
Abstract
Keywords
Case management is the primary model of service delivery both in Australia's public community mental health services and in similar services within comparable countries around the world [1, 2]. There has been considerable research into the roles and activities of mental health case managers [3], outcomes for patients receiving different forms of case management [4] and work-related stress associated with case management [5]. There is evidence that the size and characteristics of the caseload for which a case manager is responsible is relevant to each of these domains [4, 6, 7]. This evidence is discussed in greater detail here.
Caseload size
The available evidence suggests that there is wide disparity internationally in the size of the caseloads carried by case managers working in public community mental health services [8]. In some instances this is a function of the implementation of a specific model of case management. Intensive case management, also known as assertive community treatment, is based on intensive therapeutic contact with a small number of patients. Even within this model, however, there is considerable variation, with Australian caseloads typically being in the lower range [7] and UK caseloads in the higher range [9–11]. In the USA, caseload size is highly variable, even when the model of care is broadly similar [12, 13].
In an early study Intagliata suggested that caseloads in excess of between 20 and 30 would result in reactive case management, with deficiencies in service planning, support for families and carers and liaison with other services [14]. Subsequent research has lent support to this proposition [5, 13, 15]. When faced with high caseloads, case managers deal with crises and immediate problems and are less likely to keep in touch with families or contact patients when they are in hospital [6].
There is mixed evidence as to the impact of caseload on patient outcomes. Most evidence suggests that intensive case management reduces inpatient usage when compared with standard case management [16]; there is little evidence to suggest that it results in reduced symptoms or higher levels of functioning [8]. Patients provided with more intensive case management are less likely to be lost to follow up and therefore receive superior continuity of care [17]. The evidence concerning the impact of caseload on practitioner stress is also equivocal [7, 18, 19]. It is possible that overall workload rather than caseload is a contributor to stress and that practitioners with high caseloads generally manage their workloads by allocating less time and providing fewer services to each person within the caseload.
In summary, it appears clear that caseload affects case manager activities and service responsiveness but it is less clear as to the secondary effect on the well-being of patients or case managers. Aside from direct and indirect impact of caseload, there are important issues of equity and fairness with respect to distribution of caseload within a mental health team.
Managing caseload: controlling size of caseload and adjusting for complexity and other factors relevant to caseload burden
The number of patients for whom a case manager has case responsibility is at best a crude indicator of the workload associated with the caseload [20, 21]. Patient characteristics, case manager characteristics, characteristics of the service and support environment, geographical considerations and how new the patient is to the service have all been identified as being relevant to the workload associated with a case management caseload. There have been a number of attempts to develop tools designed to adjust caseload to take into account some or all of these factors, both for use in general health settings [22] and mental health settings [21].
Although workload management tools offer the potential benefit of reducing errors associated with human judgement by integrating a complex range of factors to yield a single numerical score [20, 21], they have been criticized on the grounds that they either fail to capture or they distort key elements of the practitioner–patient relationship [23], or that information yielded is unreliable because it is inaccurately or incompletely compiled [22]. It has also been pointed out that when workload tools substantially rely on practitioner reports of patient contact rates, there is risk that practitioners will over-service easier patients to maintain a caseload that appears high but is not well-targeted [21].
Little is known about the extent to which caseload management tools are used in routine service management, and anecdotal reports suggest that caseload monitoring is typically informal.
Background
The Victorian Psychiatric Services Certified Agreement 2004–2007 required area mental health services to introduce a locally agreed caseload management system that met the requirements of the Certified Agreement. The aim of the presents study was to investigate caseload management procedures within Victoria's public community mental health services prior to the time when they were required to implement caseload management under the agreement, so as to establish a baseline against which the impact of changes could be evaluated. Of particular interest was the relationship between existing caseload management practices and case manager well-being and self-efficacy.
Method
Overview of study design
The study reported here was cross-sectional and used quantitative methods to determine the status of caseload management, case manager self-efficacy and work-related stress prior to implementation of new caseload management procedures as mandated by an industrial agreement. The aim was to find out about caseload management processes in routine service management and to better understand the relationship between these practices and case manager activity and well-being.
Ethics approval
This study was approved by the Behavioural and Social Sciences Ethical Review Committee of the University of Queensland
Participants
All Victorian mental health professionals performing case management roles were eligible to participate. The Department of Human Services identified services where case management is provided and alerted them to the survey. A total of 188 completed the survey. Although the exact number of people providing case management is not known because staffing profiles do not specify service role, it is estimated that this was a response rate of just over 15%. Characteristics of respondents are set out in the first part of the results section.
Measures
The study used both standardized measures and measures developed specifically for the study. Case manager self-efficacy was measured using the Case Manager Personal Efficacy Scale (CMPES) [6]. The CMPES is a 17 item measure with good internal consistency (Cronbach α = 0.82 in the original study and 0.88 in the present study) that has previously been found to be sensitive to caseload [6]. Work-related stress was measured using the Mental Health Professionals Sources of Stress (MHPSS) scale [24]. The MHPSS is a 42-item measure consisting of seven subscales, each of six items.
New measures developed for the present study included items designed to obtain key demographic information about respondents, items designed to elicit information about procedures used to allocate new cases and to monitor caseloads, and attitudes towards currently used case allocation and caseload monitoring procedures.
Procedure
Mental health professionals working as case managers in Victoria's mental health services were invited to participate in the study, using the Department of Human Services email network. The email message provided a website address and secure log-on procedures. Once logged on, the participant completed informed consent procedures and was directed to the questionnaire.
Data analysis
Online survey data were automatically uploaded to a Mysql database and then imported to SPSS version 14 (SPSS, Chicago, IL, USA), which was used for all data analysis.
Results
Respondent demographic characteristics
Gender breakdown indicated that 130 (70%) were female and 58 (30%) were male. The mean age of respondents was 41 years, with the youngest respondent being 22 and the oldest being 64. Respondents had an average of 14 years of mental health experience, with the lowest being 6 months and the highest 42 years. The predominant professional group was nurses (52%), followed by social workers (19%), psychologists (15%) and occupational therapists (12%). Only five psychiatrists/psychiatric registrars completed the questionnaire. Team leaders comprised 20% of respondents. The largest group (65%) worked in adult mental health services. Nineteen per cent worked in child and adolescent mental health services and 17% worked aged mental health services. All the demographic indicators suggested that the sample was broadly representative of the community mental health workforce in Victoria.
Caseload size
Full-time case managers (n = 109) reported an average caseload of 20 (range = 2–59). This is the same average caseload size reported in an earlier national study [6]. Team leaders with case loads (n = 29) reported an average caseload of 12 (range = 1–30). Reported caseload size in the online study was consistent with caseloads reported by team leaders and service managers in a parallel qualitative study.
Case manager self-efficacy
Mean score on the CMPES was 63.0 (SD = 9.97) for the full sample (n = 188) and 62.7 if team leaders were excluded (n = 150). These scores were similar to those obtained in a national study (n = 291) in which CMPES was 64.4 (SD = 8.39) [6]. A mean score of 63 suggests that case managers in this sample typically rate themselves as able to perform most core case management roles. Availability of support services, sufficient time to respond to patient needs and keeping up with paperwork were the items with lowest scores. These were all substantially lower than those reported in the earlier national study, suggesting that there may be emerging limitations to self-efficacy in these areas.
Work-related stress
Mean score for the MHPSS was 1.3, which is comparable with scores reported in previous studies [18, 24]. Respondents identified workload as the major source of stress. Within the workload subscale the item ‘too many patients’ was endorsed by 27% of respondents as ‘does apply to me’. This was a lower rating than ‘too much work’ (38%), ‘too many different things to do’ (34%) and ‘not enough time to complete tasks’ (33%). Nonetheless ‘too many patients’ had a relatively high endorsement among the 42 items in the scale and would appear to be one of the major sources of stress.
Relationship between caseload size and stress and personal efficacy
Size of caseload was significantly correlated with scores on the Workload subscale of the MHPSS (r = 0.26, p < 0.01), the Professional Self-Doubt subscale (r = 0.15, p < 0.05) and the total scale score (r = 0.16, p < 0.05) but not with other subscales. Size of caseload was also significantly (negatively) correlated with the CMPES total (r = − 0.22, p < 0.01). This was consistent with previous findings of a similar significant association (r = − 0.2, p < 0.01) [6].
Case allocation
Self-nomination (52%), team consensus (41%) and team leader decisions based on either an allocation tool (30%) or personal judgement (29%) were the ways by which participants indicated that case allocation occurred all or most of the time. Participants were generally happy with procedures for case allocation, with 71% indicating that it was always or mostly fair and 67% indicating that they were very or mostly satisfied with procedures. Participants were asked about the benefits of using an allocation tool that had an algorithm or formula to determine where a new case should be allocated. A greater proportion (45%) indicated that such a tool would result in fairer allocation, compared to those (20%) who indicated that it would result in a less fair allocation. Only 30%, however, indicated that it would result in more appropriate allocation whereas 36% indicated that it would result in less appropriate allocation of new cases.
Higher caseloads were associated with lower rating of fairness of allocation (r = − 0.18, p < 0.05) but not with global satisfaction concerning allocation. Both rating of the fairness of case allocation and global satisfaction with case allocation were significantly associated with allocation by team consensus (r = 0.26, 0.24, p < 0.01) and allocation by team leader using judgment (r = 0.23, 0.21, p < 0.05). Self-nomination and allocation using an allocation tool were not associated with either rating of fairness or with global satisfaction. Higher case manager personal efficacy scores were associated with both global satisfaction with case allocation (r = 0.46, p < 0.01) and with higher rating of fairness of case allocation (r = 0.31, p < 0.01). Only one form of case allocation (team leader using judgement) was associated with higher CMPES scores (r = 0.23, p < 0.01). Higher stress as measured by MHPSS was associated with lower global satisfaction with case allocation (r = − 0.42, p < 0.01) and lower rating of fairness of case allocation (r = − 0.24, p < 0.01).
Caseload monitoring
Self-monitoring of caseloads was the dominant means by which caseloads were reported as being monitored after initial allocation. Ninety-one per cent of participants indicated that they monitored their caseload all of the time or most of the time. The next highest ratings were for monitoring via team meetings (23% all or most of the time) or by team leaders (22% all or most of the time). It was notable that the team leaders saw the situation somewhat differently and were significantly more likely (z = 3.6, p < 0.001) to indicate that they were involved in monitoring of caseloads all or most of the time. More active monitoring of caseloads was associated with smaller caseloads, especially when monitoring occurred during team meetings (r = − 0.29, p < 0.01).
There were clear relationships between both the extent and form of caseload monitoring and scores on the work-related stress and case manager personal efficacy measures. These were moderately complex and are set out in Table 1.
Level of caseload monitoring vs case manager personal efficacy (CMPES) and work-related stress (MHPSS)
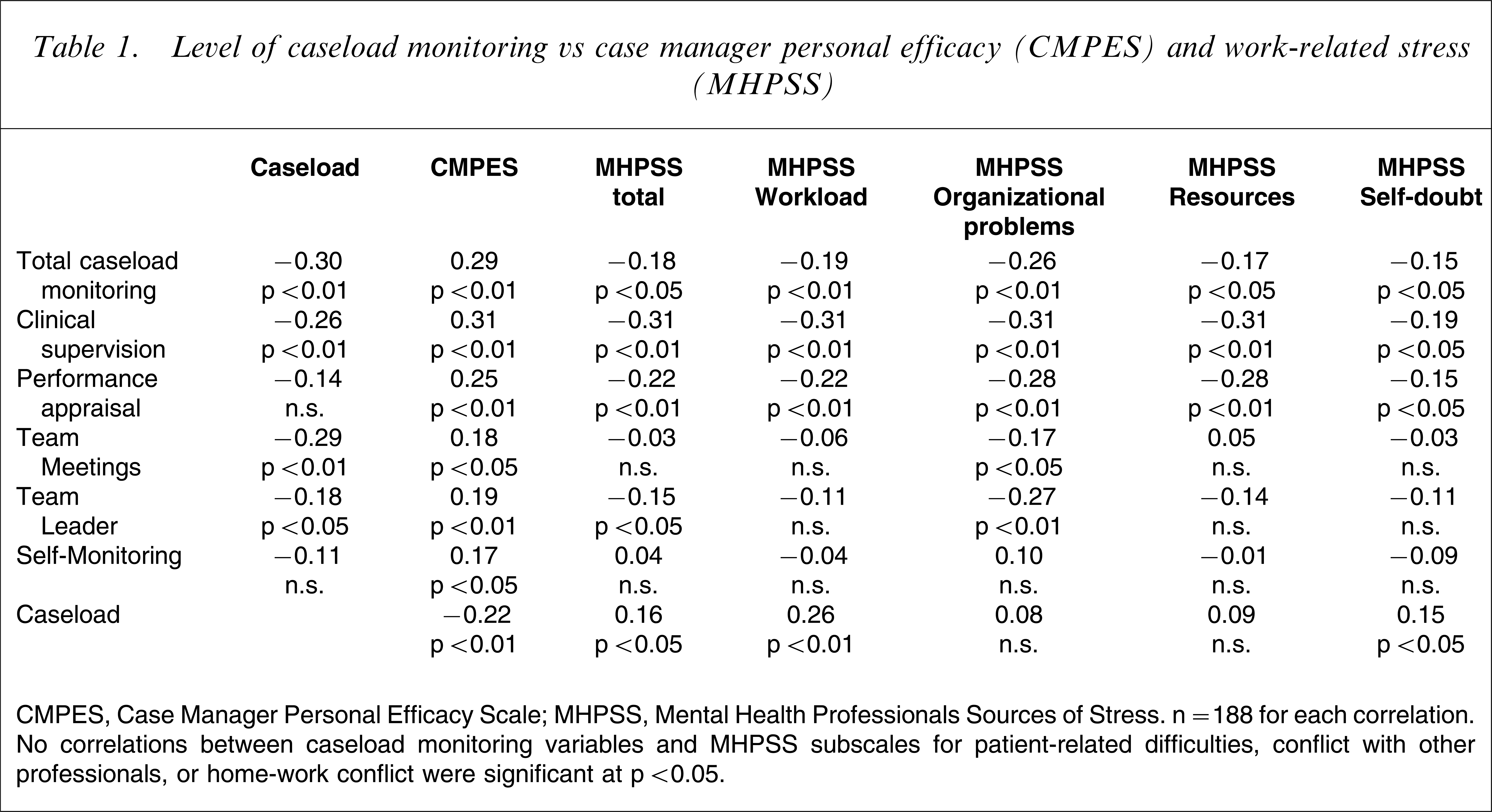
CMPES, Case Manager Personal Efficacy Scale; MHPSS, Mental Health Professionals Sources of Stress. n = 188 for each correlation. No correlations between caseload monitoring variables and MHPSS subscales for patient-related difficulties, conflict with other professionals, or home-work conflict were significant at p < 0.05.
To evaluate the relationship between extent of monitoring and personal efficacy and work-related stress scores, a single score for caseload monitoring was calculated by combining scores for the specific forms of monitoring. A higher total monitoring score was associated with higher case manager personal efficacy as measured on CMPES (r = 0.29, p < 0.01) and with lower work-related stress as measured on MHPSS (r = − 0.18, p < 0.05). Examination of the relationship between total monitoring and MHPSS subscales indicated that the strongest association was not between monitoring and workload (r = − 0.19, p < 0.01) but between monitoring and organizational problems (r = − 0.26, p < 0.01).
To determine whether the benefits associated with higher levels of caseload monitoring were mediated by caseload size, two multiple regression analyses were conducted. In the first analysis CMPES was the dependent variable, caseload was entered as the first independent variable and the single monitoring score was entered as the second independent variable. In the second analysis, MHPSS was the dependent variable, caseload was entered as the first independent variable and the single monitoring score was entered as the second independent variable. The effect of this analysis was to confirm the relationship between caseload monitoring and both personal efficacy (standardized β = 0.25, p < 0.01) and work-related stress (standardized β = − 0.15, p < 0.05). Caseload alone was not significantly associated with either dependent variable in the multiple regression.
Greater use of clinical supervision to monitor caseloads was associated with higher case manager self-efficacy (r = 0.31, p < 0.01) and lower work-related stress (r = − 0.31, p < 0.01). The same patterns of relationship were evident in relation to monitoring of caseload during performance appraisal (r = 0.25, p < 0.01; r = − 0.22, p < 0.01) and monitoring of caseload by the team leader (r = 0.19, p < 0.01; r = − 0.15, p < 0.05), but the strength of the relationship was weaker. Monitoring of caseloads during team meetings (r = 0.18) and self-monitoring (r = 0.17) were both significantly associated with higher case manager self-efficacy scores, but not with work-related stress scores, with alpha at 0.05. All reported relationships remained significant when team leaders were excluded from the analysis. In summary higher rates of caseload monitoring, regardless of form of monitoring, were significantly associated with higher case manager self-efficacy, although some forms of monitoring were more strongly associated than others. Monitoring though clinical supervision, performance appraisal or by the team leader were significantly associated with lower work-related stress.
Discussion
With respect to caseload size, the results suggested that, typically, full-time case managers were working with caseloads of 20 patients. This is well within the range that Intagliata considered necessary for service planning, family support and liaison with other agencies [14]. Caseloads of 20 would normally enable provision of intensive case management to a small number of patients and routine care coordination for the majority.
There was evidence that higher caseloads were associated with increased work-related stress, especially stress associated with workload and professional self-doubt. Higher caseload was also associated with lower case manager personal efficacy. Although a relationship between caseload and stress has not been consistently found in previous research, this finding is consistent with results obtained in a recent Australian study [18]. The finding in this study that higher caseloads were associated with reduced case manager personal efficacy is consistent with results of an earlier study [6] and suggests that this is a robust relationship. Taken together, the present findings concerning the relationship between caseload and both work-related stress and case manager self-efficacy suggest that there are human costs and service delivery costs that increase when caseloads get higher. These findings support the need for active management of caseloads to minimize risk of overload.
Both the expressed preferences of participants and evidence as to the relationship between approach to caseload management, and both case manager self-efficacy and case manager stress support an active role for the team leader, both in allocation of new cases and in monitoring of caseload. Respondents indicated preference for management of caseload through exercise of clinical judgement over application of a formal allocation tool. There was evidence that caseloads were most effectively monitored through individual supervision of case managers.
The present study had two important limitations and it is important to give consideration to these before discussing the implications of the findings. First, a cross-sectional survey provides a weak basis for causal inference. Although the findings are suggestive of a possible causal relationship between caseload monitoring and both lower stress and higher personal efficacy, a differently designed study would be necessary to establish whether or not there was a true causal relationship. Second, the study sample was approximately 15% of the total population of case managers in Victoria's mental health services. Although this was substantially higher than response rates for some online surveys [25] and participants appeared to be broadly representative with respect to the variables measured, caution is required when generalizing findings. There was no evidence, however, that respondents had strongly negative or positive views or that their caseloads or other characteristics were atypical. Of particular importance, given the industrial context of the study, there was no evidence that participants agreed with the position of the industrial organizations who initiated the agreement.
Notwithstanding the need for caution, the results may have implications for the operation of mental health case management services. First, the findings lend support to the value of active monitoring of caseload, especially when this occurs through one-on-one supervision. Even when monitoring does not result in lower caseload, it may assist the case manager both to feel greater control in relation to this dimension of the work and also to know that more senior clinical staff are aware of the situation. Second, the findings do not suggest that the best form of monitoring will necessarily make use of some form of caseload measuring tool or algorithm. Although the use of such tools has been previously recommended [20, 21], and the industrial agreement prescribed their introduction, there was no evidence that they had the widespread support of case managers or that their use reduced work-related stress or increased case manager personal efficacy.
The present findings suggest that caseload management may be most effective when team leaders utilize all available data to monitor the caseloads of mental health case managers and make use of this data within an ongoing supervisory relationship. Caseload management tools may be useful for collection and organization of data for decision making but should not necessarily provide the basis for determination of caseload.
Footnotes
Acknowledgements
Funding and practical assistance for conduct of this study was provided by the Victorian Department of Human Services.