
Abstract
Within developed countries, case management has become a dominant paradigm for the delivery of public mental health services. This is despite a lack of clear consensus as to what case management entails [1] along with doubts that have been raised about its overall clinical efficacy and cost effectiveness [2]. Case management is integrally linked to de-institutionalization because it aims to provide continuity of community-based care [3]. In so doing it reduces the exposure of both the person suffering a mental illness and the wider community to any adverse consequences of less restrictive treatment. Marshall's meta-analysis [2], while raising doubts about the clinical impact of case management, did confirm that it succeeded in providing continuity and thus fulfilled a major public policy objective.
Ideally, case management provides a single point of contact with services, a means of monitoring mental state and psychosocial functioning and a process by which the person suffering a mental illness can access a wide range of services [4]. Research conducted in Australia [5] determined that the core functions of case managers working in community mental health services included: individual psychotherapy/counselling, assessment, psychoeducation, crisis intervention, monitoring daily living skills, monitoring medication, support, building daily living skills and liaison with other care agencies.
Health professionals such as social workers, nurses, psychologists, doctors and occupational therapists characteristically work within the model sometimes termed ‘clinical case management’ [4–6] to distinguish it from a brokerage model [1], in which the only role of the case manager is to purchase and/or arrange access to services.
The extent to which case management can fulfil public policy imperatives is dependent on the capacity of case managers to undertake their core roles. These include regular and flexible contact with clients, contact with family or other carers, liaison with other service providers and maintaining continuity of contact when the client is being treated in hospital. The amount and nature of contact necessary will be influenced by the particular circumstances and needs of each case. However, there is evidence that the total caseload of the case manager (i.e. the number of clients for whom he/she has case management responsibility) impacts on role performance. Intagliata [7] for example recommends caseloads of 20–30 clients where a broad range of roles is required.
Baker and Intagliata [8] refer to research indicating that as caseload increases, contacts become less frequent and approach to work becomes more reactive. It has less of a rehabilitation focus and the proportion of time spent on paperwork increases. Onyett [9], in his discussion of the Bridge Project, noted that as caseload increased, client contacts became more impersonal.
King et al. [10] analyzed the self-reports of mental health case managers around Australia. This study showed that not only is general case manager selfefficacy a function of caseload, it is clear that case managers report specific roles as being especially sensitive to caseload. These include timely response to client needs, documentation of work, receptiveness to urgent client needs, contact during hospital admissions, home visits and advocacy.
This study also confirmed earlier findings [11] that higher caseloads are not strongly associated with psychological stress or ‘burnout’. This does not mean that case management is not a stressful occupation; rather, it suggests that stress is caused by factors other than the size of a case manager's caseload. As the caseloads get higher, case managers make adaptive responses by doing less with each case. This data therefore lends support to the claim that there is a dose–response relationship between therapist time and effectiveness [8], [12].
However, while there is evidence of a relationship between caseload and case manager role performance, the relationship between caseload and client outcome is less clear. The Fort Bragg study [13] failed to find measurably superior clinical or psychosocial outcomes for young people receiving intensive case management and continuous care compared with conventional services. Studies that have compared the clinical impact of low caseload, high intensity case management based on the PACT model, with standard case management have also shown, at best, modest effects [14–16]. Caseload when determined by a crude and simplistic index of clients per case manager may not predict client outcome at all. This examination of factors that contribute to caseload is in part predicated on the expectation that more meaningful determination of caseload will result in more effective exploration of the relationship between caseload and client outcome.
However, study of client outcome is not the only reason for measuring caseload accurately. Insofar as caseload is relevant to case manager role performance, it is also relevant to budget and funding issues. Regional funding of psychiatric services is increasingly based on measurable parameters within the population [17], [18]. However epidemiological data is meaningful with respect to service provision only if it is possible to also quantify the service response characteristics of the workforce. In the area of community mental health, this means being able to identify the kinds of services a case manager can deliver, given a specified caseload.
In practical terms, planners and administrators are generally able to obtain morbidity data for the relevant population and to identify service standards. However, the number of case managers required to meet service standards within this population cannot currently be ascertained because of inadequate understanding of the impact of caseload.
A third reason for accurate measurement of caseload is fairness and equity in distribution of workload. It may also be relevant to the evaluation of staff performance and determination of workforce efficiency. Team leaders and service managers need some basis for rational assignment of new cases and for determining whether or not a case manager is overloaded. The facility with which a case manager addresses role demands is a potential measure of efficiency. While we suspect that total caseload predicts role performance, we know little about the practices that enable effective role performance with higher caseloads. Setting standards based on caseload alone is probably inadequate unless staff have an incentive to exceed those standards either by successfully managing a higher caseload or by exceeding role performance standards.
Caseload management is therefore an issue crucial to all players within the community mental health movement. To clients, it will directly affect the style and focus of their treatment experience but may or may not impact on outcome. To professionals it determines their work experience, the balance of proactivity versus reactivity and their sense of their own general efficacy. For mental health services, caseload has the potential to affect response to public policy and service standard demands, client satisfaction, staff satisfaction, team cohesion and total service costs.
The relevance of caseload to client care and to service planning has been long recognized, but there is only one published account of caseload measurement in mental health case management. Meldrum and Yellowlees [19] described a project at a Brisbane mental health service, in which case manager workload was determined taking into account contact frequency, client factors contributing to work difficulty and community liaison demands associated with the client. They reported that the calculation of workload helped to inform discharge planning, by identifying low need clients, and was accepted by clinicians after initial reservations. The only other attempt to develop a method to determine caseload in mental health concerned the work of psychiatrists rather than case managers [20].
What variables may be considered in determining caseload?
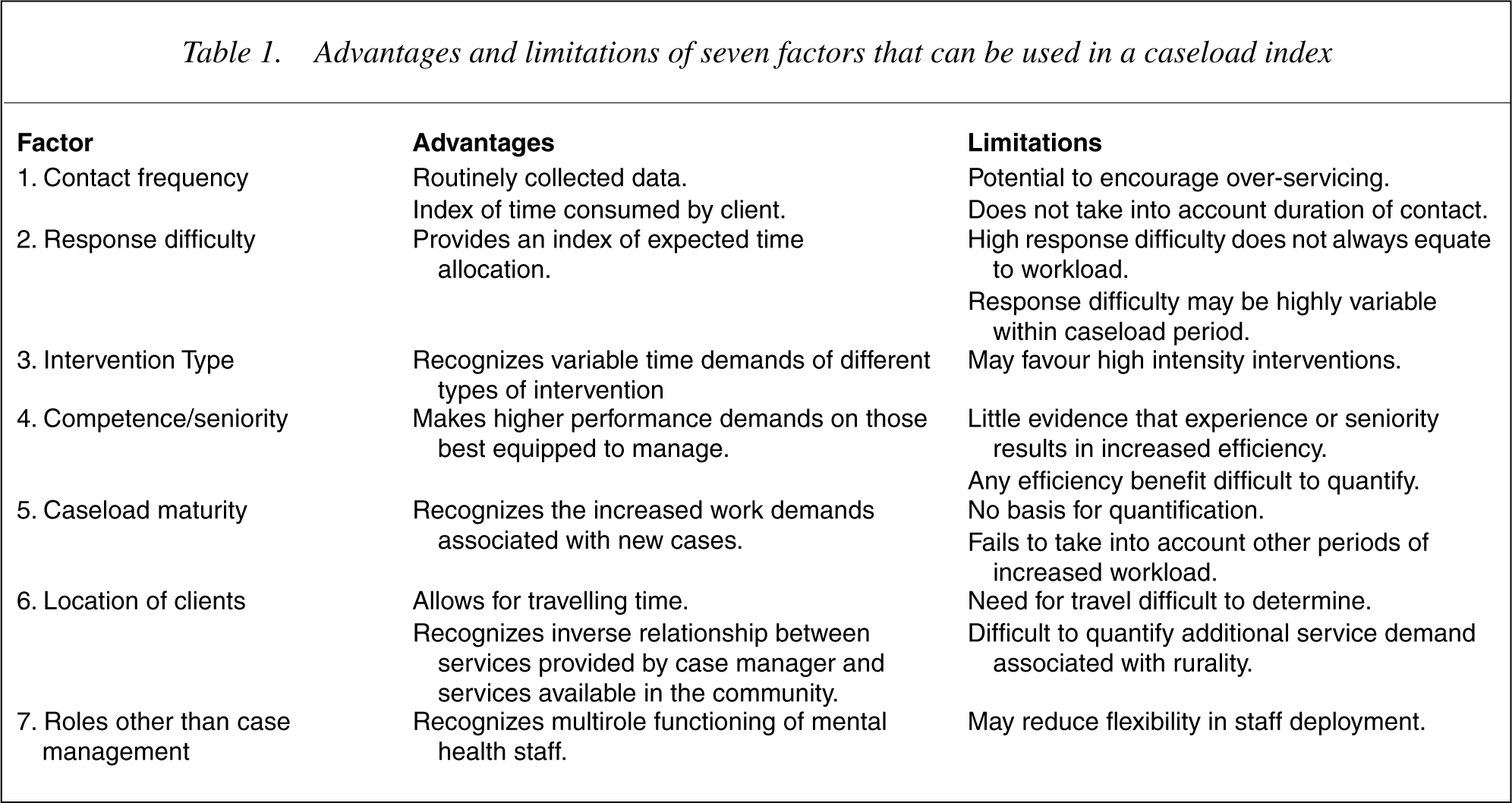
After consideration of the limited published material reviewed above, and consideration of unpublished caseload measurement practices in Victoria and Queensland, the authors identified seven variables used in caseload measurement. These variables have specific advantages and disadvantages with respect to their application in case management and a summary of these is provided in Table 1.
Advantages and limitations of seven factors that can be used in a caseload index
Contact frequency
Contact frequency is a means of measuring service demand. It is an index of decisions made by both clients and case managers that services are required. There are three advantages of this measure. First, it distils the informed judgement and experience of case managers. Second, contact frequency readily lends itself to quantification and can be combined with other quantitative measures such as contact duration. Finally, contact data is often routinely recorded and electronically stored, making it readily accessible.
However, as a means of determining caseload, contact frequency has a number of limitations and disadvantages.
The first is that frequency of contact is not the only factor that determines caseload. Caseload is probably dependent on the quality of the contact as much as the frequency. The quality of a contact will influence the volume of follow-up work required as well as the less tangible factor of emotional burden, a factor which might be crudely quantified in terms of the amount of time required to achieve emotional equilibrium after a contact. It is possible to imagine a high frequency workload, which is less demanding than a lower frequency load with greater difficulty rating.
Second, determining caseload on the basis of contact frequency has the potential for creating an unintended adverse consequence – over-servicing. Staff may acquire a motive to maintain high contact frequency with relatively undemanding clients rather than providing the minimum service necessary to achieve the desired end. This could ultimately result in less than optimum throughput and inadequate services to complex highload clients.
Finally, there is limited empirical basis for estimating the mean contact frequency necessary to obtain acceptable case management outcomes. Common assumptions may be quite fallacious. In this context, evidence that weekly contact results in similar outcomes to those achieved by a high intensity PACT type service [16] and that clients managed in caseloads of 30–35 have equivalent outcome to those managed in caseloads of 10–15 [16] is worthy of note.
Client needs and response difficulty
Measurement of client needs and/or response difficulty gives a quantitative value to the level of service required for each client. Client needs and response difficulty can be measured by a standardized checklist that takes into account variables such as symptom severity, independent living skills, level of risk to self or others, level of family or social supports, level of service engagement. Examples of such an instruments are the unpublished response difficulty checklist developed by the Victorian Mental Health Branch and the UK developed CANSAS [18].
High response difficulty is associated with factors such as suicidality, frequent relapse, multiple diagnoses, aggression and difficulty with engagement. When response difficulty is used, caseload is a product of the total number of clients and their response difficulty scores, rather than client numbers alone. In the approach taken by Meldrum and Yellowlees [18], response difficulty was the sum of clinical complication and need for community liaison. However, it is not clear whether a standardized approach was taken in rating these two variables.
The major limitation of this approach is that neither need nor response difficulty necessarily increases service load. Some factors that make for high response difficulty may in fact reduce load by rendering a service response impossible. A second problem is that response difficulty can be very unstable and vary considerably over relatively short periods. A response difficulty score might be valid one week but invalid the next. Caseload adjustments need to take a longer-term perspective. The impact of client needs on caseload will depend on the extent to which the case manager is personally intervening to address need. In some cases, high service need may be met by external agencies rather than the case manager.
What is therefore required is better empirical evidence as to the possibility of estimating the lifetime expected response demand for a given client. This is a related task to that undertaken by the psychiatry subgroup of the Australian National DRG project [17].
Intervention type
Case management is a therapeutic rather than an administrative role [4] and case managers are expected to deliver a range of evidence-based interventions, including enhancing living skills, individual psychotherapy and family psycho-education. Different kinds of intervention will have different time demands and it might therefore be expected that the intervention profile of a case manager will be a factor in caseload. Case managers who use time-intensive interventions such as individual psychotherapy or intensive skills training will have higher workload demands than case managers who run an occasional group psycho-education session. Intervention type (defined as ‘approach’) forms an important part of the caseload index approach described later.
The major limitation of the use of intervention type in determining caseload is that it assumes clinicians make rational choices about intervention and use the most cost-efficient and clinically effective intervention available when working therapeutically with clients in case management. Principles of evidence-based practice should provide a framework for rational clinical interventions. However, both the complexity of specific clinical cases and the limitations of the available evidence base for psychosocial interventions in mental health makes it difficult to justify prescriptive approaches to intervention [21], [22]. The use of intervention type in determining caseload can therefore have the potentially inequitable outcome of reducing caseload for case managers who elect to undertake more intensive approaches to clinical intervention with their clients. In the face of this problem it is likely that service managers will be under pressure to unreasonably prescribe intervention approaches.
Case manager competence
The use of a measure of case manager competence in the determination of caseload derives from an assumption that case managers are not equally effective and possess different skill levels that will affect caseload capacity. At face value this is a reasonable assumption since variability in work rate and efficiency is commonly found. The difficulty is that there are no standardized means of determining either the basis for efficiency or the size of the efficiency effect. Factors such as seniority and experience are likely to be the best indicators of efficiency, although they may not be good predictors as seniority may be determined by factors other than case management efficiency and experience may not equate with efficiency.
There may be a moral argument for requiring more senior people to manage higher caseloads, but this will not necessarily produce satisfactory work outcomes. There is little basis for determining the size of a seniority factor, except perhaps relative wage rate. In view of these difficulties, there is a real risk that any competence factor will be somewhat arbitrary in the current service environment. Similar objectives could be achieved through linkage of salary to workload and client outcomes, but this would also be difficult to achieve.
Caseload maturity
Anecdotal reports by case managers and analysis of tasks involved in case management at different periods of time in the case management process, suggest that there is a relatively greater burden of work earlier rather than later in the process. During the early period, the case manager is required to form a relationship with the client and significant others, to make a full psychosocial assessment, to develop a case management or individual service plan and to facilitate linkages to other services.
The burden of these early tasks probably has to be considered in emotional terms as well as time. Formation of an adjustment to a new relationship is likely to make demands that extend beyond the hours spent with the person. Once these early tasks have been completed, the tasks involve relationship maintenance, review and revision of service plans. There will be periods of crisis with some clients requiring intense involvement, but it is likely that on average, the workload will be significantly reduced. The quantum of reduction is a matter for empirical investigation and factoring caseload maturity into total caseload will require some arbitrary judgements until such data is available.
Failure to take into account maturity or at least to test the hypothesis that average maturity is equal for all case managers is likely to significantly distort the distribution of actual work between case managers. Maturity can be easily measured as the time elapsed between initial contact and the present time. There may well be a threshold period of two or three months, after which elapsed time has no further impact.
The greatest limitation of this factor is the lack of quantifiable empirical evidence demonstrating that caseload maturity affects workload. While in general it might be stated that new staff should have significantly smaller caseloads than established staff, further research is required to quantify the adjustment warranted by the maturity factor. A second limitation is there are a range of other moments in a case management process, such as relapse and discharge that also significantly increase workload. Including such factors would present major practical difficulties for routine caseload management.
Geographical distribution of clients
If case management requires visits to the client's home (which will frequently be the case) travelling time is a significant variable that will need to be taken into account in estimation of caseload capacity. It is usually possible to calculate travelling time, given the geographical spread of clients and frequency of home visiting. The major difficulty with this variable is that it is difficult to empirically determine the need for home visits and therefore the quantum of time that should be allowed. It might be possible to make some relative adjustments but the size of the allowance will probably depend primarily on the model of work (see the following).
Case managers most affected by geographical factors are those working in regional or remote areas. These case managers may have an additional workload burden associated with absence of a range of local services. The effect of this may be to increase the range of tasks performed by case managers in relation to each client. If this is the case, then the implication is that a lower caseload will be required to preserve an equivalent total workload to that of city-based case managers. The limitation here is that while there is face validity, in the absence of research it is not possible to quantify the effect of geography of caseload.
Case manager roles other than case management
In many service environments, case managers perform a variety of roles other than case management. Other roles include service management, supervision, community education, community development and specialist clinical service provision such as individual, family or group psychotherapy or provision of rehabilitation activities. It is not always easy to identify boundaries between the case management role and sthese other roles, but it cannot be assumed that case managers have an equal quantity of non-case management responsibility. It is therefore an important task, preliminary to determination of caseload, to identify the proportion of each case manager's time that can be dedicated to case management. It should be possible for team leaders or service managers to specify, in advance, the proportion of work time that each case manager will allocate to case management.
This was acknowledged by Meldrum and Yellowlees [19] who asked case managers to estimate the time they spent on case management and adjusted workload to reflect this. The major weakness of their approach and a practical matter that will confront all service managers is reliance on case manager estimates, which may not be reliable and where there is a motive for low estimates as case managers who provide a lower estimate will be rewarded with a lower caseload. Service managers may need to set the proportion of time to be spent on case management to overcome these difficulties.
Three approaches to a caseload index
It is clear from the above that there are arguments for and against the inclusion of most of the variables we have identified. Services are therefore required to make decisions about the particular mix of variables when developing a caseload management strategy. The following are examples of particular measurement approaches developed in Victoria and Queensland.
The Melbourne model
The Melbourne model is based on use of contact frequency data and is primarily concerned with achieving equity between case managers with respect to work activity demands. All services in Victoria are required to routinely collect contact data, including telephone contact. Data are recorded on an electronic database with fields that include date, duration, location and other people involved in the contact. Reports can be generated that provide summaries of the frequency, duration and nature of contacts for individual clients.
The work upon which this is based has been previously published [23]. In this modelling process, routinely collected contact data within the Area Mental Health Service was used to characterize patterns of care within the service. Specifically within the continuing care (case management) program, Meadows found that the frequencies of contact could be usefully grouped into three levels. These three levels of contact identified widely differing numbers of individuals but pooled the total contact numbers within the clinical service into three bands: high, medium and low contact frequency. Each band consumed broadly equivalent total staff time; however, there were fewer higher contact frequency clients than those in the medium and low bands.
If we take a baseline of the number of clients in the high contact group, then the numbers of clients in the medium and low contact groups were approximately four and eight times the high contact group, respectively. Hence it appeared that every client in the high contact group was consuming approximately eight times the energy and input of a typical client in the low contact group. This provided a route into a caseload management score, which essentially adjusted the caseload in terms of equivalent numbers of cases of the lowest intensity type.
The Queensland model
This model was developed at the University of Queensland but is derived from earlier work done by two of the authors (King and Le Bas) in Victoria. The aim is to address efficiency and productivity as well as equity. It specifically ignores contact frequency and attempts to address the equity issue through case distribution. Under this model, the team leader is responsible for ensuring that each case manager has a broadly equivalent range of high, medium and low response difficulty/contact frequency clients. This is achieved by assigning a response difficulty rating at the time of client review.
The formal variables entered into the algorithm consist of time allocated to case management (taking into account geographical distribution of clients and non-case management roles), caseload maturity, and seniority of the case manager. The weightings for caseload maturity and seniority are somewhat arbitrary but simple to calculate and produced acceptable outcomes in a pilot project. The geographical distribution weighting is more difficult to calculate but has unquestionable validity. The impact of geographical distribution of clients will vary according to the location of the service.
The Queensland model makes significant demands on the team leader to calculate, review and adjust weightings on an ongoing basis. While this is somewhat timeconsuming it does have the advantage of engaging the team leader directly with the work demand characteristics of case managers and it should facilitate supervision and effective communication with service management.
The caseload index approach
The caseload index (CLI) arose from the realization that a tailor-made computer information system [24] could assist in caseload management. Along with the Response Difficulty Measure, the CLI includes the concept of ‘approach’. Approach is divided into two categories: maintenance and intensive/extended. As such, it is sensitive to the acuity of symptoms alongside decisions about relevant clinical goals, the latter allowing for the recognition of rehabilitation and psychotherapy efforts [25]. Equally, it recognizes that there are clients with high levels of response difficulty who do not respond to intensive treatment; as such a more modest approach need be reflected.
Considering response difficulty and approach as orthogonal, a ‘case-weight’ is generated for each client and then summed for each case manager. An adjustment is made for actual time per week in case management and clinical seniority. In accordance with this model a client may have high response difficulty plus intensive approach, resulting in a high score for loading or, at the other end of the load weighting, low response difficulty and low intensity approach. Medium case load weightings are assigned in cases of high response difficulty but low intensity approach or low response difficulty but low intensity approach.
Because the factors involved are dynamic rather than static qualities, the index requires that data in the information system be kept up to date (at least each quartile). Within the developmental system it was possible to arbitrarily vary weighting for each of the categories. It proved of interest that the variance in weighting chosen 8 [1] was identical to that empirically derived in the first model.
The CLI is a comparative index and does not entail normative standards for caseload levels.
Discussion
While it is clear that caseload is highly relevant to workforce planning, client service provision and staff management, it is far from clear as to the best procedure for determining caseload. We have identified seven factors that might be considered in a calculation. In each case, there are difficulties associated with either the validity of the factor or the reliable measurement of the factor. Decisions about the use of specific factors may also be influenced by the primary objective. If the main purpose is to optimize service efficiency, contact frequency may not be a useful measure. On the other hand, if the primary objective is to achieve workload equity, contacts and response difficulty may be very important.
It is also evident that, even where relevant factors can be identified, the quantification of these factors may be difficult. We have suggested that it is possible to develop caseload algorithms that can be used in calculating caseload. However, we must acknowledge that the quantification of some of the variables that are used in an algorithm is at best approximate. This would appear to be equally true of the approach reported by Meldrum and Yellowlees [18] where clinical complication and community liaison scores have unknown validity and reliability.
There is need for a great deal more research, designed to quantify the effect of the seven variables on workload and ultimately on client outcome. In the absence of such research, team leaders and service managers are required to make judgements, based on their experience and priorities, as to the extent to which the specified variables are considered in determining caseload. While we acknowledge the difficulties associated with this process, the importance for equity and efficiency means that difficulty is not sufficient excuse for failing to attend to caseload issues. The methodologies presented represent rational approaches to the problem and provide the service manager or team leader with tools that supplement those provided in the earlier work by Meldrum and Yellowlees [18].
What remains to be done is to implement and test algorithms, developed from the methodologies outlined here, over an extended period of time. We need empirical data concerning the impact of caseload management on both quality of client care and on the wellbeing of case managers. This process will facilitate progress from concept to clinical tool.