
Abstract
Drug users are significantly more likely to be affected by psychiatric conditions such as depression, psychosis, schizophrenia and personality disorders [1–3]. Whether these are due to drug effects or to pre-existing morbidities [4] is uncertain but drug exposure and psychiatric dysfunction in expectant mothers may act as independent risk factors for poor outcomes such as prematurity, low birthweight [5], increased maternal morbidity and mortality [6] and poor parenting practices [7], which all may, in turn, lead to adverse childhood outcomes such as failure to thrive [8] and suboptimal neurodevelopment [9, 10].
The number of pregnancies affected by drug exposure is increasing rapidly and may even affect up to 50% of births in high-risk areas [11]. There is little information, however, about the combined impact of psychiatric dysfunction and drug dependency (dual diagnosis, DD) on perinatal outcome, especially in regards to the presentation and course of neonatal abstinence syndrome (NAS). The present aim therefore, was to assess population characteristics of mothers and infants with comorbid psychiatric disorders and exposure to drugs of dependency. We hypothesized that DD women will have worse perinatal outcomes than those affected only by drug-use issues (DU). The present results will have wide-ranging implications for health regions in developed countries with similar management policies to those of New South Wales (NSW) and the Australian Capital Territory (ACT) in Australia.
Methods
Study design and data source
This was a geographically defined, statewide, multi-centre audit using routinely collected information extracted from clinical records. A retrospective search was made in the medical record database of all public hospitals providing obstetric services in NSW and ACT in order to identify women and their live newborn infants who were documented as being exposed to drugs of dependency and who delivered between 1 January and 31 December 2004.
The directors and nursing managers of all public hospitals with obstetric services (n = 82) were first surveyed via questionnaires conducted under the auspices of the NSW Pregnancy and Neonatal Service Network in 2005 [12] to ascertain if any woman with perinatal drug-use problems delivered in their services between 1 January and 31 December 2004. Details about public hospitals in NSW and ACT are found elsewhere [13].
A total of 41 (50.0%) of these hospitals replied in the affirmative. This information, however, was corroborated by a database search from the medical records of all public maternity hospitals for women with at least one hospital admission (pregnancy or birth) for that birth during 2004 and who had at least one ICD diagnostic code for drug dependency-related diagnosis. The 10th Revision of the Australian Modification Codes of International Classification of Diseases and Related Health Problems (ICD-10-AM) [14] was utilized for the search. Local, institutional or Area Health drug and alcohol services also collaborated in providing audit information for cross-referencing of cases and missing information but the primary source of data was from database searches of medical records from each hospital.
Records were reviewed on site at each hospital by one of the researchers for maternal demographics, drug usage and antenatal and delivery outcomes. In NSWand ACT, pregnant women are provided with a card that provides pertinent details regarding any previous pregnancies and the progress of the current pregnancy. This card is carried by the woman and is either absorbed into the woman's inpatient file or photocopied, should the woman wish to keep the card. As a result, details regarding the mother's pregnancy are easily obtained from inpatient medical records. Infant records were also reviewed for neonatal outcome, drug withdrawal sequelae and specific outpatient follow-up services and child-at-risk issues. Standardized drug and alcohol histories were not administered in these hospitals but pertinent details were obtained from each pregnant woman on their first presentation for antenatal care and then repeated routinely on admission to any of the obstetric hospitals. Other than methadone dosages, drug quantification was generally not well documented in clinical notes. Toxicology screening of either the mother or infant, although common practice in many hospitals, was not routinely performed except when clinically or legally required.
DSM-IV criteria of common mental disorders were determined by the clinicians involved in either the drug or pregnancy care of the woman. Common axis I disorders included depression, anxiety disorders, bipolar disorder, attention-deficit–hyperactivity disorder and schizophrenia. Common axis II disorders included personality disorders and mild mental retardation.
We did not include women delivering in the private system, which accounts for 26.8% and 38.4% of the deliveries in NSW and the ACT, respectively [15]. Previous studies from Australia and the USA have shown that the number of drug-exposed women in the private system is considerably lower than in the public system, [16, 17] and due to time constraints we were unable to explore the extent of perinatal drug exposure in the private system because this would have necessitated soliciting permission from the research ethics committee of each individual private hospital. Further study regarding this subject is required because the demographics of privately insured women are no doubt considerably different from those without private insurance in many countries of the world [18].
Validity and accuracy of case ascertainment
The ICD-10-AM was introduced in Australia in 1998. Its quality and reliability of coding in routinely collected hospital discharge data from Australia was assessed by Henderson et al. [19]. This validation audit showed good-to-excellent coding quality for specific major diagnoses, comorbid diagnoses, major procedures, and minor procedures [19]. To increase the accuracy of the case ascertainment of the ICD-10-AM hospital search, we cross-referenced the results with the local, institutional or Area Health drug and alcohol services databases. A total of 338 (38.4%) of the study population were ascertained from hospitals with specialized drug and alcohol services (n = 11).
Definitions
An infant of a drug-using mother was defined as one whose mother admitted to the use of any drug of dependency or its derivatives (other than nicotine and alcohol) during her current pregnancy and/or if toxicology screening of meconium or neonatal urine detected any of these drugs. Drugs considered in this category were opiates (buprenorphine, codeine, heroin, morphine, methadone, pethidine, tramadol), stimulants (cocaine, amphetamines and derivatives), depressants (e.g. benzodiazepines), cannabinoids and inhalants. Polydrug use was defined as a simultaneous dependency on two classes of drugs, for example opiates and non-opiates, excluding cannabis, nicotine and alcohol. Rural or urban residential status was determined by the NSW Area Health regions that corresponded to the particular category in Accessibility-Remoteness Index of Australia (ARIA) [20].
Ethics approval
Approval for the present study was obtained from the governing Human Research Ethics Committees of Area Health Service in NSWand ACT. Case ascertainment rate by individual hospitals was suppressed to protect confidentiality of patients from smaller hospitals.
Statistical analysis
Statistical analyses were performed using SPSS version 13.0 (SPSS, Chicago, IL, USA). Data are presented as proportions with 95% confidence intervals (CIs) and medians with interquartile range (IQR) where appropriate. The χ2, Fisher exact and Mann–Whitney U-tests were used where appropriate. The level of statistical significance for all analyses was set at p < 0.05 using two-tailed comparisons.
Results
The denominator (n = 62 682) used in the prevalence calculations is the number of all deliveries in public hospitals births in NSW and ACT during 2004, which was obtained from the Australian Institute of Health and Welfare (AIHW) National Perinatal Statistics Unit (NPSU) [13]. A total of 73.2% and 61.6% of the deliveries in NSW and ACT, respectively, took place in public hospitals during 2004 [14]. Of these, 879 (1.4%, 95%CI = 1.3–1.5%) were born to mothers who used drugs of dependency. Eight infants (0.01%, 95%CI = 0.01–0.03%) were stillborn. There were 396 women (45.4%) diagnosed with at least one psychiatric condition during the antenatal period (DD). Depression was the most common diagnosis and affected 298 (75.2%) DD women. Other conditions are listed in Table 1. Most women (286, 73.1%) had a single psychiatric diagnosis, 88 (21.4%) had two and 10 (2.5%) had three diagnoses. All 10 women with triple diagnoses used amphetamines only. Psychotropic agents were prescribed for 123 (31.1%) of DD women.
Frequency of DSM-IV psychiatric comorbidities in dually diagnosed drug-using mothers (n = 369)
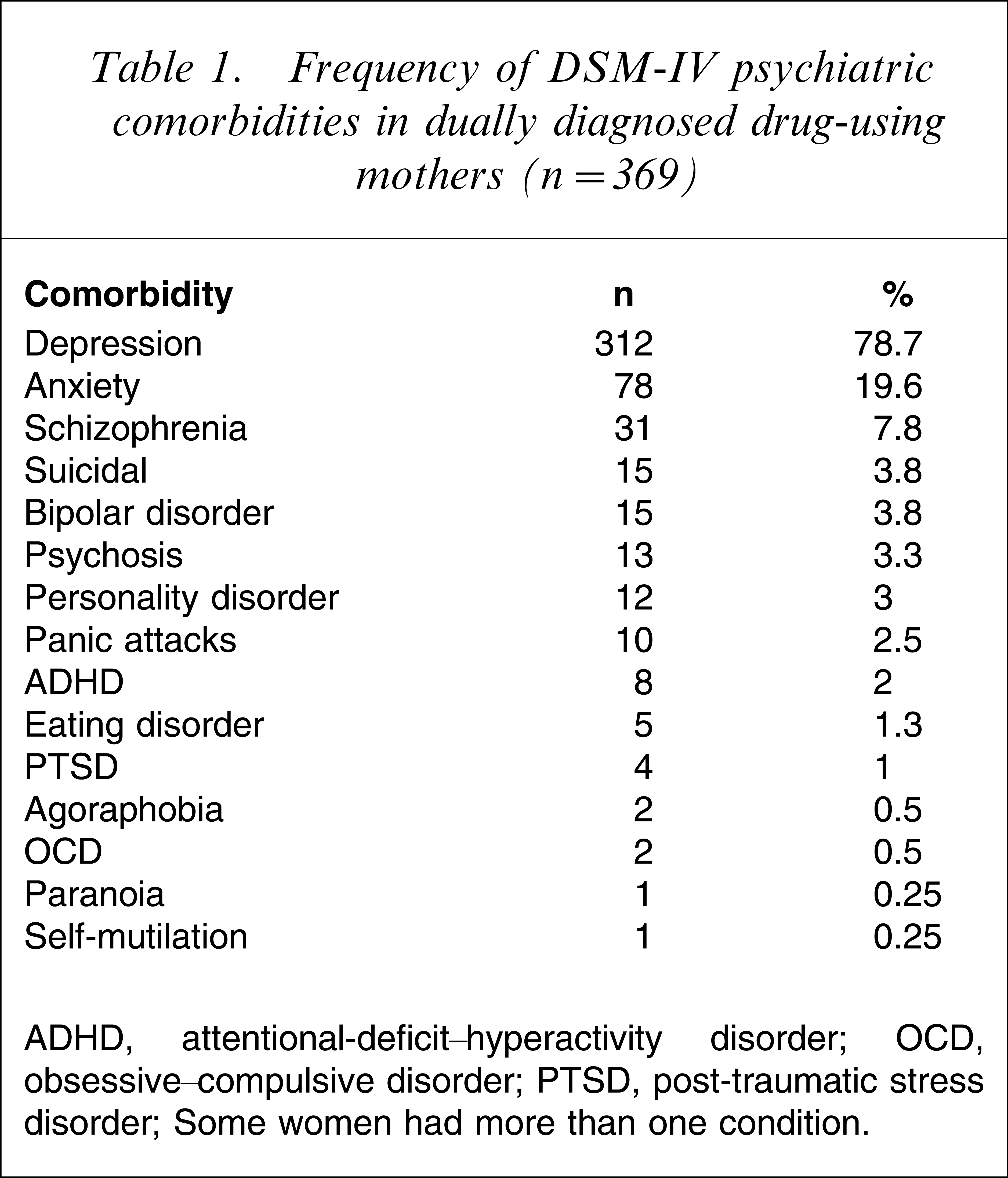
ADHD, attentional-deficit–hyperactivity disorder; OCD, obsessive–compulsive disorder; PTSD, post-traumatic stress disorder.
Some women had more than one condition.
Maternal characteristics and utilization of antenatal care services
DD women were older and had more previous pregnancies than DU women. DD women presented 1 week earlier for antenatal care than DU women but regular ongoing visits were not sustained and DD pregnancies were completed with considerably fewer antenatal visits than DU pregnancies. Other maternal factors, for example frequency of blood-borne diseases and length of postnatal hospitalization were comparable (Table 2).
Subject characteristics
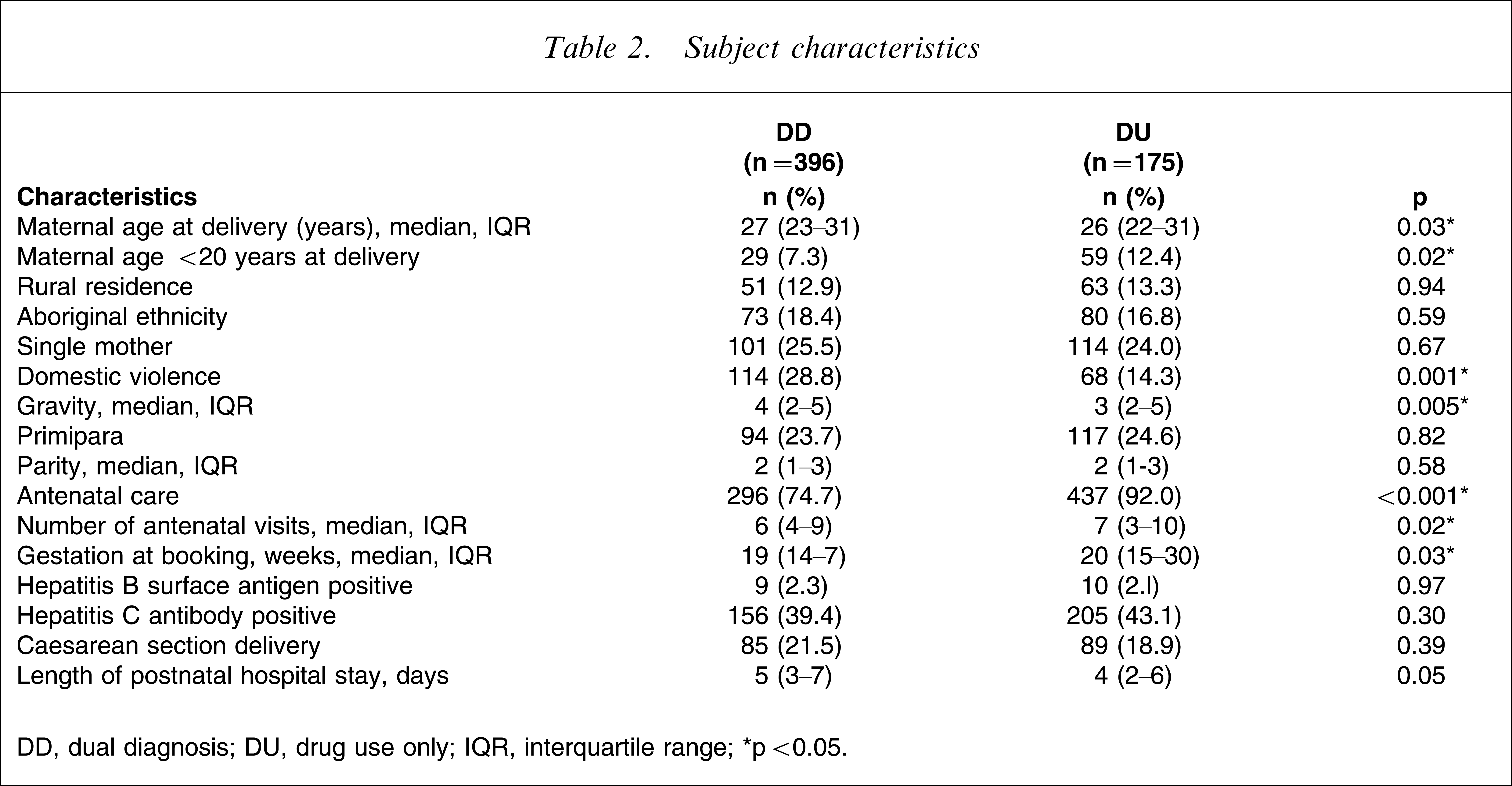
DD, dual diagnosis; DU, drug use only; IQR, interquartile range.
∗p < 0.05.
Pattern of maternal drug use
DD women were less likely to be on opiate-maintenance programmes (e.g. methadone, buprenorphine) but were more likely to use amphetamines, benzodiazepines and multiple classes of drugs (not including cannabis). Amphetamine-users were significantly more likely to be affected by a psychiatric comorbidity than non-amphetamine users (116, 58% vs 280, 41.7%, p < 0.001, Table 3).
Types of drugs used by mothers
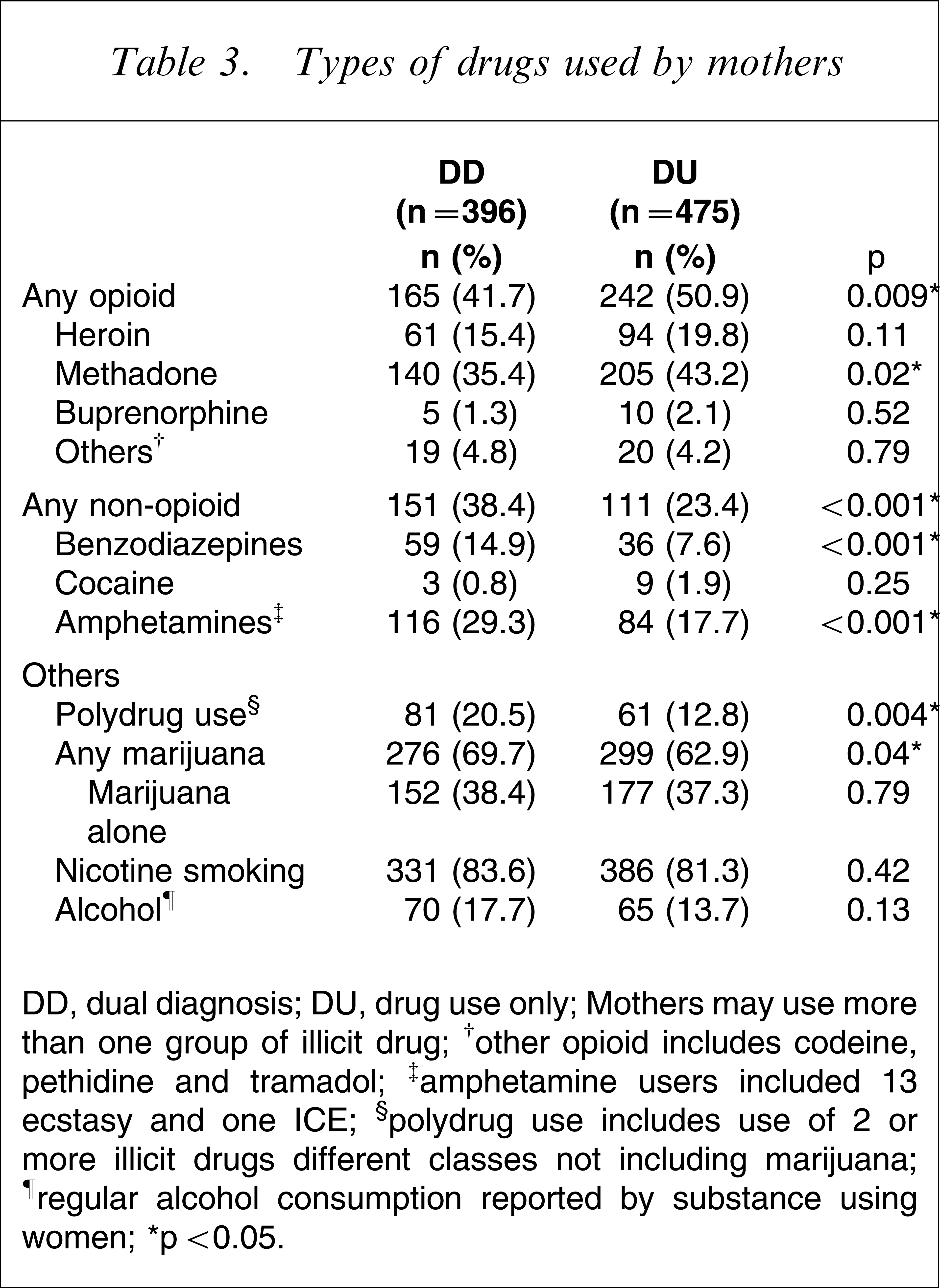
DD, dual diagnosis; DU, drug use only.
Mothers may use more than one group of illicit drug; †other opioid includes codeine, pethidine and tramadol; ‡amphetamine users included 13 ecstasy and one ICE; §polydrug use includes use of 2 or more illicit drugs different classes not including marijuana; ¶regular alcohol consumption reported by substance using women.
p < 0.05.
Neonatal characteristics
There was no difference in gestation, birthweight, condition at birth (Table 4) or the incidence of congenital malformations, which affected 30 (7.5%) and 48 (10.1%) of DD and DU infants, respectively (p = 0.23). DD infants were less likely to be admitted to a nursery or to be monitored with a withdrawal scale after birth. They were also less likely to require pharmacotherapy for withdrawal management even though maximum withdrawal scores on the Finnegan Neonatal Abstinence Severity Score [21] were not different between the groups. The characteristics of withdrawal pharmacotherapy (e.g. the need for morphine or phenobarbitone or the duration of pharmacotherapy) were also not different between the groups. DD infants remained longer in hospital after birth than DU infants (median = 11 days, IQR = 7–20 vs 4 days, IQR = 2–6, p < 0.001).
Infant characteristics by maternal psychiatric status
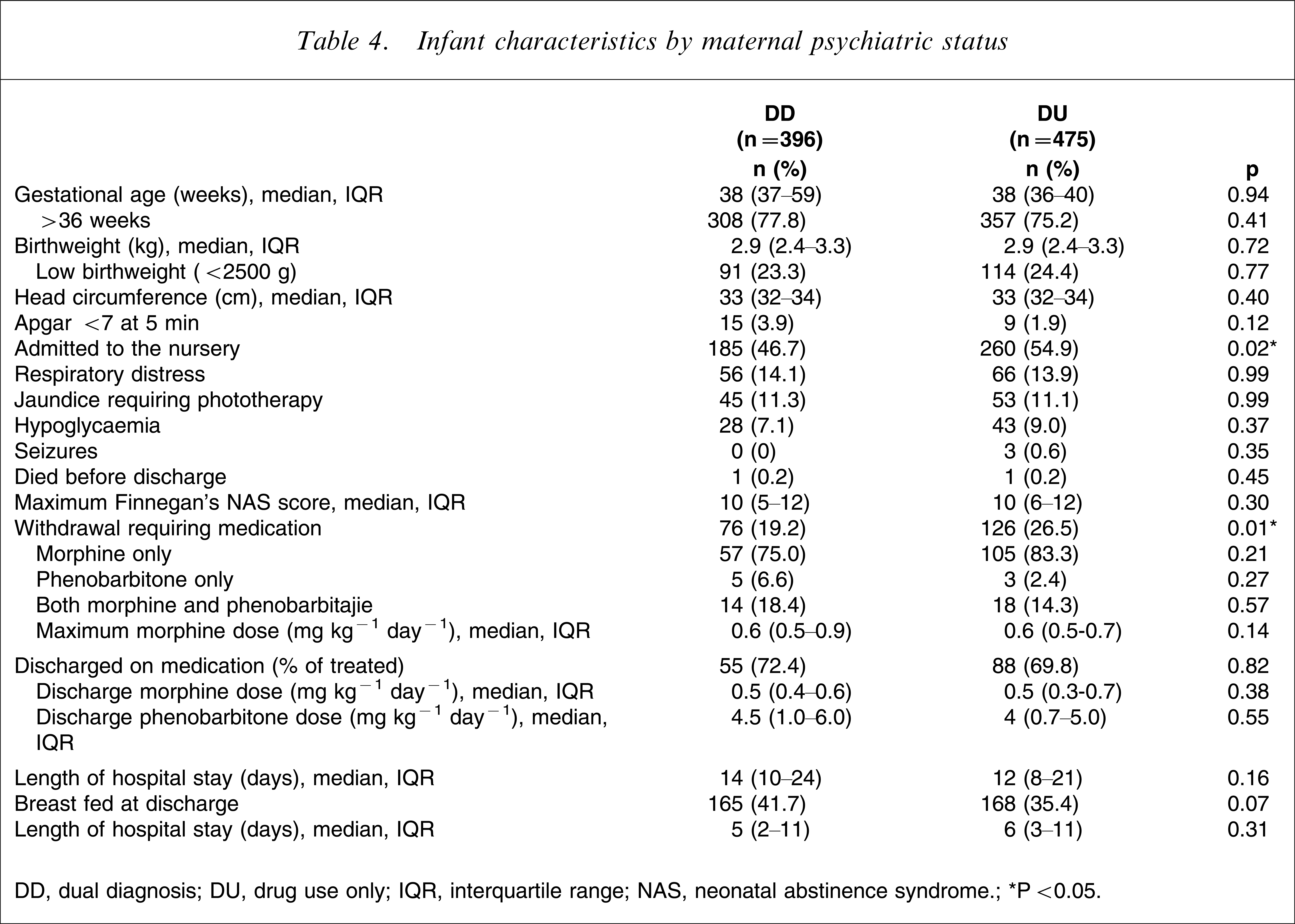
DD, dual diagnosis; DU, drug use only; IQR, interquartile range; NAS, neonatal abstinence syndrome.
∗P < 0.05.
Postnatal follow up and social issues
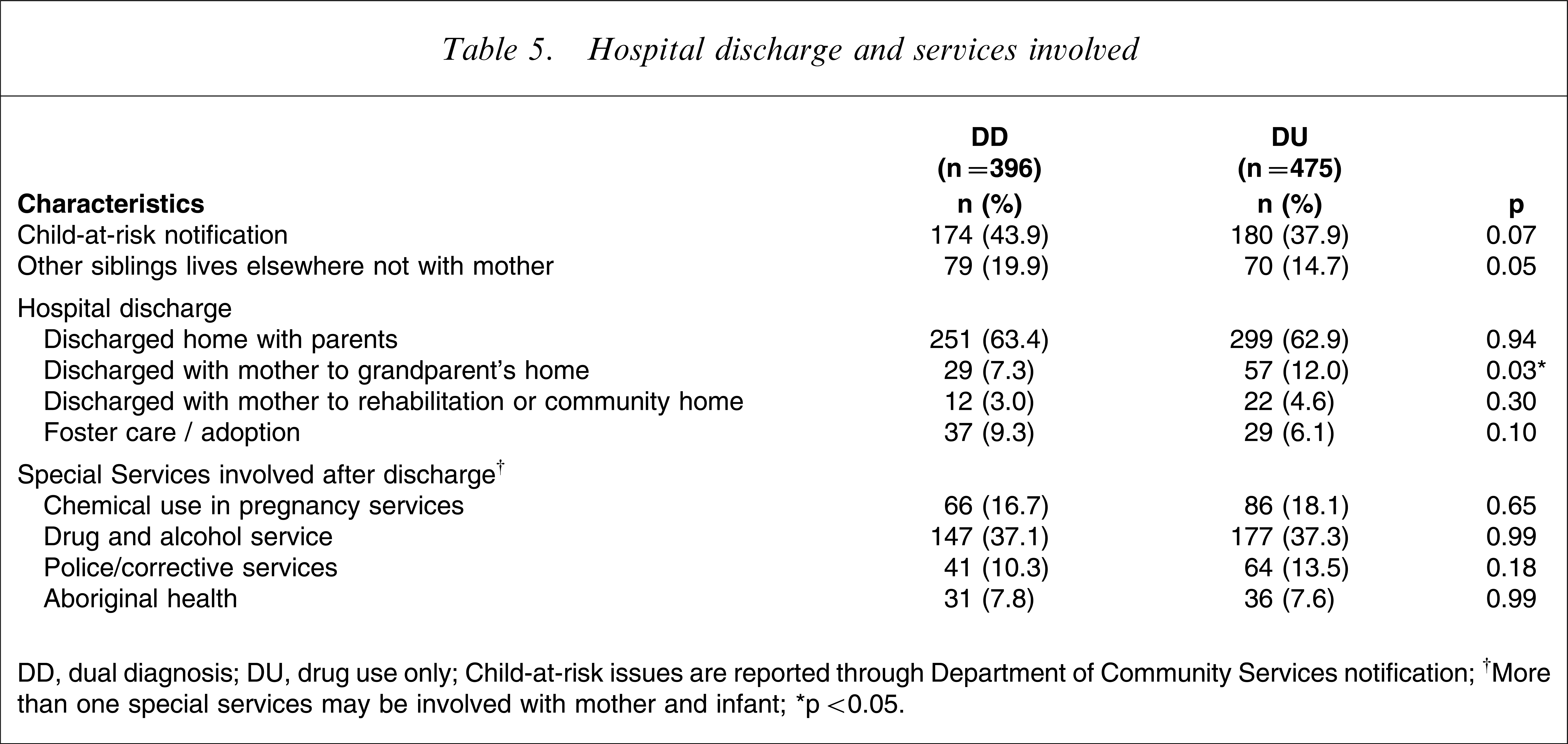
Most of the infants were followed up after hospital discharge in a clinic situated within the hospital of birth. The majority of infants were discharged to a parental home but more DU patients were discharged to a relative's home compared to DD patients. The type of postnatal follow up was unverified or could not be ascertained from the medical records for almost one-third of all infants (n = 100, 25.3% DD; n = 100, 30.5% DU, p = 0.09). The majority of mothers were discharged into the care of a general practitioner and DD women were more likely to be discharged from hospital with definitive follow up (229, 48.2% vs 152, 38.4%, p = 0.003).
DD women were twice as likely to be subject to domestic violence (114, 28.8% vs 68, 14.3%, p = 0.001, Table 5) but women with a depressive primary psychiatric comorbidity were less likely to be at risk of domestic violence than non-depressed DD women (81/312, 25.9% vs 37/84, 37.0%, p = 0.001). The rates of involvement, however, in criminal activities (32, 10.2% vs 11, 11.2%, p = 0.435) and homelessness (22, 7.0% vs 10, 10.2%, p = 0.881) were not different between the two groups. The infants of depressed DD women were less likely to be considered as children at risk (127, 40.7% vs 55, 65.5%, p < 0.001) or to have had other siblings fostered (23, 7.3% vs 21, 25%, p < 0.001) than infants of non-depressed women.
Hospital discharge and services involved
DD, dual diagnosis; DU, drug use only.
Child-at-risk issues are reported through Department of Community Services notification.
†More than one special services may be involved with mother and infant.
∗p < 0.05.
Influence of opiates on outcomes in dually diagnosed women and infants
Opiate-using DD women (165, 41.6%) were more likely to be polydrug users (98, 59.4% vs 25, 10.8%, p < 0.001), to smoke cannabis (157, 95.1% vs 80, 34.6%, p < 0.001) and to be treated with psychotropic medications (65, 39.3% vs 58, 25.1%, p = 0.002) than non-opiate-using DD women (231, 58.3%). Opiate-using DD women were also more likely to be incarcerated than non-opiate users (29, 17.5% vs 14, 6.0%, p < 0.01).
Compared to non-opiate-exposed DD infants, opiate-exposed DD infants were more likely to be transferred to a special care nursery (122, 79.3% vs 76, 32.9%, p < 0.001). Their withdrawal scores were significantly higher (median = 10, IQR = 7–12 vs 4, IQR = 3–7.5, p < 0.001) and they were more likely to need pharmacological withdrawal treatment (86, 52.1% vs 89, 38.5%, p = 0.007) with higher doses of morphine (median = 0.65 mg kg−1 day−1, IQR = 0.5–0.9 vs 0.5 mg kg−1 day−1, IQR = 0.52–0.57, p = 0.03) and to be discharged from hospital on withdrawal medications (57, 34.55% vs 3, 1.3%, p < 0.001).
Infants of opiate-using DD women were also less likely to be breast-fed (52, 31.5% vs 126, 54.5%, p < 0.001), and more likely to be hospitalized longer after birth (median = 11 days, IQR = 6.7–20, vs 4 days, IQR = 2–6, p < 0.001), to be considered as children at risk (98, 59.3% vs 84, 36.3%, p ≤ 0.001) and be fostered prior to discharge from hospital (24, 14.5% vs 16, 6.9%, p = 0.01).
Effects of psychotropic medications
Psychotropic medications were used by 123 DD women (31.1%) at the time of delivery: 92 (23.3%) of the DD sample were treated with a single agent, 16 (4%) with two, four (1.2%) with three and one (0.3%) with four medications. All medications were commenced prior to delivery but doses were not recorded due to the frequent fluctuations in dosages of different drugs.
Medicated women were more likely to be opiate users (65, 52.8% vs 111, 40.6%, p = 0.028) and to be first seen for antenatal care at an earlier gestation (median = 17 weeks, IQR = 13–23 vs 20 weeks, IQR = 14–28, p = 0.02). They were, however, less likely to receive any form of antenatal care (85, 69.1% vs 219, 80.2%, p = 0.02) even though the total number of visits throughout pregnancy was not different between the two groups (medicated: 3 visits, IQR = 0–7 vs non-medicated: 5 visits, IQR = 1–8, p = 0.08). In addition, maximum Finnegan withdrawal scores (9, IQR = 3–11 vs 10, IQR = 5–12, p = 0.37) and the number of infants requiring withdrawal drugs (medicated: 21, 17.1% vs non-medicated: 68, 24.9%, p = 0.09) were similar.
Discussion
The present study has found that almost one in two drug-dependent mothers met DSM-IV criteria for at least one mental health disorder prior to delivery. This proportion is considerably higher than figures obtained from either large population-based linkage studies (5.5%) [22] or smaller single-centre studies (24%) [23]. Even recent interview data showed that only 32% of injecting drug users from the general population had visited a health professional for a mental health problem during the previous 6 months [24]. Differences may be accounted for by methodological variations. Linkage studies, for example, are dependent on medical record classifications and certain conditions may not be detected if they were not recorded on the patient's notes. Single-centre studies may underestimate DD due to small population samples, and interview-based studies depend considerably on the honesty of the respondent. We verified the presence of DD patients from three independent sources: nursing staff, medical records and drug and alcohol services, but it is possible that even the present figures may be an underestimation, especially if some of the affected women did not present sufficiently early for either antenatal care or psychiatric assessment.
Whether the increased rate of psychiatric disorders is due to the effects of the drugs or to an inherent genetic susceptibility [4] is unclear. For example, polymorphisms of the glutathione-s-reductase gene, GSTT1, might be a genetic risk factor of the development of methamphetamine psychosis [25], but amphetamines themselves have been shown to cause ultra-structural and molecular changes similar to Parkinson's disease via a multi-enzymatic complex known as the ubiquitin-proteasome system [26] and certainly, all women with three or more psychiatric disorders in the present study used amphetamines exclusively, suggesting a drug-related effect.
Depression, the most common mental health disorder in our cohort, affected 34% of women and was twice the rate of depression in the general pregnant population (12–18%) [27]. Depression is the predominant mental health disorder in both methadone [1] and heroin [28] users but the risk of antenatal and postnatal depression may certainly be exacerbated by lifestyle adversities such as domestic violence,[29] incarceration [30], homelessness [31], financial hardship and lack of partner support [32], all of which were common problems in the present study cohort. We acknowledge, however, that the present sample was extremely heterogeneous and that women maintained on methadone or buprenorphine may not be as likely to be in financial difficulties, for example, because they may not have to fund illicit drug use to the extent of women not enrolled in maintenance programmes.
We found that DD women were more likely to be multiparous. Even though women with psychiatric disorders such as schizophrenia and depression are reportedly less fertile than the general population [33, 34], poorer contraception or failure to recognize pregnancies may lead to more live births [35]. The consistency of antenatal care, however, was particularly poor in the DD population even when compared to the general drug-using population. This is of particular concern because poor antenatal care is an established health risk for both mother and infant [36] and is a predictor of poor obstetric outcome [37] and suboptimal child health follow up, for example immunizations, well-child visits [38].
All women in the current cohort presented for obstetric care at considerably later gestations than the average Australian woman, of whom only 12–13% present for care after the 20 week of gestation [15], at which time some therapeutic interventions such as pregnancy termination for major neonatal abnormalities or treatment for infections such as syphilis may be infeasible or ineffective. Currently accepted antenatal care schedules have not changed since they were adopted from the original recommendations from the UK in 1929 [39], where women are advised to present for antenatal care every 4 weeks until 28 weeks gestation, every fortnight to 36 weeks and then weekly until delivery. There is evidence that low-risk women may not be disadvantaged by fewer visits to a health professional during the antenatal period [40] but the combined presence of drug use and psychiatric dysfunction places a woman at higher risk of perinatal complications, and such women should be encouraged to adhere as closely as possible to the currently recommended antenatal care schedule. Certainly, financial difficulties, increased parity, younger age, single marital status, lower education, shame of the pregnancy or a fear of medical authorities may have been important deterrents to obtaining obstetric care [41], and a past psychiatric history has been associated with delayed initiation of, and inadequate continuation of antenatal care, even after adjustment for other adverse risk factors [42].
The immediate physical outcome of DD infants, however, was not significantly different from DU infants. Most of the infants were in a good condition at birth but there was a higher incidence of prematurity and low birthweight than infants of the Australian general population in 2004 (8.2% and 7.4%, respectively) [15]. Differences in nursery admission rates were unlikely to be due to common neonatal problems such as hypoglycaemia and jaundice (the rates of these were similar between the two groups), but were more likely due to a higher incidence of opiate-related NAS in the DU group [43].
The severity or incidence of NAS did not appear to be affected by the presence of psychotropic agents. There is little current information on the combined effects of drugs of dependency and psychotropic medications on pregnancy and neonatal outcome, especially on NAS. Discontinuing psychotropic medications during pregnancy may cause disease relapse [44] and worsen the woman's parenting ability. The most commonly used psychotropic agents were antidepressants, and selective serotonin re-uptake inhibitors in particular, have been shown to cause mild and self-limited adverse neonatal symptoms such as jaundice, feeding intolerance and respiratory distress [45, 46] that may not be appreciated if the infant is observed only for evidence of withdrawal from common drugs of dependency.
Data sources for substance abuse research have been critically reviewed by Garnick et al. [47]. We acknowledge that the present study design is almost entirely reliant on a passive registry of women who admitted to drug use and therefore, it is highly likely that we would not have been able to capture recreational drug users who were not linked to formal drug-treatment programmes or high-functioning women who preferred not to disclose their drug use. In turn, this would then have limited the use of meconium and urine assays to measure maternal drug exposure because these tests are often performed only on infants whose mothers have previously admitted to drug use. We believe that the design of the present study allowed us to obtain considerably more information than a prospective study, from which consent to access records would have been denied by eligible patients. For example, out of the 7119 women eligible for a study of methamphetamine use and neonatal outcome, only 1632 (23%) consented to take part, and follow up was available for only 166 of the total subjects [48].
In conclusion, the present study demonstrates that almost half of all women who admit to the use of drugs of dependency during pregnancy have some form of psychiatric morbidity. Women who use amphetamines are at particular risk. Although the short-term outcomes of their infants do not appear to be affected by exposure to psychotropic agents, the high incidence of social dysfunction in DD women emphasizes the need for routine antenatal psychosocial assessments so that earlier mental health or social interventions may be instituted, as required.[49] Further study regarding the long-term outcome of the children of women with both drug dependency and psychiatric disorders is urgently needed.
Footnotes
Acknowledgements
The authors thank the NSW and ACT NAS Epidemiology Group, nursery, obstetric and medical records staff of the birthing hospitals in NSW and the ACT: Adam Buckmaster, Adam Winstock, Anthony Galloway, Belinda Bones Saunders, Beth Burton, Bob Fonseca, Brendan McCorry, Bridgett Scott, Catherine Maher, Cheryl Laidlaw, Christine Stephens, Deborah Arthur, Di Diebert, Fiona Cooke, Gail Saul, Geoff Hardacre, Geoff Jacket, Graham Reynolds, Ian MR Wright, Inga Heyman, Janet Falconer, Jenny Stonestreet, John Leary, Jon Currie, Jonathan Morris, Joy Dickinson, Julianne Arundale, Ken Curry, Kim Smith, Linda Fawcett, Mark Tracy, Melissa Toms, Miriam Dayhew, Patricia Lutz, Paul Haber, Peter Kristidis, Rajiv K. Agrawal, Ruth Jobson, Samar Zakaria, Sarah Clews, Susanne Wooderson, Sweemee Levsen, Tracey Halliday. The research project was funded by the Leslie Stevens Fund for Newborn Care Research, Sydney Children's Hospital Foundation.