
Abstract
Post-partum suicide rates among women in the general population are relatively low and range from 0.5 to 5.9 per 100 000 live births [1]. Oates, however, who analysed the psychiatric data in the Confidential Enquiries into Maternal Deaths in the UK, reported a suicide rate of 2 per 1000 among sufferers of puerperal psychosis [2]. Suicide accounted for up to 28% of all deaths in women within the first year after giving birth and was one of the three leading causes of maternal mortality. A total of 68% of suicides involved psychiatric illness, with the women in all the early (within 42 days of delivery) suicides suffering from severe psychiatric illness. Using the Danish psychiatric registry, Appleby et al. reported a suicide rate of 6.8% among women who had been hospitalized for a post-partum psychiatric disorder [3]. Both these studies emphasized that although post-partum women may have a low rate of suicide, those who develop severe mental illness (psychosis, schizophrenia, severe and psychotic depression and bipolar disorder) in the post-partum period are at high risk, particularly during the first year after childbirth [2], [3]. Schiff and Grossman reported that 34.4% of post-partum women (n = 179) who had committed suicide had a history of psychotropic and tranquilizer use, indicating pre-existing psychiatric illness [4].
Studies among post-partum women who have committed or attempted suicide indicate the following risk factors: pre-existing psychiatric illness including substance use, infant death and being a teenager. Most studies have reported that suicide was more common in the first few months after childbirth and that suicide attempts were more violent (e.g. jumping, hanging) than expected in the non-post-partum population [4], [5].
In general, rates of suicidal ideation and suicide attempts are much more common than completed suicide [6]. Suicide ideation with high intent has been found to be a distal predictor of later suicide in most situations, and it is estimated that approximately 10–15% of attempters eventually die by suicide [7], [8].
Rates of thoughts of self-harm and suicide attempts in the post-partum period range from 5% to 14% [9]. Studies on post-partum depression in community samples have shown suicidal ideation or attempts up to 15% [10]. Although the association between suicide and post-partum depression has been reported by several studies using screening methods, Lindahl et al. emphasized the need to study suicidality among women with post-partum psychosis because these women may be excluded from most studies [9]. Epidemiological studies on suicide in India are silent on this topic even though maternal mortality rates are approximately 4 per 1000 live births, and in 35% of deaths the cause is not known. This is probably because of poor reporting methods related to maternal deaths [11].
The aforementioned review indicates that even though suicide is more common among women with severe mental illness in the post-partum period, systematic investigation regarding its prevalence and risk factors in this population is lacking. The aims of the present study were therefore to determine the prevalence of suicidal ideation including thoughts of self-harm and suicide attempts in post-partum women admitted with severe mental illness, and to describe the clinical, childbirth-related and demographic correlates of suicidal ideation.
Methods
All women who were consecutively admitted with a severe mental illness (with its onset within 6 months of childbirth) from March 2006 to September 2007, to the inpatient psychiatric unit of the National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, India, were included in the study. NIMHANS is a 600-bed psychiatric hospital that serves as a secondary and primary care set-up for the local population of south India who live in and around Bangalore, and it also has tertiary care services for people from other parts of India. The most common route to mental health services for women who are pregnant or who have given birth is via a general practitioner, a referral from a hospital doctor, traditional healers or, frequently, by self-referral. Severe mental illness was described for the purpose of the study as an ICD-10 diagnosis of any of the following: bipolar affective disorder, mania, severe depressive disorders, or psychosis (including schizophrenia). Illness onset within 6 months of delivery was chosen as an inclusion criterion because of previous studies indicating that this period appears to be at highest risk for childbirth-onset psychosis [12]. In addition most mother–infant issues related to maternal psychiatric illness are important even after the traditional puerperal period (i.e. 6 weeks after childbirth). Eighty-four women who met the aforementioned criteria were recruited and interviewed within the first week of admission. Two women were excluded from the study because one had organic mental illness and the other woman committed suicide in the hospital, within 24 h of admission. Informed consent was obtained from all subjects except when they were too ill to understand the process of informed consent and give an informed choice (catatonia, severe agitation), in which case the primary caregiver was approached. All women or their primary caregivers gave consent for the study and the study was approved by the Institutional Ethics Committee.
Using a structured interview, data were collected from the women and a significant relative (usually spouse or primary caregiver), on sociodemographic details (age and parity of mother, age and sex of the infant, place of residence). Childbirth-related information such as parity, place of childbirth (home or hospital), complications and details of infant health were also collected. The diagnosis of severe mental illness was independently confirmed by two consultant psychiatrists and diagnosed using ICD-10 [13]. Details of past psychiatric history and comorbid personality and substance use were also recorded based on interviews with patients and a significant relative (usually spouse or primary caregiver).
Psychopathology including suicidality (attempts, and ideation, including thoughts of self-harm), were assessed using the Comprehensive Psychopathology Rating Scale (CPRS) [14]. The CPRS has operationally defined 66 items, which are rated on a 0–3 scale and measures the present psychiatric state based on clinical interview. Information on suicidality on the CPRS consists of the following items: 0, enjoys life; 1, fleeting suicidal thoughts; 2, suicidal thoughts are common and suicide is considered as a possible solution; 3, explicit plans for suicide and active preparations for suicide. The suicidality item from CPRS has been validated for the assessment of suicidality in psychotic patients [15]. Details of suicide attempts (including the method used), were recorded independently based on reports by the subject and/or a significant relative (usually the spouse or primary caregiver). Presence of thoughts and behaviours of infant harm were recorded when (i) ideas of wanting to seriously harm or kill the infant were reported by the subject; and (ii) any behaviours that could result in serious and life-threatening harm to the infant were reported either by the subject or observed by a primary caregiver or nursing staff during the first week of admission. The interviews were conducted by the primary author of the article. All data were collected as part of a research study and were not part of routine clinical care.
Data analysis
Data were first recorded in an interview schedule and then coded into a computer program. Statistical analysis was performed using SPSS version 11 (SPSS, Chicago, IL, USA). The χ2 test was used to analyse the association between presence of suicidal ideation, suicidal attempts and sociodemographic (age, family type, habitat, years of marriage), childbirth-related (parity, type of delivery, complications) and clinical variables including diagnosis, nature of onset (acute vs insidious as per ICD-10), time of onset after the delivery and psychopathology.
The CPRS can be used in full or as a pool of items, for the study of a particular psychiatric syndrome [14]. In the current study psychopathological scores derived from factor analysis of the CPRS into Positive, Negative, Depressive and Mania symptom dimensions have been used [16]. Logistic regression by forward selection was performed to determine the factors influencing the presence of suicidal ideation and suicide attempts.
Results
Women in the present study ranged from 18 to 32 years of age, with a mean age of 23.3 years (SD = 3.44). More than half (64%) had received a high school education, most were homemakers (83%) and from a rural background (80%). All women were married. A total of 52% were primiparous and the average time of post-partum illness onset was 6.6 weeks after childbirth (mean = 6.6 weeks, SD = 6.65). Of the women included in the sample 31 (38%) had a history of previous episodes, with seven (9%) of those histories referring to post-partum episodes. History of major mental illness in first-degree relatives was present in 20 women (24%) in the sample (Table 1). The mean infant age at the time of assessment was 10.9 weeks (SD = 9.1) and 76 infants (87%) were full term. Fifty-two infants were male (63%) and 30 (37%) were female. A total of 68% of the women had an onset of illness within 6 weeks of childbirth (mean = 2.7 weeks, SD = 1.93).
Demographic details for women with severe post-partum mental illness
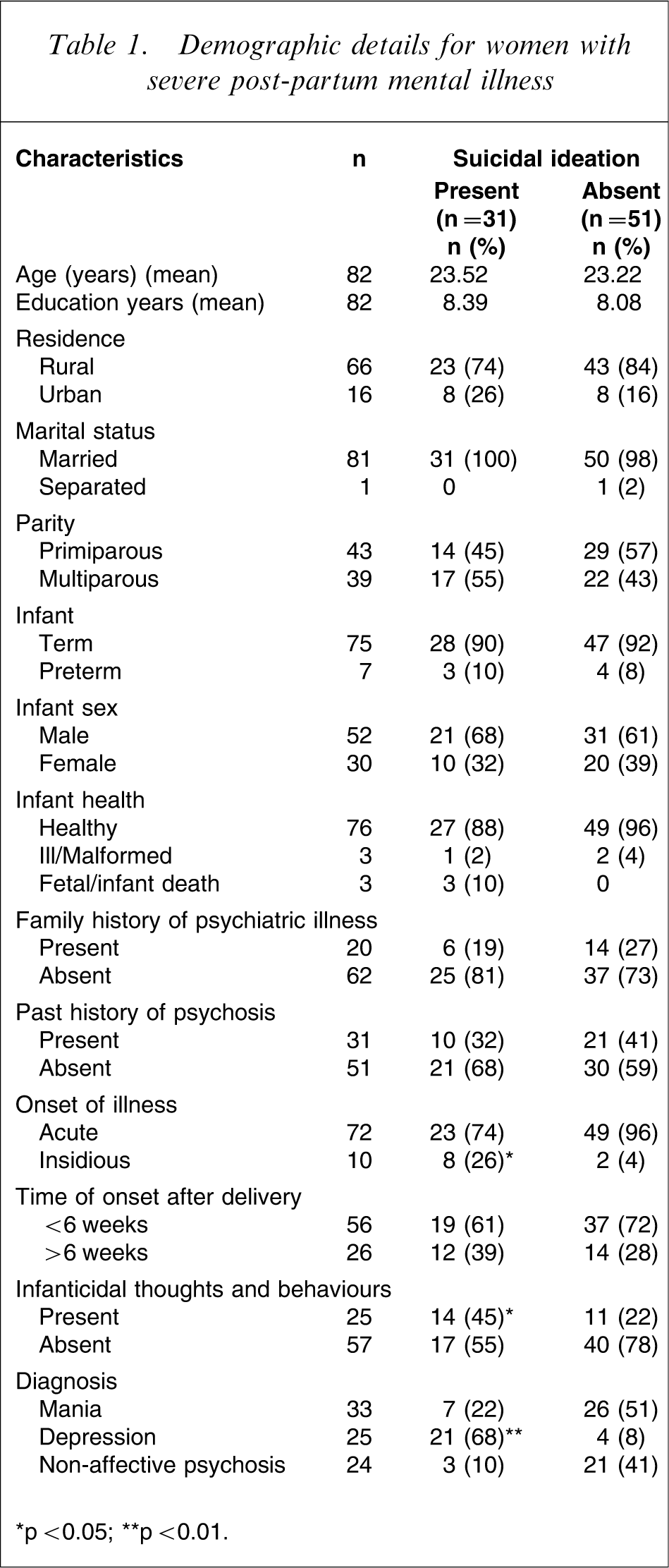
∗p < 0.05; ∗∗p < 0.01.
Psychiatric diagnosis
Thirty-three women (40%) had a bipolar affective disorder (mania or mixed affective type) and 25 women had severe depression (30%). A total of 21 women received a diagnosis of acute psychosis (26%) while only three women had schizophrenia (2.5%). The majority of the women in the sample had psychotic symptoms (98%) in the form of presence of delusions and/or hallucinations. None of the women in the sample had a comorbid personality disorder or substance use.
Suicidal ideation (scores 2 and 3 on the CPRS) was found in 38% (31/82) of the subjects and suicide attempts were reported in 18% (15/82). Suicidal ideation was seen in 21 of 25 depressed mothers (84%) compared to seven of 33 (21%) with mania (p < 0.001) and three of 23 (13%) with psychotic illness (acute psychosis, schizophrenia, psychosis not otherwise specified). Almost all of the women (14/15) who had attempted suicide had used violent methods including strangulation, hanging, jumping or immolation. Among the women who were hospitalized, three had adverse infant outcomes (infant death) and all these women expressed suicidal ideation. There was a significant association between presence of suicidal ideation and suicide attempts (r = 0.53, p < 0.001). Among the clinical variables only a diagnosis of depression and an insidious onset of illness were significantly related to suicidal ideation (p < 0.05). None of the other sociodemographic, clinical or childbirth-related variables were different between the two groups.
Infanticidal thoughts and behaviours of significant harm to the child were found in 25 of the 82 women (30%). This was in the form of mothers expressing ideas of harming or killing the infant or harmful behaviours towards the infant such as hitting, trying to smother, drown or drop the infant.
In 14 of 31 women (45%) who reported suicidal ideation, there were associated infanticidal thoughts and behaviours. Women with suicidal ideation had significantly higher infanticidal thoughts and harmful behaviours towards the infant (p = 0.024).
Predictors of suicidal ideation
Onset of illness, infanticidal behaviours and the psychopathological symptom dimensions were entered into the model of logistic regression for suicidal ideation. Among all the psychopathological dimensions, scores on the depressive symptom dimension, which included sadness, inability to feel, pessimistic thoughts, fatigability, inner tension, concentration difficulties, failing memory and lassitude (odds ratio = 1.4, p < 0.001) emerged as significant predictors of the variance of the suicidal ideation (Table 2). These variables were able to classify 89% of the data correctly into respective groups.
Logistic regression coefficients for significant predictors of suicidal ideation

Discussion
The present findings indicated a high prevalence of suicidal ideation (38%) and suicide attempts (18%) in mothers with severe mental illness in the post-partum period. Most studies on post-partum suicide are on community samples of non-mentally ill women or women with mild to moderate mental disorders. The prevalence of suicidality in these populations ranged from 5% to 14% [9], [17]. The present study has substantiated that although post-partum women may have a low rate of suicide, those who develop severe mental illness in the post-partum period are at high risk, particularly during the first year after childbirth [2], [3].
The majority of women in the current sample had attempted suicide using violent methods, confirming earlier reports of high rates of dramatic methods of suicide, with high intentionality [2], [4]. Earlier studies have also shown that in the general population, Axis 1 disorders, particularly depressive disorders and substance use disorders, are important predictors of suicidality [18], [19]. The present results also show that among post-partum women with both affective and non-affective severe mental illness, the depressive symptom dimension appeared to be the most important risk factor predicting suicidal ideation and attempts. Consistent with earlier studies [20], [21], there was a significant association between infanticidal thoughts, infant harm and suicidal complication among women with severe mental illness in the post-partum period [22], these findings have important implications.
Research has shown that fetal or infant death is a significant predictor of suicidal behaviour in post-partum women [4]. This is substantiated in the current sample, with all the women with adverse infant outcome reporting suicidal ideation.
In addition to psychiatric morbidity, several cultural and social factors are known to influence mental health (particularly depression) in the post-partum period among Indian women. Risk factors for poor mental health include partner violence, poor marital support and having a female child [17]. Women are also expected to remain indoors and not socialize much. There are several rituals, however, that ensure that the mother has rest, adequate sleep and a special diet and hence might be protective [23]. Most women deliver in their natal homes and stay on until the infant is at least 6 months old, and hence have the support of their mothers. But this also entails being away from the spouse, which might contribute to stress. Most studies that have highlighted the aforementioned sociocultural risk factors have studied women with common mental disorders. We are still not aware how these factors influence women with severe mental illness, and the area needs further study. Although the current study did not specifically assess other sociocultural issues, gender of the infant did not emerge as a significant predictor for suicidal ideation in this sample. Another cultural factor that might contribute to severity of illness at presentation might be normalization of behavioural problems in the post-partum period and late detection of the psychiatric problem. In South India, Sanni or Janni (withdrawn behaviour, irritability) among women in the post-partum period is considered common and help is sought only if the situation becomes unmanageable.
The present study was a cross-sectional study on a hospital-based population and did not compare rates of suicidal ideation or attempts with a control group of non-post-partum mentally ill women. It was also done in an inpatient sample and rates may be different in outpatient and community samples. To be generalizable, the study needs to be replicated in larger samples, in different cultural settings and in an outpatient sample with a control group.
The strengths of the study include a detailed clinical assessment including that of psychopathology, suicidal ideation and attempts. In addition, corroborative data regarding suicide were available from all family members. The fact that a single trained researcher interviewed all the women also adds to the reliability of the present findings. It is also one of the few studies that has systematically assessed both suicidal ideation and attempts in women with post-partum psychosis.
Conclusion
Suicidal ideation is common in women with severe mental illness in the post-partum period and is often associated with infanticidal ideas. Because women with severe mental illness in the post-partum period are a vulnerable group, a comprehensive risk assessment with early detection and treatment with close supervision is necessary.
Footnotes
Acknowledgements
We thank Mr Shanmugam for his assistance in statistical analysis.