Abstract
The changes that lithium brought are most fully understood when we grasp the difficulties for management that acute mania presented. Restraint in canvas camisoles, padded cells, paraldehyde, water-baths and salts—Epsom, not Lithium—met mania in echos of Bedlam still heard in the early 1950s. It is a part of psychiatric history important to remember.
John Cade and exams in Melbourne
Before the advent of lithium and neuroleptic medications, psychiatric hospitals did all they could to manage acute mania by empirical means. General hospitals, where medical students trained, could not tolerate the disturbances commonly generated in acute or chronic mania and so these patients were legally segregated into other hospitals. In Victoria, most went to the care of John Cade at Royal Park Receiving House in Melbourne, and in South Australia, to my care at Enfield Receiving House in Adelaide.
John Cade and I came to know each other fairly well. Not infrequently we had to treat the same individuals during different episodes as border-hopping was a hallmark of our two states. We phoned each other about crises. During visits to Melbourne, I sometimes lodged with John and my son used to sleep on his verandah.
I differed from some Adelaide colleagues in my reluctance to take my qualifications at the Maudsley Hospital in London, when Aubrey Lewis was at the helm. Aubrey was a graduate of the Adelaide Medical School, where it was said that he had inadvertently offended his examiners in obstetrics by dropping the baby at delivery.
Certain training in the USA appealed to me, especially that under Adolf Meyer at Johns Hopkins Hospital; however, an Australian had to await his chance. Mine eventually came in the form of a Harkness Fellowship, enabling my wife and family to visit also.
Meanwhile, I took advantage of Melbourne's offer to examine selected Adelaide graduates for the Diploma of Psychological Medicine (DPM). This required repeated visits. Since there was no air traffic, I boarded the Overlander Express at Adelaide Railway Station at 6 p.m. It arrived at Spencer Street at 8.30 a.m., providing time to be driven by cab to the arranged venue, such as Royal Melbourne Hospital or Royal Park. Ten years were needed to acquire the DPM from the University of Melbourne in this leisurely manner.
During this period, Melbourne could boast several leading figures in the psychiatric profession. They should be mentioned here, to suggest the milieu within which John Cade functioned. I had many warm welcomes, not only from John Cade but from Eric Cunningham Dax, Alan Stoller and Alex Sinclair. I came to know them personally and each of them influenced me in ways that might not have been available in Adelaide.
The Overlander Express was not infallible. One night, three of its carriages were derailed in the Adelaide Hills near Belair. Enquiries predicted its arrival time in Melbourne at 3 p.m. I phoned John Cade and asked him to notify Royal Melbourne Hospital, where the Head of Medicine, Professor Lovell, was to examine me about medicine in psychiatry, with Dr Alex Sinclair.
When I duly arrived, Alex Sinclair was waiting alone. He apologised that Professor Lovell had had to leave, but he'd made a note of his questions. Dr Sinclair placed a half-bottle of Red Label Johnny Walker on the table for my trauma on the railway.
Alex had recently returned from army service in Papua New Guinea, and was trying to interest me in serving that population. ‘Here is one of Prof. Lovell's questions’, he put to me: ‘What's the cause of a headache that fades when the head is shaken?’. ‘I can't tell you,’ I replied. ‘All I know is that it's probably not a colloid cyst of the third ventricle. That myth has lapsed.’ ‘That's the answer,’ he smiled. Then he returned the Scotch and his notes to his brief case, and we terminated. ‘Come on, Cawte. Let's go to the club for a talk’, he suggested.
Venus arising from the waves
At the receiving houses we took in violent patients, no doubt as they had always been violent in history: as madmen needing madhouses, cast out from the throng of reasonable and cooperative humanity who made up the rest of medical practice, creating the stigma of psychiatry and the alien world of asylums. We were asked to treat frenzies that sedative or hypnotic drugs, ordered by doctors to be administered by nurses, would never assuage. Memory will not let go some images of these ‘madhouse’ performances.
Even Dr Birch (the superintendent of Parkside Mental Hospital in Adelaide), surrounded by his minions, could not safely escape them. It was his custom to visit Enfield after lunch on Friday afternoons. He did not inspect the premises, but expected me to have a list of items for his comment and decision. He would park his blue Jaguar outside the window of my office and sit at my desk while we discussed administration. The cook, Mr Jarvis, did his best with a Devonshire tea. Each of us was partial to fresh crusty scones with strawberry jam and whipped cream. It was usually the most memorable feature of the afternoon. Those brown crusts on the tops of hot scones. Oh, Glorious Devon!
But one Friday I had a woman suffering from severe mania lodged in the first room of the Female Admission Ward, adjacent to my office. Marjorie A. was a big lady, of some importance, occupying a senior position in one of Adelaide's business establishments. She always conducted her profession with skill and energy. On this occasion her energy had surpassed the level permitted in business, and she had to be certified to the Receiving House. Her élan proved impossible to curtail. Being in the Receiving House only drove her to greater heights. During the Devonshire tea in the front office, Dr Birch and I heard a commotion with noises of destruction. Looking out of our side window, we saw this large and strong lady, naked and dishevelled, sitting on the roof of the female ward. She was wearing nothing but a triumphant grin, astride the joists of the roof. She was tearing at the tiles with enough strength to rip them apart. She took to spinning them through the air as if playing at Frisbee, with shouts of glee.
Apparently, she had managed to stand her bed on end in her room, allowing her to climb on it and penetrate the ceiling, emerging finally through the roof. While we watched with disbelief this Venus arising from the waves, she noticed the beautiful blue Jaguar parked below. It was too far off to hit with a tile, but by practising spinning them she was able to glide closer and closer. We were terrified that she would score a direct hit on the car's roof or windscreen. Dr Birch no doubt feared for the car and I feared for the subsequent inquiry into my ward management. Those tiles were strong, made of heavy clay by Wunderlich. She spun them from the back of her hand. Thanks be to God the Jaguar was beyond her range. In the rush of staff that followed her naked ascent through the roof, one of our attendants fractured his arm. Her feat seems an act of merriment now, as I recall it; but in truth acute mania was not so funny. It was more like a feat of desperation. We rallied with Furies.
Mania in 1952
Let me be frank about mania in 1952, lest we forget. I was invited to write an account of the management of mania at Enfield for the Adelaide Medical Students' Society's The Review (1952). This was a quarterly in which I had a close interest. It had been banned from publication a decade or so before my years as a medical student for being salacious, in the view of the Registrar. I was only too happy to revive The Review and, after due warning from the Registrar, to edit the publication.
My contribution from Enfield was called ‘The Management of Acute Mania’. The rediscovery of this paper, 40 years later, overwhelms me: not our management of acute mania before the advent of lithium, chlorpromazine and haloperidol — no disease could be more harrowing for patient, nursing staff and doctor. No, it is the authenticity of this 1952 description of the struggle by the Receiving House to manage an illness too wild, too severe and too challenging for the means at hand. Here is an edited version of my frank account, written at the time, more specific than any remembrance of things past. It was my first medical publication and I beg leave to think of it now as a page of medical history.
‘Like many other important medical conditions, mania is not encountered in our student days. Rightly concerned with the somatic illnesses at the Royal Adelaide Hospital, we are apt to overlook the vast ebb and flow of “the other half of medicine” which takes place in the general practices and in the public and private mental hospitals. For this reason, it is proposed to describe a recent case of mania at Enfield. Study of such a case is more rewarding than a lecture on the subject, and will better illuminate the treatment available in 1952. The case was selected almost at random, happening to be one of four cases at Enfield at the time the Editor of The Review made his suggestion for this article; it is especially interesting because it shows that the illness is not always as benign as it is popularly considered.
Acute mania is probably the ‘brain fever’ of early novelists. However, it may not end so happily as in those stories.
Mr WT, aged 59, a salesman, married, Anglican, was admitted to Enfield Receiving House on 22/5/52, granted trial leave 17/6/52. He was brought to Enfield in an ambulance from a suburban hospital, strapped to a stretcher, struggling, yelling, abusive and threatening. The Tenth Schedule read:
This patient arrived at the hospital last night struggling and shouting incessantly to the sister on duty ‘Get f…’. He had 30 c.c. of paraldehyde by intramuscular injection but did not settle. He threw a bottle of urine over an orderly this morning. He is unable to make speech other than obscenities.
His brother who brought him in says he was well 2 days ago and then suddenly became unable to talk or behave rationally. He attacked his brother and struck him a number of times. He has not been consuming alcohol. He has not behaved like this before.
No accompanying letter was sent, but the Statement of Particulars gave the additional information that the illness was of 3 days' duration, that he was not an epileptic, and that the supposed cause was confusional psychosis.
A provisional diagnosis of acute mania was made, and the patient was placed in a single room under half-hourly observation. He did not sleep, shouted commands and abuse, stripped, kicked the door with his feet and banged with the bed on the floor. It was decided that no more hypnotic medication should be given, and to prevent the patient injuring himself further he was transferred to a padded room in a quiet part of the building, with a floor bed, and restrained in a moleskin camisole.
Next day his gross excitement continued, with a predominant display of anger. He cursed the attendants and would not permit them to come near him. He was capricious, loudly demanding food and drink which he dashed to the floor as soon as it was offered. The torrent of talk and activity continued as before.
As evening drew on the patient's excitement continued, the display of anger still predominating, but with shifts to boasting of his integrity and skill at games, imparting confidences, and to bursts of sobbing with his face buried in the pillows. As he was clearly becoming exhausted it was possible to carry out more thorough somatic and mental examinations. He refused to tolerate the presence of attendants, so that this had to be done unaided and was hampered by spells of aggression in which the examining doctor received some ‘free kicks’ which were followed by lachrymose contrition. He was fortunately highly distractible.
He was then prevailed upon to take two cups of tea and a slice of bread and butter, a feat requiring some perseverance owing to his distractibility and caprice. A sample of talk was copied down:
Here I was at lunch. I got up from the table with a fish-bone in my throat. This was only an excuse because I felt I was going to have a black-out. Do you know what a black-out is? You're a real good sort, Doctor. Better than those bastards of orderlies. They wouldn't even give a man a drink when he sang out for one. And I'm a TPI (totally and permanently incapacitated – a term for entitlement to war service benefits.) Do you know what a TPI is? My God, I wish I could get some rest, but I can't. Give me some rest! What sort of a doctor are you? Do unto others as you would have others do unto you.
By telephone it was next ascertained from the hospital where he had been previously treated that he had a syphilitic aneurism of the ascending aorta, and in addition liver damage owing to acute infectious hepatitis.
In view of his deteriorating physical condition it was decided, in consultation with Dr HM Birch, to give him electroconvulsive therapy (ECT). At first 80 V were passed for 0.3 s, but, as anticipated from his previous huge doses of sedative, it scarcely produced the required grand mal. This was repeated after 4 h, following which he slept for 2 hours.
The next day, although still acutely manic, he voluntarily took 40 ounces of egg-flip and other fluids. A grand mal was then produced by the ECT as soon as the stomach was judged to be empty; following this he took more food.
In the 2-minute period of coma following the next grand mal, the opportunity of performing a lumbar puncture was taken. The result was as follows: cerebro-spinal fluid (CSF) clear and colourless, under 140 mm water pressure; no cells detected; protein 30 mg%; Wassermann negative; colloidal gold curve 000000000; a normal spinal fluid showing no syphilis of the nervous system.
He ate a full evening meal voluntarily, slept for 3 hours, and was transferred back to a single room.
The next day he was much improved, though still ‘high’. He bustled in for his ECT, greeting one of the doctors with excessive camaraderie, talking volubly. He said he felt at the top of the tree. Noticing myself, he said: ‘My old friend. And to think that yesterday I called him a bastard. Oh, yes, I did. I'm the bastard’. He started to weep noisily, but was easily distracted.
He slept well during the night, but when examined next morning he was perplexed and for the first time consciousness appeared to be clouded. He said: ‘Shut that door. I want to confide in you. I'm so ashamed. Now, this is the trouble: my mother died in a mental hospital. Isn't that awful? You don't know what we went through. It was awful. That's why I'm here now. What is this place? Is it Northfield or Enfield? How did I get here? I've got to get out for a game of bowls tonight. I'm expected. You know, a lot of those fellows out there used to work for me’ (pointing to a courtyard).
After 2 more days he was eating and sleeping normally, and there was no abnormality of mood. The ECT was discontinued after nine treatments. There was slight retrograde amnesia and confusion arising from the ECT, which cleared in a week. He adapted himself well to the hospital routine, and took part spasmodically in games and occupational therapy, but remained unsettled and ill-at-ease, eventually requesting psychotherapy.
This at first took the form of a personality study conducted by himself under our guidance. It was a most interesting study, during which he discovered that his acute illness, far from being a punched-out episode or bolt from the blue, was in fact an exaggeration of his usual response to emotional stress. This finding seemed to afford him some relief. He revealed that during the previous 2 years he had suffered much ill-health, including infectious jaundice, prostatectomy, and then pains in the chest, diagnosed as arising from an aortic aneurism. The latter he was informed was caused by syphilis, which was then treated with penicillin and other injections. He stated that the infection must have been picked up in England during the First War when he had become friendly with a girl whom he had thought nice, but who had given him gonorrhoea.'
Managing mania before lithium
My 1952 article continued:
‘While on the subject of seclusion and restraint of patients, it may be remarked that alienists are occasionally taunted by medical colleagues for their continued use of these “barbaric”, “humiliating”, “assaults on medical ethics”; alienists however, do not much mind being taunted, even by inconsistencies such as these, but point out that nobody hesitates to treat a case of tetanus or a fracture by exactly similar means, whether the patient likes it or not. In such cases, if the doctor feels certain that the patient's judgement is gone, he must be bold enough to replace it with his own (hoping for a charitable magistrate) or he may leave well alone. For every such problem general medicine presents, psychiatry seems to present a dozen; practical solutions are not, alas, in the textbooks.
The question has been asked: “It is understood that acute mania, if allowed to run its course, will clear up entirely; why, then, subject the patient to the frightening, dangerous, and horribly painful ordeal of ECT?”
Reverting to the case described, if ECT had been rejected, an alternative would have been the older method of prolonged deep narcosis. We are not experienced in this rather dangerous procedure at Enfield but have used Somnifaine. Amytal and Soneryl are used in the USA and Cloetta mixture (paraldehyde, chloral hydrate, isopropylallyl barbituric acid, digalin and ephedrine) in Europe. The patient is virtually anaesthetised for more than a week. The optimum therapeutic dose is very near the minimum lethal dose, but in the case described, owing to the patient's extraordinary tolerance, we felt that it would probably have exceeded it!
Cardiazol was not considered; it is a relatively violent analeptic and its only use at Enfield recently is in certain pseudo-affective schizophrenics and in the diagnosis of hidden epilepsy.
Hydrotherapy has had a great vogue in the USA; the patient sits in a tepid bath for upwards of half an hour, when the water is suddenly chilled to 70 Fahrenheit; he then wraps himself in blankets, where shivering soon gives way to surface vasodilation with a feeling of warmth and drowsiness. We find hydrotherapy a splendid sedative for certain cases, but it surely needs a co-operative patient!
Supportive measures include the various methods of keeping the patient in the best possible physical condition despite his mental illness. It will be recalled that the cardinal feature of acute mania is the disturbance of the physiological processes of sleeping, eating and sex.
More harmful than loss of sleep is loss of food intake. The urine is watched for acetone; a heavy acetonuria from fasting is an indication for tube-feeding. A standard feed contains, first, a few ounces of water, then a pint of Aktavite, with two eggs, sugar, orange juice, and a little Marmite, followed last by water. Glycerine, inevitably preferred as a lubricant by nurses, irritates the nasal mucosa; use paraffin. Tube feeding, formerly frequently required in mental hospitals, is now rarely used following the introduction of ECT. It is distressing to the patient and potentially dangerous.
Coaxing of patients is more important; in acute mania, there is a battle of wits in which the patient's distractibility can be utilised to his own good. It is never beneath the doctor's dignity in such a case to spend an hour trying to feed his patient; the first cup of tea is often the beginning of recovery — a satisfying achievement.
Occupational therapy of some sort is essential; the acute manic often fancies himself as a ‘lightweight’, ‘middleweight’, or ‘heavyweight’ and enjoys the punching ball. He never keeps it up for long, however, and may decide at 3 a.m. that cleaning the lavatory has more priority.
During the acute phase some psychotherapeutic measures are responses that one really practises instinctively after making one's initial blunders. The first measure is to observe sufficient decorum and solemnity. It is tempting, faced with an infectiously jovial maniac, to respond to his mood and return his jokes; this succeeds in making it harder for the patient to conduct himself as he might wish in the presence of a doctor. Joking conversation achieves nothing. Secondly, if one listens to the stream of talk, copying some down if necessary, it turns out not to be the ‘flight of ideas’ or disconnected ramble it would appear. It may contain, as it did in the case described, information germane to the actual treatment. Curiously, glimpses of content thus obtained show that it is depressive in nature or concerned with circumstances that one would logically expect to produce depression. In these cases (the majority) the elation is a depressive equivalent, perhaps a defence against depression. And thirdly, in bellicose patients, a display of overwhelming strength often brings humorous resignation and averts a fight: to see the morning-tea delivered by four attendants is an interesting sight and psychotherapically effective!
Unfortunately, clear-cut issues are rare in psychiatry; while it is true that most recovering maniacs neither desire nor need formal psychotherapy, individual cases show clear indications and benefit greatly from it. The method to be used suggests itself during investigation of the complaint-material. The method used in this case happened to be similar to the Meyerian personality study, for reasons personal to the therapist. It was, it happens, pertinent to the case. If the therapist is not ‘at home’ in Freudian usage, through ignorance or some personal aversion, he has several other alternatives at his disposal while still using some Freudian concepts. Patience in developing a satisfactory doctor–patient relationship, combined with caution in interpreting and interfering, appear to be factors common to all safe methods.
In the case described a promising line of treatment was not followed up because the therapist did not have sufficient time to assess its risks and therefore chose not to interfere. In a psychiatric clinic of some 80 beds, run rather doggedly by two full-time doctors, opportunities are bungled and a tithe of the necessary treatment carried out. Enfield doctors are not alone to blame for this inadequacy. More at fault is the fear and contempt for mental illness still projected by otherwise responsible physicians at our teaching hospitals, and introjected by their students. Many students have, at first, much curiosity concerning mental sickness, feel some kinship with those sick, and should be spared this implicit discouragement from throwing in their lot with this most fascinating aspect of medicine. These students will eventually correct conditions imposed by their predecessors; it is a pity that it is being unduly delayed in Australia.] [1]
Reflections
Such severe or delirious mania was then common behind the walls of the Receiving House. Casting out this incubus spelt pain for the patient and penance for the doctor and the staff. This account, then, is how it was, from notes made at the time. It illustrates our attempts to develop sensitivity to the problems of patients, for whom many modern therapists might rely on drugs and systems, and so may be valuable as we celebrate John Cade's discovery.
John Cade – on the day of his retirement (Photograph courtesy of Mrs Jean Cade)
Left to right: Poul Christian Baastrup, John Cade and Mogens Schou (Photograph courtesy of Professor Schou)
John Cade, 1948 – on his way to the laboratory taken at the gate of his house at Bundoora Repatriation Hospital, Melbourne. (Photograph courtesy of Mrs Jean Cade)
John Cade (Photograph courtesy of Mrs Jean Cade)
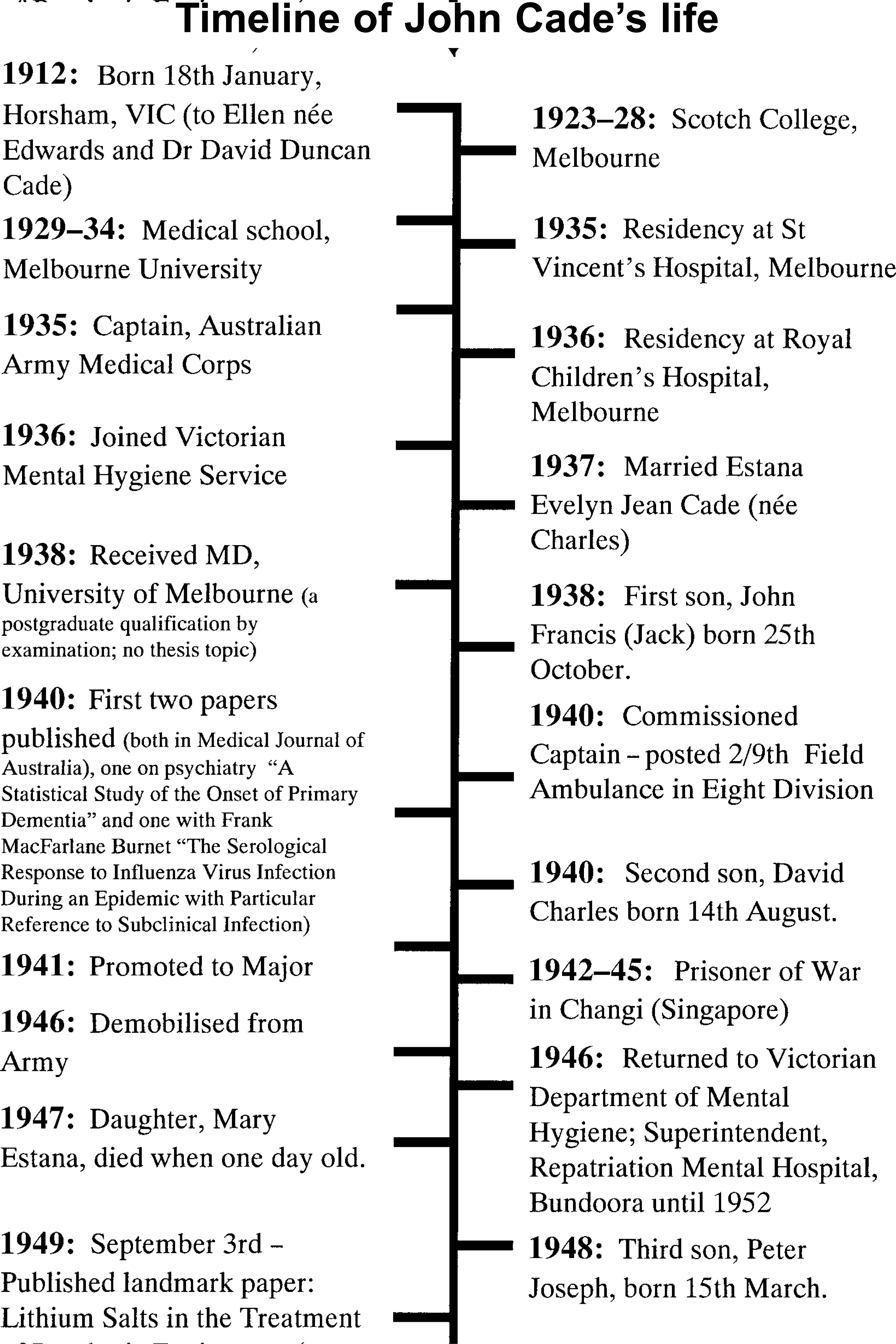
Timeline of John Cade's life
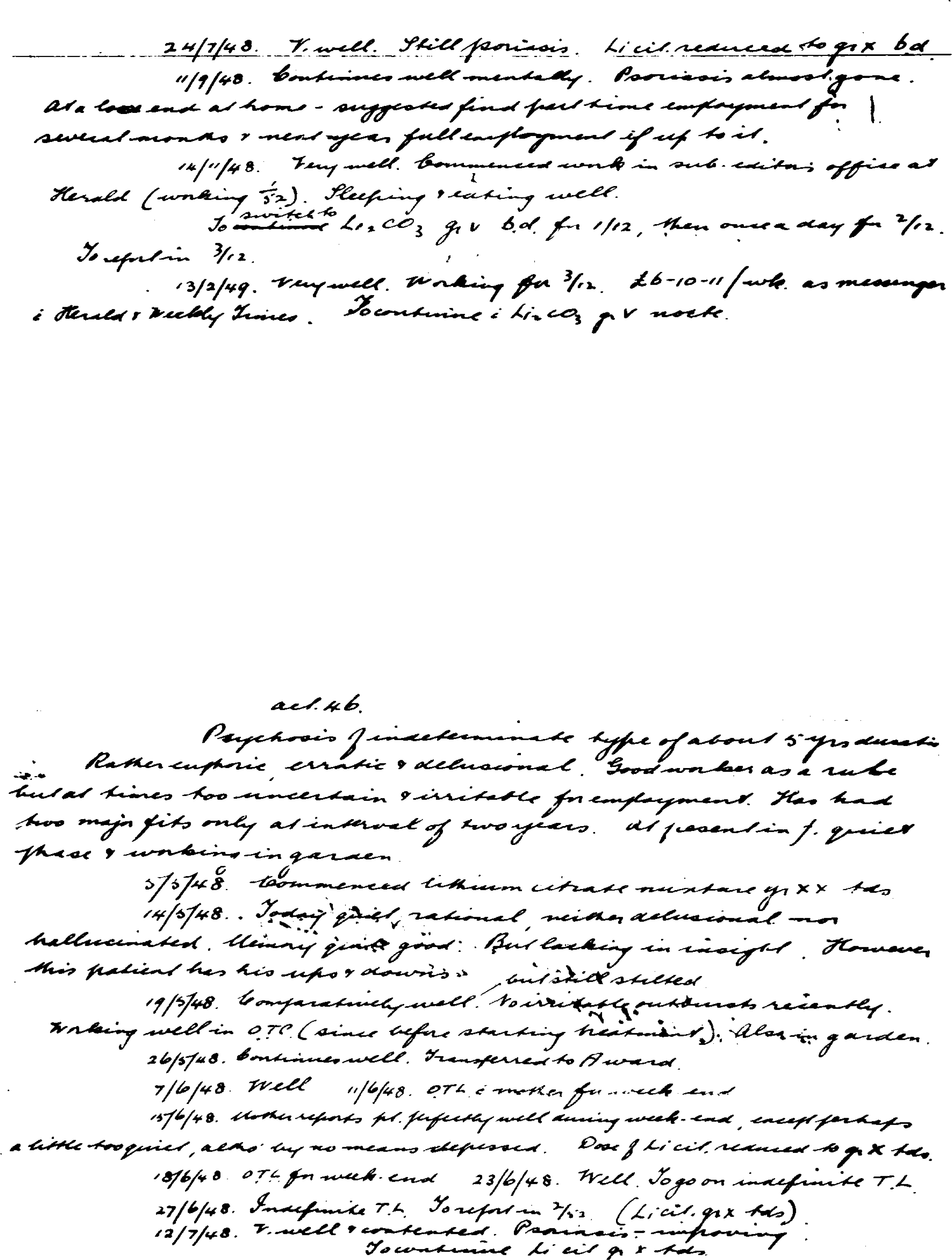
Cade's notes of patients described in his 1949 report in the Medical Journal of Australia: Case 1
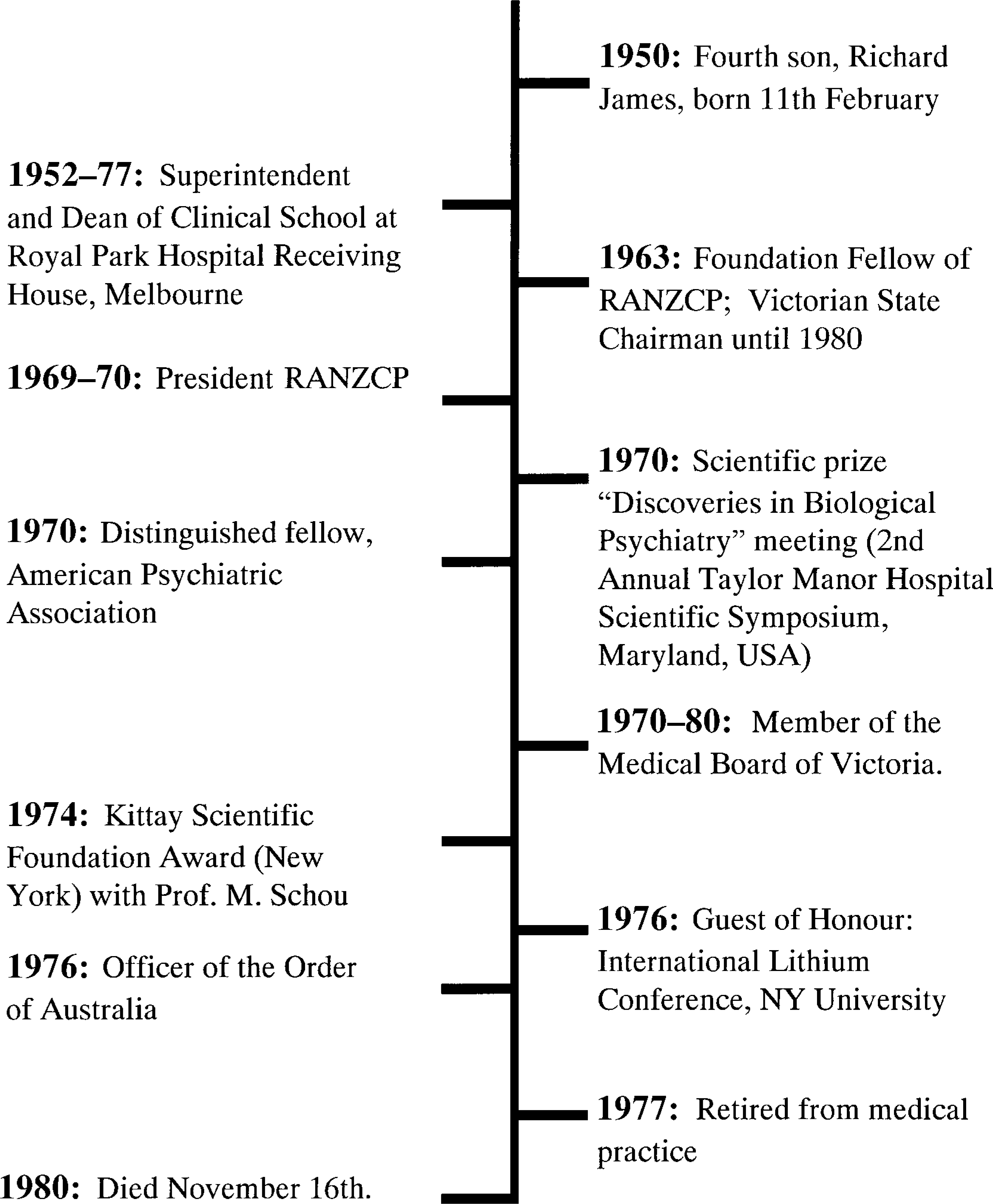
Cade's notes of patients described in his 1949 report in the Medical Journal of Australia: Case II
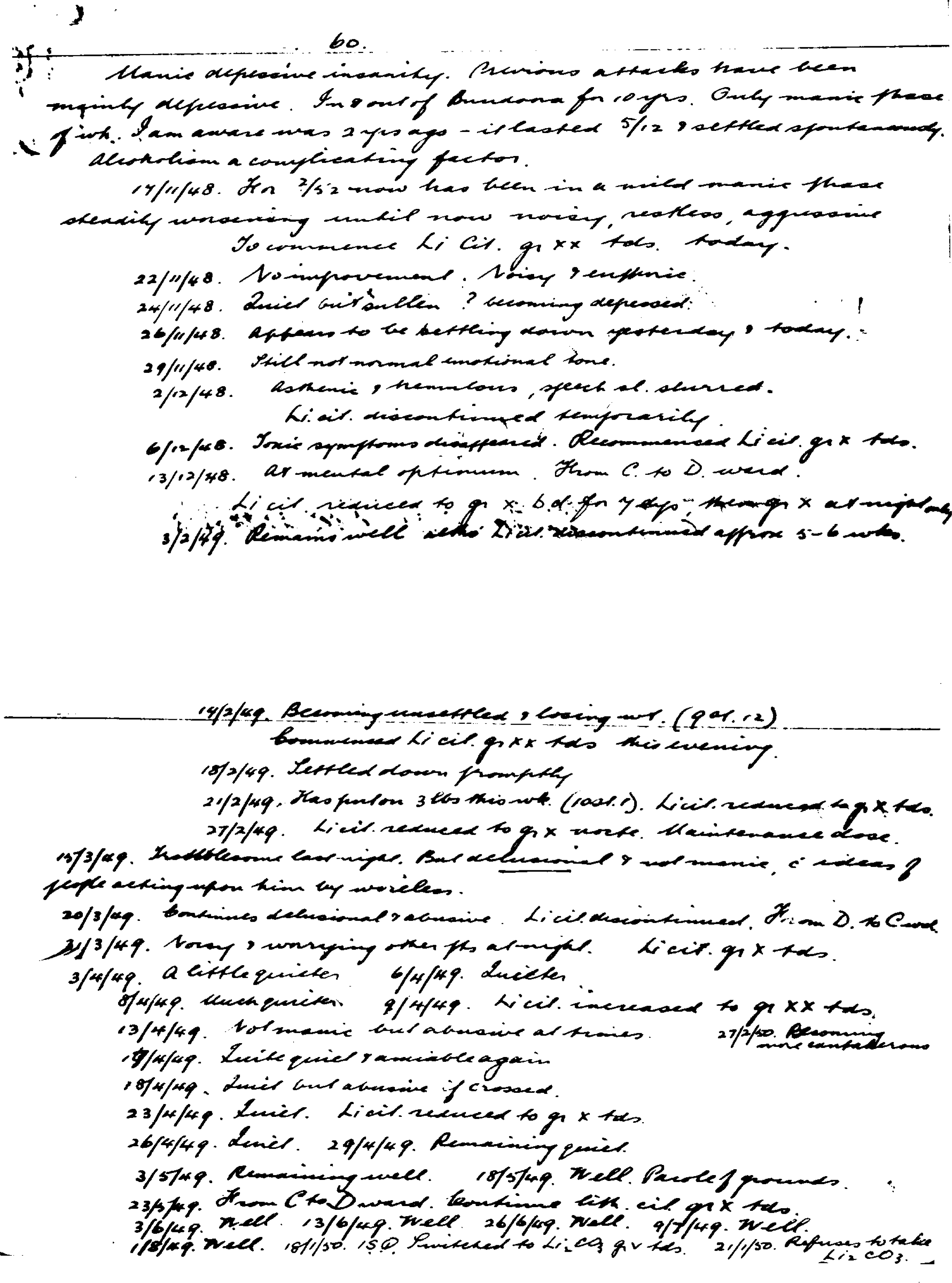
Cade's notes of patients described in his 1949 report in the Medical Journal of Australia: Case III
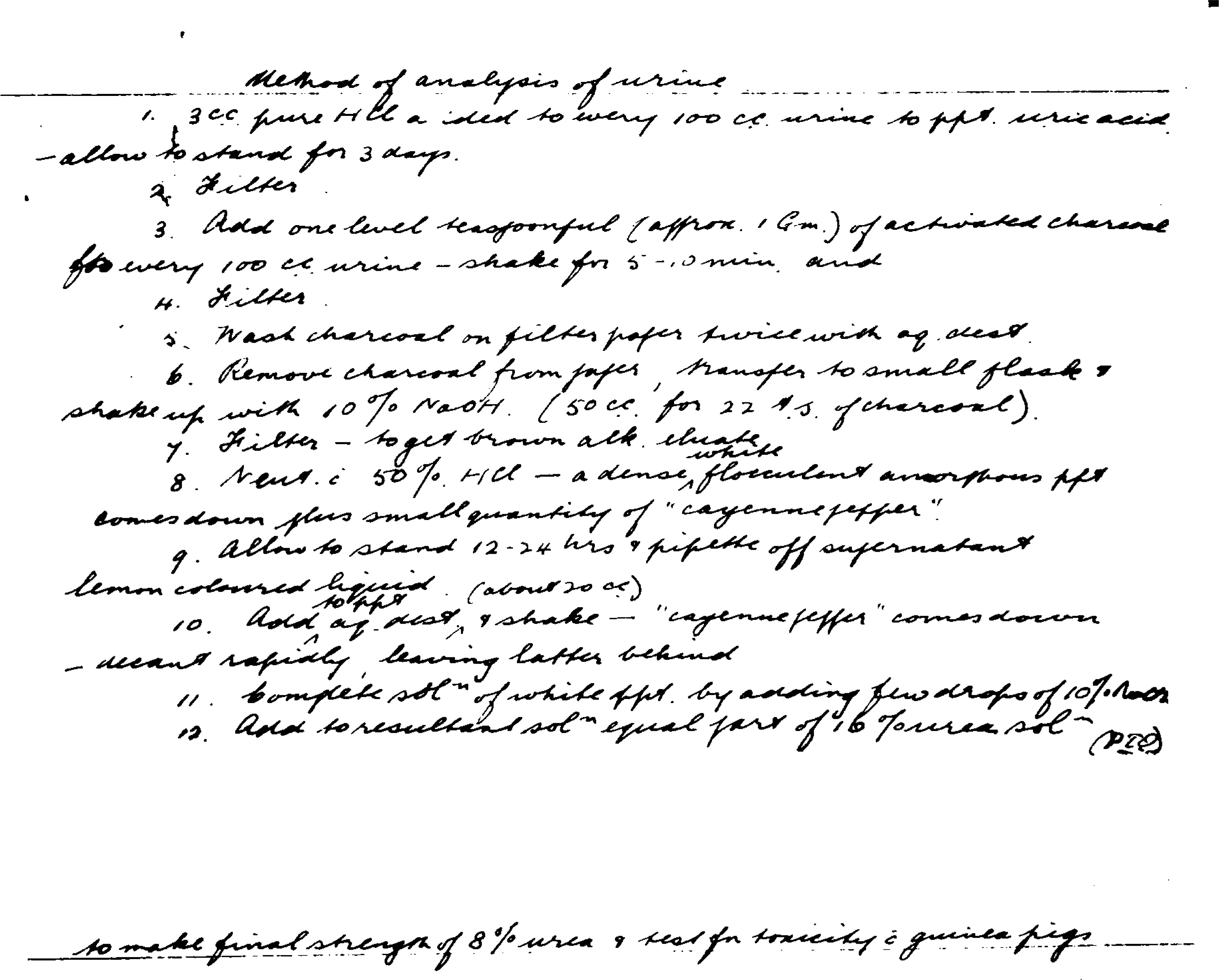
Cade's laboratory notes — methods of urine analysis
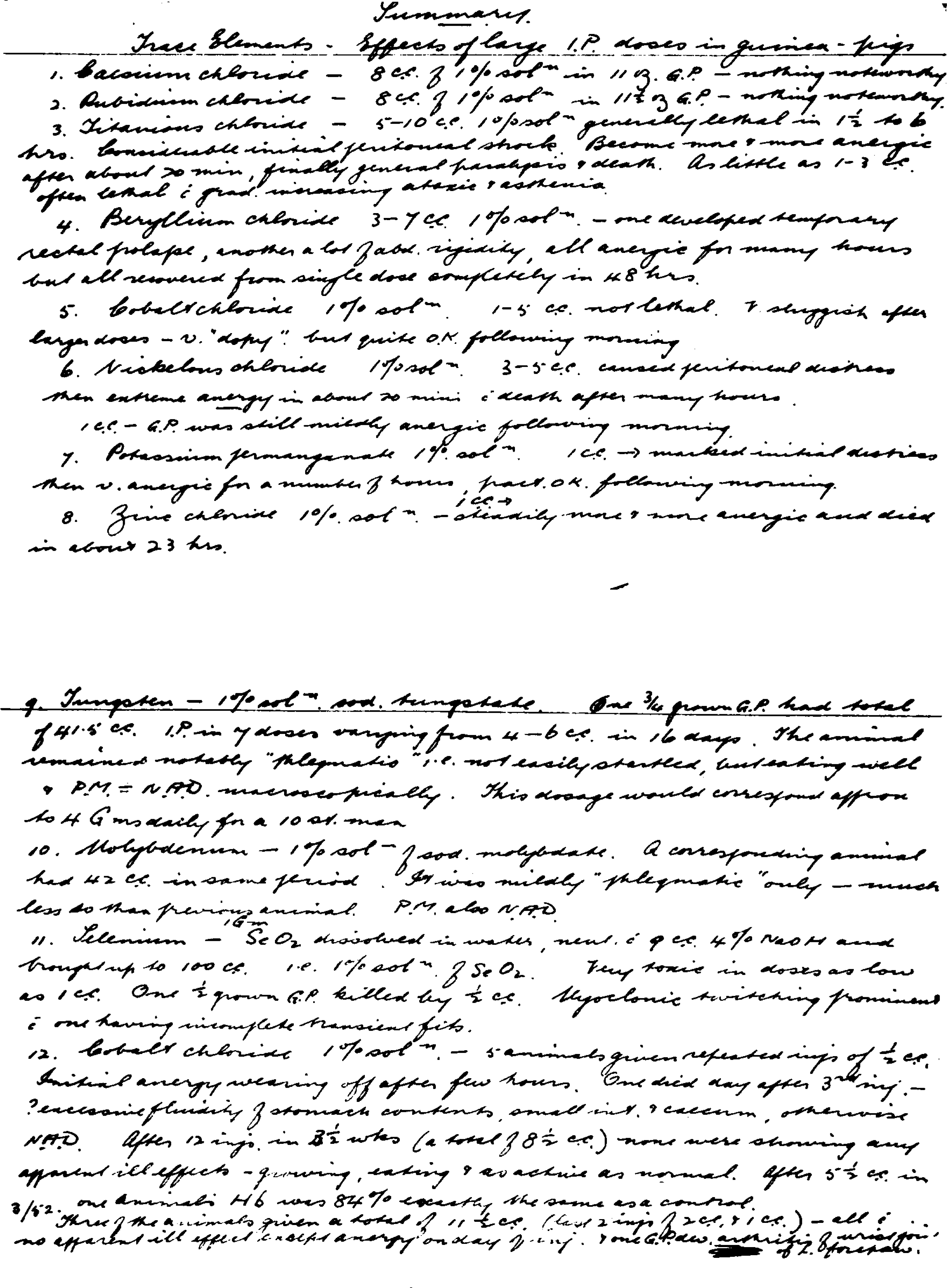
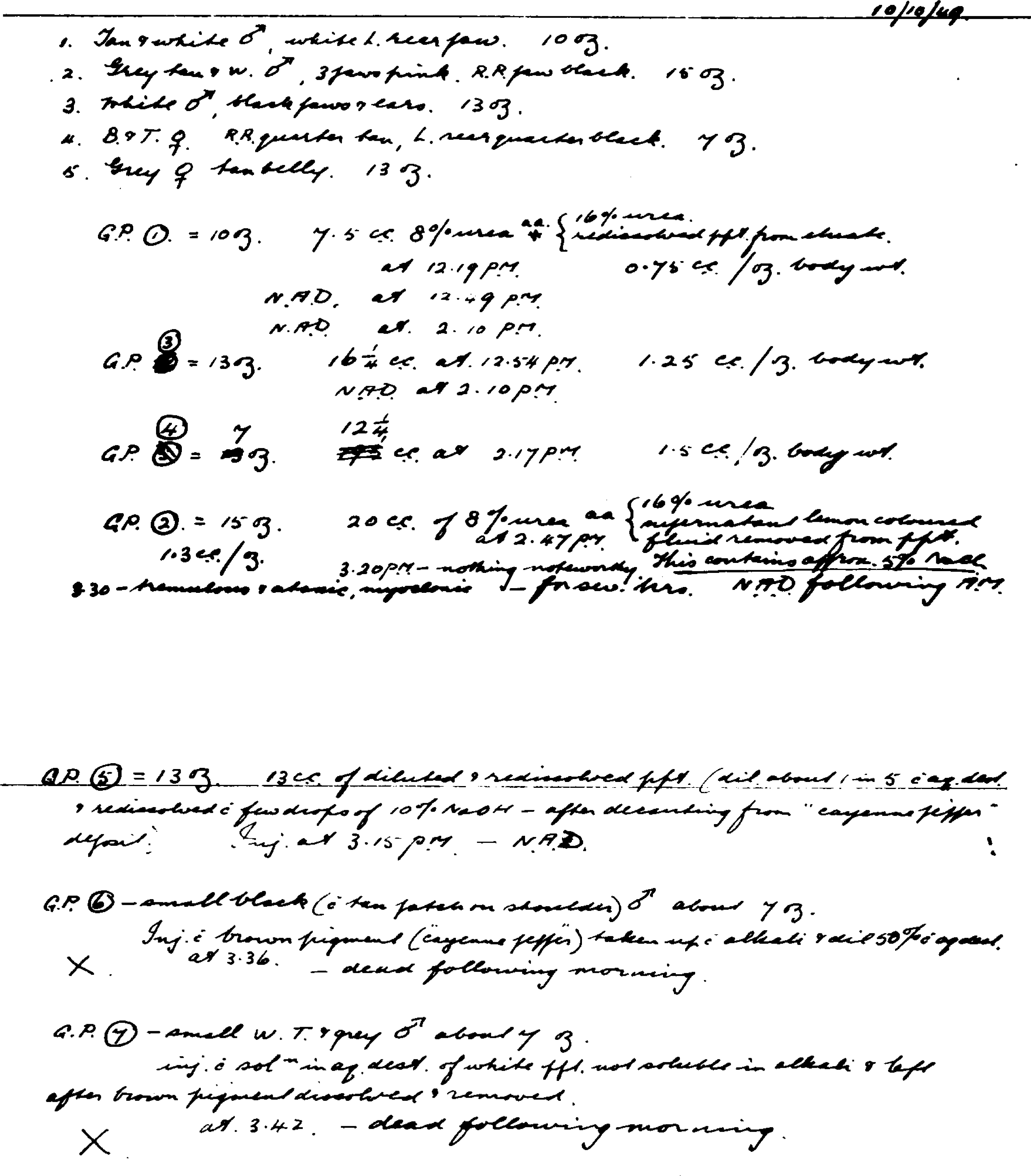
Cade's laboratory notes – The effect on guinea pigs of injections of various compounds
Cade's laboratory notes – the effect of various trace elements on guinea pigs