
Abstract
The essential feature of somatization disorder (SD) is a pattern of recurring, multiple, clinically significant somatic complaints that cannot be fully explained by any known general medical condition or the direct effects of a substance [1]. The aetiology of SD is considered to be a mix of psychosocial and biological factors [2]. Some studies with auditory evoked potentials [3] and combining evoked potentials and regional cerebral blood flow [4], have suggested that SD patients suffer from subtle neuropsychological disturbances, compared with normal controls, that consist of impairment in attentional processing. They have an impaired ability to filter out and not respond to relatively meaningless afferent stimuli [5, 6]. In addition, some patients show a disturbance of bifrontal cognitive process with a predominance in the non-dominant hemisphere [7]. Despite these data, no single photon emission computed tomography (SPECT) research has been done on SD patients except one isolated case-report [8] in which the patient described suffered from associated depression, and this disorder produces by itself anomalies in SPECT image.
Single photon emission computed tomography research in diseases strongly related to SD such as chronic fatigue syndrome (CFS) demonstrates abnormalities that seem to correlate with clinical status [9, 10], concretely, an asymmetry (right more than left) of tracer uptake at the parietotemporal level is demonstrated in CFS compared with major depression [9]. As a consequence, a pathophysiological role of frontal blood flow in the cognitive impairment and physical activity limitations in CFS has been hypothesized [9]. In addition, it seems that SPECT is more useful than magnetic resonance imaging (MRI) in following the clinical progress of CFS patients for two reasons: (i) SPECT detects significantly more abnormalities than MRI; and (ii) SPECT abnormalities appeared to correlate with clinical status whereas anomalies detected with MRI did not reverse with improved clinical status [10]. Another disorder related to SD is Munchausen syndrome. One patient with this uncommon disorder was studied with SPECT and a marked hyperperfusion of the right hemithalamus was found although cranial computed tomography (CT) scan had been normal [11]. Finally, in patients with conversion disorder studied with SPECT a left temporal and parietal perfusion decrease has been demonstrated [12].
The objective of this study is to assess any possible abnormalities in SD patients when studied with SPECT scan.
Method
Patients
The study was carried out in the Somatoform Disorders Unit of the Hospital Miguel Servet, Zaragoza, Spain. The inclusion criteria were: (i) a DSM-IV diagnosis of SD using the Standardized Polyvalent Psychiatric Interview (SPPI) [13], an interview specifically designed for medical patients that has been widely used by our group in the Zaragoza Somatization Study [14–17]; (ii) not fulfilling criteria for any other axis I psychiatric disorder. The reason for this criteria is that SPECT scan can show abnormalities in patients with disorders such as depression [8, 18] and anxiety disorders [19, 20] (we did not consider axis II comorbidity because there is no scientific data confirming that that these are associated with brain SPECT abnormalities); (iii) not being diagnosed with any other medical condition that might produce abnormalities in SPECT scan; (iv) normal CT and MRI images; (v) agreement to sign a written informed consent after the procedure had been fully explained.
All the patients referred to the Somatoform Disorders Unit during the period 1997–1999 who fulfilled DSM-IV criteria for SD were included in the study. From them, 47 (75.8%) were excluded due to axis I psychiatric comorbidity. Two other patients (3.2%) were ruled out due to an associated brain illness with abnormal CT and MRI images. Finally, two other patients (3.2%) did not give informed consent to have SPECT. So, only 11 SD patients (17.7%) could be included in the study. In these patients we studied the dominant hemisphere using Annet's hand preference questionnaire [21], based on the method used by Lishman and McMeekan [22], as has been described in a previous paper on lateralization in SD patients [23]. Finally, the lateral predominance of the symptoms was assessed based on the chief pain complaint according to the patient's perception.
Single photon emission computed tomography imaging procedure and evaluation
All the subjects were studied in the supine resting position with closed eyes in a quiet room in which visual and auditive stimulus were reduced to a minimum. Fifteen minutes before the injection a dummy run with normal saline was used to acclimatize the subject. The technique used for SPECT was 99mTC-D,1,hexamethylpropyleneamideoxime (99mTC-HMPAO; Ceretec®, Amersham International, Bucks, UK) in the first four patients and 99mTc-Bicisate (Neurolite®, Dupont Pharma, Hamburg, Germany) in the other seven patients, and both were prepared according to the manufacturer's instructions. The SPECT study was performed 15 min after injection of 740 MBf with a 360° rotating single-head gamma camera system (Apex SP-GHR Elscint®, Haifa, Israel) equipped with a low-energy all-purpose collimation. Data were obtained in 64 × 64 pixel matrices through 360° rotation at 60 intervals for 6° per arc interval, zoom 2. Reconstruction was performed by filtered backprojection using a Butterworth (Haifa, Israel) filter and attenuation on scatter correction of 0.12 cm–1. The resulting images were re-oriented to the orbital meatal line and transverse, coronal and sagital projection were generated. All images were displayed relative to the mean maximum cerebellar perfusion count derived from both cerebellar hemispheres. The SPECT scans were evaluated without knowledge of clinical data.
Results
We summarize in Table 1 sex, age, the results of SPECT, dominant hemisphere and lateral predominance of symptoms. In Figure 1 the scan images of three of the cases with hypoperfusion can be seen compared with the SPECT image of a healthy person.
Upper left, case 3: hypoperfusion of left frontal brain (red arrow) and right cerebellum (green arrow); upper right, case 8: hypoperfusion of right hemisphere except cerebellum (blue arrow); lower left, case 11; hypoperfusion of bilateral rear temporoparietal brain (yellow and orange arrows) and right cerebellum (red arrow); lower right, normal SPECT scan from a healthy person. All images are transverse projections.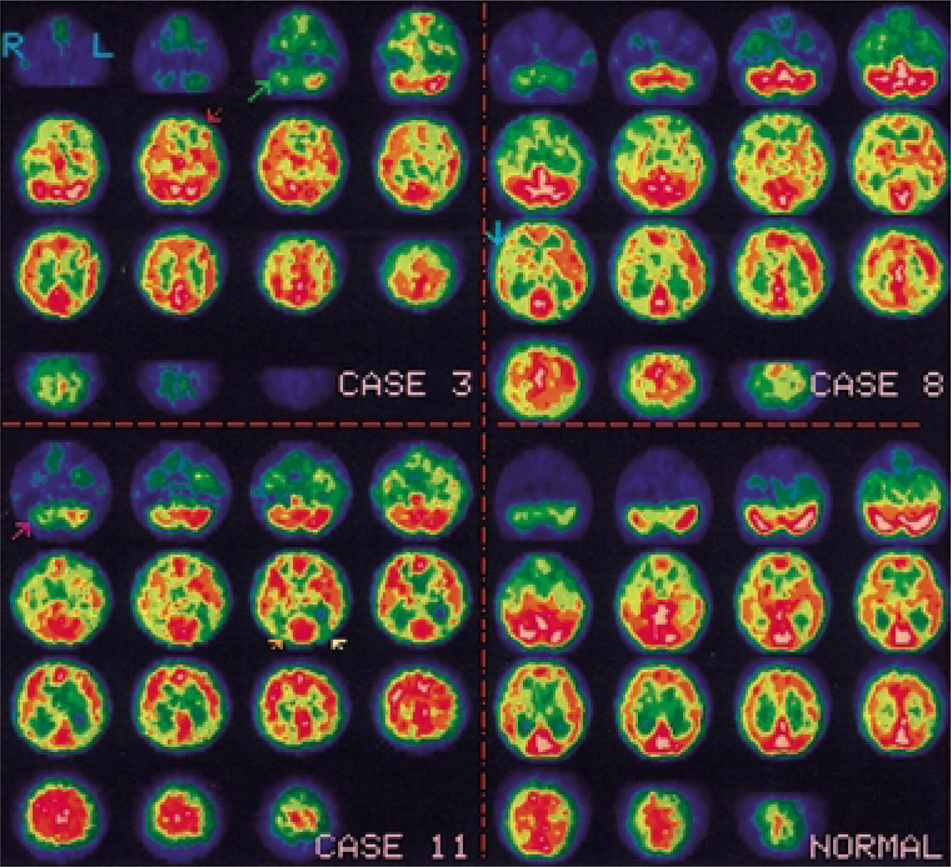
Characteristics of the somatization disorder patients studied with SPECT scan
Discussion
This is the first study, to our knowledge, in which a series of SD patients has been studied with SPECT. These patients had a rare characteristic: at the moment when SPECT was carried out they did not fulfil criteria for any other DSM-IV axis I psychiatric disorder. This fact is important because, for instance, depression, the most common psychiatric disorder associated with SD, is known to alter SPECT images [8, 18] and to be related to cerebral asymmetry [24, 25]. A sample of ‘pure’ SD patients is a rare feature because nearly three-quarters of these patients are diagnosed with another psychiatric disorder [16]. Finally, all these patients presented no other brain disorder and their CT and MRI images were normal when SPECT was performed.
However, there are several limitations in this research. First, the small number of patients. In general, published studies with SD patients use small samples [3–6] due to the relatively low prevalence of SD patients [26]. In this study, the need to rule out those patients with any associated psychiatric disorder reduces the sample even more. Second, this is not a controlled study with a matched sample of healthy controls. An ad-hoc matching would be biased. Third, a profile of neuropsychological tests would be advisable to correlate functional abnormalities with neuropsychological impairment (not routinely performed in our unit). Fourth, a follow-up would be recommended to confirm that the SPECT abnormalities endure.
Despite these limitations, our findings point to possible abnormal brain function of SD patients and confirms studies [3–7] that suggest subtle neuropsychological disturbance.
Other conclusions are:
1. Hypoperfusion showed a predominance of right hemisphere (four cases). In the other three patients hypoperfusion did not present lateral predominance (cases number 3, 4 and 10). The region affected varied: right cerebellum (four cases), frontal and prefrontal (three), temporoparietal (two) and the complete hemisphere (one).
2. There was a relationship between the hemisphere affected and the lateral predominance of pain symptoms. In the cases of unilateral hypoperfusion, it happened in the non-dominant hemisphere and pain symptoms took place in the contralateral hemibody.
3. The SPECT image is more appropriate to detect brain abnormalities in SD patients than morphological tests such as CT or MRI, given the functional nature of the postulated disturbance (in all the cases in which SPECT showed abnormalities both CT and MRI were normal).
It is not easy to explain the neurobiological basis of these findings. Pain sensitivity and negative affect (a personality trait precursor to depression) have been associated with a hyperactivity of right hemisphere (the non-dominant) and to the predominance of pain symptoms in left hemibody [25]. The left predominance of pain symptoms is found not only in SD patients but in all pain syndromes [23, 27, 28]. However, previous reviews do not find an association between pain symptoms and a specific SPECT pattern [29].
In the patients in which we can observe image abnormalities, there is a trend to associate SPECT hypoperfusion of the non-dominant hemisphere with predominance of pain symptoms in the contralateral hemibody. Unfortunately, there are no previous studies on SD patients, and reviews on SPECT patterns in other kinds of pain are inconclusive.
This study can be the basis for the following hypothesis: a certain number of SD patients show hypoperfusion of the non-dominant hemisphere in SPECT images. However, lack of research and the fact that SD is associated with other psychiatric disorders, has made it difficult to confirm it. Specific research studies on ‘pure’ SD patients, using sequential SPECT exams associated with neuropsychological assessments is needed, and studying correlations with dominant hemisphere and lateral predominance of symptoms.
Footnotes
Acknowledgements
The Spanish ‘Fondo de Investigaciones Sanitarias de la Seguridad Social’ (FISss) supported this research.