
Abstract
Keywords
Converging evidence suggests an association between trauma, particularly childhood maltreatment and adult somatization [1, 2]. For example, individuals with a history of child abuse and those with post-traumatic stress disorder (PTSD) have been found to show more somatization and endorse more medically unexplained symptoms than non-traumatized subjects [3–5]. Conversely, child abuse and neglect have often been observed in patients with conversion and somatization disorders [6–10].
The close link between severe traumatic experiences and somatization is also acknowledged by the syndrome of complex PTSD or disorder of extreme stress not otherwise specified, which requires somatization as one out of six diagnostic criteria [11–13]. This syndrome was first introduced in the early 1990s and describes a specific pattern of psychopathological symptoms and personality features that are considered to be the long-term sequelae of severe, chronic and often interpersonal traumatic experiences, in particular child abuse [11, 14, 15]. In addition to somatization, the criteria for the formal diagnosis consist of (i) impairment of affect regulation including impulse dyscontrol and self-destructive behaviour; (ii) altered states of consciousness with amnesia and dissociative symptoms; (iii) alterations in self-perceptions including intense feelings of guilt and shame; (iv) distorted relations to others with isolation and distrust; and (v) alterations in one's system of meanings. Although complex PTSD is not recognized as a freestanding diagnosis in DSM-IV, but listed under ‘associated and descriptive features’ of PTSD, support for the construct validity of the syndrome has come from studies of community and primary care samples, psychiatric inpatient and outpatient populations as well as forensic settings [16–23]. Further evidence for the syndrome of complex PTSD has originated from studies focusing on severely traumatized individuals such as survivors of childhood sexual abuse [12, 24, 25] and combat veterans [20, 26, 27]. Additionally, evolutionary and cross-species perspectives support the concept of complex PTSD [28].
Although it has been found to be a useful and valid diagnostic category in different settings, the syndrome has not yet been assessed in patients with somatization disorder (SD), although somatization is one of its diagnostic criteria. Apart from the high prevalence of childhood maltreatment in these patients [9, 10], however, there is further indirect evidence indicating that complex PTSD might be relevant for this particular population. For example, affect regulation and dissociation are both constitutive of complex PTSD and play a major role in SD [1, 10, 29]. Furthermore, feelings of guilt and shame, social isolation and distrust, which belong to the psychopathology captured by complex PTSD, are also core features of depressive disorders often associated with SD [30].
In a previous study we found that childhood physical and/ or sexual abuse was more frequent in SD patients than in patients with major depressive disorder (MDD) matched for gender and age [9]. Here we report the frequency and correlates of complex PTSD in the same sample. Specifically, we hypothesized that SD patients with complex PTSD compared to those without this syndrome and to the MDD patients exhibit (i) more general psychopathology; (ii) more interpersonal problems, and (iii) a reduced health-related quality of life.
Method
Participants
The study design and selection criteria are described elsewhere [9]. In brief, 28 patients with DSM-IV SD as confirmed by the respective section of the Structured Clinical Interview for DSM-IV, Axis I (SCID-I) [31] were included and compared to 28 age- and gender-matched patients with MDD as diagnosed by the Mini-DIPS, the brief German version of the Anxiety Disorders Interview Schedule [32, 33]. None of the MDD patients met criteria for current or lifetime SD as assessed on the SCID-I [31]. All participants gave written informed consent. The sociodemographic characteristics of the two samples are presented in Table 1.
Subject characteristics
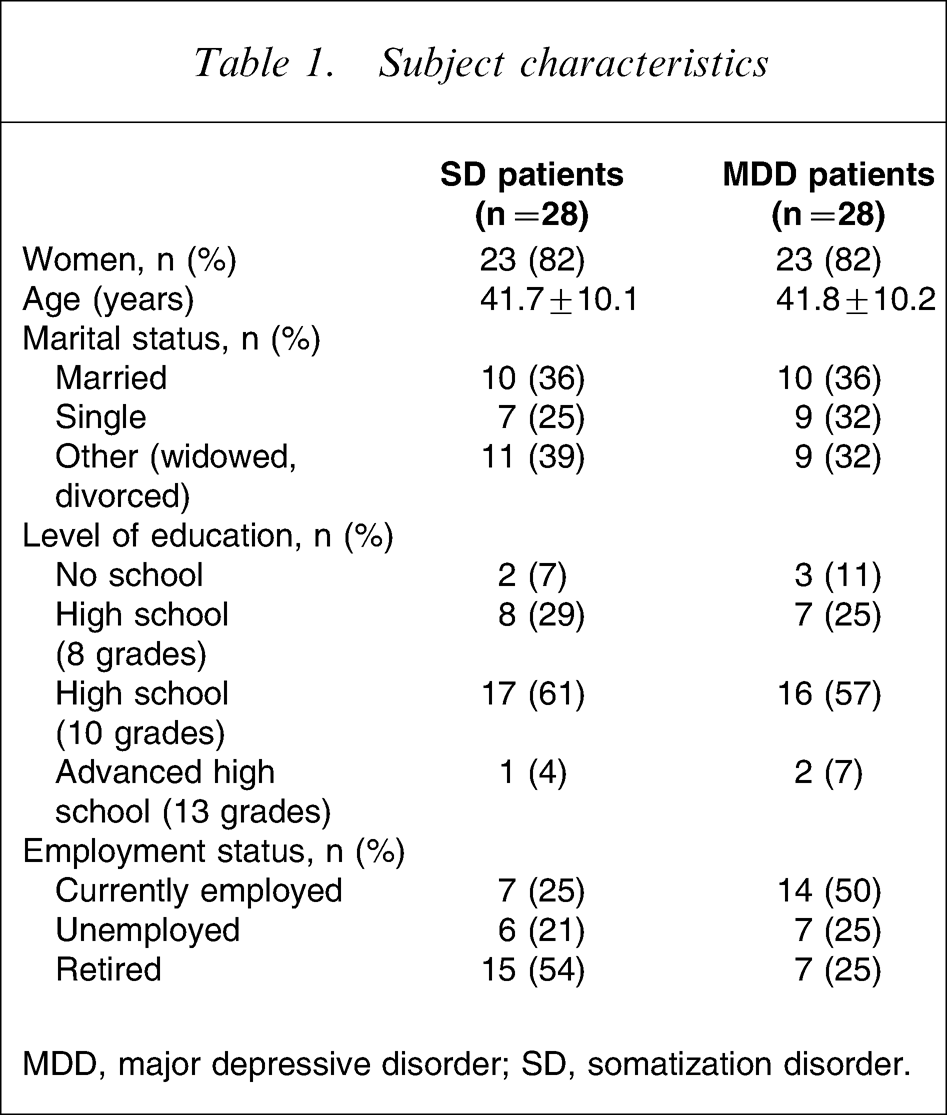
MDD, major depressive disorder; SD, somatization disorder.
Instruments
The Structured Interview for Disorders of Extreme Stress (SIDES) was developed to provide clinicians and researchers with a rational way to measure the construct of complex PTSD [17]. This 40-item scale assesses the presence and severity of the diagnostic criteria as outlined in the previous section. The interview allows both a current (i.e. within the last 3 months) and lifetime diagnosis. The psychometric properties including inter-rater reliability and internal consistency were found to be sound [17], and another validation study reported good convergent and divergent validity [34]. Likewise, internal and external validity of the German adaptation of the SIDES were found to be good [35].
The Brief Symptom Inventory (BSI) is a widely used self-report measure to assess current psychopathology [36]. In addition to nine syndrome scales (somatization, obsessive compulsion, interpersonal sensitivity, depression, anxiety, anger–hostility, phobic anxiety, paranoid ideation, psychoticism) a global rating (Global Severity Index, GSI) reflects the general psychological distress. The reliability and validity of the German version of the BSI parallel the original version [37].
The Inventory of Interpersonal Problems–Circumplex Scales (IIP) dimensionally assesses the nature of dysfunctional interpersonal patterns [38]. It consists of eight scales (domineering, vindictive, cold, socially avoidant, non-assertive, exploitable, overly nurturant, intrusive) and provides a total score indicating the general degree of interpersonal problems. The psychometric properties of the German version of the IIP are very similar to those of the original version [39].
The SF-36 Health Survey is an internationally well-established self-report inventory of functional impairment and well-being [40]. Eight domains are assessed: physical functioning; role limitations due to physical health problems (role–physical); bodily pain; general health perception; vitality; social functioning; role limitations due to emotional problems (role–emotional); and emotional well-being. In contrast to the aforementioned measures, lower scores indicate more impairment. The reliability and validity of the German version of the SF-36 are as good as the original version [41].
Statistical analysis
Data analyses were performed using SPSS version 12.0 (SPSS, Chicago, IL, USA). We applied the χ2 test for categorical variables; if case frequency was lower than 5, Fisher's exact test was applied. Due to the small sample size, we used non-parametric tests for between-group comparisons of the psychometric measures (Mann–Whitney U-test, Kruskal–Wallis H-test). Additionally, we calculated effect sizes (Cohen's d). Because the group comparisons were considered exploratory and hypotheses-generating in nature, statistical significance was based on two-sided tests evaluated at the 0.05 level of significance. To account, however, for multiple testing, comparisons that remained significant after Bonferroni adjustment were identified in the results tables.
Results
As illustrated in Figure 1, current and lifetime diagnoses of complex PTSD were significantly more frequent among SD than MDD patients (35.7% vs 3.6% and 50.0% vs 10.7%, respectively). Compared to the control group, SD patients had an eightfold higher risk for lifetime diagnosis of complex PTSD (odds ratio (OR) = 8.33, 95% confidence interval (CI) = 2.04–34.07) and a 15-fold higher risk for current complex PTSD (OR = 15.0, 95%CI = 1.76–127.54). Among the somatization subjects, the mean age of those with current complex PTSD (43.7±8.8 years) did not differ from the mean age of those without this condition (40.6±10.9 years, U = 76.5, p = 0.516). Likewise, there were no gender differences between those with and without complex PTSD (90.0% vs 77.8%, χ2=0.655, p = 0.418).
Frequency of complex post-traumatic stress disorder (current and lifetime diagnoses) in patients with (▪) somatization disorder and (□) major depressive disorder.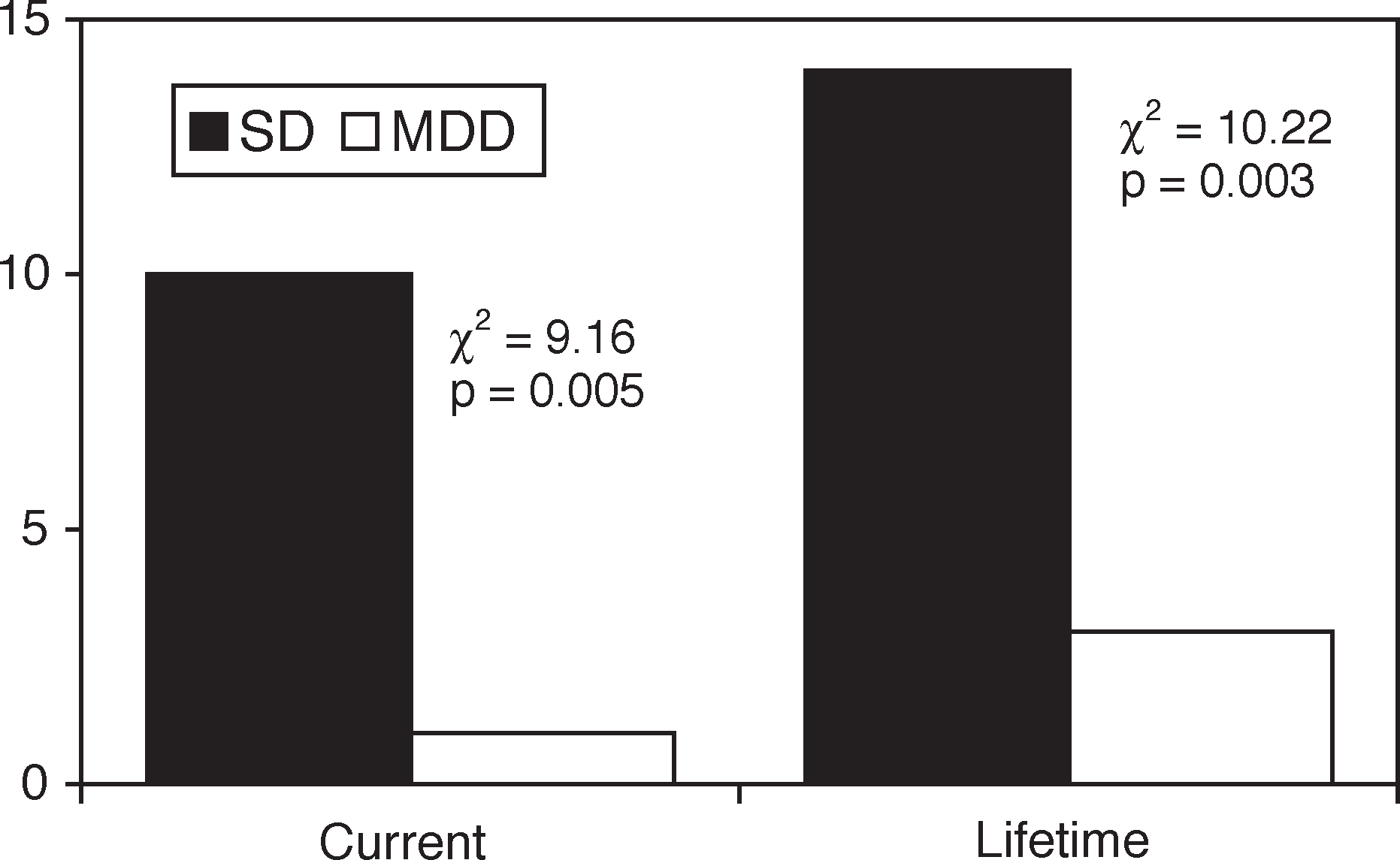
SD patients with current complex PTSD had significantly higher scores for the BSI subscales obsessive compulsion, anger–hostility, and psychoticism compared to those SD subjects without this syndrome (cf. Table 2). Furthermore, they also had significantly more psychopathological impairment in the BSI dimensions obsessive compulsion, anxiety, anger–hostility, phobic anxiety, paranoia, psychoticism, and the GSI than MDD patients without current complex PTSD. Comparison of the BSI means between SD patients with and without complex PTSD produced moderate to large differences as indicated by Cohen's d ranging between 0.4 and 1.2.
Comparison of pychopathology (BSI)
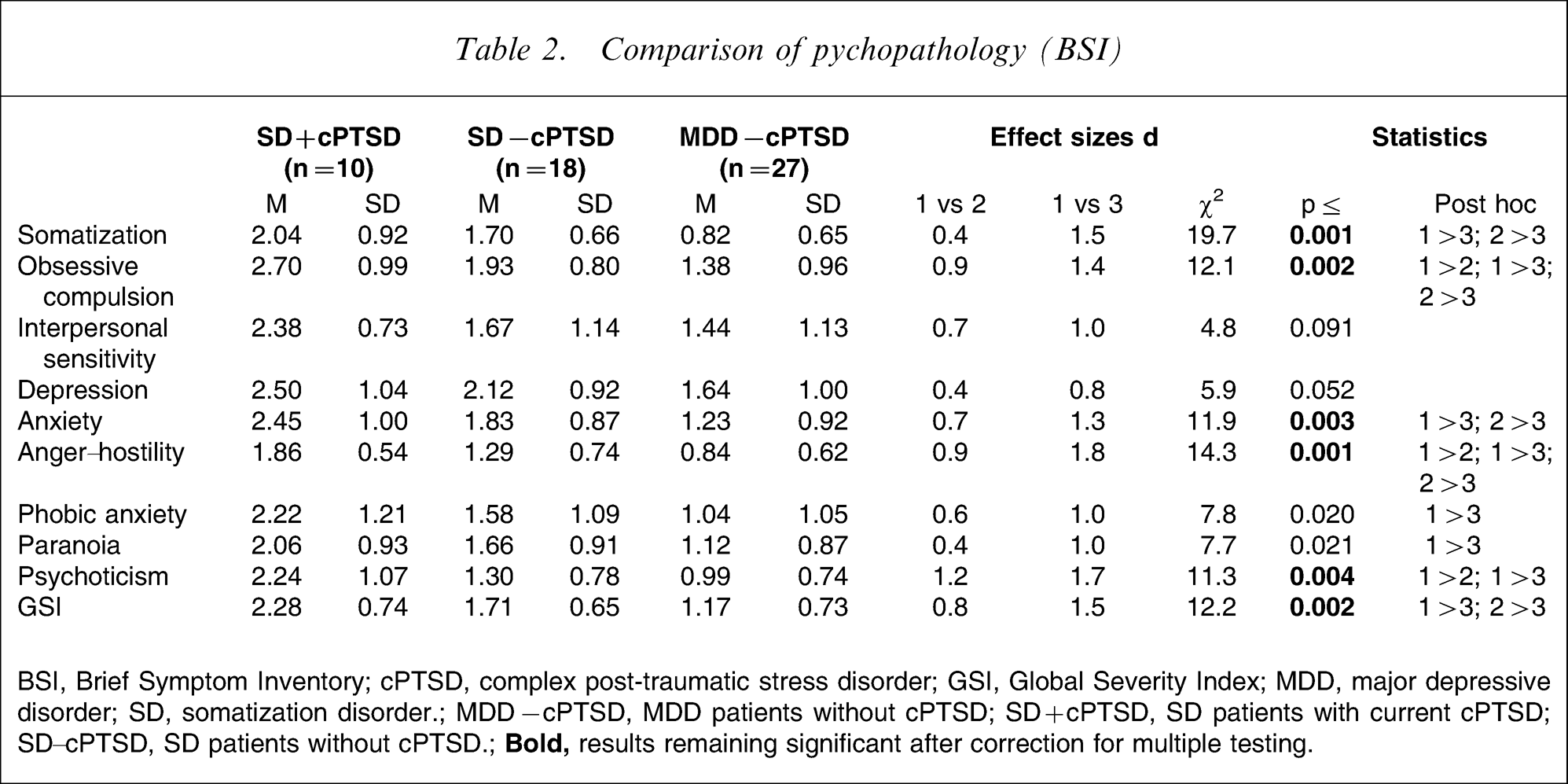
BSI, Brief Symptom Inventory; cPTSD, complex post-traumatic stress disorder; GSI, Global Severity Index; MDD, major depressive disorder; SD, somatization disorder; MDD − cPTSD, MDD patients without cPTSD; SD + cPTSD, SD patients with current cPTSD; SD–cPTSD, SD patients without cPTSD.;
The differences with respect to interpersonal problems were moderate to large for the IIP subscales vindictive, cold, socially avoidant, non-assertive, exploitable, overly nurturant and the IIP total score (cf. Table 3). Statistical significance, however, was found only for the dimensions cold and socially avoidant as well as the IIP total score.
Comparison of interpersonal problems (IIP)
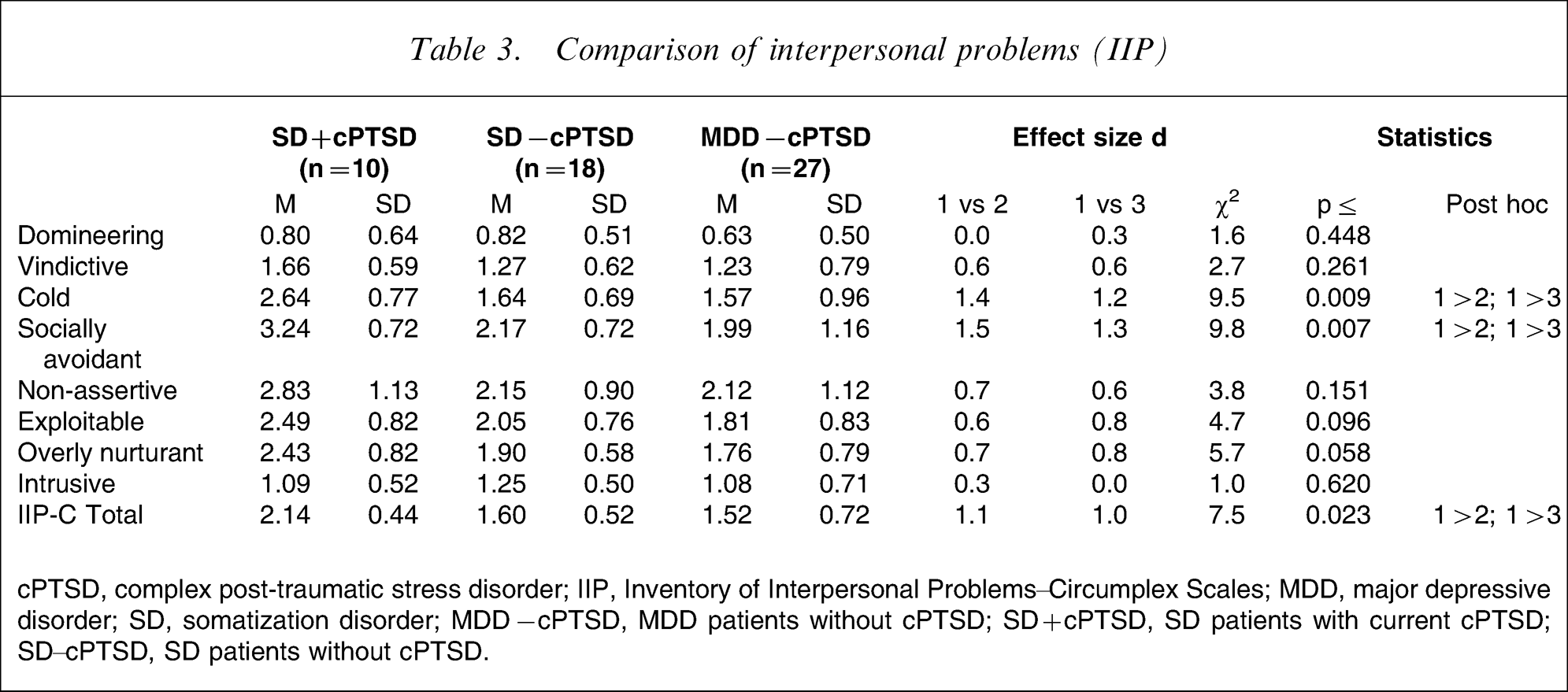
cPTSD, complex post-traumatic stress disorder; IIP, Inventory of Interpersonal Problems–Circumplex Scales; MDD, major depressive disorder; SD, somatization disorder; MDD − cPTSD, MDD patients without cPTSD; SD + cPTSD, SD patients with current cPTSD; SD–cPTSD, SD patients without cPTSD.
Regarding the health-related quality of life as captured by the SF-36 Health Survey, there were moderate differences between SD patients with and without complex PTSD with respect to physical functioning, vitality, social functioning and emotional well-being (cf. Table 4). These differences, however, were not significant.
Comparison of health-related quality of life (SF-36)
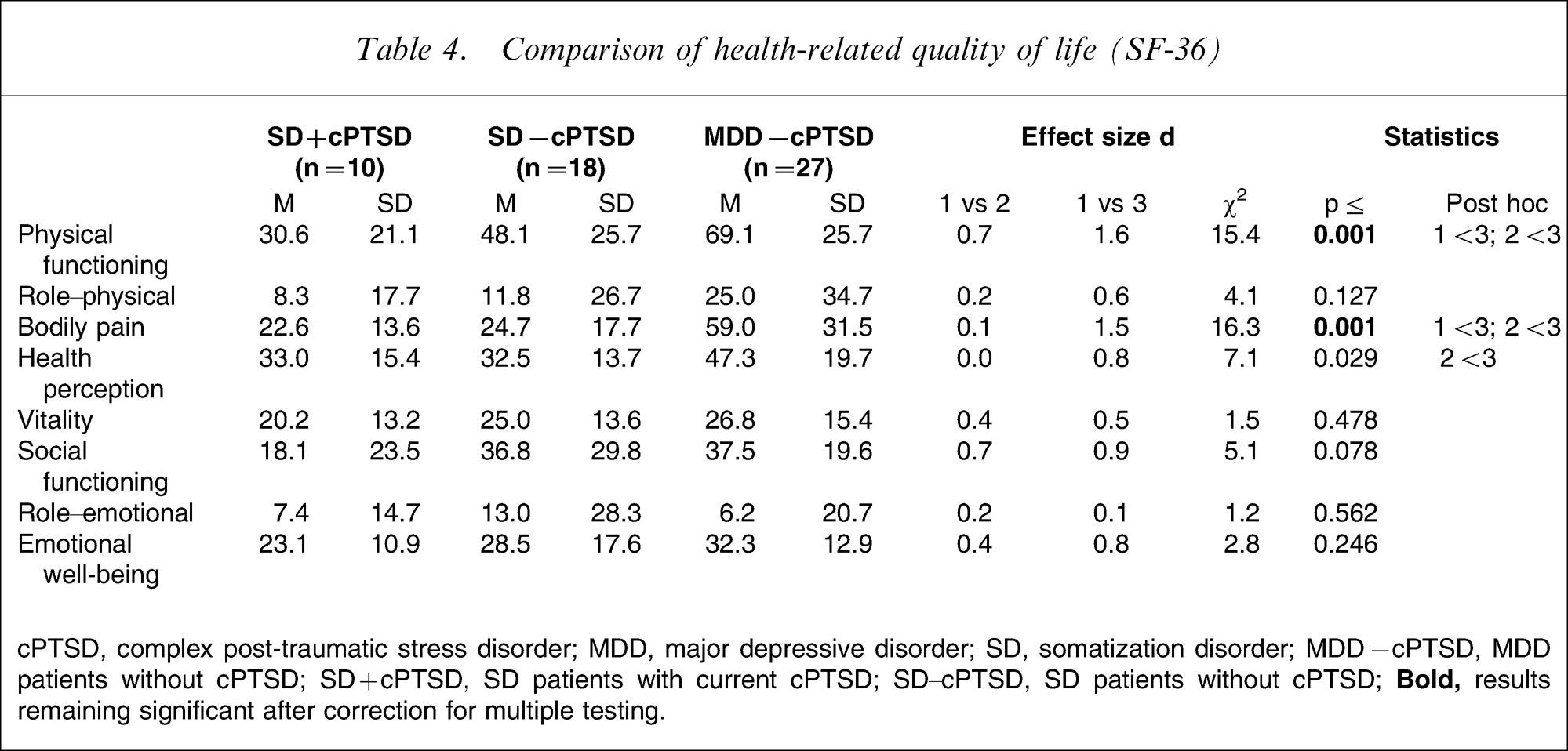
cPTSD, complex post-traumatic stress disorder; MDD, major depressive disorder; SD, somatization disorder; MDD − cPTSD, MDD patients without cPTSD; SD + cPTSD, SD patients with current cPTSD; SD − cPTSD, SD patients without cPTSD;
Discussion
To the best of our knowledge this is the first study assessing complex PTSD in patients with SD as compared to patients with MDD matched for age and gender. The present findings indicate higher current and lifetime prevalence of complex PTSD in SD patients (35.7% and 50%, respectively) compared to MDD patients (3.6% and 10.7%, respectively). Considering the high rates of childhood maltreatment in subjects with SD [9, 10], the rates for complex PTSD found in the present study are consistent with corresponding research on survivors of childhood abuse [12, 24, 25]. For example, 61% of participants of the DSM-IV field trial for PTSD with early onset abuse (i.e. before the age of 14 years) met diagnostic criteria for lifetime complex PTSD and 35% for current complex PTSD [13].
Those SD patients with current complex PTSD had more psychopathological impairment than the two other groups, with moderate to large effect sizes (cf. Table 2). This is consistent with prior studies from different settings indicating that subjects with complex PTSD exhibit more psychological distress than subjects without the syndrome [16, 20, 23, 27, 35]. These results suggest that complex PTSD might capture a subgroup of patients with severe psychopathology.
Because alterations in relations with others is one of the diagnostic criteria for complex PTSD [11, 13], it is not surprising that among the SD patients those with complex PTSD had more interpersonal problems as reflected by higher IIP-C scores (cf. Table 3). Additionally, their self-reported interpersonal style was particularly characterized by cold and socially avoidant behaviour, which corresponds well to the relationship disturbances constitutive of complex PTSD, that is, the inability to trust, social withdrawal and hostility [11–13].
Although statistically not significant, the differences in the SF-36 subscales physical functioning, vitality, social functioning and emotional well-being between SD patients with and without complex PTSD suggest clinically relevant impairment in these dimensions, because the corresponding effect sizes were at least moderate.
Some methodological limitations of the present study merit discussion. Due to the relatively small size of the study population (n = 28 in each sample) statistical power may be compromised, for example, the precision of risk estimates was low as reflected by large confidence intervals. A post-hoc analysis, however, regarding the frequency of lifetime complex PTSD as one of the main outcome criteria indicated that the power of the χ2 test was 91% with an alpha of 5%. Nevertheless, the present findings should be regarded as preliminary and need to be replicated with larger numbers of patients suffering from SD. Furthermore, because we included patients referred to a university department (i.e. a tertiary care setting), it remains unknown if the present results can also be applied to other samples of somatizing individuals, for example, in the general population or in primary care settings. Finally, the construct validity of complex PTSD has been questioned and there are doubts as to whether it ‘rises to the level of a true diagnosis’ or is ‘merely a proxy for comorbidity in general’ [42]. In contrast, others have strongly advocated the concept of complex PTSD [43].
Despite these limitations we suggest that the concept of complex PTSD has clinical utility when applied to SD patients because it identifies a distinct subgroup of individuals with severe psychological distress, interpersonal problems as well as impaired physical and social functioning. Considering the difficulties of the treatment of SD patients and the lack of a lasting and clinically meaningful effect [44], it might be assumed that therapy for SD patients with complex PTSD is particularly challenging. Correspondingly, complex PTSD was a negative predictor of treatment outcome and quality of life measures in chronic PTSD [21]. Recent studies, however, provide evidence that psychodynamically oriented trauma-focused treatment [45] and cognitive behavioural approaches including dialectical behaviour therapy [46, 47] are effective for patients with complex PTSD. Thus, integrating trauma-therapeutic techniques and interventions might improve psychosocial treatment outcomes of SD patients with complex PTSD. Although we are in need of future research to further clarify these issues, we believe that complex PTSD represents a heuristically valuable concept in the assessment and treatment planning for patients with SD.