
Abstract
Population estimates for the 12 month prevalence social phobia (SP) range from 2 to 8% [1–3], with higher rates in alcohol use disorder individuals [4]. A review of studies examining rates of SP in clinical alcoholism patient samples reported prevalence typically in the range of 10–20% [5], while rates tend to be higher in mixed alcohol/other drug samples [6–8].
SP typically has an earlier onset age than for substance use disorder (SUD), and consequently most attempts to understand the association between these two sets of disorders have worked on the basis of the direction of causality primarily working from SP to SUDs [9]. Models include the self-medication hypothesis [10], a general model that can be applied to the functional relationship between a range of substances and a range of coexisting psychiatric conditions, and the stress response dampening model [11], which is more specifically oriented to alcohol's ability to reduce anxiety.
Thomas et al. looked at the association between SP and a range of substance use and psychiatric variables in the alcohol treatment Project MATCH sample [12]. They compared 397 participants with SP with 397 non-SP participants matched for gender, age and treatment, with both groups meeting a range of other psychiatric diagnoses. Given their sample size they were able to divide the groups into exploratory/confirmatory subgroups to counter the risk of type I error from a large number of comparisons. Factors differing across diagnostic group for both exploratory and confirmatory samples were that the SP group were more dependent on alcohol and relied more on alcohol to improve sociability and enhance functioning, and had a higher lifetime prevalence of major depressive episode. The two groups did not differ for drinking pattern, tranquillizer use, or age of onset of alcohol problems, current depressive symptoms, current psychiatric severity, sociopathy/socialization, or lifetime diagnosis of antisocial personality disorder. The authors had specifically hypothesized that gender interactions might exist, but this did not prove to be the case.
When broader measures of anxiety disorder in substance treatment populations are examined in comparison to non-anxious individuals, there are few differences in clinical presentation [13]. Having an anxiety disorder has been found to predict shorter duration of treatment [14] or has no association [15], while there were few associations (two out of 15 utilization measures) in a small Australian sample [16]. SP and/or generalized anxiety disorder has been found to predict better outcome in one study [8], no association was found in a second [16] and an indirect association with worse drinking outcome was found only via reduced retention and increased levels of depression [14].
Evidence as to the impact of comorbidity on treatment outcome is mixed, with some showing worse treatment outcome predicted by comorbidity generally [17] and anxiety disorders more specifically [14], while anxiety disorder may not predict treatment retention, or level of treatment attendance [15]. The presence of SP has also been linked to better outcome [8].
In the only published trial of concurrent alcoholism and SP treatment for this population Randall et al. randomized patients to either cognitive–behavioural therapy (CBT) for alcoholism or CBT for both conditions currently [18]. The combined treatment group faired worse on drinking-related measures at 3 months after treatment, while there were no differences between the two for SP symptoms.
In summary, SP is common in SUD treatment settings. Despite SP being more common in mixed substance settings most research has been undertaken with alcohol treatment samples. While some differences between SP and non-SP groups have been found, SP is often not isolated from other diagnoses and there is generally a failure to distinguish the impact of SP per se versus a more generalized effect of a broader range of coexisting conditions. This shortcoming is most obvious when elevated rates of specific disorders are identified when comparing SP versus non-SP groups, because almost any diagnosis raises the odds of a second diagnosis [19]. The failure to control for comorbidity per se is particularly important because coexisting conditions are the rule rather than the exception in SUD treatment settings, and so any attempt to highlight differences for a specific diagnosis should make this distinction.
Given the high rate of SP identified in the present sample, and the limitations of the literature as described here, the purpose of the present study was to identify any differences between SP and non-SP patients in an SUD setting in terms of clinical presentation, treatment utilization, and treatment outcome and, if any differences were found, to clarify whether these were features particularly associated with the diagnosis of SP or were common to the broader group with other coexisting conditions.
Method
Participants
Participants were initially drawn from two outpatient government-funded specialist community alcohol and drug services (CADS) in the cities of Hamilton and Christchurch, New Zealand. The aim was to recruit a representative treatment-seeking adult sample, and for this reason exclusions were kept to a minimum. Patients were excluded if they were aged <17 years or were deemed too psychiatrically unwell or cognitively impaired to understand and tolerate the interview procedure. Patients serving a term of imprisonment at the time of assessment were also excluded because this would have markedly affected pattern of recent substance use. One hundred and five patients completed the initial assessment and all agreed to a 9 month follow-up interview, which was completed by 102 patients. Current SP was diagnosed in 33 patients. This SP group was compared to those with no coexisting psychiatric diagnosis (NPD, n = 29) and those with a coexisting psychiatric diagnosis other than SP (OPD, n = 40).
Design and procedure
Interview
DSM-IV Axis I diagnoses were generated using the computerized Composite International Diagnostic Interview (CIDI) [20]. The CIDI has been shown to have good reliability and to be appropriate for a wide range of clinical settings [21], with agreement between CIDI-Auto and clinical diagnosis for SP found to be fair, producing a higher rate of agreement than for most other anxiety disorders or a major depressive episode [22].
DSM-III-R diagnoses of conduct disorder and antisocial personality disorder were made using the corresponding sections of the Diagnostic Interview for Genetic Studies (DIGS) [23]. Past 6 months substance use was recorded using the timeline follow-back procedure [24], with responses confirmed by a nominated collateral informant. Treatment utilization prior to baseline and follow-up interview were recorded using a semi-structured interview. Additional instruments administered at baseline and follow up were the Medical Outcomes Trust 12-item short form health scale (SF-12) [25], and the Social Problems Questionnaire (SPQ) [26].
The question posed in this paper was whether SUD treatment patients with coexisting SP differ from non-socially phobic SUD treatment patients. If any differences emerged then the next question was whether the differences were associated with SP per se or whether they were the consequence of having a coexisting condition. To answer these two questions the SP group was compared to both the NPD and OPD groups, with the OPD group acting as a psychopathology control group. The three groups were compared on demographic, current clinical, and past treatment utilization variables at baseline, while follow-up data were used to compare the groups on treatment outcome and treatment utilization.
Statistical analysis
All variables were initially explored using diagnostic status as a nominal categorical variable (SP/NPD/OPD), using χ2 for categorical dependent measures and ANOVA for continuous dependent measures. For p < 0.15 two pairwise analyses were conducted: first to see if the SP group were significantly different from NPD; and second to compare SP with OPD. Again χ2 and ANOVA were utilized. For outcome measures the baseline value was controlled for by entering the baseline value as a covariate.
Results
Rates of current coexisting conditions other than SP for the SP/OPD groups respectively were: major depressive disorder 54%/38% (χ2=2.12, NS), bipolar disorder 15%/23% (χ2=0.63, NS), any mood disorder 79%/70% (χ2=0.73, NS), post-traumatic stress disorder 21%/50% (χ2=6.43, p = 0.011), panic disorder 45%/8% (χ2=14.02, p < 0.001), agoraphobia 45%/15% (χ2=8.18, p = 0.004), and antisocial personality disorder (ASPD) 18%/30% (χ2=1.54, NS).
Mean onset age of SP was 11.5 years (SD = 6.4). This was earlier than the onset age of first SUD for 79%, the same for 6% and later for 15% of the sample, with a mean latency to onset of SUD of 7.1 years (SD = 8.5).
The only significant difference for demographic variables (Table 1) was for years of education, in that the SP group was less educated than the NPD group (t = 2.16, p = 0.035) but no different than the OPD group (t = 0.84, p = 0.404).
Demographic variables
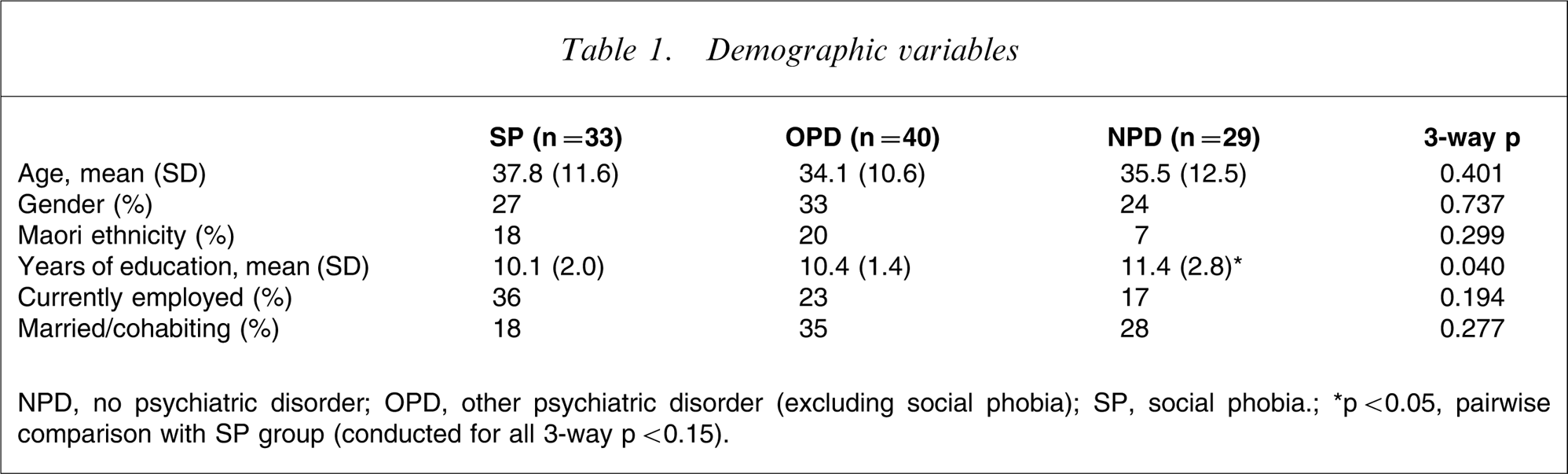
NPD, no psychiatric disorder; OPD, other psychiatric disorder (excluding social phobia); SP, social phobia.; ∗p < 0.05, pairwise comparison with SP group (conducted for all 3-way p < 0.15).
For current amphetamine dependence, number of substance dependences and current ASPD, significant differences were between OPD and NPD, but not for SP (Table 2). Percentage using days was lower for SP compared to OPD (t = 2.03, p = 0.046) but not compared to NPD (t = 1.42, p = 0.161). There were no significant pairwise comparisons for percentage days using cannabis.
Baseline clinical variables
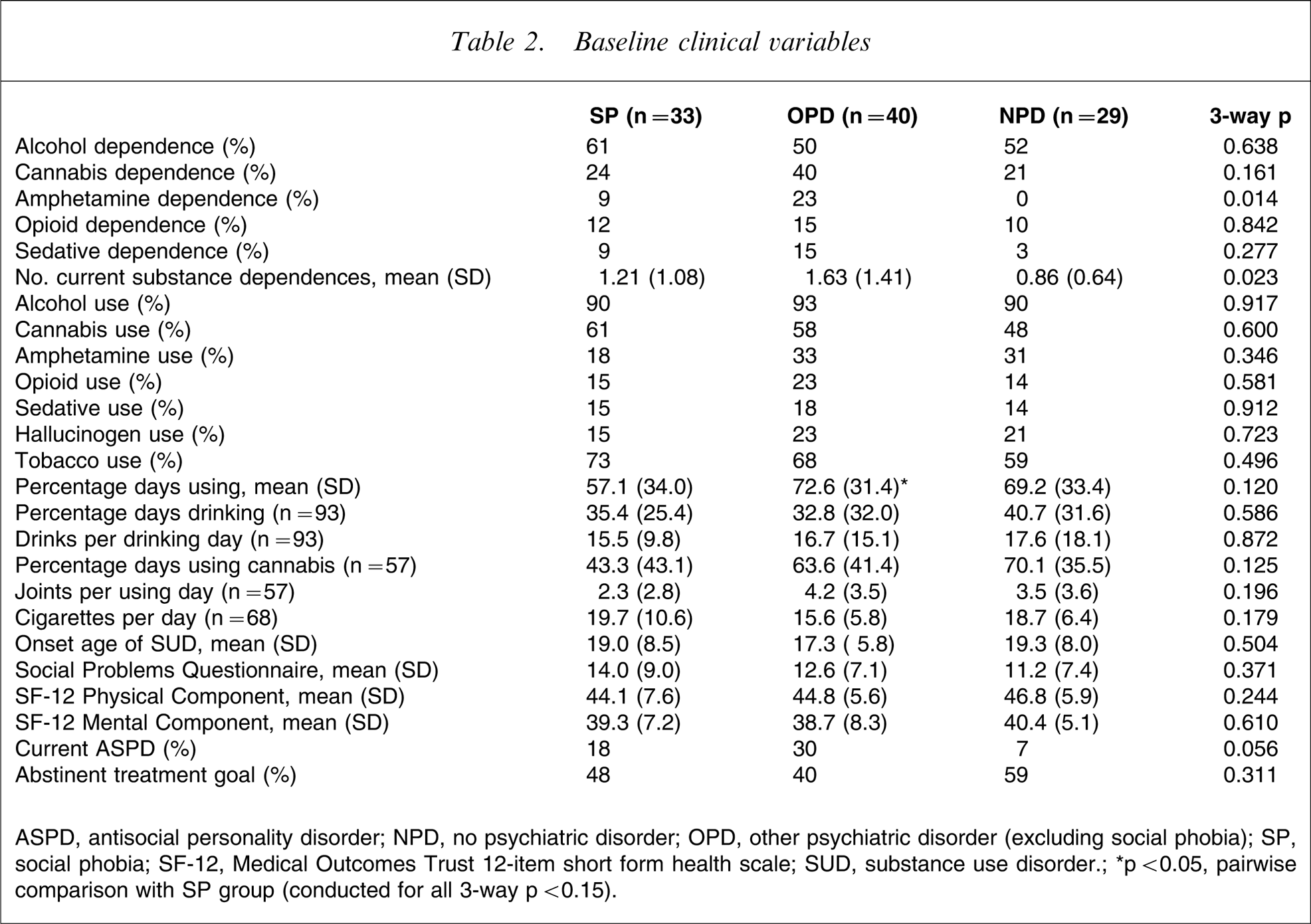
ASPD, antisocial personality; NPD, no psychiatric disorder; OPD, other psychiatric disorder (excluding social phobia); SP, social phobia; SF-12, Medical Outcomes Trust 12-item short form health scale; SUD, substance use disorder.∗p < 0.05, pairwise comparison with SP group (conducted for all 3-way p < 0.15).
The SP group did not differ significantly from either other group for history of inpatient mental health treatment (Table 3). SP were more likely to have a history of being prescribed psychiatric medication than NPD (χ2=5.04, p = 0.025), but were no different than OPD (χ2=0.04, p = 0.841). SP patients were also more likely to be prescribed antidepressants than NPD patients (χ2=5.42, p = 0.020) but were no different to OPD patients (χ2=0.00, p = 0.958). The difference in history of being prescribed anxiolytics/tranquillizers just failed to reach significance between SP and NPD (χ2=3.71, p = 0.054) and between SP and OPD (χ2=3.51, p = 0.061).
Past treatment utilization
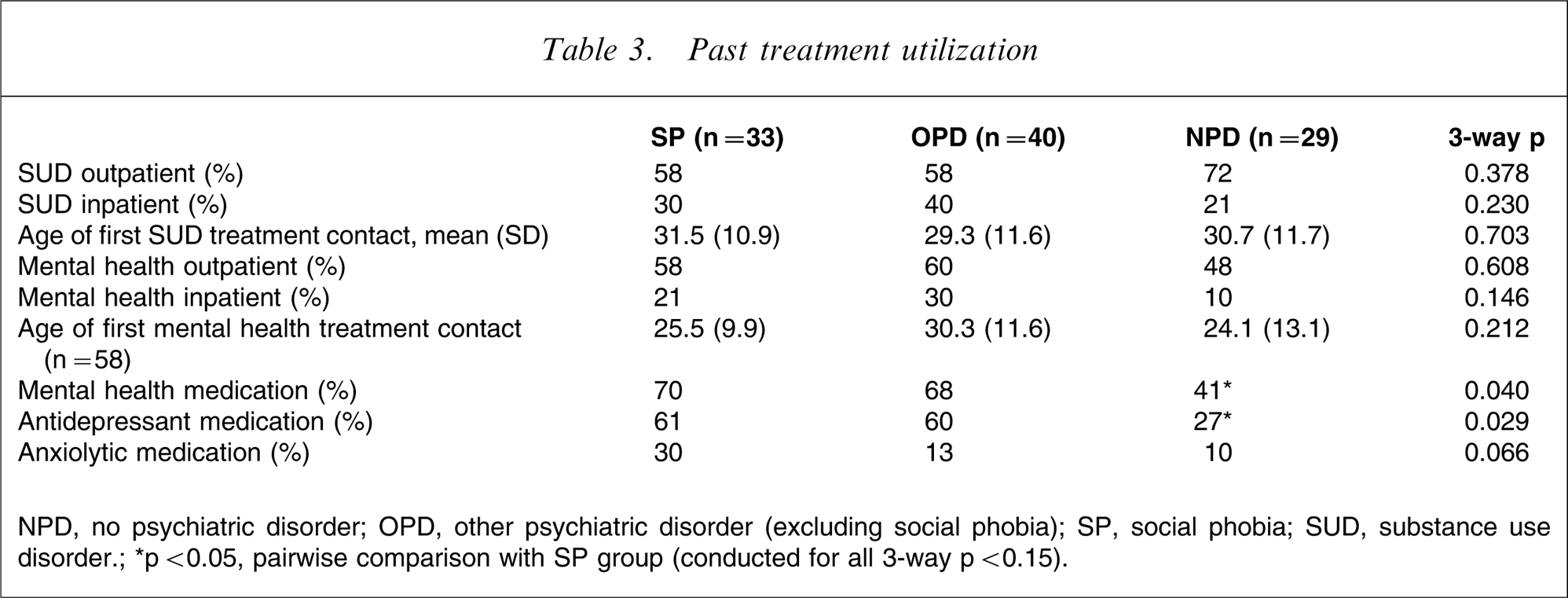
NPD, no psychiatric disorder; OPD, other psychiatric disorder (excluding social phobia); SP, social phobia; SUD, substance use disorder.; ∗p < 0.05, pairwise comparison with SP group (conducted for all 3-way p < 0.15).
SP had lower 9 month SF-12 Mental Component scores (Table 4) compared to NPD (F = 4.70, p = 0.034) when baseline Mental Component scores were controlled for, but did not differ from OPD for Mental Component scores (F = 0.41, p = 0.523). Diagnostic group did not predict outcome as captured by substance use measures, social problems or employment.
Treatment outcome
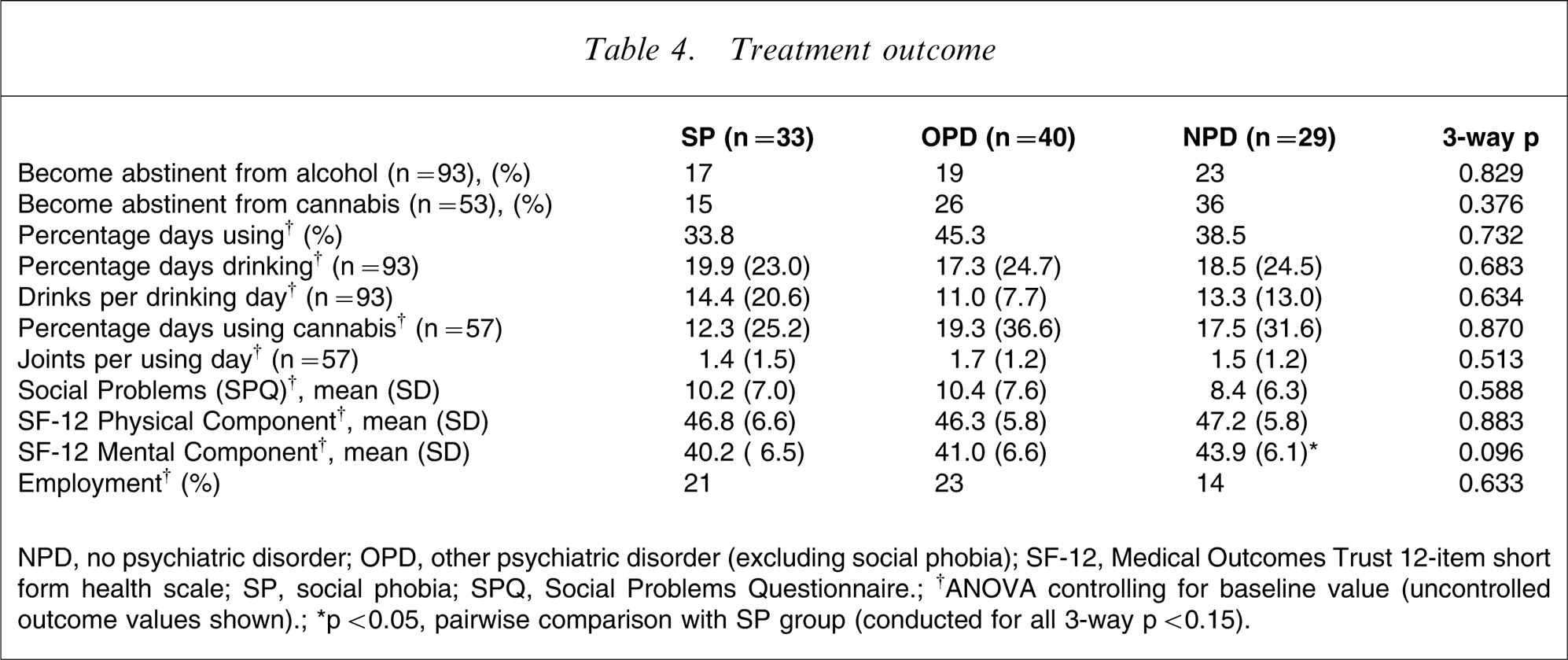
NPD, no psychiatric disorder; OPD, other psychiatric disorder (excluding social phobia); SF-12, Medical Outcomes Trust 12-item short form health scale; SP, social phobia; SPQ, Social Problems Questionnaire.; †ANOVA controlling for baseline value (uncontrolled outcome values shown).; ∗p < 0.05, pairwise comparison with SP group (conducted for all 3-way p < 0.15).
There were no significant pairwise comparisons for prescription of mental health medications during the index treatment/follow-up period (Table 5).
Index treatment utilization
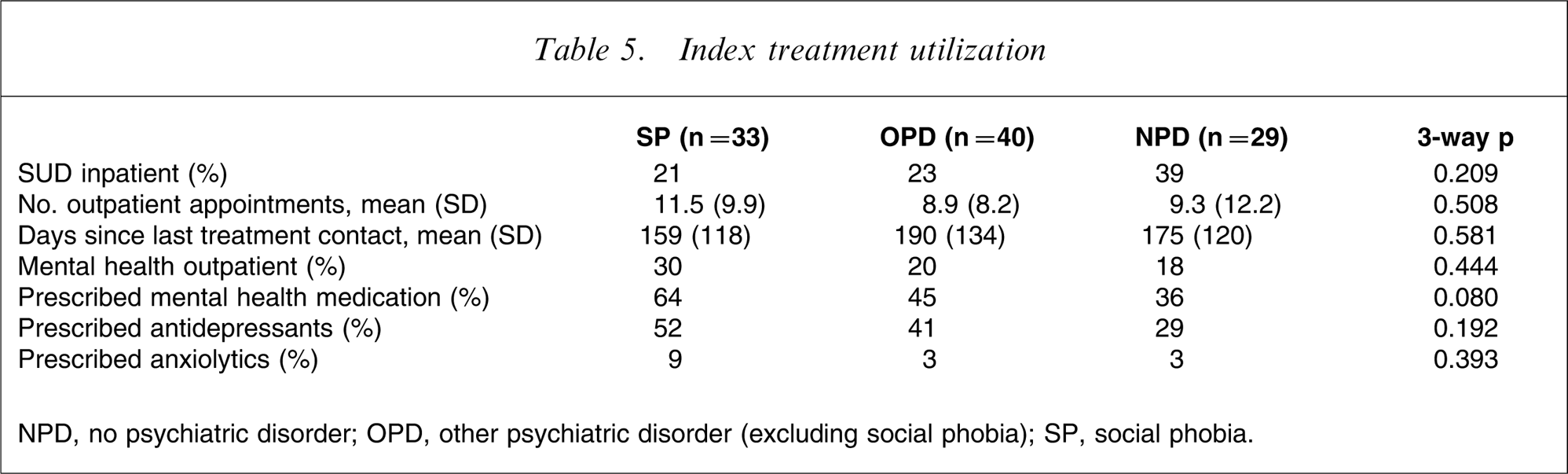
NPD, no psychiatric disorder; OPD, other psychiatric disorder (excluding social phobia); SP, social phobia.
Discussion
The present study identified relatively few differences between SP patients and either OPD or NPD patients when a range of patient characteristic, treatment utilization, and outcome variables were considered. Where differences between groups have been identified these have typically been between SP and NPD but not OPD, as is the case for education, ever being prescribed mental health medication generally or antidepressants specifically, and follow-up SF12 Mental Component Scores, or that the SP group appears to represent an intermediary between the OPD and NPD group, with the OPD group being consistently more pathological than the NPD group. Variables for which this was the case were current amphetamine dependence, current number of substance dependencies, current ASPD, and having ever been admitted to an inpatient mental health treatment facility. The SP group did appear more pathological than either other group for having ever been prescribed anxiolytics, although this result failed to reach significance. In contrast, the SP group were the least pathological in number of days using any substance, with this result echoed by the pattern of cannabis use.
Clearly a potential weakness of the study is the limited sample size. A power analysis showed that when power was set at 80%, and alpha at 5%, a moderate to large effect size (ES) was detected when comparing SP with NPD (ES = 0.72) and SP with OPD (ES = 0.67). But given the large number of comparisons made and the absence of any significant effects that distinguish SP from both OPD and NPD, and the consistent ranking of the three groups identified here, it can be concluded that, for this sample, the presence of SP does not predict a substantially different clinical presentation, treatment utilization, or treatment outcome than is the case for non-SP in a manner that would indicate a direct role of SP per se rather than comorbidity in general.
Having argued against large or widespread differences between SP and OPD/NPD, it is not reasonable to conclude that SP patients should be treated as indistinguishable from non-SP patients. It is possible that there exist important differences between these groups that were not measured in the current study, or that a small number of variables measured do in fact differ between the groups, but with a small to moderate effects size that, although not able to be identified statistically in the current study, may nevertheless be clinically significant, as may be illustrated, for example, by the comparatively low rates of employment and high levels of social problems (SPQ scores) for the SP group.
The present study found treatment utilization to be associated with comorbidity in general, but not SP specifically, while comorbidity was a poor predictor of treatment outcome. These findings, and the absence of marked differences in presentation, would suggest that treatment specifically targeting comorbid SUD and SP may not be a high priority.
The fact that the SP group were often intermediate between OPD and NPD across a range of clinical variables, despite a full range of other comorbidities present within the SP group, raises the possibility that SP may act as a protective factor in this population. The mechanism for this is unclear, but it is possible that SP may reduce the risk-taking behaviour that is often a feature of substance misuse and which in turn may contribute to a range of negative outcomes including social functioning, and physical and mental health. This would be an effect specific to SP in a substance-misusing population rather than a positive factor of SP more generally. In the absence of other research in this population also controlling for the presence of comorbidity in the non-SP group, this possibility remains highly speculative and warrants further investigation.
Footnotes
Acknowledgements
This study was funded by the Alcohol Advisory Council (ALAC) and could not have been undertaken without the support of management and staff at the three participating services.