
Abstract
Keywords
Studies on treatment-seeking populations and population surveys have found that up to 60% of people with schizophrenia abuse a number of psychoactive substances [1], [2]. Cannabis is probably the illicit substance most often consumed by such ‘dually diagnosed’ patients [3] and the research literature contains consistent evidence that cannabis consumption is a risk factor for psychotic symptoms [4] and that continued use is associated with a worse course of schizophrenia spectrum disorders [5–8]. One explanation for the high rate of substance use in patients with schizophrenia is the self-medication hypothesis (SMH) [9], [10]. This posits that substance use is a consequence of an individual's attempts to alleviate distressing emotional states. Schneier and Siris first adopted and discussed the SMH with regard to schizophrenia [11]. They found that patients with schizophrenia preferentially used psychotogenic substances such as cannabis in a counterintuitive way, intending to alleviate mental distress but worsening it in the longer run.
From prospective studies on the relationship between cannabis use and the onset of psychosis there is not much support for the SMH. A recent meta-analytic study of seven longitudinal cohort- and population-based studies concluded, after having controlled for various other aetiologies. that cannabis use was associated with subsequent risk of psychotic symptoms than vice versa (i.e. that a person with psychotic symptoms has a greater risk of using cannabis in later life) [12]. Prospective studies that directly examined the SMH found, with the exception of one study [13], that early psychotic symptoms were not associated with an increased risk of cannabis use in later life [14], [15].
Another way to evaluate the SMH is to assess reasons for substance use in patients with schizophrenia. The evidence from such studies, however, is ambiguous. Noordsy et al. found that a small minority of patients with schizophrenia stated that alcohol use relieved specific positive symptoms, whereas a similar proportion described a worsening [16]. Dixon et al. reported that some patients with schizophrenia used substances to reduce hallucinations and suspiciousness, whereas in a larger minority substances increased positive symptoms, with cannabis and cocaine being those most often related to an increase [3]. Addington and Duchak found that the most commonly reported reasons for alcohol and cannabis use in stable schizophrenia outpatients were to relax, to increase pleasure, to get high, and to reduce depression. A worsening of positive symptoms, however, after the use of cannabis was also reported by more than half of these patients [17].
In contrast, Test et al. found that a majority of patients stated that their paranoia and hallucinations improved with substance use, whereas only a small minority noticed a worsening [18]. Hamera et al. found no associations between daily self-reports of distress caused by schizophrenia symptoms and intake of alcohol, cannabis, and caffeine [19]. Exploratory research on self-regulation of symptoms and drug-induced exacerbation of schizophrenia symptoms found only weak or non-existent relationships, without any consistent pattern [20]. Another study reported a trend for alcohol to be used more often for self-medication purposes than opioids and cannabis [21]. A further study found that the most important motivators of cannabis use in schizophrenia patients were boredom, social motives, sleep disturbances, anxiety, agitation, negative psychotic symptoms, and depression [22]. In the same study, positive symptoms of psychosis and side-effects of antipsychotics were not important motivators of cannabis use.
The mixed findings regarding self-reported reasons for substance use can be attributed to a number of factors. First of all, the investigated samples in previous studies on self-reported reasons for substance use mostly comprised patients with schizophrenia using/abusing a variety of substances. Studies considering only specific substances reported differences between reasons for the use of cannabis and those for alcohol [17], [21], [23], but similarities for cannabis and opioids [21].
Second, most previous studies did not consider a potential influence of different frequencies of substance use on reasons for use and vice versa [3], [17], [20], [21], [23]. One study that distinguished between different frequencies found that patients’ reasons for substance use were also influenced by the amount consumed over the preceding month [24].
Third, it can be argued that reasons for substance use in a population of patients with schizophrenia might differ substantially depending on whether patients were symptomatic or not during their exploration. Thus, an assessment of patients’ schizophrenia symptoms when investigating their reasons for substance use is necessary for comparable results. Previous studies investigating inpatients [3], [23], [25], outpatients [17], [20], [21], or both [22], [24], presumably included patients with different symptom severity.
Fourth, almost all studies on reasons for substance use did not distinguish between different classes of neuroleptics by which patients were treated. This distinction might have been important because one possible explanation of the untoward effects of cannabis on schizophrenia symptoms is that conventional neuroleptics – and especially haloperidol – are particularly disadvantageous for cannabis-using patients with schizophrenia [26], [27]. To our knowledge, the only study that considered different classes reported that fewer patients on atypical antipsychotics than patients treated with traditional neuroleptics stated that alcohol and/or cannabis helped them with overcoming a feeling of being ‘slowed down’ attributed to their medication [17]. Thus, studies on reasons for substance use in traditionally treated patients with schizophrenia who use cannabis might have partially confounded patients’ attempts to counteract side-effects of their medication with attempts to alleviate distressing emotional states more directly related to their disorder. Atypical neuroleptics are associated with a different cluster of side-effects, such as the induction of weight gain and insulin resistance. Such symptoms seem less prone to be positively influenced by cannabis use.
The aim of the present study was therefore to (i) investigate self-reported reasons for cannabis use in patients with schizophrenia treated with atypical neuroleptics and exhibiting a low level of symptoms; and (ii) examine if there are differences between reasons of patients with schizophrenia and those of healthy controls, matched for frequency of cannabis use.
Methods
Sample
The sample consisted of 36 cannabis-using schizophrenia outpatients from the cantons of Zurich and Aargau, Switzerland, treated with atypical neuroleptics (risperidone, n = 5, olanzapine, n = 9, quetiapine, n = 8, amisulpride, n = 5, aripiprazole, n = 2, or clozapine, n = 7). The presence of schizophrenia was ascertained by the patients’ clinical records. Patients with records indicating other diagnoses, especially schizoaffective or affective disorders, and/or any substance use disorder other than cannabis, were excluded. Moreover, patients displaying acute psychotic symptoms or signs of acute cannabis intoxication at the time of assessment were also excluded.
Measures
Patients and controls completed a questionnaire assessing demographic and drug use characteristics, and a 15-item questionnaire assessing reasons for cannabis use (Cronbach's α = 0.78, Table 1). This questionnaire was based on self-reported reasons for substance use, found in other studies [3], [17], [18], [20], [21], [24], [28]. Patients with schizophrenia were further interviewed using the Positive and Negative Syndrome Scale (PANSS) [29] and asked two specific questions: (i) whether they intended to reduce medication side-effects; and (ii) whether they intended to reduce hallucinations when using cannabis.
Reasons for cannabis use.
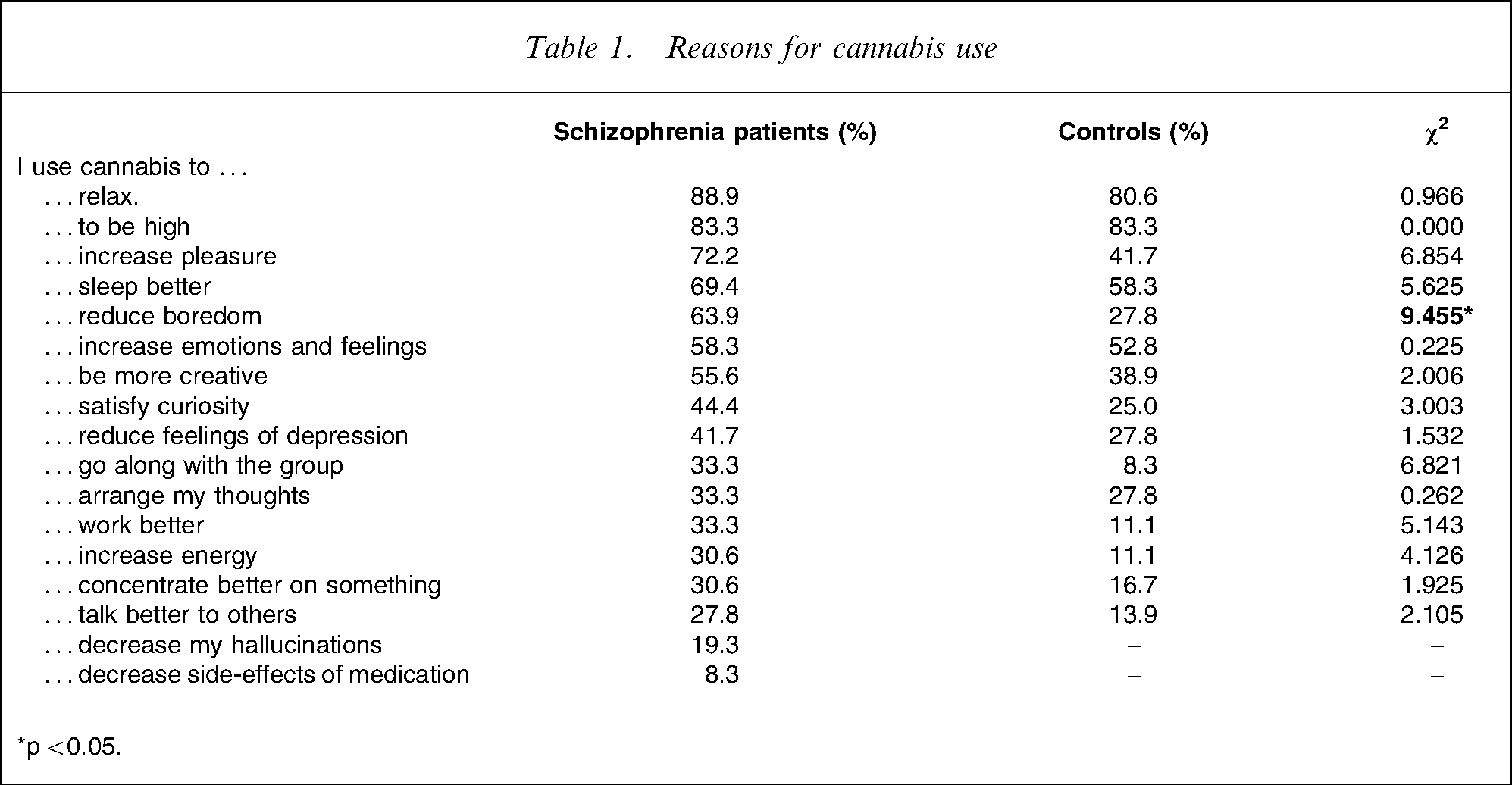
∗p < 0.05.
Procedures
All patients were informed about the present enquiry by their treatment provider, generally a psychiatrist, and were then contacted by an external interviewer and interviewed at their usual outpatient treatment location. By signing the consent form, patients expressed their understanding of the study's purpose and their willingness to participate. The study protocol was approved by the ethics of the canton of Zurich and patients were paid $CHF 30 for their participation.
One hundred and forty-six students who reported using cannabis completed the same questionnaire online. Of these, 36 students with no previous or current psychiatric treatment were matched for gender, age, and frequency of cannabis use (Table 2).
Frequency of cannabis use
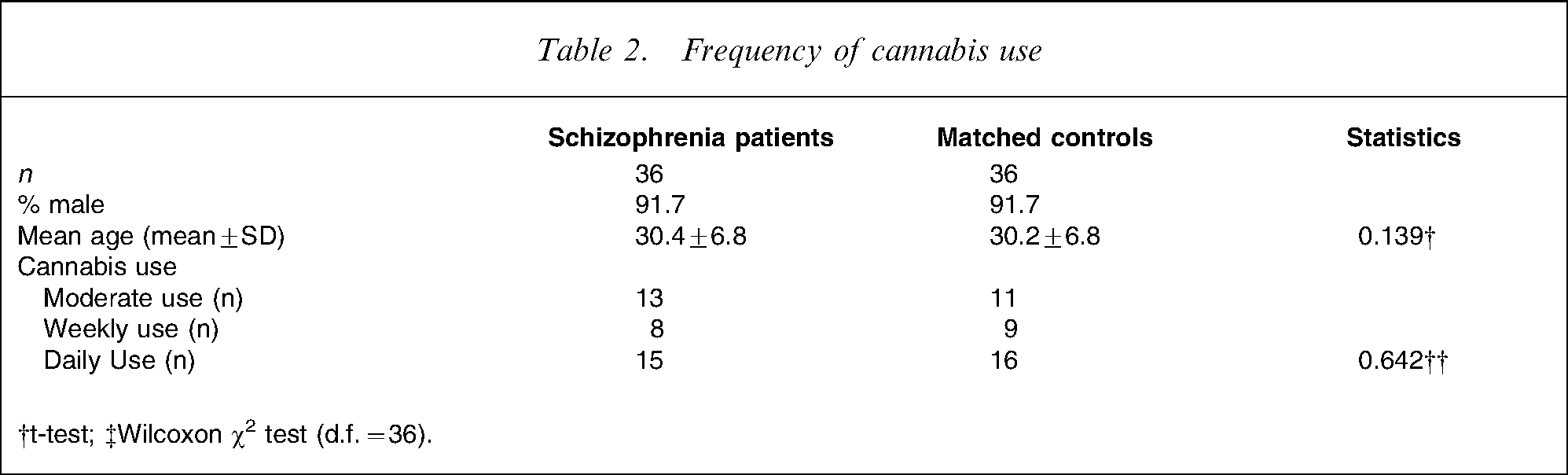
†t-test; ‡Wilcoxon χ2 test (d.f. = 36).
Statistical analyses
Frequencies of reported cannabis use were divided into three categories: moderate (once used–weekly use), weekly (weekly–daily use) and daily (daily use). Differences in reasons for use between patients with schizophrenia and matched controls were analysed by comparing the numbers of yes answers using the t-test for dependent samples overall, and for the frequency of cannabis use categories using the Wilcoxon χ2 test. At the single-item level, differences between patients and controls were analysed using χ2 tests with Bonferroni corrections for multiple comparisons. The PANSS was evaluated according to Kay et al. [29] for the positive, negative and general schizophrenia symptom scales. Two-tailed level of significance was set at p < 0.05. All statistical analyses were performed using SPSS version 15 (SPSS, Chicago, IL, USA).
Results
Evaluation of PANSS results confirmed that subjects with schizophrenia were stable outpatients. The mean positive symptom score was 15.4 (SD = 5.0), the mean negative symptom score was 14.9 (SD = 5.5) and the general symptom score was 32.0 (SD = 7.0). Patients did not differ on the PANSS with regard to the three categories reflecting different frequencies of cannabis use (positive scale: χ2 (2)=0.478, n.s., negative scale: χ2 (2)=1.536, n.s., general scale: χ2 (2)=1.263, n.s.). Overall, cannabis-using patients with schizophrenia treated with atypical neuroleptics more often agreed with the proposed reasons for use than controls (mean for patients with schizophrenia: 7.67, SD = 3.53, mean for students: 5.08, SD = 2.82, t(1)=2.163, p < 0.05). The same was true for the moderate use category (χ2 (1)= − 2.229, p < 0.05) but not for the weekly use (χ2 (1)= − 1.268, n.s.) and the daily use categories (χ2 (1)= − 1.578, n.s.). At the individual-item level, patients (all frequency categories) differed from controls (all frequency categories) regarding the reason ‘reduce boredom’ (χ2 (1)=9.455, p < 0.05, Table 1). Only 8.3% of patients agreed with the statement ‘I use cannabis to reduce side-effects of medication’ but 19.3% agreed with the sentence ‘I use cannabis to reduce my hallucinations’.
Discussion
The main result of the present study was that patients with schizophrenia treated with atypical neuroleptics – apart from more often answering yes to almost every proposed reason – differed only marginally from healthy controls regarding every single reason for cannabis use.
The small sample size in the present study might have prevented us from finding more significant differences between patients and controls. This might especially be the case for the items ‘increase pleasure’ and ‘go along with the group’ (χ2>6.5). A tendency to be more suggestible is well known for patients with schizophrenia and might therefore be the cause for more frequent yes answers [30], [31].
The only reason that was put forward more often by patients than by controls was that they intended to use cannabis to ‘reduce boredom’. Furthermore, the explorative analysis found that the subgroup of patients who consumed cannabis daily, more often stated that they used cannabis to increase pleasure and to go along with the group. These differences (reduce boredom, go along with the group, increase pleasure) might point to a feeling of social marginalization experienced by patients with schizophrenia. Interestingly, the reason ‘consuming alcohol and/or illicit substances with the intention to reduce boredom’ has rarely been explored in previous studies [3], [17], [18], [20], [21] and those few studies addressing it investigated samples with a mixture of different substances and different categories of use/abuse [22–24]. The present results are comparable to those of the Schofield et al. study that investigated reasons for cannabis use in a sample of individuals with psychotic disorders, predominantly in outpatient treatment and assumingly mainly treated with atypical neuroleptics [22]. Their most common reasons for cannabis use were to reduce boredom (86%) and ‘to do something with friends’ (81%). In our opinion, the aforementioned reasons (e.g. to reduce boredom) might instead point to an unsatisfactory situation regarding leisure time, to underemployment, difficulties with partnership, or related factors than to a need to alleviate mental distress as hypothesized in the SMH [3], [16], [18], [23], [24].
Reasons that would reflect more clearly an effort to become more functional (consuming cannabis to ‘sleep better’, to ‘work better’, or to ‘increase energy’) were not reported more frequently. The same was true for reasons that might have represented an intention to counteract deficits in cognitive processing (‘concentrate better on something’ and ‘arrange my thoughts’).
Only a small percentage (8.3%) of patients stated that side-effects of their medication were reduced when they used cannabis. We therefore assume that there was only little contribution of medication side-effects to patients’ reasons for cannabis use. Interestingly, 19.3% of patients with schizophrenia stated that they used cannabis to reduce hallucinations, which is counterintuitive. But analogous findings have also been reported by Addington and Duchak (n = 21, 40%) [17], by Goswami et al. (n = 5, 40%) [21], and by Schofield et al. (n = 101, 11%) [22]. Therefore, these findings point to the existence of a subgroup of patients with schizophrenia who respond favourably to cannabis or might even profit in some way from its use.
In summary, reducing boredom and improving social interaction were the most important reasons for patients with schizophrenia to use cannabis. Treatment of circumstances associated with social marginalization might reduce patients’ tendency to use cannabis, and thus might reduce relapse to psychosis.
There are several limitations to the generalizability of the present findings: We relied on self-declaration when assessing frequency of cannabis and other drug use and did not apply a standardized scale. The control group of psychology students did not only systematically differ from patients regarding mental health but also with respect to their educational background. Furthermore, we did not screen the controls for the presence of psychosis. The administration of a Likert scale in place of yes/no answers would have increased the variability and possibly increased the likelihood of more significant differences. Finally, cannabis use is widespread in Switzerland and legal sanctions are rare [32]. Thus, the present findings might not pertain to countries with a less liberal policy towards cannabis use.
Footnotes
Acknowledgements
This study was supported by Grant No. 02.001033 from the Swiss Federal Office of Public Health.