
Abstract
Acute mania in bipolar disorder usually results in admission to hospital with the aim of rapid symptom control. The Royal Australian and New Zealand College of Psychiatrists clinical practice guideline (CPG), published in 2003, recommends that acute treatment should be with a mood stabilizer with/without adjunctive/symptomatic treatments (benzodiazepines and antipsychotics) [1]. There is good evidence demonstrating superiority of lithium, valproate and carbamazepine over placebo in acute mania [2], [3]. Carbamazepine is not used as a first line option, however, because of mixed results in maintenance studies [1], poor patient acceptability (due to adverse effects), and enzyme-inducing properties (causing self-induction and many drug interactions).
The CPG recommends initiating lithium at 750–1000 mg daily, adjusting to achieve a serum level of 0.8–1.2 mmol L−1 [1]. Valproate is recommended to start at 400–800 mg daily with adjustments to achieve a serum level of 300–800 µmol L−1 (approx. 45–115 µg mL−1l) or to use a loading strategy commencing with 20–30 mg kg−1 per day aiming for the same concentration range [1].
Although general advice is that lithium should be titrated (based on concerns about a narrow therapeutic index) [4], [5], John Cade's original description of lithium in the treatment of manic disorder was of a loading strategy [6]. Eight of the 10 patients given the equivalent of approximately 1900 mg of lithium carbonate daily responded within 3–14 days of starting. Cade concluded that it was advisable to initiate treatment with the maximum expected dose and gradually reduce the dose after resolution of the acute mania [6]. Loading strategies with sodium valproate have recently been reported as safe and effective [7–10].
Both serum level and time taken to achieve therapeutic levels are factors in the degree and rapidity of response [11–19]. Lithium levels of at least 0.8 mmol L−1, and often 1.0 mmol L−1 have been associated with response rates similar to that reported by Cade [4], [11], [17]. Recommendations for valproate typically identify a wider therapeutic range: 350–875 µmol L−1 (50–125 µg mL−1) [1], [20–22], although evidence is growing to support a similarly narrow window for valproate. An initial study with valproate reported that levels >45 µg mL−1 (300 µmol L−1) were associated with greater improvement and that levels >125 µg mL−1 (875 µmol L−1) were associated with adverse effects [22]. More recently, Allen et al. have proposed a target serum valproate level >94 µg mL−1 (approx. 650 µmol L−1) for best response in acute mania [19]. Goldberg et al. in a naturalistic study found that the number of weeks needed to achieve therapeutic serum levels predicted the length of time to achieve remission in mania. Delay in optimizing the serum level, irrespective of the mood stabilizer chosen, could delay clinical response [16].
A local guideline for lithium treatment was developed, including advice on loading [23]. The loading strategy suggested was 30 mg kg−1 per day (to a maximum of 2000 mg day−1) aiming to achieve a serum level of 1.0–1.4 mmol L−1 within 5 days. As part of the guideline development process a small internal file review (39 consecutive bipolar mania admissions over 8 months in 2000) showed that the rate of response with lithium loading appeared to be faster (achieving levels of ≥1.0 mmol L−1 in 5 days; n=12/27) compared with dose titration to achieve similar levels (n=15/27). The average length of hospital stay was halved by loading (mean = 20.2 days, SD = 7.11, vs titrating mean = 39.9 days, SD = 24.2, p = 0.011).
A larger review of the use of mood stabilizers in acutely manic inpatients in a naturalistic setting was therefore undertaken to assess whether clinical practice followed these evidence-based recommendations. With the results of the internal review suggesting that lithium loading was effective in shortening the response time, a secondary objective was to replicate this finding on three broad indicators of outcome as a result of loading compared with titrating mood stabilizer treatment.
Methods
Patients and setting
This study was a retrospective review of all patients with bipolar disorder, manic episode admitted to two psychiatric inpatient units in Auckland, New Zealand over a 12 month period (1 January–31 December 2001) who were started on lithium or valproate within 72 h of admission (n = 93). Patients were identified from the electronic Patient Information Management System and each paper clinical file was then screened for inclusion in the study. Patients prescribed mood stabilizers prior to admission were included only if there was evidence that the medication had not been taken leading up to admission and acute treatment was restarted, or if there was an abrupt increase in the usual maintenance dose.
In the absence of written statements of prescriber intentions, lithium loading was defined as a total daily dose ≥1500 mg in the first 24 h or a serum level in the first 3 days of treatment ≥1.0 mmol L−1, and valproate loading as a dose of ≥20 mg kg−1 per day or a total daily dose ≥1500 mg in the first 24 h or a serum level >350 µmol L−1 (50 µg mL−1) in the first 3 days. All other prescribing variations were defined as dose titration.
The two acute adult inpatient units serve a total population of almost 300 000 adults within the Auckland region (2001 Census [24]). The area has the fastest growing population in New Zealand and the inpatient units also support the greater Auckland region as needed (adult population, 786 468 [24–26]). The emphasis on community-based care has been associated with a relative reduction in availability of acute psychiatric beds [27], with consequent increased levels of acuity and average length of stay (LOS) [28]. Liaison with the patient's community psychiatrist often determined the medication chosen or continued during the hospitalization. Both units have a small locked intensive care unit (ICU) for management of more acutely behaviourally disturbed patients.
Data collection and analysis
The data retrieved from the clinical file for each admission included demographic (gender, age, and ethnicity) and clinical data (legal status, discharge diagnosis, psychiatric admission history, LOS, intensive care and seclusion use, mood stabilizer and adjunctive/symptomatic treatment). The clinical data were used as indirect indicators of outcome because no standardized rating of response was used in routine practice. All serum levels and any adverse effects (either subjectively or objectively recorded) were also collected with the corresponding prescribed dose.
Data were collected and entered into a Microsoft Access database by final year undergraduate pharmacy students. Statistical differences between the two treatment strategies were investigated using χ2 tests for categorical values and t-tests for continuous variables. When sample distributions did not satisfy assumptions of normality (e.g. LOS) or when samples were small (e.g. <30) non-parametric tests were used. A general linear model was used to test for differences between the three indirect outcome indicators (log transformed), hospital LOS, time spent in ICU and seclusion and the two treatment strategies. The model included demographic (age, gender, ethnicity), clinical and acuity (mania with/without psychosis, compulsory status, comorbid substance use disorder, admission history, lithium or valproate) covariates and the interaction between ‘mood stabilizer and dosing strategy’. Statistical analyses were conducted using SPSS version 15 (SPSS, Chicago, IL, USA) and a significance level of 5% was considered statistically significant.
This audit of clinical practice was undertaken as part of the service's quality assurance processes and as such did not require ethics approval.
Results
A total of 93 admissions met the inclusion criteria over the 12 month study period. A loading strategy was prescribed in 46.2% and titration in 53.8% of admissions. Table 1 shows the demographic, clinical and acuity indicators (legal status, use of adjunctive medication in the first 72 h, in particular i.m. medication) and mood stabilizer choice for the total study population and between the two dosing strategies. Psychotic symptoms were present in the majority of admissions (n = 84; 90.3%) and one-third of admissions had a comorbid diagnosis of a substance use disorder (n = 30; 32.3%). More than 80% of patients were admitted under compulsory status, and almost all received adjunctive treatment acutely. These findings indicate high levels of acuity and disturbed behaviour. Lithium was the mood stabilizer prescribed for more than two-thirds of the study population.
Bipolar mania inpatient population treated with acute mood stabilizer treatment (lithium or valproate)
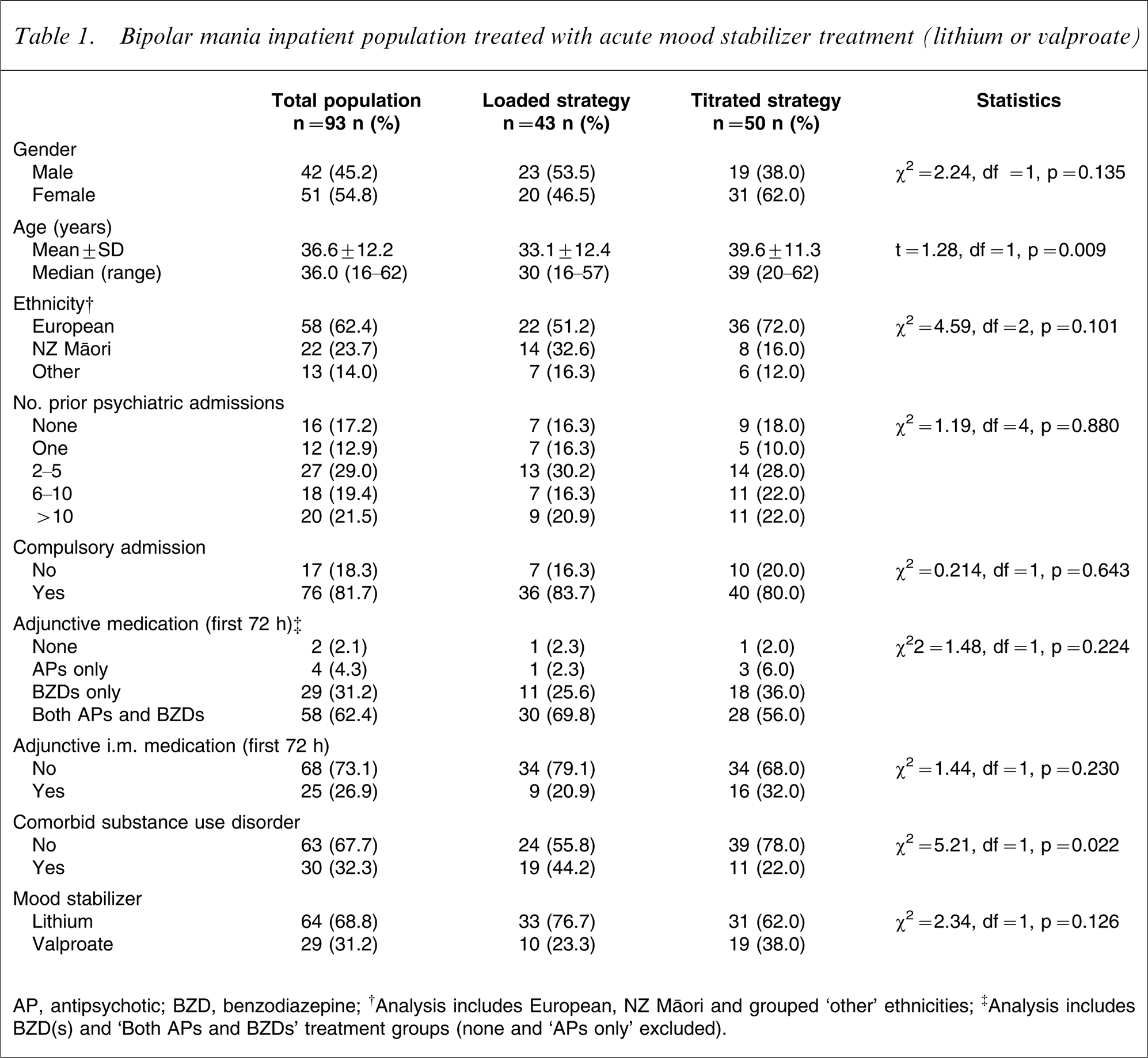
AP, antipsychotic; BZD, benzodiazepine.
†Analysis includes European, NZ Maori and grouped ‘other’ ethnicities.
‡Analysis includes BZD(s) and ‘Both APs and BZDs’ treatment groups (none and ‘APs only’ excluded).
The two treatment groups were similar with respect to gender and ethnic background, psychiatric hospitalizations, and acuity indicators (Table 1). The two significant differences found were that the loaded group were younger and a higher proportion had comorbid substance use disorder. The 93 admissions involved 73 people, of whom 16 had more than one admission during the 12 month study period. There was no difference in the distribution of the patients admitted more than once between the loaded or titration groups (χ2=0.145, df = 1, p = 0.703).
Mood stabilizer treatment strategy
Dosing and serum levels
The mood stabilizer dose prescribed on day 2 of treatment was significantly higher for the loaded group irrespective of mood stabilizer choice; average lithium dose was 1679 mg day−1 (median = 1600 mg day−1) for loading compared to 994 mg day−1 (median = 1000 mg day−1) for titrating strategy (Mann–Whitney U-test, p < 0.001); and average valproate dose was 1930 mg day−1 (median = 1850 mg day−1) for loading compared to 1032 mg day−1 (median = 1000 mg day−1) for titrating strategy (Mann–Whitney U-test, p < 0.001). Although twice as many patients in the loaded group (84% vs 40.0%) achieved the maximum dose prescribed during their admission within 24 h of starting treatment, clinicians used a fairly rapid dose titration. The maximum daily dose was reached in an average of 5.7 days (median = 3 days) compared to an average of 4.1 days (median = 2 days) for the loaded group (Mann–Whitney U-test, p = 0.001).
Although at least one serum level was recorded in all but six admissions, this was often taken after day 5. The average time after starting treatment until the first recorded serum level was 5.1 days (median = 4 days, SD = 4.1, range = 1–21 days), and there was no difference between treatment strategies (loaded median = 4 days vs titrated median = 5 days, Mann–Whitney U-test, p = 0.589). When the level was taken earlier and was sub-therapeutic it was rarely repeated. Consequently, it was not possible to fully validate the loading or titration groups with serum levels. In two-thirds of admissions (68.8%) it was not possible to determine if a therapeutic level had been reached by day 3; and even at day 5, in almost half the admissions (47.3%), it still was not possible to determine if dosing had achieved a therapeutic level (lithium serum level ≥1 mmol L−1 or valproate >350 µmol L−1).
For admissions in which levels were known, at day 3 more patients who had received the loading strategy had reached a therapeutic level (Table 2). Subsequently there was no difference between the two strategies.
Serum levels recorded with acute mood stabilizer treatment
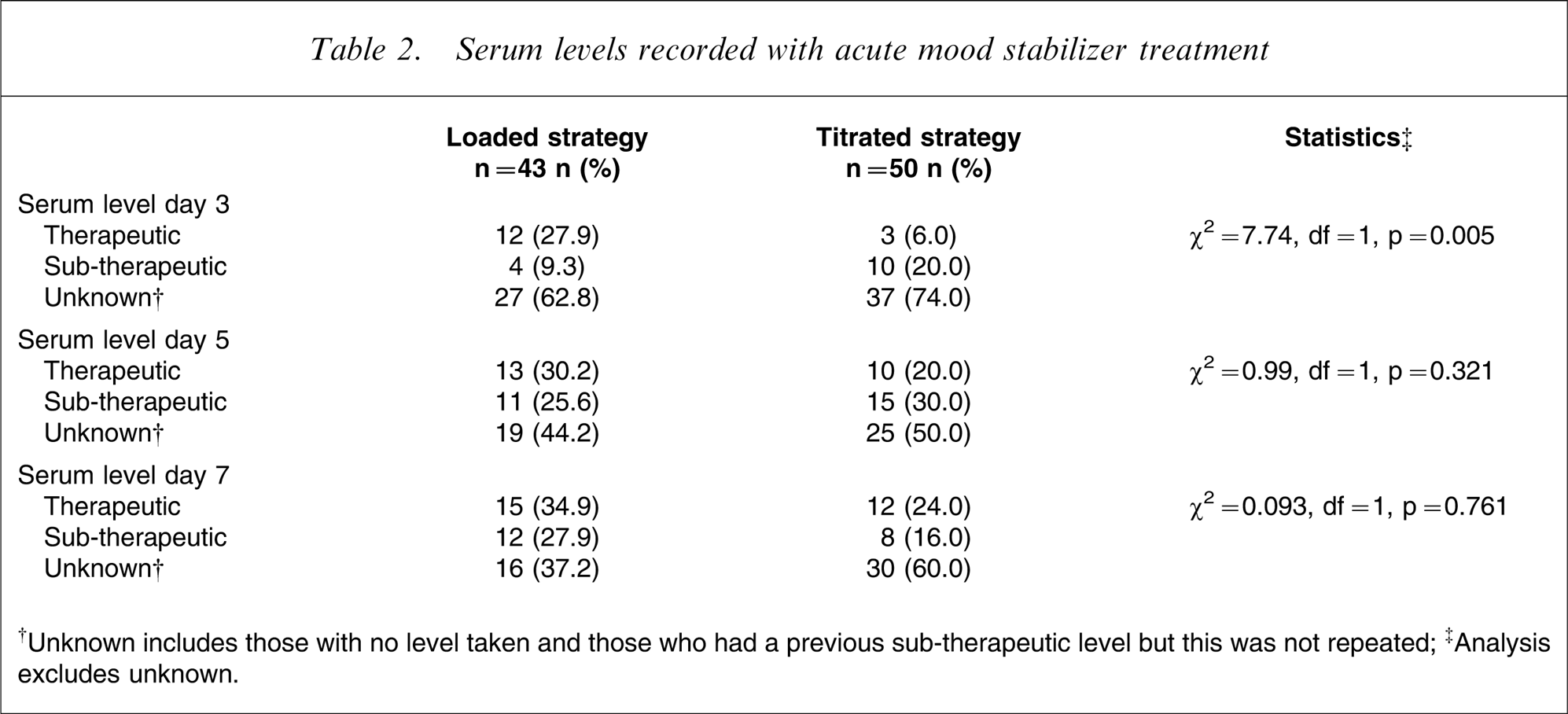
†Unknown includes those with no level taken and those who had a previous sub-therapeutic level but this was not repeated.
‡Analysis excludes unknown.
The high level of unknown serum levels in the audit was unexpected, mainly due to not measuring valproate levels. By day 7 at least one serum level had been recorded for 62.5% of the lithium group and for only 24.1% of the valproate group.
Indicators of outcome
Table 3 shows the comparison of three indicators of outcome between loading and titrating. The average hospital LOS for the total population was 30.2 days (SD = 24.1, median = 21.0 days, range = 6–126 days). No difference in average LOS in hospital was found between loaded or titrated groups.
Indirect indicators of outcome with acute mood stabilizer treatment
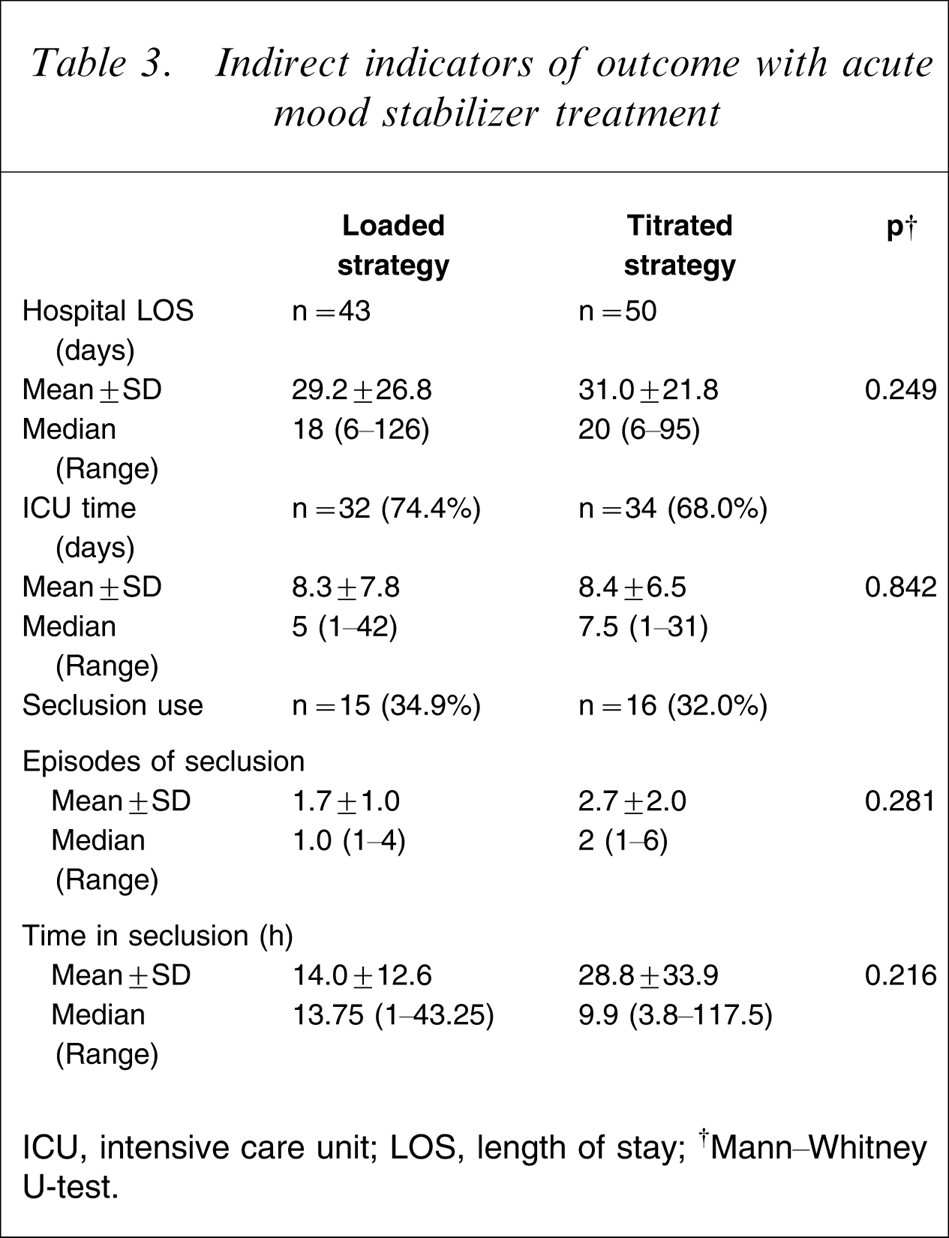
ICU, intensive care unit; LOS, length of stay;
The second indicator was treatment in the ICU. Treatment in this setting was required for 71.0% of admissions (n = 66/93) and this proportion was not significantly different between treatment groups (loaded = 74.4%, titrated = 68.0%, χ2=0.462, df = 1, p = 0.497). Length of time in ICU was an average of 8.4 days (SD = 7.1, median = 6.0 days, range = 1–42 days) with no significant difference between treatment strategies. Third, seclusion was needed in one-third of admissions (n = 31/93, 33.3%) and again this was similar in both treatment groups (loaded = 34.9%, titrated = 32.0%, χ2=0.087, df = 1, p = 0.769). Neither the average number of episodes in seclusion nor the total time in seclusion was found to differ significantly between loaded or titrated strategies.
The general linear analysis investigating independent variables associated with total hospital LOS (log transformed) found associations only with ethnicity (p < 0.001) and comorbid substance use disorder (p = 0.009); NZ Māori had longer hospital LOS (mean = 44.9 days vs European 27.3 days vs other 18.2 days), as did those without a comorbid substance use disorder (mean = 31.5 days vs with comorbid substance use disorder 27.3 days). The lack of association for the interaction effect (p = 0.852) inferred that the pattern of association between loading and titrating for total LOS was the same for both lithium and valproate, and undertaking a subgroup analysis for each mood stabilizer was not necessary.
Similarly, time in ICU (log transformed), was associated only with ethnicity (p = 0.006); NZ Māori having longer time in ICU (mean = 9.7 days vs European 4.7 days vs other 4.9 days). Last, the analysis examining time in seclusion (log transformed) found no associations with any of the covariates or the mood stabilizer×treatment strategy interaction included in the model.
Adverse effects
In 40 admissions (43.0%) at least one adverse effect was recorded that could have been related to mood stabilizer treatment. Table 4 shows the frequency of adverse effects between the four treatment groups. Other adverse effects included dry mouth, increased thirst and appetite, weight gain, night sweats, stiffness, shivering and blurred vision. One patient treated with valproate developed clinically significant thrombocytopenia 4 days after discharge.
Adverse effects recorded during inpatient admission
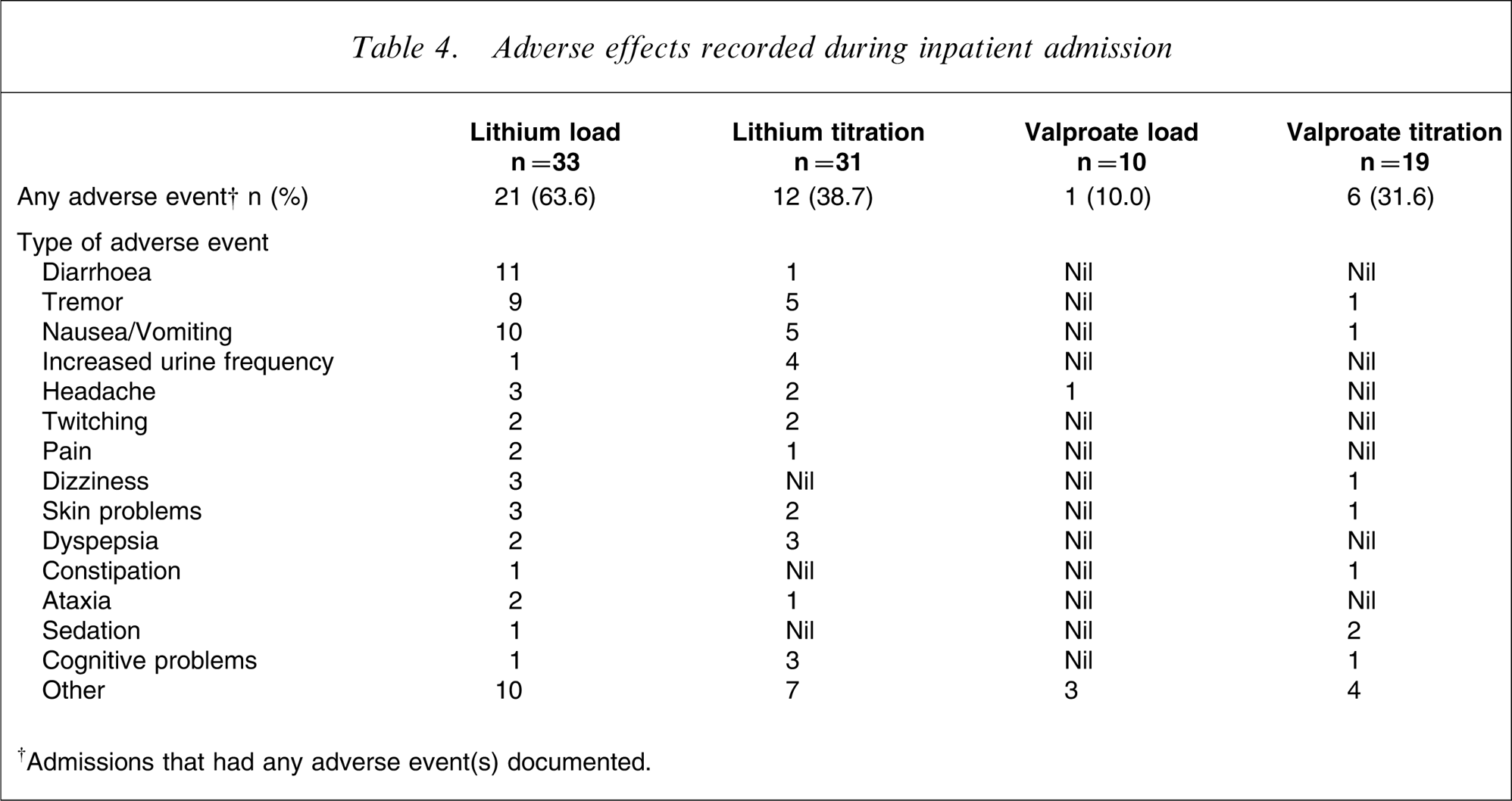
†Admissions that had any adverse event(s) documented.
The rates of reported adverse effects did not differ significantly between the two dosing strategies (loaded = 51.2%, titrated = 36.0% (χ2=2.17, df = 1, sp = 0.141). There was a difference found, however, for patients treated with lithium (n = 64, χ2=3.98, df = 1, p = 0.05); the loading group having a higher proportion reporting adverse effect(s) (63.6%) than the titrated group (38.7%). No difference was found with valproate treatment between loading and titration (n = 29, χ2=1.67, df = 1, p = 0.197). Overall there were significantly more adverse effects reported with lithium than with valproate, irrespective of loading or titration (51.6% vs 24.1%, respectively, χ2=6.12, df = 1, p = 0.013).
Discussion
This review of lithium or valproate in acute mania in routine inpatient practice found that most demographic, clinical and acuity indicators between patients prescribed loading versus titration treatment were similar. The loaded group were found to be younger and had more recorded comorbid substance use, but there was no difference between any of the indirect indicators of illness severity or behavioural problems; compulsory status, use of adjunctive medication, in particular i.m. administration in the first 72 h, need for intensive care and/or seclusion between the treatment groups. The decision-making process regarding dosing strategy did not seem to be based on these patient variables. Although there was a difference in the dosing strategy prescribed between loading and titration, with the majority of the loaded group prescribed maximal doses from the outset, the major finding of the present study was that serum levels were not used routinely early in treatment to guide dosing in order to achieve optimal response. It is concerning that only one-third of loaded patients were known to have achieved a therapeutic level by day 7. The low rate of serum levels in the titration group is equally concerning because the treatment recommendation, regardless of dosing strategy, is to achieve levels within a specified range. Despite the finding that maximum daily dose was reached in an average of 5.7 days for the titration group, only one-quarter of patients were known to have a therapeutic level at day 7. This suggests that clinicians were treating bipolar mania without serum levels to guide dosing and assessment of therapeutic response; instead they were using their clinical experience of dosing alone.
The secondary investigation of broad indicators of outcome found no difference in the length of hospitalization, time in intensive care or seclusion between loading and titration. These measures suggested that overall, outcome, with respect to rapid resolution of mania and discharge from hospital, was less than optimal; patients had relatively long hospital admissions (average = 1 month) and spent >1 week in intensive care. In summary, this clinical practice was inconsistent with evidence-based recommendations for either mood stabilizer in order to achieve best clinical outcome.
Cade's pioneering study showed dramatic improvement with lithium loading [6]. This early work was unsupported by serum levels, but in 1976 Stokes et al. showed that higher lithium doses achieved greater improvement in mania, and the rate of clinical improvement was positively correlated with day 7–10 serum levels; mean for the high dose group = 1.06 mmol L−1 [12]. Moscovich et al. reported rapid reduction in psychopathology in nine patients with high-dose lithium loading (2400–4050 mg day−1) [13], and in another open-label pilot study 60% of the 15 patients had a 50% improvement in symptoms within 10 days of starting lithium at 20 mg kg−1 per day. The mean serum concentration after 4 days of treatment was 1.1 mmol L−1 [18].
Valproate loading in acute mania has also been investigated [8], [9], [29]. Hirschfeld et al. reported that valproate loading (30 mg kg−1 per day reducing to 20 mg kg−1 per day on third day) had greater efficacy compared with standard treatment at days 5, 7 and 10 [29]. Another double-blind study of valproate loading (20 mg kg−1 per day) compared to slower titration in mania found that mean serum levels were significantly higher after day 2, and by day 7 the loading group had a significantly greater improvement compared to the titration group [8].
In the present inpatient study where mood stabilizer treatment was used in a non-experimental manner, we expected that clinicians would use serum levels to establish that effective therapeutic levels had been achieved quickly, thereby justifying the assignment of patients to the loading group. We found, however, an inconsistent approach to the use of serum levels: regular and timely checking of serum levels, particularly of valproate, was not part of these clinicians’ routine practice.
The low frequency of serum level monitoring found in the present study is likely to have been a primary contributor to the lack of difference in outcomes found between dosing strategies. Although loading doses of 20–30 mg kg−1 per day are recommended for lithium and valproate, the key to optimal response is the rapid achievement of adequate serum levels; delays in optimizing therapeutic levels result in worse short-term outcome [16]. Effective and safe loading requires that changes to doses (either upwards or downwards) are made as early as day 3 but certainly by days 5 and 7. The low rates of recorded serum levels reflect a failure to follow recommended practice. It is likely to have resulted in delayed adjustments to dose to achieve desired therapeutic levels, especially in the valproate group.
Although it was not the primary focus of the present study, difference in outcome between loading and titration had been expected. Both groups, however, had similarly suboptimal outcomes. A number of factors may have contributed to this lack of difference between dosing strategies. First, the relatively rapid rate of dose escalation in the titration group meant that it was possible that some of this group may have met the serum level definition of loading if serum levels had in fact been recorded. Second, the one factor associated with hospital LOS and time in ICU was ethnicity; the duration of both of these variables was increased for NZ Māori. Although statistically there was no difference in ethnic distribution between the two treatment groups, almost double the proportion of NZ Māori were in the loaded group and this may have been due to small sample size rather than a lack of difference per se. Therefore variations in management due to ethnicity may have skewed the outcome indicators. The overall high rate of antipsychotic and/or benzodiazepines used adjunctively in the first 72 h in both treatment groups (98% of admissions) is a third factor that may have obscured any differences between the two dosing strategies, especially the two acute measures; time spent in intensive care and seclusion.
Adverse effects were more common with lithium, and in particular for those loaded with lithium (63%). Most of the adverse effects reported were to be expected from lithium's pharmacological profile. Keck et al. found that a similar proportion of patients (60%) loaded with lithium reported adverse effects [18]. Loading dose studies with valproate have generally reported good tolerability, low incidence of side-effects and no significant differences between loading and titrating strategies [7], [8], [29]. The lithium used in this hospital was most commonly the standard-release formulation (primarily because of cost) and it is possible that the rate of absorption and therefore peak concentration may explain some of the adverse effects reported with lithium. Loading strategies with twice-daily lithium dosing of a slow-release formulation may be less likely to cause adverse effects such as nausea, vomiting, diarrhoea and tremor. Therefore, a logical recommendation arising from the study is that lithium loading should be prescribed as twice daily with slow-release tablets to increase tolerability.
The inclusion of a retrospective analysis of indirect outcome measures in a clinical practice audit confers a number of limitations. Small sample size, use of case notes and use of indirect measures of acuity and response (such as discharge from hospital) rather than standard measures of illness severity and symptom improvement may have contributed to the lack of difference found between loading and titration of mood stabilizers. With an average hospital LOS of 1 month, this may have been an insensitive indicator of outcome, related less to individual clinical need and more to other service factors. Furthermore, differences between loading and titrating would likely occur early in treatment, especially the first week, and would be attenuated over the long admission time. Because the present study was undertaken primarily as an audit of practice it was not designed with the power to detect a difference between loading and titration. Hirschfeld et al. had estimated that a clinical trial of valproate required 105 patients in each dosing group using direct measures of mania [29], more than double the number of admissions included in the present study.
Other clinician and/or patient factors besides those examined in the study may have influenced the clinical decision to load the mood stabilizer and thereby affected outcome. The variable and inconsistent use of serum levels, irrespective of dosing strategy, may indicate that testing was stimulated by non-response. Conversely, lack of serum levels especially in the first week may have resulted in suboptimal treatment, particularly with valproate. Finally, the absence of serum levels meant that the assumption that prescribed medication was administered and taken as directed could not be validated.
Despite these limitations, this audit of clinical practice highlights an important finding: improving clinical outcome for patients with bipolar mania requires regular and timely measurement of mood stabilizer serum levels. The fact that this naturalistic study failed to demonstrate better outcomes with mood stabilizer loading does not mean that loading is not an effective strategy. Rather it emphasizes that because dosage does not in itself predict a greater likelihood of a positive response, measurement of serum levels is essential because the link is between rapidly attained high serum levels and positive outcomes. Furthermore, regular serum levels inform better clinical decision-making, which should speed up response times. Clinicians who use loading dose strategies in particular, must regularly measure serum levels to ensure that loading has actually occurred, and monitor for adverse effects. These findings present an important lesson for clinicians already established in routine practice and at a trainee level.
Footnotes
Acknowledgements
The authors would like to thank the Oakley Mental Health Research Foundation for financial assistance; final-year undergraduate Pharmacy students Michelle Plant and Nadine Burjony for collecting the data; and Mental Health Services staff at Waitemata District Health Board for their support.