
Abstract
For many years it has been understood that case managers must often provide direct clinical services, [1–3]. These clinical services delivered in a community setting have different elements to similar services provided in a hospital environment. The components of case management have been described as (i) initial phase: engagement assessment and planning; (ii) environmental interventions: linkage with community resources; (iii) patient interventions: intermittent individual psychotherapy, living skills training and psychoeducation; and (iv) crisis intervention and monitoring [4]. Recent research has identified the core functions required of case managers working in public community mental health services which include: (i) individual psychotherapy and/or counselling; (ii) assessment; (iii) psycho-education; (iv) crisis intervention; (v) monitoring daily living skills; (vi) monitoring medication; (vii) support; (viii) activities of daily living; as well as (ix) liaison with other care agencies [5].
The goals of case management have been determined as: (i) keeping people in contact with services [6]; (ii) earlier, less frequent and shorter hospitalisations [7,8]; and (iii) improved quality of life, self-care skills and social functioning of the clients [7,9].
Researchers have observed that the policy of continuing community care by case managers has a great number of benefits but also has some difficulties [10–12]. One of the particular difficulties experienced by case managers working in community settings was the level of intensive care required when a client became acutely unwell [13].
Problems for staff
Mental health professionals are subjected to similar organisational stressors to other workers. They also face additional emotional strain by the very nature of their professions in dealing with troubled persons often over extended periods of time. [14, p. 83]
Moore and Cooper stated that only carers, who are well, are able to provide the ‘best care’ [14]. Case management has been found to have high levels of job stress by a number of researchers [15–17]. Emotional exhaustion, depersonalisation, larger case load size and General Health Questionnaire levels above norms for the general population were determined in community mental health workers [16,17]. The levels of morbidity in case managers were linked to increased client symptomatology [16].
For staff working in community mental health settings there are a number of risks that must be addressed. Clients who have been in long-term institutional care may not wish to live outside the institution, or may not be able to adapt to it [18]. Working in community settings can place a great deal of direct client responsibility on case managers, which may expose weaknesses in the skills of inexperienced or inept staff [19]. The stress factors of working outside a hospital setting and working with clients suffering from mental illness were closely associated with the levels of burnout [20]. It has also been noted that mental health professionals are ‘prime targets for disillusionment, distress and burnout’ [21, p. 724].
Most of the studies of case management have examined models of management and their effectiveness, often on a cost–benefit basis. Several patient characteristics have been associated with fluctuation in treatment costs [22]. Very little attention has been paid in studies of case management to factors such as duration of illness, nature of adjustment, level of social relationships, presence of affective symptoms and level of cognitive functioning [23]. Many of these identified patient characteristics may also be associated with increased level of workload burden for case managers.
The World Health Organization [24] has determined that important factors related to stress and burnout in the helping professions are the inability to help an acutely distressed client and a lack of observable progress with patients (p. 11). Some of the organisational factors that may cause stress are: (i) caseloads consisting predominantly of extremely difficult patients; (ii) role or case overload; (iii) lack of a sense of impact on and control over one's work situation (p. 11).
In an effort to establish an appropriate level of professional supervision for case managers, it was believed that the reasons for the difference in workload demand had first to be detected. The level of workload burden and the professional capability of a case manager are closely linked to the number of cases effectively managed. Effective case management is in turn related to the equitable allocation of cases to each case manager.
Rationale
Allocation of cases for case management at the Royal Brisbane Hospital Integrated Mental Health Service (RBHIMHS) has generally been on an ad hoc basis, often determined by the number of cases currently being managed. Problems that have emerged in this area are as follows.
How to fairly allocate cases in a case management system. How to ensure consistency of case management service when the case managers may have different professional backgrounds and training. How to quantify the difficulty and clinical needs of individual clients and identify heavy service users appropriately. How to prevent work overload and possible resultant ‘burnout’.
Objective
The purpose of the study was to develop a single instrument that would be able to accurately determine the level of work load burden imposed on case managers by the level of their clients needs.
Process of development of a new Clinical Load Monitoring Tool
Extensive literature searches on Winspirs 4.0 (Silver Platter, Norwood, MA, USA), using Index Medicus/MEDLINE, PsycLIT and the Cochrane Library as well as Medscape (http://www.medscape.com), utilising such phrases as ‘case management’, ‘mental illness’, ‘community care’, ‘clinical care’, ‘workload’, ‘burnout’ and ‘stress’ revealed that no information had been published on the development of a tool to identify components of a case manager's clinical load that enabled monitoring of their workload burden.
A single clinical assessment tool developed by the Chatswood Community Mental Health Team, Sydney, New South Wales (unpublished) had been used at the Integrated Mental Health Service previously on a related project. It was decided to use this tool as a base and modify it to make it more comprehensive and objective. A consultation process within the RBHIMHS was undertaken to determine what adjustments were required. The adjusted tool was piloted, reviewed and definitions altered to suit the needs of the service and case managers. The draft document was circulated widely to other services for comment. Each service advised that they had particular needs for their respective programs and the tool was similarly piloted, reviewed and adjusted to suit their specific requirements.
The instrument has three primary components which are: (i) frequency of face-to-face contact; (ii) extent of clinical complication; and (iii) the need for community liaison. The components of the scale and definitions that are issued each month with the data gathering sheet are available from the correspondence author on request.
During the course of development of the Clinical Load Monitoring (CLM) tool, case managers were surveyed to determine the ‘other’ duties in which they were involved. These duties ranged from attending meetings with other services, professional development programs to educational programs conducted by government and non-government agencies. This survey was administered in conjunction with the introduction of the CLM in an attempt to clarify the percentage of time actually spent on case management.
Data gathering
Data on clinical factors and community liaison were gathered from 41 case managers from the two continuing care teams each month over a period of 15 months. Data were gathered at the end of each calendar month with a submission time within 10 working days after the end of the month. Case managers were also requested to indicate the percentage of time spent on case management for the month. The Case Load Score was then calculated by multiplying the sum of community liaison figure and clinical factors number by the frequency score: frequency X [clinical factors + community liaison score] – minimum score of 2 (1 X [1 + 1]) – maximum score of 35 (5 X [4 + 3]). For more information refer to Table 1.
Sample Score Calculation
Case Load Scores for each client in a case manager's list are summed to give a clinical load number. To facilitate standardisation of the clinical load number to enable comparison of scores, a nominal load score was calculated by extrapolating the clinical load to a value equalling 100% of time spent on case management. Data were then entered in the Statistical Package for Social Services (SPSS) [25] for analysis. Reports were issued to each discipline senior, team leaders, service director and district manager monthly.
Results
There was little variation over time in the average numbers of clients case managed, the percentage of time spent on case management or the mean nominal load scores in the two continuing care teams which cover epidemiologically similar designated geographical areas within the District. A comparison of team data revealed some minor fluctuations in nominal load scores each month. For individual case managers, the percentage of time spent on case management ranged from 15% to 94%. The number of clients case managed ranged from 4 to 33. The nominal load scores showed a similarly diverse range from 36 to 1015.
The monthly average number of clients case managed by each team ranged from 11 to 19 with some variation between each team. The average percentage of time each team spent on case management ranged from 44.79% to 66.23%. The calculation of a nominal load score enabled more equitable distribution of caseloads to each of the two continuing care teams. Comparison of the number of clients being case managed or the percentage of time spent on case management did not give an accurate representation of the level of workload burden (refer to Table 2).
Variations in Average Nominal Load Scores of the Northern Team and the Southern Team
Discussion
Prior to the introduction of the clinical load monitoring tool, the number of clients being case managed by each team may have been the benchmark for ‘heavy work load’. The data gathered in this pilot project has revealed that it is the various aspects of the client needs that contribute to the level of workload burden experienced by each case manager.
Benefits
One of the main benefits of the tool has been the equity of allocation of caseloads. An additional benefit is that in the review of cases by either the Team Leader or the discipline senior, the case manager has hard data that is comparable with all other case managers in the service. Stress levels have been able to be clearly explained to case managers in supervision as being related to the workload burden that they are carrying, thereby reducing the risk of burnout. Less-experienced staff may benefit from the use of a system that allows them to identify the level of clinical load in each client and to assist them in developing appropriate monitoring techniques to allow them to be productive, healthy workers.
Analysis of the database has determined the levels of low, medium and heavy service users in each of the two continuing care teams. Each client who records heavy service use each month is recorded in a separate database and if such use continues for a 3 month period, the client is then reviewed for transfer from the continuing care team into the Mobile Intensive Treatment Team. Those clients who have recorded a load score of fewer than 10 for 3 consecutive months are further investigated for discharge from case management. Such investigation includes the completion of the Health of the Nation Outcome Scale [26] by the case manager and special review at the team meeting.
The differences in the number of clients being case managed by each of the two continuing care teams is evident in Figure 1. When the variable of workload burden is considered and a nominal load score calculated, the variation between the teams is greatly reduced. In Table 2 it may be seen that a team with fewer average cases and spending equal or less time on case management may be just as effectively engaged as one that has a greater number of allocated cases to manage with a larger percentage of time devoted to case management.
Average number of clients case managed by the Northern Team (▪) and the Southern Team (♦).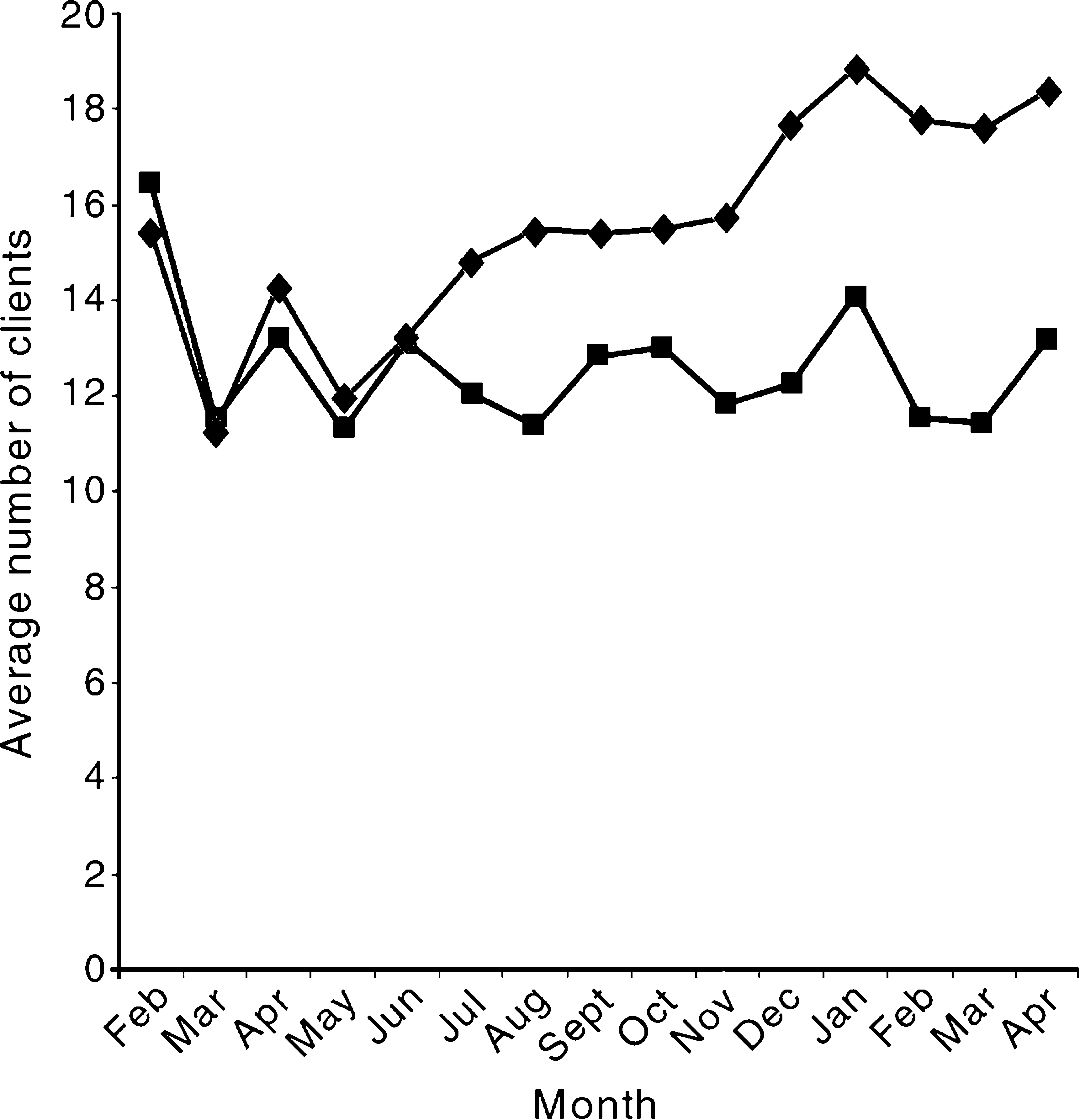
Observations
Since the introduction of the CLM tool some 18 months ago, some observations have been made regarding the impact of its use by both management and clinicians.
Management
Senior management has begun to use the CLM in planning allocation of staff and resources to teams. Team leaders and discipline seniors are cooperating in the allocation of cases using the CLM as a baseline for distribution of additional cases to case managers.
The identification of cases for discharge has been assisted by the classification of ‘low service users’ through the CLM. Those clients who scored below 10 over a period of 3 consecutive months were further investigated for discharge from case management. ‘Heavy service users’ identified through the CLM have been transferred to intensive treatment areas.
Clinicians
The clinicians seem more able to identify those clients who place a heavier work load burden on them and use this knowledge to prioritise their work time management. The regular reporting of their clinical load appears to have had a level of positive reinforcement for the case managers and their initial reluctance about using the tool had diminished greatly.
Future directions
The next phase of the use of the clinical load monitoring tool has been commenced at the RBHIMHS. The component of time has been introduced in the data gathering. Time has been defined by five categories ranging from a face-to-face contact of less than 15 minutes, which would rate 1, to more than 2 h per contact, which would rate 5. All time components should include travel time to and from the client's place of residence.
The CLM tool will be used in all future allocation of cases for case managers. It will be used to determine the clients who are heavy service users who may require more intensive case management or special programs. Similarly, clients who may be discharged from case management will also be able to be identified using this reporting measure.
The tool should also be used to determine the level of workload burden that a case manager is able to carry. If this process is carried out at a personal and a professional level the risk of burnout should be greatly reduced. Each case manager should be able to recognise, from perusing their report sheet and clearly identifying their levels of work-related stress, which of the clients being case managed is contributing to that burden. Supervision in the workplace should also link the reported data with the monitoring processes undertaken.