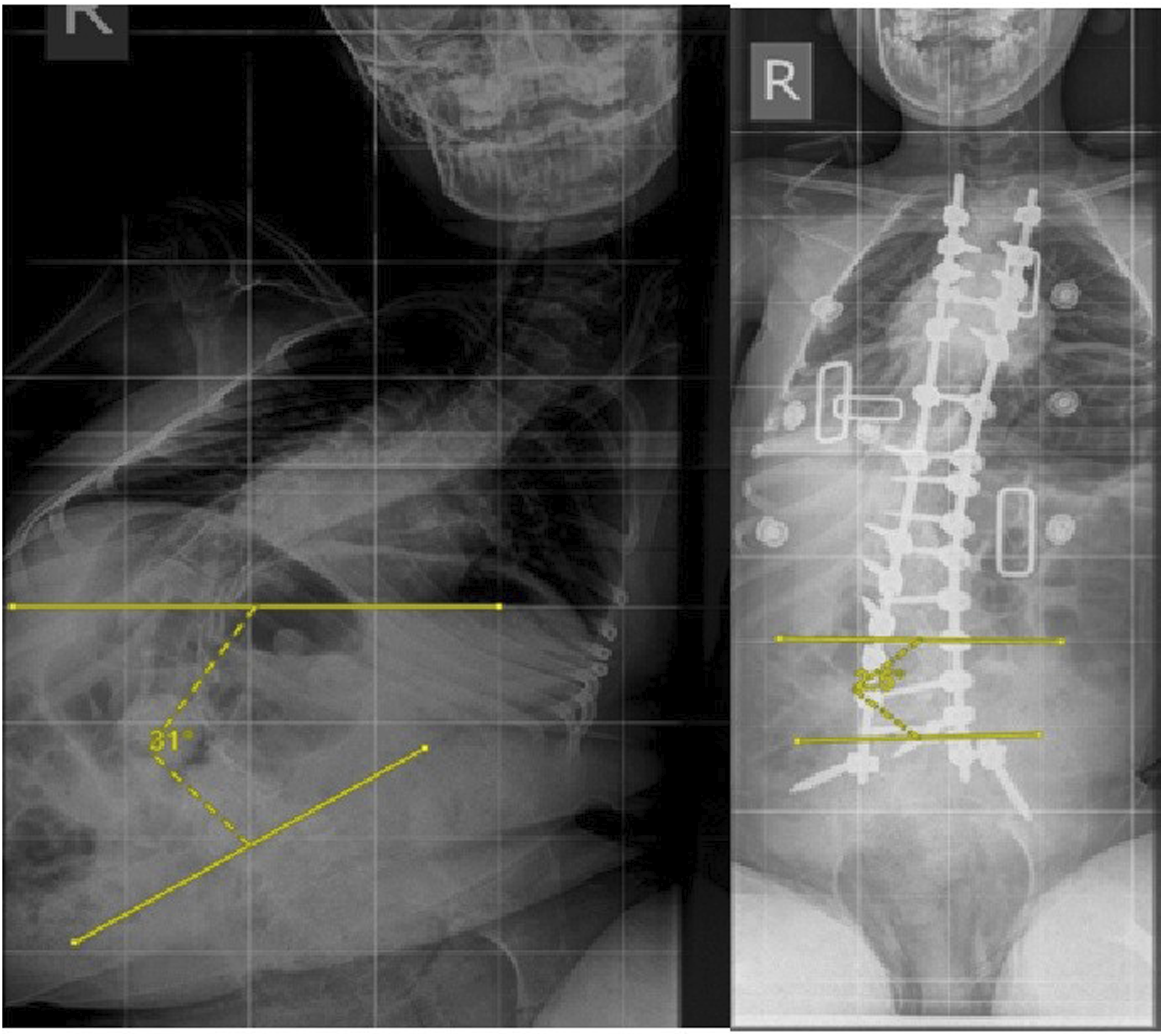
The mean estimated intraoperative blood loss was 873.1 ± 558.1 mL, and the mean anaesthesia time was 468.8 ± 123.7 minutes. All cases were performed under continuous neuromonitoring, with no intraoperative adverse events or signal changes recorded.
No early postoperative wound infections or wound-related complications were reported. No patients required return to theatre or readmission within 90 days. One patient (6.25%) developed a late superficial wound infection at 4 months, which resolved with oral antibiotics alone. Figure 5 Image Depicting the Healed Surgical Scar after Rocket Incision in a 7 year old With Early Onset Scoliosis, Used for Insertion of Managed With Magnetic Growing Rod
Mean hospital length of stay was 22.3 ± 40.5 days, skewed by one outlier (172 days) due to non-medical rehabilitation delays. When excluded, the adjusted mean stay was 11.2 ± 5.5 days, aligning with institutional averages for neuromuscular fusion. The mean follow-up duration was 8.4 months (range: 3-14 months).
Discussion
The Rocket incision offers a novel, anatomy-informed modification to the standard posterior midline approach, specifically designed to reduce distal wound complications and enhance pelvic correction in neuromuscular scoliosis. Unlike salvage strategies such as plastic closure or muscle flaps, the Rocket incision functions as a preventative solution—offloading tension, preserving vascularity, and providing wider anatomical access at the caudal wound. Importantly, by redirecting the distal portion of the incision laterally, it also positions the wound away from the perianal region, which is a common source of contamination in patients with bowel incontinence. This anatomical reorientation addresses one of the underappreciated contributors to wound morbidity in this population. This study evaluates the effectiveness of the Rocket incision in a cohort undergoing posterior spinal fusion to the pelvis.
Our findings support the technique’s dual goals: achieving durable wound closure and maintaining high-quality deformity correction. Pelvic obliquity, a primary outcome of this study, improved from 19.8° to 3.2°, with 81.3% of patients achieving correction to within 5° of a level pelvis. This compares favourably with prior series using conventional midline exposures, where final pelvic obliquity typically ranges from 6° to 10°, and correction to <5° is achieved in 50-60% of patients.5-7
We believe the Rocket incision contributes to this enhanced correction not only through improved soft tissue management but also by facilitating broader exposure of key stabilising structures. 8 The semilunar design enables direct access to the sacroiliac joints and iliolumbar fascia—particularly on the concavity side—allowing for targeted release of pelvic attachments that contribute to rigid obliquity. This extended reach is rarely possible with traditional midline incisions unless more aggressive lateral dissection is performed. As such, the Rocket incision may offer both a biomechanical and technical advantage in achieving pelvic realignment.
Coronal deformity, as measured by Cobb angle, improved from 81.5° to 21.0°, representing a 74% mean correction. This exceeds the typical range of 60-68% reported in large neuromuscular scoliosis series using standard exposures9,10 and was achieved without compromise in surgical access or construct integrity. No patients experienced loss of correction or radiographic decompensation during follow-up.
Wound outcomes were equally compelling. No early wound complications or unplanned returns to theatre occurred, and only one patient (6.25%) developed a late superficial wound infection, which resolved with oral antibiotics. These outcomes compare favourably with published early infection rates of 10-20% in this population, particularly in patients with cerebral palsy.4-7 We attribute this to the Rocket incision’s ability to redirect closure vectors away from the poorly perfused sacral apex and enable layered closure with better implant coverage, particularly over pelvic screws.
From a technical perspective, the procedure allowed for reattachment of paraspinal musculature using fascial cuffs, maintaining soft tissue bulk and implant coverage. The semilunar design also enabled broader mobilisation of paravertebral muscle, potentially reducing implant prominence and tension on skin closure.
Beyond radiographic correction and wound integrity, the Rocket incision demonstrated favourable perioperative parameters that compare well with existing neuromuscular scoliosis literature. The mean anaesthesia time in this series was 468.8 minutes, consistent with the 450-500 minutes reported by Sharma et al. 11 and Ramo et al (2014) in cohorts of cerebral palsy and spinal muscular atrophy patients undergoing fusion to the pelvis.
The mean estimated blood loss was 851.3 mL, which lies at the lower end of the 800-1500 mL range commonly seen in posterior fusion with pelvic fixation (Sharma et al 2009; Ramo et al 2014). This may reflect improved soft tissue preservation through the Rocket incision, which minimises lateral undermining and enables layered reattachment of musculature.
Postoperative recovery was similarly consistent with prior series. The mean hospital stay was 12.6 days, aligning with the 12-14 day averages reported by Ramo et al. 12 and Tsirikos et al. 9 Importantly, the absence of early wound complications likely contributed to the lack of delayed discharges, reoperations, or extended inpatient wound management.13–19
These results suggest that the Rocket incision achieves soft tissue and skeletal goals without compromising operative efficiency or early postoperative recovery.
Importantly, in three patients who initially underwent surgery using the Rocket incision for insertion of MAGEC rods in early-onset scoliosis, definitive posterior spinal fusion was performed 4-5 years later through the same incision. These revision surgeries were completed without complication and with excellent exposure, highlighting the Rocket incision’s durability and its potential role in staged or long-term deformity strategies.
Strengths of this study include its consistent technique, single-surgeon approach, prospective data collection, and clearly defined outcomes. However, it is limited by its retrospective design, modest cohort size, single-surgeon experience, and relatively short follow-up, which may underestimate the true incidence of late wound complications. Additionally, while the Rocket incision technique proved reproducible in our series, there may be a learning curve for other surgeons, particularly in preserving vascular perforators and achieving symmetrical flap mobilization. These factors may impact generalizability and should be considered when interpreting our findings. Finally, the relatively short follow-up duration may underestimate the true incidence of delayed or late-onset surgical site infections, which often manifest beyond the 90-day surveillance window.
Given its favourable safety profile, technical reproducibility, and potential for wider soft tissue and skeletal release, the Rocket incision may be considered a promising technique in high-risk cases. However, these findings remain preliminary, and further prospective studies with control groups are essential to confirm its broader utility and comparative advantages.
Conclusion
The Rocket incision appears to be a safe and anatomically sound modification to the posterior approach in neuromuscular scoliosis. It provides excellent coronal and pelvic realignment while significantly reducing wound-related morbidity. While early results are encouraging, this study’s retrospective design and limited cohort size necessitate cautious interpretation. Prospective, controlled studies are needed to validate its long-term effectiveness and broader applicability.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.