
Abstract
Over the past decade governments, health services and policy makers have emphasised the need for improved community care for patients with severe mental illness. The movement towards de-institutionalisation has seen a burgeoning of differing models of community care with the most notable described as assertive case management [1], intensive case management [2] and the rehabilitation model [3]. Though researchers have identified three broad community care models: standard case management, rehabilitation-oriented community care and intensive case comprehensive care, in practice, differences are difficult to establish [4]. Common to all models is the desire to achieve improved care through increased treatment intensity and low client to clinician ratios.
Evidence for the efficacy of community care has been variable. Most notably the PRiSM studies conducted in England have raised some doubt about the improved outcomes of intensive community-based services compared with standard care in terms of violence toward members of the public, homelessness and suicide [5], measures of disability and symptoms [6], service costs [7], impact on care-giving [8] and user satisfaction and service needs [9]. Mueser et al. [4] have provided a useful review of 75 studies within the area of community care and case management. Of the controlled studies investigated in assertive case management and intensive case management, 61% reported a significant reduction in hospitalisation; 75% reported improved housing stability; 20%, a reduction in time in jail; 50%, a reduction in symptoms; 21% reported increase in positive social functioning and all studies reported moderate improvements in quality of life and cost expenditure compared to a control group.
Nearly all studies in the area of community care have employed a randomised control group design [10–15]. While there are obvious advantages to this type of quasi-experimental design, it makes it difficult for researchers to control for covariate variables which may have some impact on outcome variables of interest such as admission and bed-day rates and more importantly whether differences observed are attributable to intervention type or inherent group differences. Although studies often provide data on the characteristics of experimental and control group cohorts, too few have tested for group equivalence or controlled for differences with covariate designs [16]. Most notably differences in diagnosis, onset of illness, ethnicity, educational level and employment status between experimental and control groups may contribute to group differences in treatment outcome. Other notable concerns include effects of regression towards the mean when selecting patients for inclusion to intensive treatment due to recent high inpatient utilisation [16]. By selecting like for like patients in both treatment and control conditions, researchers can observe the extent to which these phenomena occur. The purpose of this study was to match clients who have received intensive community case management with those with standard community treatment on a number of demographic variables which were thought to contribute to inpatient bed-days. By holding patient characteristics constant, differences observed in outpatient contacts and inpatient bed-day rates could be more confidently attributed to differences in community treatment. Such a design can allow for hypotheses to be tested as to the pretreatment levels of inpatient bed-day rates and outpatient contacts between the two groups. Furthermore, the study employs a naturalistic design where differences between two treatment regimes are analysed as part of normal service delivery activities rather than periodic ‘boutique’ service models supported for the sole purpose of research. Another aim of the study was to investigate whether there was an observed relationship between the number of outpatient contacts made and inpatient bed-days. In addition to this, the investigators were also interested to identify whether the increase in costs in delivering outpatient contacts were offset by a decrease in costs of inpatient care claimed to be delivered by intensive community case management programs [14,17,18].
Method
Match group selection
Eighty patients receiving assertive community case management for at least 1 year with the Fremantle Hospital and Health Service Mental Health Rehabilitation Community Team were selected as the intensive community case management group. Inclusion into the assertive community case management program required patients to have at least two episodes of inpatient care with a prolonged stay of over 30 days within an approved psychiatric hospital at least 1 year prior to receiving treatment, and a recognised psychiatric diagnosis longer than 5 years. All patients had to reside within the Fremantle catchment area which serves 120 000 people in the southwest metropolitan region of Perth, Western Australia. Assertive case management involved the assignment of each patient to a dedicated case manager who was primarily responsible for the overall psychiatric care of the patient. The intensive case management program is a mobile multidisciplinary team, consisting of a psychiatrist, community mental health nurses, social workers and occupational therapists. Nurses and allied health staff occupy non-discipline specific case manager positions. The majority of treatment occurs within the community, including medication management and mental health examinations. The Fremantle Hospital and Health Service Mental Health Rehabilitation Community Team met five out of the six operational definitions of the Intensive Case Management (ICM) model set down by Mueser [4] including (i) low patient to staff ratio of 10:1, (ii) most services provided in the community, rather than in the office, (iii) assignment of patients to a dedicated case manager, (iv) time-unlimited service and (v) most services provided directly by the ICM team and not brokered out. Though the service provides 7 days a week cover, the sixth component of the model of providing 24 h coverage was not offered.
Eighty patients from the Western Australian Health Department Mental Health Information System were matched on ICD-9 diagnosis, age, gender, length of illness, age at first inpatient and outpatient contact, marital status, educational level, employment status, country of birth, year of arrival to Australia and religion. All service data were collected as a requirement of all government mental health services within Western Australia to record service activity. The data have undergone reliability and validity checks to support State and Commonwealth service planning as well as epidemiological research. Matched patients were excluded if their age, onset of illness, length of illness varied more than two years either side of their intensive case management counterpart. Matched patients were also excluded if they received any inpatient or outpatient treatment within the Fremantle catchment area, were not active within the Mental Health Registry 1 year prior to intensive case management treatment or deceased during the study period. No matched control patients had received intensive community treatment since the Fremantle Mental Health Rehabilitation Community Team are the only service within the Perth metropolitan region that meets the Mueser [4] operational definition of intensive case management. Matched control patients received standard clinic base community treatment with higher patient to carer ratio (30:1 vs 10:1). Data were collected on all approved psychiatric hospital inpatient bed-days and outpatient contacts 1 year prior, 1 year after and 2 years after patients receiving intensive case management. Equivalent data were collected for the matched control group subjects with the entry date of their assertive case management cohort to act as pre- and post-treatment collection dates. Group equivalence on the matching variables were tested using Chi-squared and analysis of variance. Intensity of assertive community treatment was calculated by dividing the number of outpatient contacts by 52 weeks to give a score of average weekly contacts.
Due to the quasi-experimental nature of the design the following a priori hypotheses were made. The first hypothesis was that there would be no significant difference between assertive case management and standard treatment patients in inpatient bed-days and outpatient contacts 1 year prior to assertive community case management. An analysis of variance was performed to test this hypothesis. The second hypothesis was there would be an interaction effect between group membership and inpatient bed-days and outpatient contacts over time favouring a decrease in inpatient bed-days and an increase in outpatient contacts for the ICM group. To test the second hypothesis a within/between-subjects repeated measures analysis of variance was performed on the inpatient bed-day and outpatient contacts, 1 year prior, and 1 and 2 years after intensive case management.
Treatment cost calculations
In order to calculate the costs of each method of treatment, average inpatient bed-day rates and outpatient episode costs were used from the Mental Health Classification and Service Costs (MH-CASC) Project [19]. The researchers in the present study decided to use this source since it provided a nationalised standard cost for inpatient and outpatient services across Australia. This project involved calculating standardised operational costs across 22 integrated mental health services, with sites in all states, involving 30% of the Australian specialised mental health workforce and 15 000 consumers to derive cost structures. The average costs included salaries and related costs for clinical staff as well as overhead and administrative infrastructure expenditure. These were derived from the cost centres of each participating service in the MH-CASC study in which Fremantle Hospital and Health Service was a part. The report calculated an average inpatient cost per treatment day of $331. The outpatient contacts were calculated by dividing the average community treatment costs of $94 per day by two since the Mental Health Information System of Western Australia deemed that each outpatient contact was defined to last no longer than 4 h equating to half a working day. Costings were generated for each time period between the treatment groups on outpatient contacts and inpatient bed-days. Cost differentials were calculated by observing the difference between overall inpatient bed-day costs and costs of overall outpatient contacts. Total operational costs were calculated by summing both outpatient and inpatient cost regimes for each treatment group. Costs are calculated in Australian dollars. Paired two-tailed t-tests were used to determine significantly different costs across the study period for each treatment type.
Results
Patient characteristics
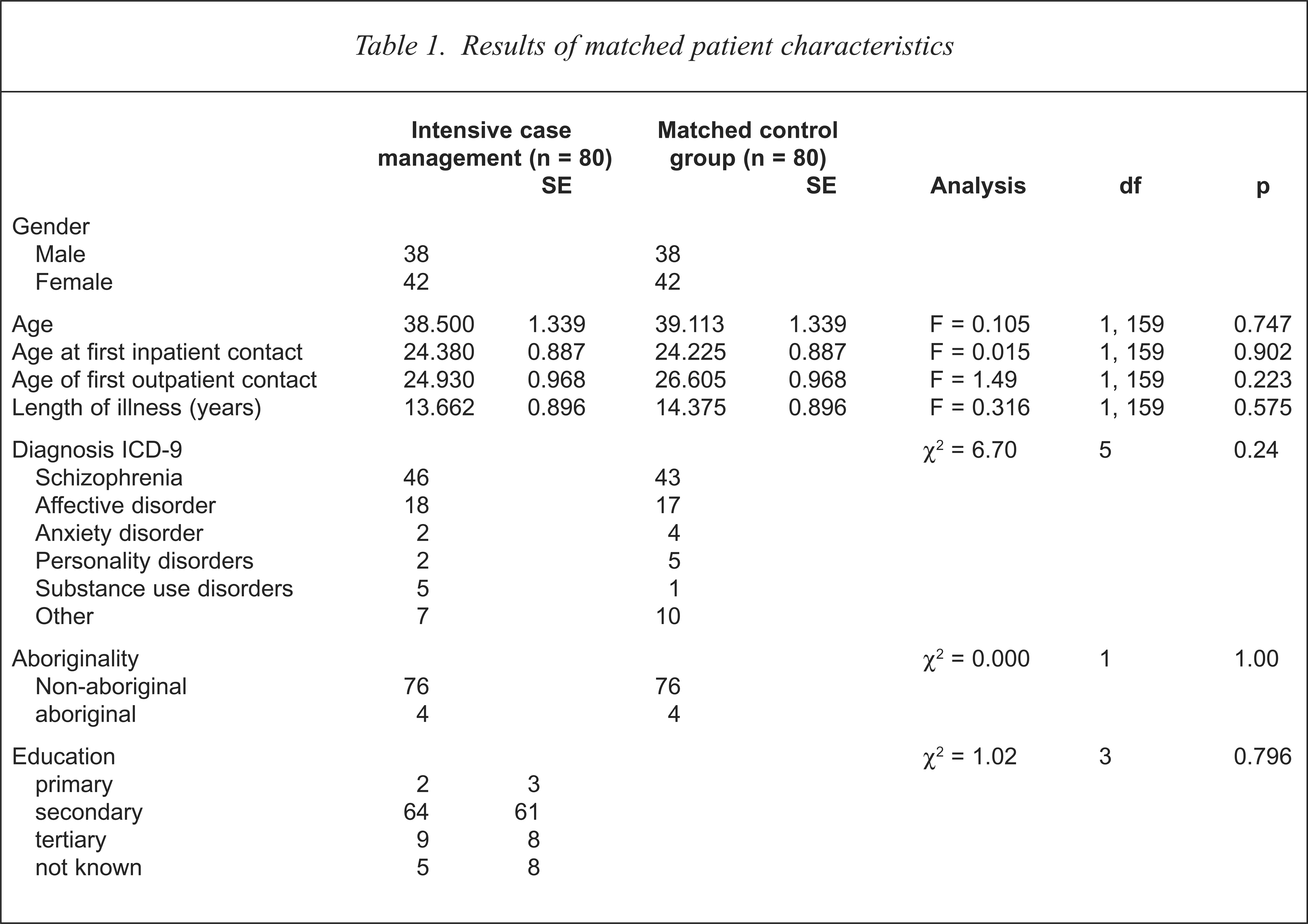
Of the 80 patients receiving intensive case management 57% had an ICD-9 diagnosis of schizophrenia. 22% with affective disorders, 6% with substance use disorders, 3% with personality disorders, 3% with anxiety disorders and 9% with other nonspecific diagnoses. The Chi-squared test indicated matched group equivalence in diagnosis (χ2 = 6.70, df = 5, p = 0.24) (refer to Table 1). Male patients represented 47.5% (n=38) while females represented 52.5% (n = 42) of the sample. Gender (χ2 = 0.00, df = 2, p= 1.00), age (F = 0.105, df= 1, 159, p = 0.747), age at first inpatient contact (F = 0.015, df = 1, 159, p = 0.902), and outpatient contact (F=1.49, df = 1, 159, p = 0.223), as well as length of illness (F = 0.316, df = 1, 159, p = 0.575), were statistically invariant between ICM and matched control patients. Chi-squared tests identified equivalence in proportional cell representation between ICM and matched control patients on marital status (χ2 = 3.89, df = 5, p = 0.564), educational level (χ2 = 6.24, df=8, p = 0.620), employment status (χ2 = 4.46, df=6, p = 0.614), religion (χ2 = 4.46, df = 11, p = 0.614), aboriginality (χ2 = 0.00, df = 1, p = 1.00), country of birth (χ2 = 24.44, df = 25, p = 0.494), and year of arrival to Australia where indicated (F = 0.008, df= 1, 45, p = 0.927).
Results of matched patient characteristics
Inpatient bed-days and outpatient contacts
Test for pretreatment equivalence
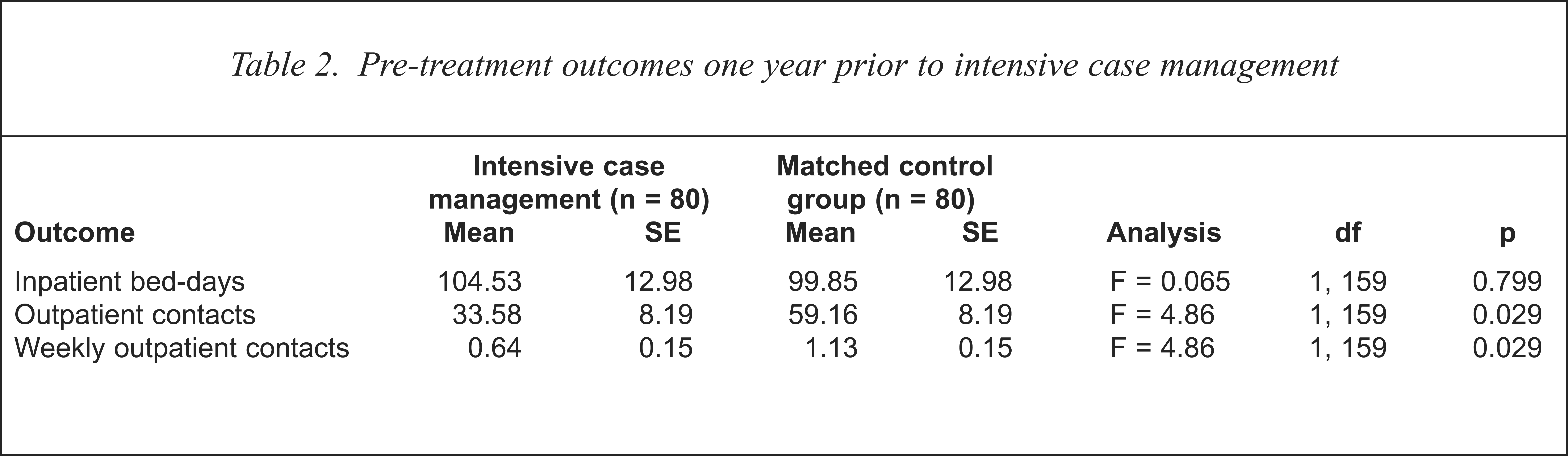
Analysis of variance confirmed that inpatient bed-days were equivalent between ICM and matched control patients indicated (F = 0.065, df = 1, 159, p = 0.799) (see Table 2). Outpatient contacts were significantly different in the pretreatment period (F = 4.86, df = 1, 159, p = 0.029) indicating matched control subjects having 57% more outpatient contacts than ICM patients. It could be argued that inpatient bed-days are a more reliable indirect measure of chronicity than outpatient contacts. The analysis of variance was not significant (F = 0.065, df = 1, 159, p = 0.799) indicating that inpatient bed-days were equivalent between ICM and matched control patients. Although when demographic variables were held constant between the two groups before treatment, the ICM group appeared to have significantly lower outpatient contacts (F = 0.646, df = 1, 159, p = 0.029). Even when inpatient treatment proved equivalent, it appears that the ICM group were treated less assertively before intensive case management than their matched control cohorts. This may be due to the fact that most ICM patients were members of an older psychiatric hospital in the south-west metropolitan region of Perth prior to ICM that may have emphasised more traditional notions of psychiatric care.
Pre-treatment outcomes one year prior to intensive case management
Interaction of group membership and treatment outcome
Inpatient bed-day rates
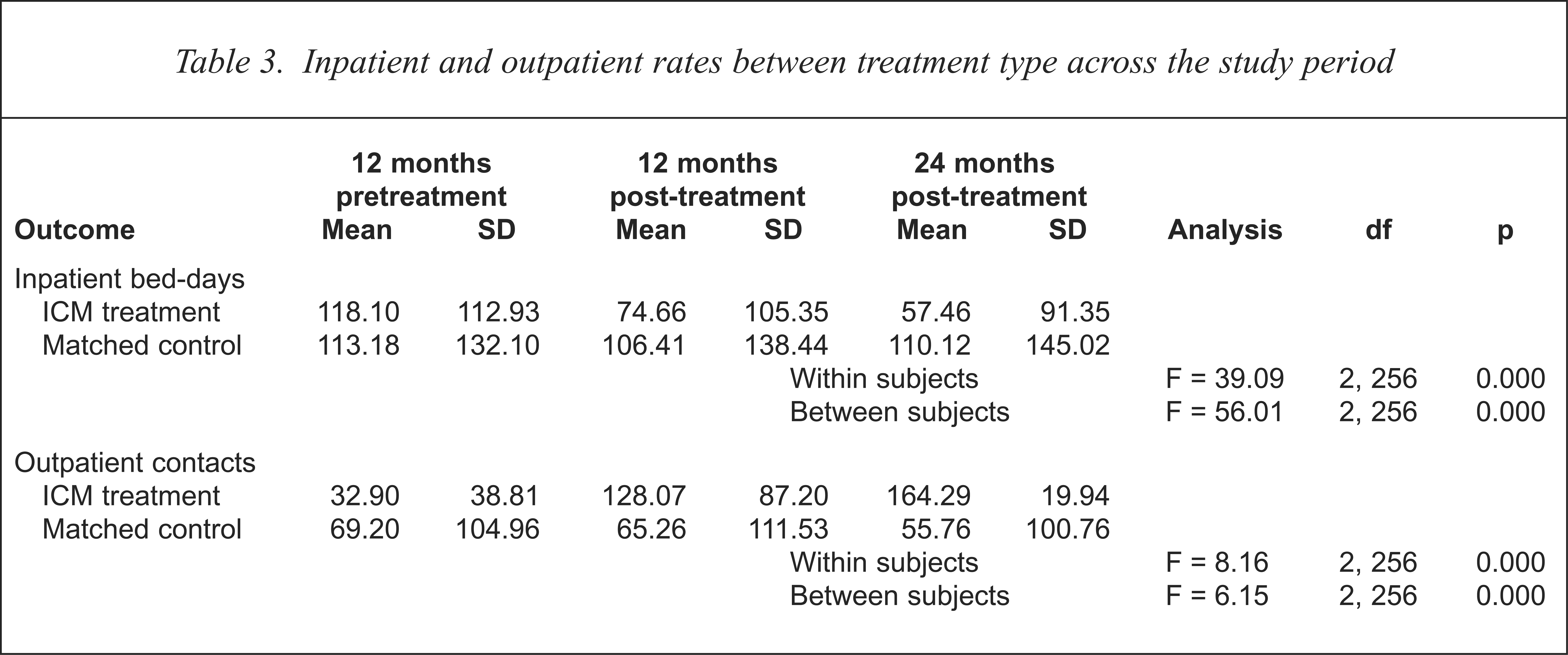
The repeated measures analysis of variance over the 3 year period ran list-wise deletion of data resulting in 15 patients from the ICM group being dropped from the analysis. Their corresponding matched control group subjects were also dropped leaving a matched group of 65 subjects in each group expanding 1 year preceding ICM treatment and 2 years after ICM treatment. The Pillais multivariate test of significance was significant (F = 6.28, df = 2, 127, p = 0.002) for inpatient bed-days. Within-subject effect revealed a significant difference with bed-day rates (F = 8.16, df = 2, 256, p = 0.000) as well as a significant interaction effect between group membership and inpatient bed-days (F = 6.15, df = 2, 256, p = 0.002) (see Table 3). Univariate F-tests revealed a significant difference in inpatient bed-day rates between 12 months prior to ICM treatment and 12 months after ICM treatment (F = 12.10, df = 1, 128, p = 0.001) while changes between 12 months and 24 months after ICM treatment were not significantly different (F = 2.06, df = 1, 128, p = 0.153). Post hoc analysis revealed that the ICM treatment group were different between 12 months before and after ICM treatment (t = 3.20, df = 1, 78, p = 0.002) while inpatient treatment remained unchanged for the matched control group (t = 0.77, df = 1, 78, p = 0.439). Observation of the means (see Table 3) shows a significant reduction in inpatient bed-days for the ICM group from an average of 118 bed-days to 74 while the matched control group remained statistically the same at 113 at pretreatment to 106 at 12 months after treatment.
Inpatient and outpatient rates between treatment type across the study period
Outpatient contacts
The Pillais multivariate test of significance was significant (F = 61.09, df = 2, 127, p = 0.000) for outpatient contacts. Within-subject effect revealed a significant change with outpatient contacts (F = 36.09, df = 2, 256, p = 0.000) as well as a significant interaction effect between group membership and outpatient contacts (F = 56.01, df = 2, 256, p = 0.000). Univariate F-tests revealed a significant change in outpatient contacts both between 12 months prior to ICM treatment and 12 months after ICM treatment (F = 57.97, df = 1, 128, p = 0.000) and between 12 months and 24 months after ICM treatment (F = 9.16, df = 1, 128, p = 0.003). Post hoc analysis revealed that the ICM treatment group reported a significant increase in outpatient contact between 12 months before and after ICM treatment (t = 9.76, df = 1, 78, p = 0.000) while outpatient contacts remained unchanged during the same period for the matched control group (t = 0.64, df = 1, 78, p = 0.522). Significant increases in outpatient contacts continued for the ICM group between the 12 months and 24 months of ICM treatment (t = 2.64, df = 1, 64, p = 0.010) while within the same period the matched control group remained unchanged (t = 1.47, df = 1, 64, p = 0.146). Average weekly outpatient contact increased for the ICM group from one contact per two weeks to 2.4 contacts per week. This continued to increase to 3.1 contacts per week in the second year of treatment. Average weekly outpatient contacts for the matched control group subjects remained constant at 1.3 in the year preceding ICM treatment, 1.25 contacts in the year after treatment and 1.05 contacts in the 24 months after ICM treatment.
Treatment costs
A steady reduction in total operational costs was observed in favour of the ICM treatment group with savings totalling $1156 244 over the 2 years treatment period (see Table 4). Savings for the matched control group were also observed over the same period of $326 809. The differences in treatment costs between the 65 subjects in each treatment is $396 111 in the first 12 months of treatment and $801 475 after 24 months of treatment favouring the ICM treatment in both time periods. Although the total cost of outpatient contacts dramatically increased from $126 289 to $461 023 in the first 12 months of treatment for the ICM group (t = 9.76, df = 1, 79, p = 0.000) this was offset by a $988 035 decrease in inpatient costs. Over the same period, reductions in inpatient costs were $219 122 for the matched control group. Inpatient costs were significantly reduced for the ICM group between 12 months prior and 12 months after ICM treatment (t = 3.20, df = 1, 79, p = 0.002) and between 12 months prior and 24 months after ICM treatment (t = 4.22, df = 1, 79, p = 0.000). No significant reductions for the matched control group were recorded over the same time period.
Costings ($) between treatment types for inpatient and outpatient services across study period
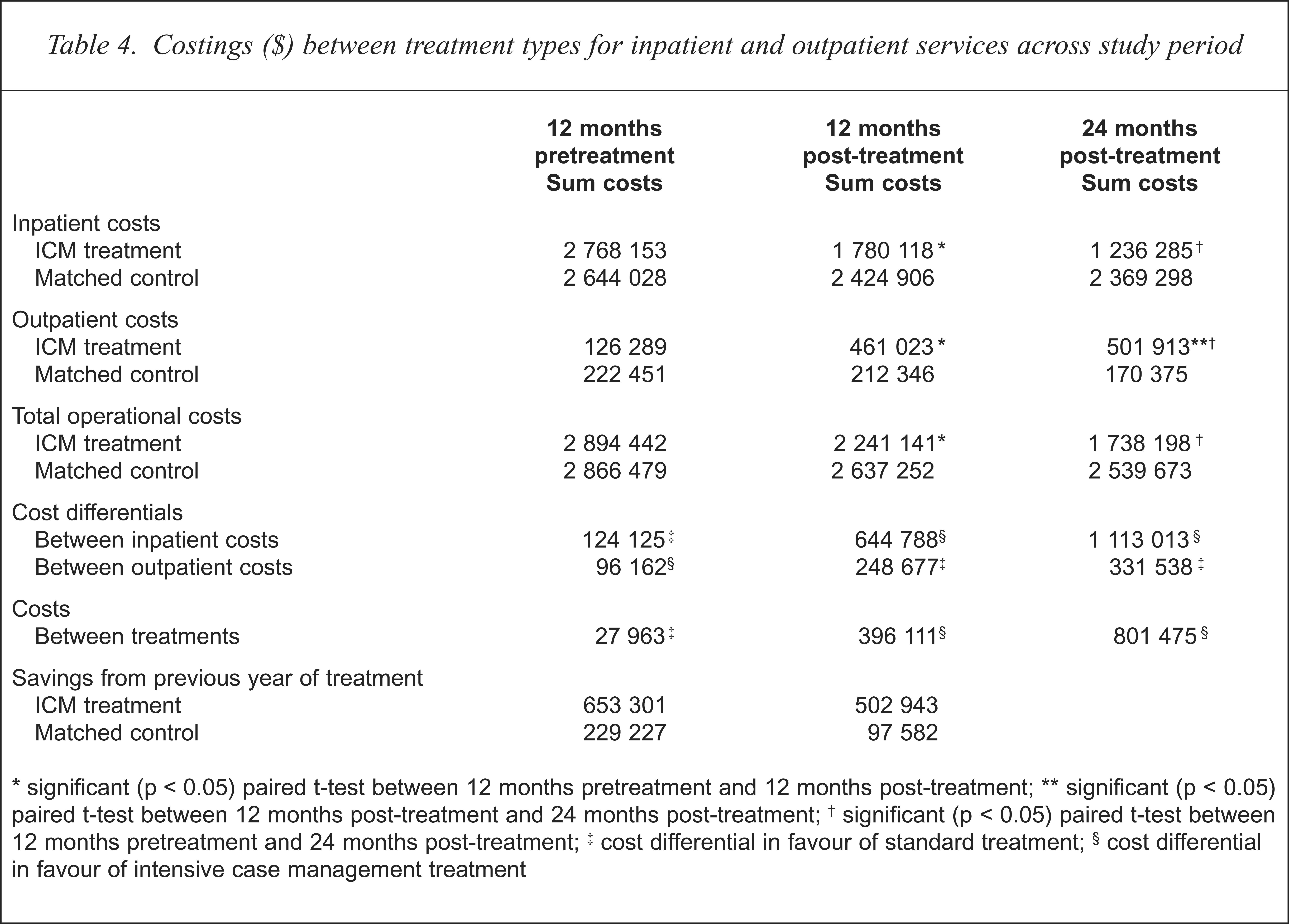
significant (p < 0.05) paired t-test between 12 months pretreatment and 12 months post-treatment;
significant (p < 0.05) paired t-test between 12 months post-treatment and 24 months post-treatment;
significant (p < 0.05) paired t-test between 12 months pretreatment and 24 months post-treatment;
cost differential in favour of standard treatment;
cost differential in favour of intensive case management treatment
Discussion
The study was able to demonstrate that ICM can be efficacious in reducing inpatient service utilisation and cost effective when compared with standard community treatment received by subjects equivalent or matched on diagnosis, age, gender, length of illness, age at first inpatient and outpatient contact, marital status, educational level, employment status, country of birth, year of arrival to Australia and religion. It is possible that other extraneous variables that the authors did not control for may have contributed to differences between the two groups. However, of the eight control variables matched for equivalence, none of them proved variant and they account for the majority of diagnostic and social variables which may contribute to possible group difference. When outpatient contacts are significantly increased as part of the ICM model, significant reductions are experienced with inpatient bed-day rates. The cost of increasing outpatient services to the chronically long-term mentally ill can be offset by significant reductions in inpatient service utilisation. In the case of this study when 65 subjects received three times as many outpatient contacts their inpatient contacts reduced significantly by 36.8%. When outpatient contact remained at around one contact per week as observed for matched control subjects and remained stable over the 3 year study, inpatient contacts reduced insignificantly by 6% in the first 12 months and rose by 3% in the 24-month period. The cost differential between the two treatment regimes calculated at $801 475 in favour of ICM treatment.
The study set out to observe whether holding certain demographic and diagnostic variables constant in a matched selection process produce equivalent pretreatment levels of inpatient and outpatient levels of service utilisation. The study confirmed that when the above-mentioned variables were matched or held equivalent both ICM subjects and matched control subjects had statistically equivalent pretreatment levels of inpatient bed-day rates. Although outpatient contacts were lower in the ICM subject prior to treatment this may be due to the membership of these subjects to a more traditionally oriented psychiatric hospital service. The evidence suggests that when outpatient contacts are steady at one outpatient contact a week over the 36-month trial period no significant gains were recorded in inpatient service utilisation. Increasing outpatient contacts between 3 and 4 contacts a week via the ICM model demonstrated significant improvements in continued reduced inpatient service utilisation. In this instance this paper supports previous investigations [14,17,18] arguing that the increase in outpatient cost expenditure can be offset by a significant reduction in inpatient costs.
Effectiveness of ICM models are best observed when patients display a history of high service utilisation [20]. It is important that ICM models have strict entry criteria which includes high service utilisation as part of entry requirements. Gains are best observed among those patients that have proven to be recidivistic and difficult to treat. Cost effectiveness may erode when less stringent entry criteria occurs and patients are placed on short-term intensive treatment regimes. This study shows that although gains can be experienced within the first 12 months of treatment, these effects can accumulate as subjects remain in the ICM program up to the 24-month period. Although some studies have shown that switching subjects back to less intensive treatment leads to an increase in hospital days [21], other studies have suggested that short-term ICM treatment can be beneficial [22]. Further research is required in the area to determine the longitudinal effects of ICM models when patients are returned to more standard treatment methods. The future of research in the area certainly lies not in establishing the efficacy of ICM models but in identifying what components of treatment contribute to significant gains and how long these effects continue once treatment is withdrawn or continued [4].