
Abstract
The onset of most mental disorders tends to occur in adolescence and young adulthood [1], but many young people fail to seek help or delay seeking help. Delays in treatment are associated with poorer outcomes [2]. The most frequently reported reasons for delayed help-seeking have been lack of recognition that the problem is a mental disorder and poor knowledge about appropriate forms of help [3]. The term ‘mental health literacy’ has been used to describe knowledge and skills that aid the recognition, management and prevention of mental disorders [4]. Studies in this field have found that, among young people, lack of knowledge is common, with recognition rates of approximately 50% for depression [5, 6] and 25% for psychosis [5].
In regard to the specifics of recognition, accurate labelling of mental disorders (depression or psychosis) by young people has been found to be strongly associated with an appropriate choice of help and treatment, even after adjusting for other predictors such as age, gender, exposure to someone else with the illness and exposure to awareness campaigns [7]. Indeed, labelling a problem as a specific mental health problem has been found to be a key factor in reducing time to help-seeking [8], and detection of a mental disorder is greater if the patient explicitly raises the problem with their family doctor/general practitioner (GP) [9, 10]. So, although labelling is a very specific component of mental health literacy, it is likely to be a central one. It may trigger a schema of health beliefs that can point a person in the right direction for help and treatment, and increase the likelihood of detection by health-care professionals.
Although it is known that elements of mental health literacy vary with age among both young people [5] and adults [11], what is not known is how labelling develops with age during adolescence and young adulthood. In particular, we do not know how various types of labelling change with age and the factors associated with these developmental trends. Gender differences in labelling have similarly not been investigated developmentally. Female subjects tend to show more accurate labelling than male [11–13], but it is not known when this gender difference begins to appear or what factors produce it. Indeed, despite the mounting literature examining the benefits of labelling for help-seeking [7, 8] and potential harm of labelling in relation to stigma [14, 15], no-one to date has examined how labelling emerges and evolves in adolescence and young adulthood and what factors might mediate this development. This is a period of life in which there will be increasing exposure to mental disorders in both self and peers, but there is also a great deal of cognitive maturation and academic learning occurring that can affect labelling.
There are a number of factors previously found to be associated with labelling that may mediate any age and gender effects. These factors include exposure to mental illness through personal experience or through family members or friends [7, 14, 16, 17] and, to some extent, education [12]. Factors found to be associated with other aspects of mental health literacy (e.g. knowledge of effective help-seeking) are also potential mediators. These include language spoken at home and exposure to community awareness strategies [7]. More recently, the influence of parental knowledge and attitudes on young people's mental health literacy has been reported [18, 19], but to date has not been investigated in the area of labelling.
It is possible that the development of labelling may differ between disorders. Studies of labelling to date have focused primarily on depression and psychotic disorders [7, 14, 16]. The investigation of other disorders would broaden the generalizability of the findings. Anxiety disorders are particularly relevant in this regard, given their high prevalence and typical first onset in this age group [1, 20].
The aims of the present study were therefore to (i) describe the most common terms used by young people to label depression, psychosis and an anxiety disorder (social phobia); (ii) determine whether labelling changes with age and whether this change differs according to gender; and (iii) examine factors that may be mediating any developmental changes; these include exposure to mental disorders in self or others, mental health campaign exposure, level of education, parental use of labels and language spoken at home.
Method
Sample
A computer-assisted survey of 3746 Australians aged 12–25 years was conducted during June–August 2006. The sample was contacted using random-digit dialling to cover all of Australia. If the young person lived with a parent who was able to understand and communicate in English, then one parent was also invited to be interviewed. The response rate was 61.5% for the young people and 68.5% for co-resident parents, Further details of the sample are reported elsewhere [21, 22].
Interview
The interview was based on a vignette of a young person with a mental disorder [21]. On a random basis, respondents were read one of four vignettes: depression, depression with alcohol misuse, social phobia, and psychosis. The vignettes were written to satisfy DSM-IV criteria. Respondents were read a vignette of the same gender and age group as their own [21]. Respondents aged 12–17 years were read a version of the vignette describing a 15-year-old, and 18–25-year-olds were read a version portraying a 21-year-old. Parents interviewed were read the same vignette as their child.
After being presented with the vignette, respondents were asked a series of questions to assess a number of areas, including their recognition/labelling of the disorder in the vignette; what they would do to seek help if they had the problem; beliefs about interventions, stigmatizing attitudes and social distance; the six-item version of the Kessler Psychological Distress Scale; exposure to mental disorders and media campaigns about mental health; and sociodemographic characteristics. Parents were asked a subset of the same questions as their child, with changes in wording to reflect the parent's perspective.
The present paper focuses on responses to the depression, psychosis and social phobia vignettes only, because each of these represent a single diagnostic group. The paper presents data on the recognition, exposure and sociodemographic questions, so these are described in detail here. Description of the vignette was followed by an open-ended question asking ‘What, if anything, do you think is wrong with John (male version)/Jenny (female version)?’, for which unprompted responses were recorded. Interviewers recorded responses according to pre-coded response categories (depression, schizophrenia, psychosis, mental illness, stress, nervous breakdown, psychological/ mental emotional problem, has a problem, cancer, nothing, don't know) derived from a content analysis of responses to the same questions in earlier surveys [4, 5]. A content analysis of responses that did not fit these pre-coded categories led to post-coding of 56 other categories. Many of these responses were used to describe the social phobia vignette, which had not been used in surveys previously. For simplicity, the post-coded response categories that were among the four most common and the most accurate responses for each vignette are described here, because these are the focus of analysis in this paper. They include anxiety/anxious, anxiety disorder, drugs, eating disorder (anorexia, bulimia, eating disorder), low self-confidence/low self-esteem, physical problem (glandular fever, chronic fatigue syndrome, diabetes), shy, social anxiety/ social phobia. A series of questions was asked to ascertain personal exposure to mental disorders. Respondents were asked: ‘Has anyone in your family or close circle of friends ever had a problem similar to John's/Jenny's?’, ‘Have they received professional help or treatment for these problems?’, and ‘Have you ever had a problem similar to John's/Jenny's?’, ‘Have you received any professional help or treatment for these problems?’. In regard to exposure to media campaigns about mental health, respondents were asked ‘Have you seen, read or heard any advertisements about mental health problems in the past 12 months?’, ‘In the past 12 months, have you received any information about mental health problems from your teachers (12–17-year-olds)/workplace/TAFE (Technical College)/University (18–25-year-olds)?’, and ‘Have you heard of beyondblue: the national depression initiative?’. All exposure questions coded the responses as either ‘yes’, ‘no’, ‘don't know’ or ‘refused’. Finally, respondents were asked a range of sociodemographic questions to ascertain their age, gender, language spoken at home and, for parent respondents, their highest level of education.
Given the previously reported associations of labelling with age, gender, education, language spoken at home, exposure to mental disorders and exposure to mental health campaigns, these factors were selected for inclusion as possible predictors of label use. Parental education level was used as a proxy measure of the young person's exposure to an educationally stimulating environment.
Ethics
Ethics approval was obtained from The University of Melbourne Human Research and Ethics Committee.
Validation of the vignettes
Psychiatrist diagnoses of vignettes (coded by DSM-IV chapters)
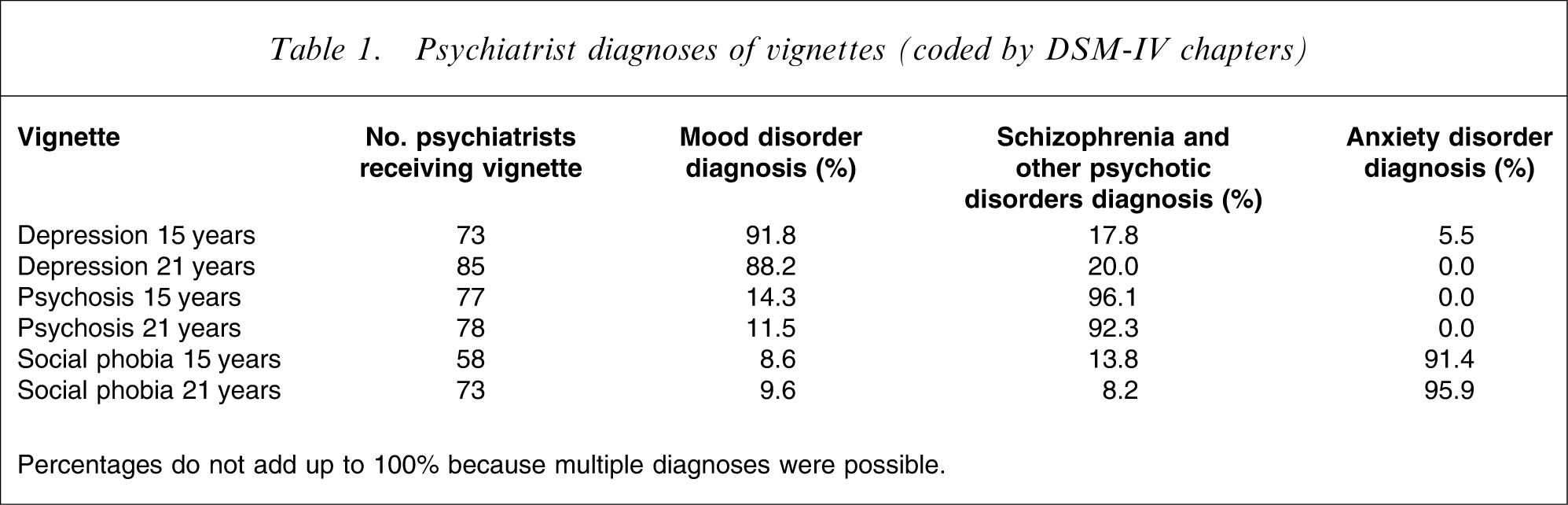
Percentages do not add up to 100% because multiple diagnoses were possible.
Psychologist diagnoses of vignettes (coded by DSM-IV chapters)
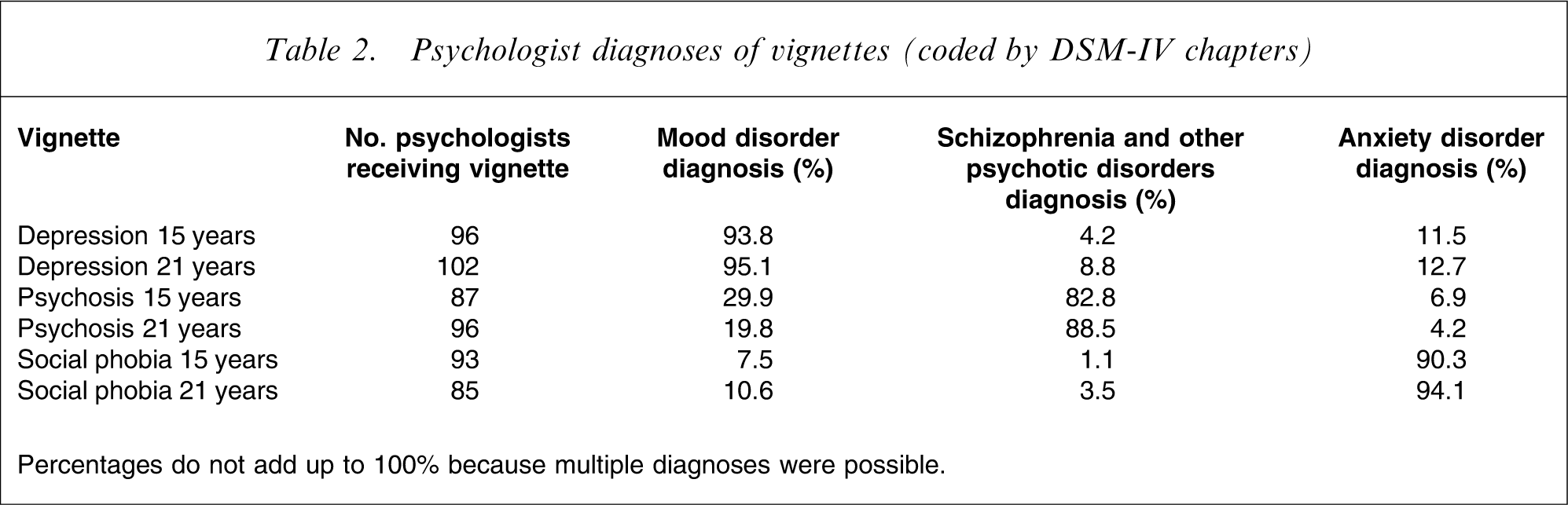
Percentages do not add up to 100% because multiple diagnoses were possible.
Data analysis
Age and gender differences in labelling were analysed using per cent frequencies to determine the rate of accurate labelling, as well as the rate of all other labels commonly used by young people to describe each of the three vignettes. Accurate labelling was defined as those labels that approximated the DSM-IV diagnostic label [26] upon which the vignettes were based and validated [23–25].
Following this descriptive analysis, multiple binary logistic regression analyses were used to examine predictors of the labelling outcome variables identified here (most accurate and most common) for each vignette. The predictors covered sociodemographic factors (age, gender, language spoken at home) and exposure factors (exposure to mental disorders and help-seeking, campaign exposure). All the predictor variables were dichotomous, except for age (12–25 years), which was analysed as a continuous variable.
For the subsample of young people who also had one of their parents respond, an additional set of multiple binary logistic regression analyses was conducted to examine the influence of parent characteristics (parent education level and label used by parent) on the child's use of labels. The aim was to determine whether parent education level and parent label use were associated with young people's label use in this subsample. ‘Parent education level’ was dichotomized according to ‘degree/diploma or higher’ versus ‘other’; and ‘label used by parent’ used the same list of the most accurate and four most common labels identified by the young people for each vignette.
Results
Labels used by young people to describe the vignettes
Overall, 929 young people received the depression vignette, 968 received the psychosis vignette and 905 received the social phobia vignette. For the depression vignette, 69.1% (n = 642) of respondents used the accurate label of ‘depression’ and this was also the most frequent response, followed by ‘stress’ (6.7%, n = 62), ‘drugs’ (5.0%, n = 46), ‘eating disorder’ (4.8%, n = 45) and ‘physical problem’ (4.8%, n = 45). For the psychosis vignette, 33.4% (n = 324) accurately labelled this as ‘schizophrenia’ or ‘psychosis’ and this was the most frequent response, followed by ‘depression’ (24.8%, n = 240), ‘mental illness’ (18.5%, n = 179), ‘psychological/mental/emotional problems’ (8.3%, n = 80) and ‘paranoia/paranoid’ (2.9%, n = 28). For the social phobia vignette, only 5.0% (n = 45) correctly labelled it as either ‘social anxiety’, ‘social phobia’ or ‘anxiety disorder’. The most common label used to describe this vignette was ‘low self-confidence/self-esteem’ (22.7%, n = 205), followed by ‘shy’ (20.4%, n = 185), ‘depression’ (13.4%, n = 121) and ‘anxiety/anxious’ (10.3%, n = 93).
Variation in label use according to age and gender
Correct label use steadily increased with age for all three vignettes (Figure 1), with female subjects generally using accurate labels more frequently across all age groups and vignettes, apart from the psychosis vignette, for which male subjects used the accurate label more frequently for the 12–13 year age group and the 22–23 year age group. The use of the terms ‘depression’ and ‘anxiety’ to describe the social phobia vignette also increased with age, the latter more so for female subjects. Describing the depression vignette with the term ‘physical problem’ and, to a lesser extent, ‘drugs’ also showed some increase with age, particularly by male subjects. For the depression vignette, the label ‘eating disorder’ was far more frequently used by female subjects and this tended to decrease with age. The only other clear decrease in use of a label with age was the term ‘shy’, used to describe the social phobia vignette, and overall this term was more frequently used by male subjects.
Frequency of use of accurate and common labels to describe the vignettes according to age (2 year groups) and gender.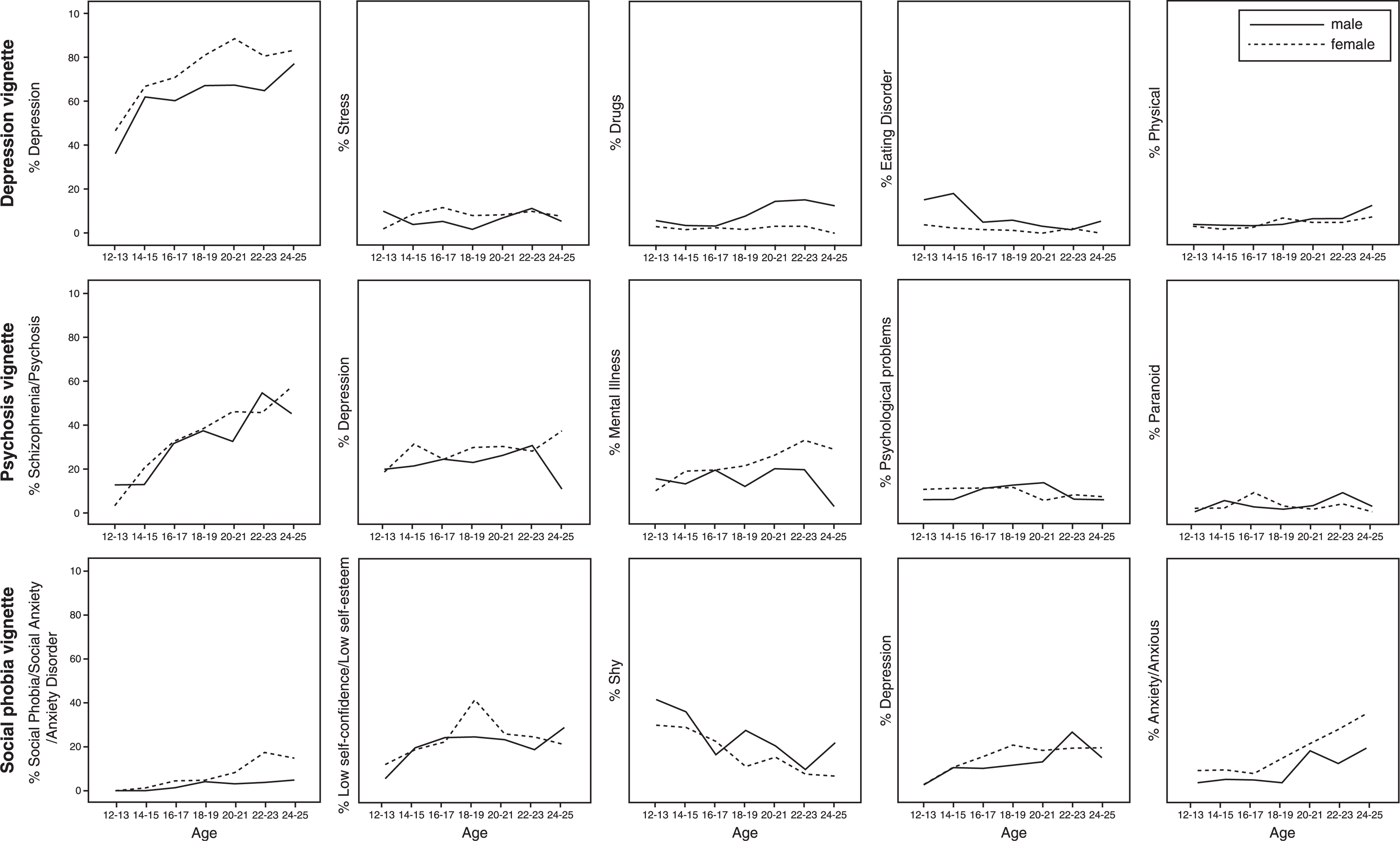
Variation in exposure to mental disorders and campaigns according to age and gender
For the whole sample of young people, personal experience of a mental disorder and having sought help (Figure 2a) and exposure to a family member or friend who had experienced a mental disorder and sought help (Figure 2b) steadily increased with age. Exposure to mental health advertising (Figure 2c) and exposure to the national depression initiative beyondblue campaign (Figure 2d) increased with age up to 16–18 years then tended to plateau. Exposure to mental health information at school, university or workplace peaked at 15 and steadily declined with age (Figure 2e). Exposure to all life experience and environmental factors followed a similar gradient for both genders, but male subjects’ exposure was almost always less than that of female subjects’.
Frequency of exposure to mental disorders and types of mental health campaigns according to age (2 year groups) and gender.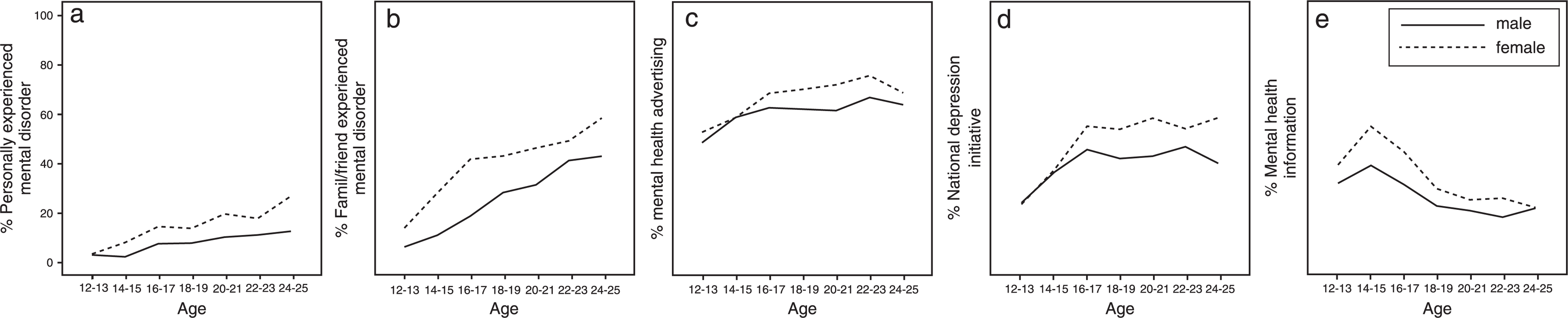
Factors associated with correct label use
Predictors of accurate and most common labels for the depression vignette by youth
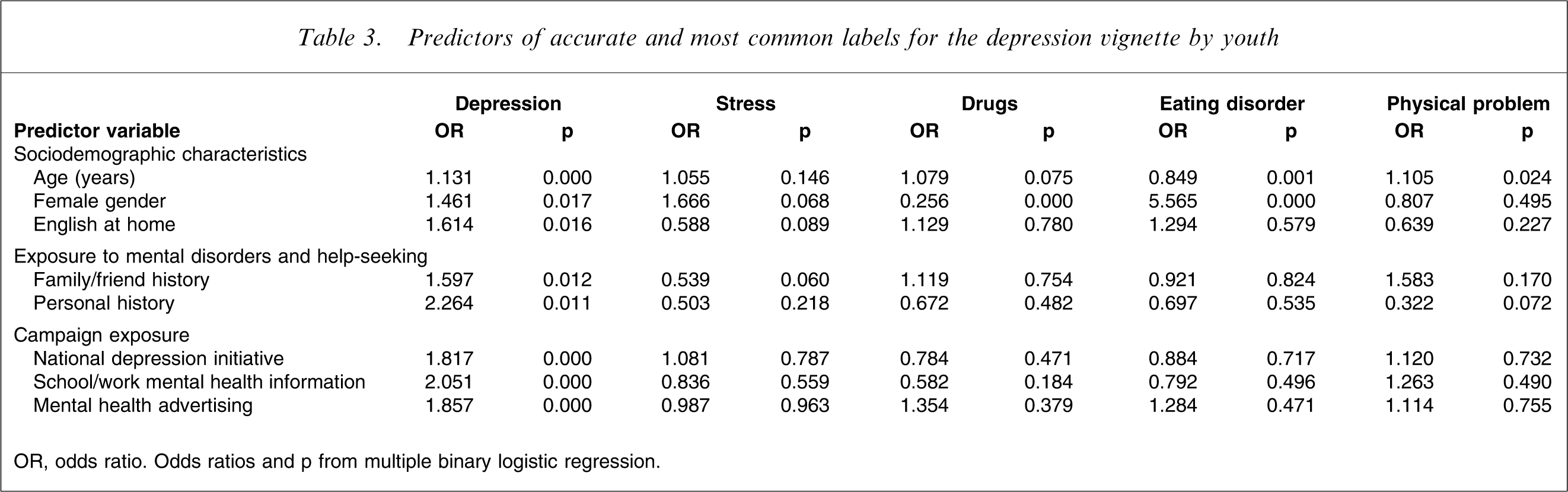
OR, odds ratio. Odds ratios and p from multiple binary logistic regression.
Predictors of accurate and most common labels for the psychosis vignette by youth
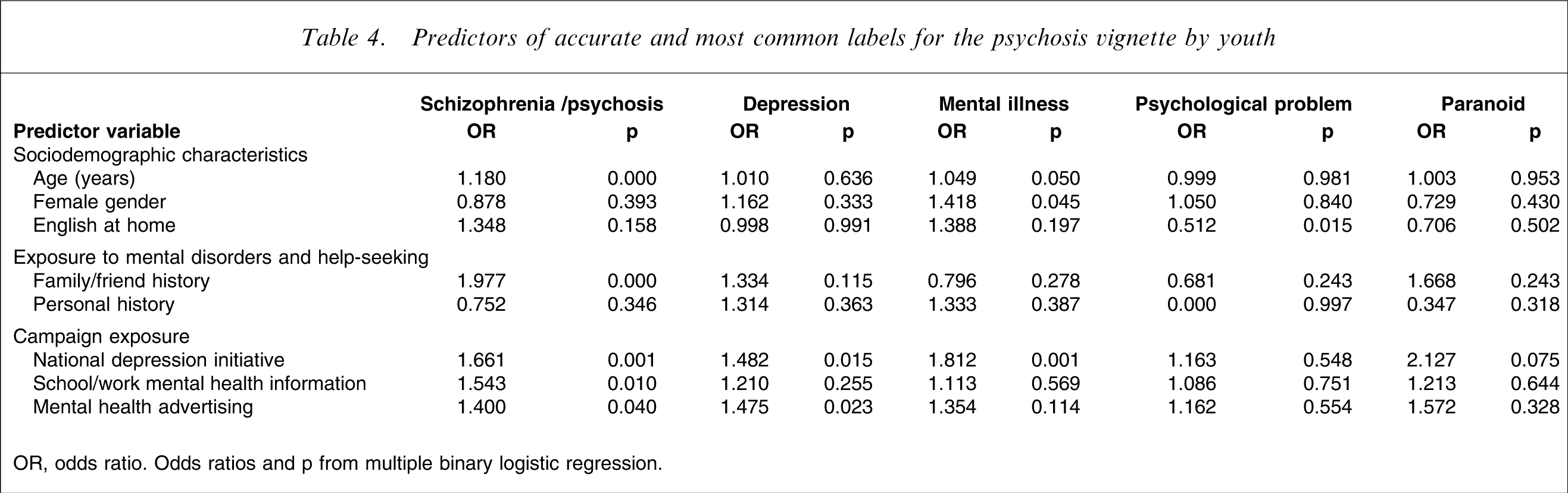
OR, odds ratio. Odds ratios and p from multiple binary logistic regression.
Predictors of accurate and most common labels for the social phobia vignette by youth
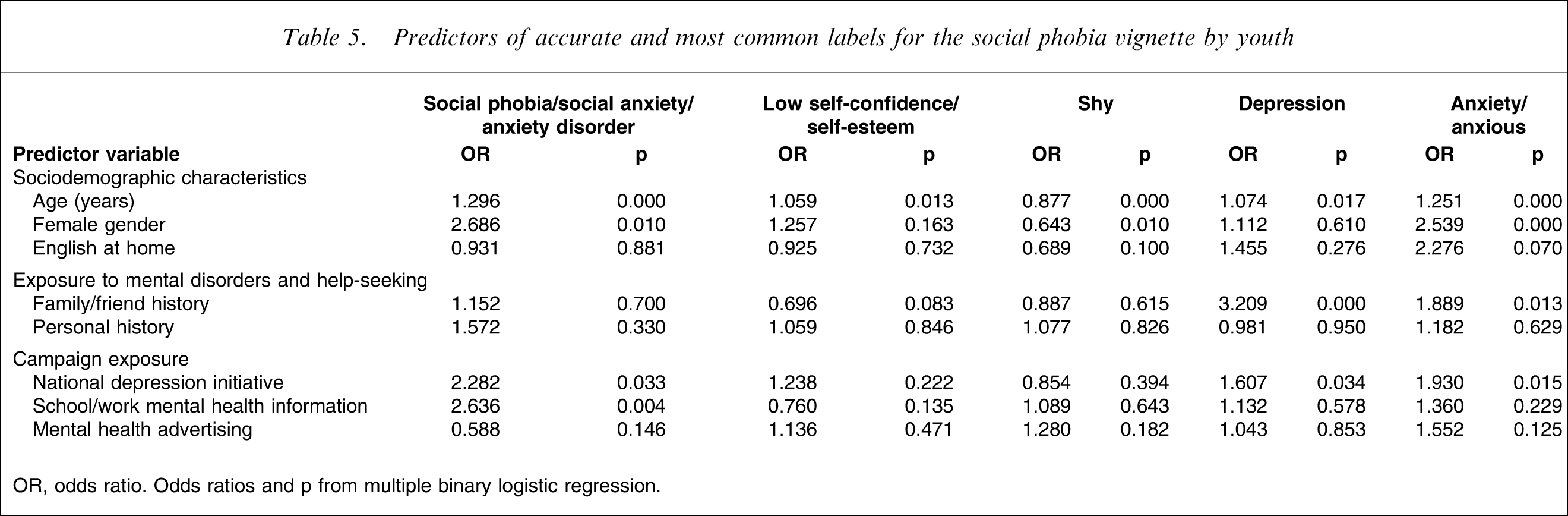
OR, odds ratio. Odds ratios and p from multiple binary logistic regression.
Factors associated with other labels
For the depression vignette, the label ‘drugs’ was associated with male gender and the label ‘eating disorder’ was associated with younger age and female gender. For the psychosis vignette, the label ‘mental illness’ was associated with older age and female gender, while use of the label ‘depression’ was associated with exposure to the national depression initiative and mental health advertising. The use of all labels for the social phobia vignette tended to increase with age, except for the label ‘shy’, which tended to be associated with younger age and male gender. Female gender was associated with the anxiety and depression cluster labels for the social phobia vignette, and exposure to a family member or friend with social phobia symptoms was associated with the use of labels ‘depression’ and ‘anxiety’.
After age, the most common predictor of label use for all vignettes was exposure to the national depression initiative beyondblue campaign. Furthermore, this exposure was always associated with accurate or approximate labels for example ‘depression’ and ‘mental illness’ for psychosis and ‘depression’ or ‘anxiety’ for social phobia.
Associations with labelling by parents
For the subsample of young people with an associated parent respondent, correct label use by the young person was associated with accuracy of parent label for all three vignettes (depression, odds ratio (OR) = 1.721, p = 0.029; psychosis, OR = 2.192, p = 0.001; social phobia, OR = 10.865, p = 0.011). For the depression vignette, the use of the label ‘eating disorder’ was associated with the parent labels ‘depression’ (OR = 4.272, p = 0.008) and ‘eating disorder’ (OR = 3.414, p = 0.026), and the use of the label ‘physical problem’ was associated with the parent label ‘eating disorder’ (OR = 7.877, p = 0.009). For the social phobia vignette, the use of the label ‘anxiety/anxious’ by the young person was associated with the parent label ‘social anxiety/social phobia/anxiety disorder’ (OR = 4.481, p = 0.007). Parent education level was not associated with any of the most accurate or most common labels used to describe the vignettes.
Discussion
Accuracy of labelling by young people varies greatly between disorders. A consistent finding across disorders, however, is that more predictors were found for use of accurate labels compared to almost all other non-diagnostic labels.
Accurate labels tend to be the most frequently used labels by young people to describe depression and psychosis, although many other psychiatric and lay terms are also used. Depression was correctly labelled twice as frequently as psychosis. This difference is consistent with previous findings for young people, as well as for adults [5, 6, 27]. The other two most common labels used for psychosis, however, ‘depression’ and ‘mental illness’, although either inaccurate or non-specific, reflect a belief that it is a serious problem. When the percentages using these other labels are taken into account, labelling of some form of serious disorder is comparable between depression and psychosis. Conversely, social phobia is most commonly labelled using lay terms rather than conventional psychiatric labels. This is the first study to report findings on the labelling of social phobia. Despite it being one of the most common disorders in this age group [20], it is clearly poorly identified and the labels used suggest that its seriousness may often be minimized.
Use of accurate labels increased with age, and female subjects were more likely to use them, which is consistent with previous findings [13]. Female gender was a predictor of accurate label use for depression and social phobia, which may be a result of the higher prevalence of these disorders among female subjects [20]. Likelihood of using an accurate label was also associated with exposure to the mental health community awareness strategies of the national depression initiative, and mental health information received through education or work settings. It is important to note that part of the national depression initiative involved interventions based in educational and workplace settings, so the two sorts of exposure are not independent [28]. Accurate labelling of depression and psychosis was associated with exposure to family or a friend with the disorder, which may be due to higher treated prevalence of these disorders compared to social phobia [20, 29]. Language spoken at home was not found to be associated with any form of labelling, confirming findings by Klimidis et al. [17]. Given that age is associated with increased exposure to mental illness in self or others and to mental health campaigns, these exposures are potential mediators of age differences in labelling. These factors, however, do not fully account for the age differences in labelling because they remained after adjusting for exposure differences.
Parents also play a role in the development of labelling. It appears that the accuracy of the label used by parents to describe a mental disorder is more important than the child's general exposure to vocabulary through having better educated parents. This finding strengthens understanding of the important role that parents play in young people's mental health literacy, as highlighted in previous studies [18, 19].
Inaccurate labelling is also important to consider because, as Klimidis et al. have suggested, use of lay terms may lead a person to think of the problem as within the bounds of normal and hence not seek care [17]. Young male subjects are at particular risk of inaccurate labelling that may prevent effective help seeking. Not only was male gender less frequently associated with accurate label use, it was more frequently associated with inaccurate label use, such as ‘drugs’ for depression or ‘shy’ for social phobia. This finding indicates that young male subjects need more targeted efforts to improve their capacity to label disorders.
As well as involving the use of lay labels, mislabelling can also take the form of labelling a disorder as another disorder. Although this type of mislabelling may still lead a person to help seeking, the type of help sought may not be optimal. For example, the use of the label ‘depression’ to describe psychosis may be problematic, because earlier findings suggest that it is less frequently associated with effective help-seeking compared to a correct label [7]. Another example of this is that female subjects were five times more likely to mislabel the depression vignette as an eating disorder, which has unknown implications for help-seeking pathways.
It is apparent that different disorders have different patterns of labelling. Although depression is well labelled, some of the more common labels, such as ‘stress’ and ‘drugs’, indicate that it is easily minimized. Psychosis appropriately attracts more serious labels, whereas social phobia is generally minimized. It is also apparent that the national depression initiative has had general effects that are associated with mislabelling of many disorders as ‘depression’. This effect may be occurring because there have not been community awareness initiatives sufficiently targeting other disorders. This finding may suggest, as highlighted by others previously [12, 30], that different disorders require differing approaches to the improvement of labelling. The need to improve labelling of social phobia is particularly pressing so that its impact is not minimized.
Many factors found here to be associated with accurate labelling are modifiable. They could be modified through population mental health initiatives, whether it be through increasing exposure to community awareness campaigns, exposing young people to people who have actually experienced the disorder through school presentations and the like, or through enhancing parent mental health literacy.
The present findings highlight the breadth of common labels used by young people and this is the first study of its kind to examine how labelling of mental disorders evolves during adolescence and young adulthood and how this varies between genders. An understanding of the development of labelling can assist the population health practitioner to be aware of current language used to describe disorders to aid effective communication in community awareness strategies. (For example, emphasizing that social phobia is more than just shyness and that depression is more then just stress.)
The present study has a number of strengths, including the large nationally representative sample, the coverage of the age range in which mental disorders often have first onset, the inclusion of parents, and the validation of the vignette labels using a substantial sample of mental health professionals. Another strength was that the focus of the survey on mental health was not mentioned until much later in the survey, reducing the potential for biases in the labels given. The findings, however, must also be considered in light of some of the study's limitations. Labelling of a problem as described in a vignette, although convenient as a means of measuring mental health literacy, may not truly reflect the actual experience of conceptualizing a problem in real life, whether it be in oneself or others. Furthermore, some of the disorders involve cognitive impairments, which may affect the ability to label appropriately in real life. For this reason, the task of labelling a vignette may more accurately reflect the capacity to describe an illness in a peer rather than oneself.
In conclusion, an understanding of the landscape of labelling of mental disorders and factors that mediate their development can be harnessed to improve the effectiveness of community awareness initiatives. This in turn has the potential to improve labelling of mental disorders by young people and perhaps increase appropriate help-seeking during this crucial onset period.
Footnotes
Acknowledgements
Financial support was provided by the National Health and Medical Research Council, the Sidney Myer Health Fund, the Colonial Foundation and beyondblue: the national depression initiative. Amy Morgan, Claire Kelly, Robyn Langlands, Betty Kitchener and Len Kanowski had input into the survey content. Darren Pennay and Graham Challice from the Social Research Centre provided advice on survey methodology. Amy Morgan assisted with the data analysis and Kathryn Junor assisted in design of the figures.