
Abstract
Use of legal and illegal substances, particularly by adolescents and young adults, is widespread and their harmful use is an important public health problem around the world. Nicotine, alcohol and cannabis are the most common substances used and abused by adolescents and young adults. Every year tobacco smoking takes the lives of approximately 4 million people worldwide [1]. Alcohol-related morbidity and mortality account for a substantial burden of disease and disability [2]. Research has shown that individuals who begin to use substances at younger ages are more likely to become dependent on substances, to engage in the use of illicit drugs such as heroin, and to experience adverse psychosocial consequences related to illicit drug use [3–5]. Consequently, there is increasing interest in pathways that lead to early onset of substance use initiation, and in exploring whether similar risk factors predict early initiation of substance use and subsequent substance use disorder.
Why do some individuals start using substances at a young age? One way to approach this question is to identify the characteristics of those who use substances, that is, risk factors for use of substances and early onset of such use. Information on these characteristics and the environmental background related to the use of substances in early adolescence may prove important to those concerned with issues of aetiology and prevention. Such information may also help to refine causal hypotheses for the origin and prevention of substance use and abuse [6–9]. This perspective suggests that preventive interventions should focus on reduction of risk and enhancement of protective factors to prevent later substance abuse.
The factors that underline a person's use of substances are likely to involve a complex interaction of individual, family and social–environmental factors, as well as genetic and biological influences [10–12]. Of the several domains associated with use of illicit drugs, two that have been given considerable attention are family and individual (personal) factors. Social theory and empirical evidence consistently point to the family environment as an important influence on child and adolescent behaviour, including substance use [13]. In addition, there have been numerous studies of individual predictors of substance use in adolescents [10]. Notwithstanding, there is a paucity of evidence about the impact of early life risk factors on initiation of substance use in early adolescence and whether these factors predict emergence of substance use disorders.
Of the family determinants, a number of factors have been shown to be predictive of use of substances. For example, children reared in families with lower socioeconomic status (SES) have been found to use substances greater than others [14]. The composition and functioning of the family has also been found to have a significant relationship with substance use and dependence [14], [15]. Research indicates that disrupted family structure and changes in maternal marital status predict increased risk of substance abuse in adolescents and young adults [14–16]. In addition, research on parenting practices has found inadequate parental monitoring (control and supervision) to be predictive of problem behaviours, including substance use in offspring [17], [18]. Furthermore, family modelling of drug-using behaviour and parental attitudes toward children's drug use are related specifically to substance use in adolescence [19–22].
In regard to the personal characteristics, male adolescents and young adults have shown a higher prevalence of substance use [14]. Empirical research has shown that gestational age and weight at birth are inversely associated with a diverse range of health outcomes. For example, children with low birthweight (<2500 g) have been found to be more likely to report symptoms of mental health problems and poor school performance [23], [24]. It is unclear whether the association holds for use of substances during child development. Several mental health and problem behaviours have also been found to be associated with substance use. These include early childhood conduct disorder/externalizing behaviour [25–27] and other psychiatric disorders, such as major depression and social anxiety [14], [25].
Although a wide variety of factors are causally implicated in the context of substance use, existing evidence is mainly based on investigations that examined small groups of selected risk factors. These factors are likely to be correlated and a number may be indicators of the same underlying cause. Furthermore, limited available prospective studies leave unresolved the concerns about the strength and magnitude of the association between particular risk factors and substance use, independent of other factors that possibly confound this association. There is a need for a study that takes into consideration a number of these factors simultaneously. Finally, available evidence is mainly drawn from studies that have examined risk factors in later childhood and adolescence. There is a paucity of knowledge about independent factors in the early stages of a child's life that are associated with early onset of substance use, and whether those early life factors predict development of substance abuse or dependence (disorder) by young adulthood. Early childhood development is considered an important sensitive period of human development. This perspective maintains that the period from fetal life to early school years is crucial for brain development and can be linked with outcomes in later life across domains such as learning, health and behaviour [28], [29].
The present study reports the findings from a prospective pre-birth cohort study. The aim was to examine a wide range of predictors over the early life course (first 5 years) of a child and how these are associated with the subsequent use of nicotine, alcohol and cannabis by adolescents and young adults. Because early initiation of substance use has been suggested to lead to substance abuse and dependence, we examined whether predictors of early substance use are consistently associated with the development of substance use disorders by young adulthood. Variables under study included child birthweight and gender, child problem behaviours at 5 years, mother's age and education (when the child was born), family economic situation and maternal changes in marital status between child's birth and age 5 years, quality of marital relationship, mother's mental health and substance use at child age 5 years and mother's control and supervision of child at 5 years.
Methods
Participants
Data for this study were taken from the Mater–University of Queensland Study of Pregnancy (MUSP), a pre-birth cohort study that recruited pregnant women attending the Mater Misericordiae Hospital, one of the two major obstetric hospitals in Brisbane, Australia. The women were consecutive public patients recruited over the period 1981–1983 and were at an average of 18 weeks gestation at the recruitment interview. Baseline data were collected at the first antenatal visit from 7223 consecutive women who gave birth to live singleton babies and follow up was done at 3–5 days, 6 months, and 5, 14 and 21 years after the birth. Additional details of sampling and study methodology have appeared elsewhere [30], [31]. Informed consent from the mother was obtained at all phases of data collection and from the young adult at the 21 year follow up. Ethics committees from the Mater Hospital and the University of Queensland approved each phase of the study. The present analyses used data from the baseline, 6 month, 5, 14 and 21 year follow-up surveys.
At the 21 year phase of the study 3647 young adults completed self-report questionnaire about age of initiation of smoking, alcohol consumption and cannabis use. Of those, 2546 completed the computerized version of Composite International Diagnostic Interview (CIDI-Auto) [32]. We found that attrition or incompleteness at the 21 year follow up was related to several background characteristics. Male participants or those from lower SES were more likely to be lost at the 21 year follow up. Children whose mothers were anxious or depressed or who smoked cigarettes at 5 years were more likely to have left the study by the 21 year follow up.
Measures: outcome variables
At the 21 year follow up the study participants were asked three questions about the age at which they began using cigarettes, alcohol, and cannabis. Some 3647 young adults provided retrospective information about the age of first use of these three substances. Consistently with previous studies that have defined early initiation of substance use as 14 or 15 years and younger [5], [33], [34], we categorized the youth into three groups: never started substances; started at ≤14 years (early onset); or ≥15 years (late onset). Using the CIDI-Auto a substance use disorder was defined by the presence of DSM-IV [35] lifetime nicotine, alcohol or cannabis abuse or dependence. A subsample of 2546 young adults completed the CIDI-Auto.
Measures: independent variables
Information on child gender and birthweight (to nearest g) was obtained from hospital records; children were divided into three groups (<2500 g, 2500–3999g; or ≥4000 g, with 2500–3999 g being the reference category). Mother's age was measured at the first clinic visit (<20 years or ≥20 years). Mother's highest level of education was assessed at the first clinic visit (tertiary education; completed high school; incomplete high school). Gross family income was reported at the first clinic visit, 6 month and 5 year follow ups (selecting the 25th centile as cut-off below which family income was defined as ‘low’). The cut-offs for low income were below $AUD10 399 during pregnancy and when the child was 6 months old, and below $AUD15 599 at the 5 year follow up. Those with incomes above these cut-offs were considered middle or higher income. A composite variable was then recoded into three categories (consistent high; moderate–low; and consistent low income).
At the 5 year assessment changes in maternal marital status in the first 5 years of the child's life were obtained using questions requesting frequency of divorce, separation from partner and change of partner. A composite scale was then recoded to three levels: no change; one or two changes; or three or more changes. The quality of the marital relationship was also assessed at 5 years via the short form of the Dyadic Adjustment Scale (DAS) [36]. We then divided mothers into three categories: unpartnered; partnered with good adjustment; or unpartnered with poor adjustment (top 20% of scores for marital disagreement).
Maternal mental health at the 5 year follow up was assessed using the short form of the Delusions Symptoms States Inventory (DSSI) [37]. In this study mothers were regarded as having symptoms of depression or anxiety if they reported three or more of the seven symptoms in the DSSI depression or anxiety subscales. For maternal substance use, the mother responded to questions related to alcohol intake (recoded to abstainer or drinker), and smoking in last week (recoded to no/yes).
The mother's approach to discipline was measured at the 5 year follow up by questioning subjects with two sets of items indicating maternal control (five items, Cronbach's α = 0.64) and maternal supervision (six items, Cronbach's α = 0.73). The mothers were later categorized into three groups for each of the control and supervision variables (low, moderate, high).
Symptoms of problem behaviours in children at the 5 year follow up were derived using the Child Behaviour Checklist (CBCL), which is a maternal report questionnaire for subjects aged 4–18 years, and which asks about behavioural problems in the last 6 months [38]. Several validation studies have been published on the CBCL, and factor analyses and reliability estimates of subscales appear to be consistent with the original data [38], [39]. Because of resource constraints at the 5 year follow up, mothers completed a short form (33 items) of the CBCL. Prior analyses using a subsample of respondents indicated a strong correlation between the short and long forms of the CBCL subscales [40]. Subscales used in the current study included internalizing (social withdrawal, anxiety and depression) and externalizing behaviour (aggression). In the present study, cases of problem behaviour at the 5 year follow up were defined using 10% cut-offs of scores on the relevant scale.
Statistical analysis
We used univariate logistic regression to estimate the risk (odds ratio (OR) and 95% confidence interval (CI)) of youth initiation of substance use for each category of 14 early life variables. Because the outcome consists of three values (never used; started at ≤14 years; or started at ≥15 years), we analysed the data using multinomial logistic regression [41]. We then developed three sets of multivariate regression models including all 14 variables in the model. In order to examine associations of early childhood factors and substance use disorder, we conducted further multivariate analyses including the 12 variables that were, in univariate analyses, significantly associated with initiation of substance use. All analyses were carried out using STATA version 9 (Stata, TX, USA) and SPSS version 14 (SPSS, Chicago, IL, USA). The number of subjects in particular analyses differed slightly due to missing data for some covariates.
To determine whether loss to follow up at 21 years affected the validity of the findings, we undertook a sensitivity analysis using inverse probability weights reflecting the chances of having missing outcome data [42] under a ‘missing at random’ assumption. We began by constructing a logistic regression model examining the association of all covariates used in the primary analyses having complete data or not. The regression coefficients from this model were then used to determine probability weights for the covariates in the main analyses. In the present study, loss to follow up was predicted by child gender, mother's education, family income, maternal smoking, and child aggression. The results from subsequent analyses including inverse probability weighting based on these factors did not differ from the unweighted analyses presented here, suggesting that the present results were not substantially affected by selection bias.
Results
Of the 3647 respondents (1915 female, 1732 male) who provided information about age of initiation of use of three substances, 49.8% (95%CI = 48.1–51.4%) reported having started smoking cigarettes at some time before 21 years, 94.8% (95%CI = 94.1–95.5%) reported having consumed alcohol and 49.5% (95%CI = 47.9–51.1%) had used cannabis previously. These proportions are comparable to national estimates of substance use. For example, the Australian Institute of Health and Welfare's report of the 2004 National Drug Strategy Household Survey estimates rates of ‘ever use’ for substances in the 21–29 age band as being 43.1% for tobacco, 94.3% for alcohol and 54.5% for cannabis [43]. The mean age of participants at first use of substances was 15.5 years (SD = 2.1) for cigarettes, 15.9 years (SD = 1.7) for alcohol, and 15.8 years (SD = 1.9) for cannabis. Early onset (at ≤14 years) of substance use was 15.4% (95%CI = 14.2–16.5%) for cigarettes, 17.4% (95%CI = 16.2–18.6%) for alcohol and 12.2% (95%CI = 11.2–13.3%) for cannabis. Of 2546 young adults (51.1% female, 48.9% male) who completed CIDI-Auto at 21 years, 16.2% (95%CI = 14.8–17.7%) had ever had nicotine abuse or dependence, 27.8% (95%CI = 26.1–29.6%) had experienced alcohol disorders and 21.9% (95%CI = 20.3–23.5%) reported lifetime cannabis disorders.
Table 1 shows the relationship between early childhood factors and smoking in adolescence and early adulthood. In univariate analyses children from lower SES families (teenage or less educated mothers, or lower income families) were more likely to smoke cigarettes in adolescence, with stronger association of early onset (before 15 years) of such use. Changes in maternal marital status during first 5 years of child's life and quality of marital relationship when the child was 5 years predicted that child's subsequent smoking and its early initiation. Mother's anxiety/depression at child age 5 was associated with slight increase in risk of her child starting to smoke by 14 years. In addition, mothers who smoked cigarettes were more likely to experience early initiation of smoking in their children. Further, children who manifested aggressive behaviour at 5 years had increased likelihood of smoking in the early teen period. When all family and individual factors were included in the same model, mother's education, changes in maternal marital status, maternal smoking and child aggressive behaviour remained significantly associated with early initiation of smoking by children.
Childhood family and individual factors predicting early onset of smoking
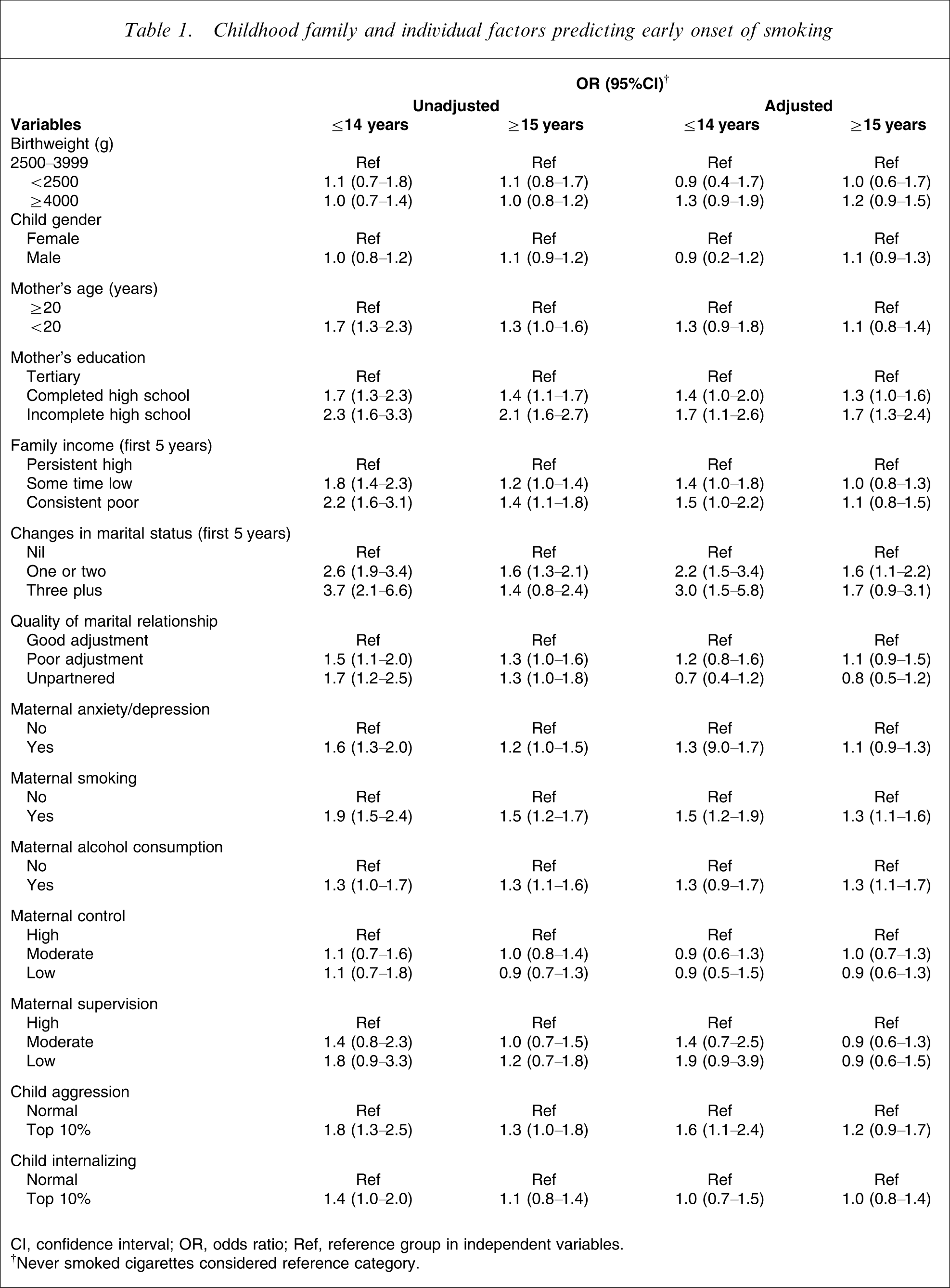
CI, confidence interval; OR, odds ratio; Ref, reference group in independent variables.
†Never smoked cigarettes considered reference category.
Table 2 presents the extent to which early childhood factors predict children's early onset to alcohol consumption. Child gender, sociodemographic background and problem behaviours at 5 years were not associated with adolescent alcohol use. But quality of maternal marital relationship, maternal smoking and alcohol consumption, and maternal supervision of child at 5 years predicted early onset to alcohol use at a younger age. The strongest association was observed for maternal drinking at 5 years (OR = 8.9, 95%CI = 5.8–13.5). Most striking is the finding that, when controlled for other covariates in Table 2, maternal alcohol consumption was the only significant factor that predicted child's subsequent alcohol consumption and its early onset.
Childhood family and individual factors predicting early onset of alcohol consumption
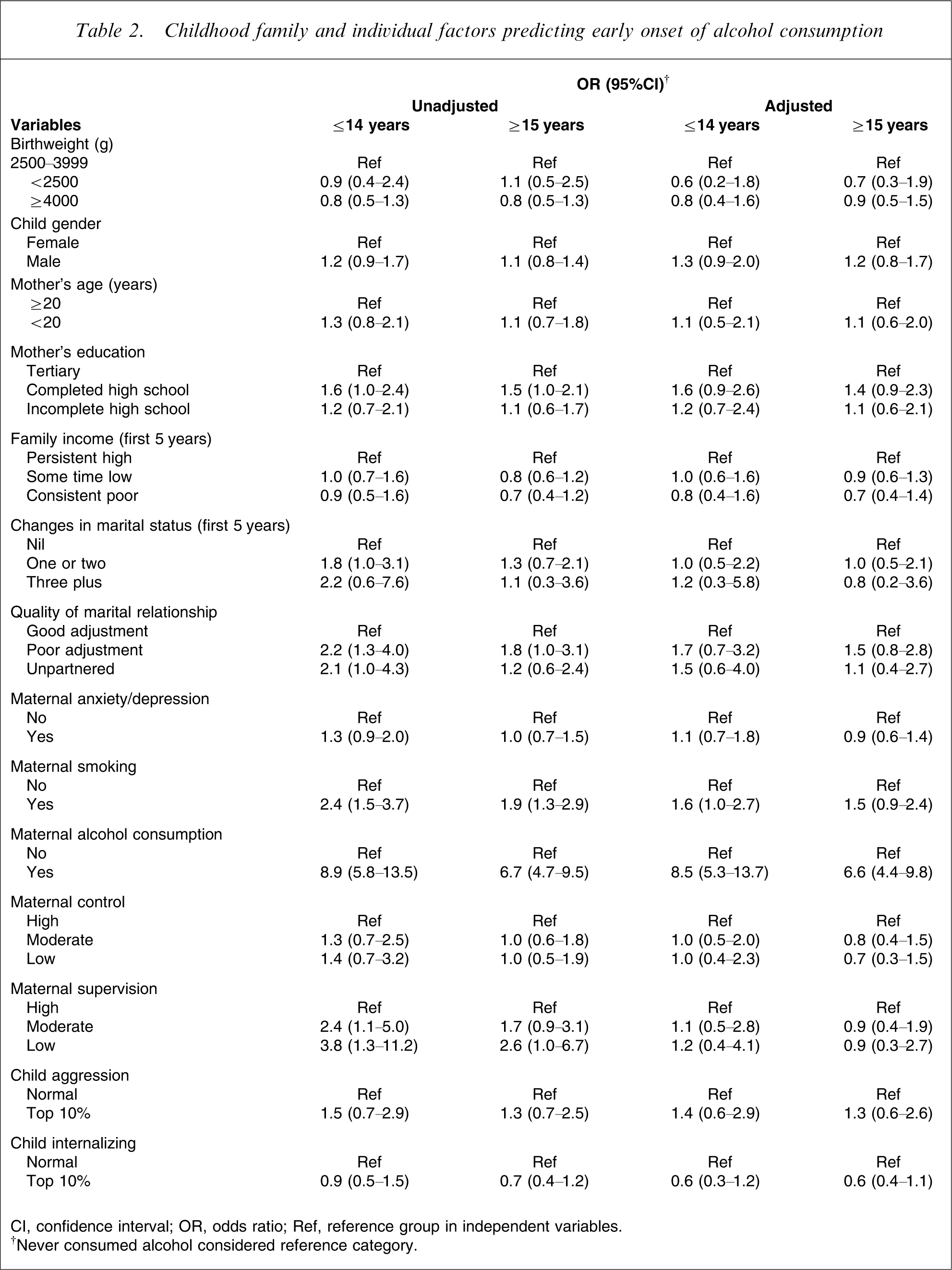
CI, confidence interval; OR, odds ratio; Ref, reference group in independent variables.
†Never consumed alcohol considered reference category.
In regard to youth cannabis use, male subjects were slightly more likely to use cannabis later in their life. Children born to teenage mothers, or who lived in families from lower economic position, or who experienced changes in their mothers’ marital status and conflict between parents had increased risk of cannabis use in early adolescence (Table 3). In addition, mother's smoking and alcohol consumption, and parenting style (control and supervision) were significantly associated with children's initiation of use of cannabis by 14 years of age. Further, children who scored in the top 10% for aggressive behaviour at 5 years were more likely than other children to begin use of cannabis in early teens. In the multivariate model, changes in maternal marital status (OR = 1.9, 95%CI = 1.2–2.9 for one or two changes; OR = 2.3, 95%CI = 1.1–4.6 for three or more changes), maternal smoking and alcohol consumption and child aggression remained independently and significantly associated with early substance use, although the point estimate of the association was attenuated compared with that seen in unadjusted analysis. Of these, changes in maternal marital status during first 5 years of the child's life appeared to be the strongest predictor of early cannabis use.
Childhood family and individual factors predicting early onset of cannabis use
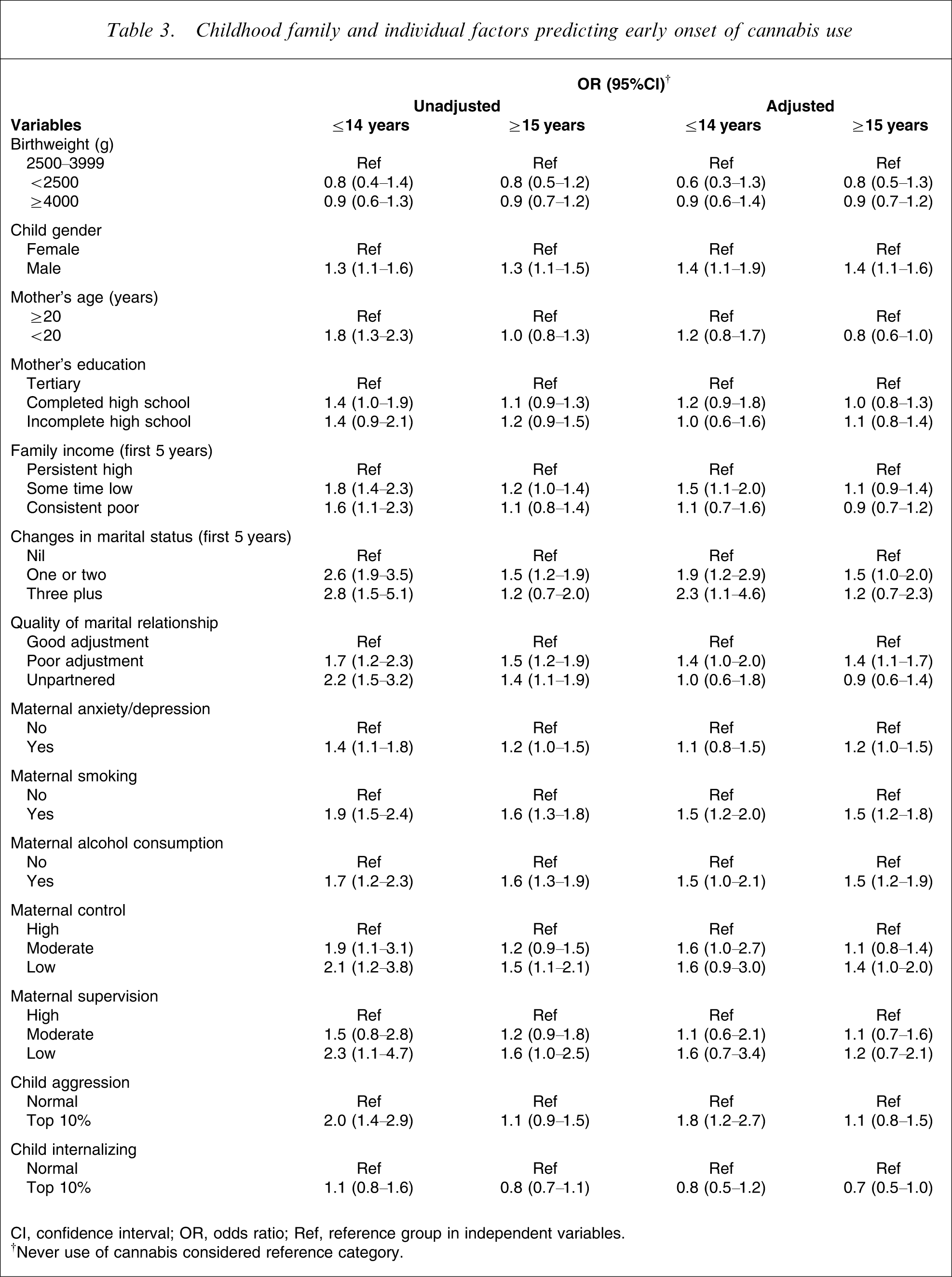
CI, confidence interval; OR, odds ratio; Ref, reference group in independent variables.
†Never use of cannabis considered reference category.
In Table 4 we examined the multivariate association between childhood factors and later development of substance use disorders by children as young adults. We included 12 variables that were significantly associated with use of any of the substances in univariate analyses. The full adjusted regression model had R2=0.08 for alcohol disorder and R2=0.07 for cannabis disorder. This means that 8% and 7% of the variability in young adults’ alcohol and cannabis disorders is explained by the variables included in fully adjusted models, respectively. Male children were substantively more likely than female children to report alcohol (OR = 3.2) or cannabis (OR = 2.6) disorders. Less educated mothers experienced greater risk of child alcohol or cannabis disorders. Children born of mothers who experienced frequent changes in marital status (three or more), or marital conflict reported greater rate of cannabis abuse or dependence but not nicotine or alcohol disorders. There was a modest association between maternal anxiety/depression and youth alcohol disorder. Further, history of maternal smoking and alcohol consumption, and low level of maternal supervision when the child was 5 years predicted that child's alcohol disorder by early adulthood. There was no independent association, however, between child aggression and later substance use disorders. Most surprising was the finding that, in the multivariate analysis, none of the childhood factors predicted subsequent nicotine abuse or dependence.
Childhood family and individual factors predicting young adult substance use disorder
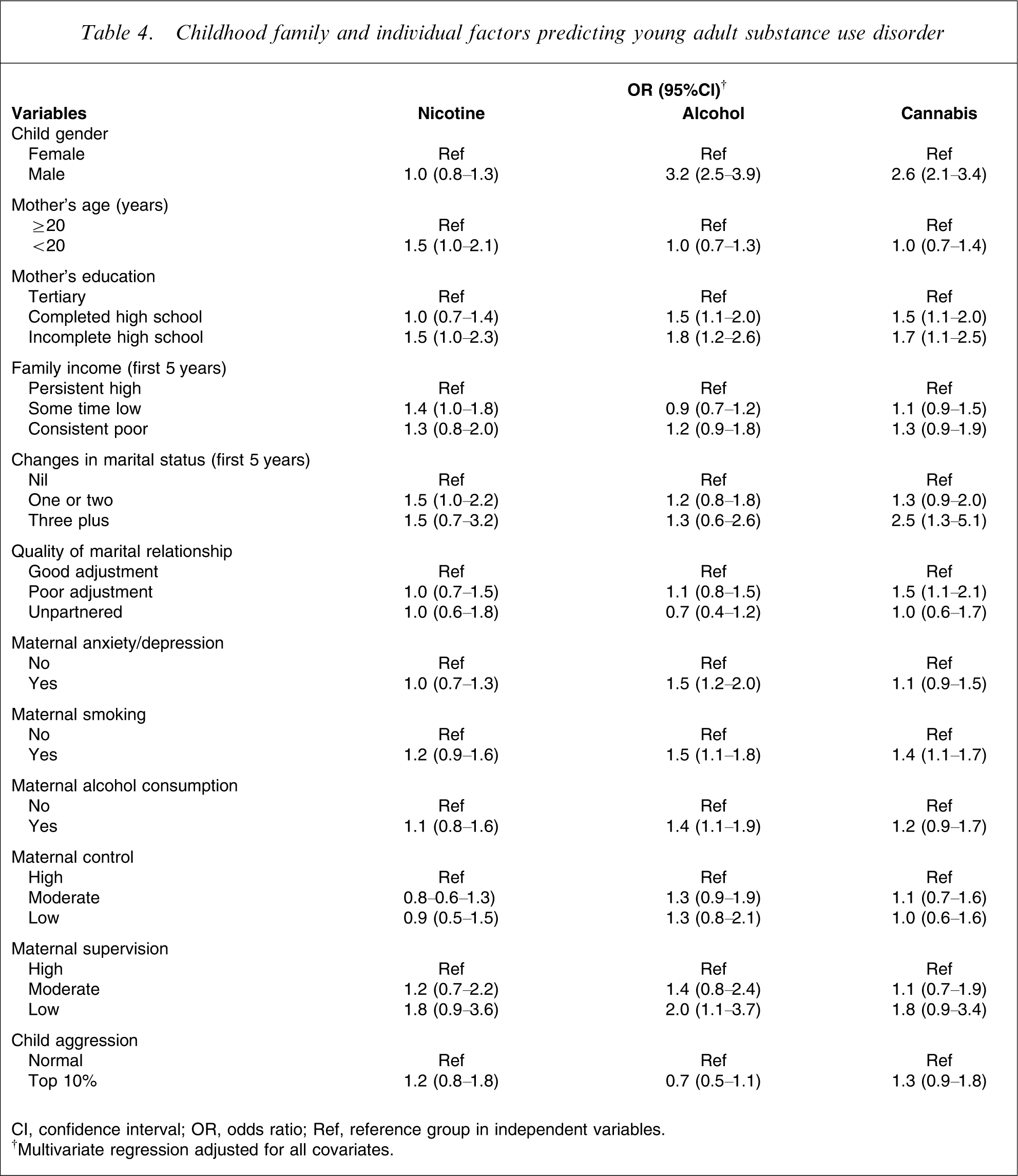
CI, confidence interval; OR, odds ratio; Ref, reference group in independent variables.
†Multivariate regression adjusted for all covariates.
Discussion
Early substance use has evident implications for explaining later drug use [3]. It is suggested that earlier patterns of substance use influence directly or indirectly the use of hard drugs and have etiological implications for subsequent patterns of substance abuse [44]. A significant body of research has implicated a wide range of factors that are used to predict subsequent substance use and abuse in adolescent and young adults [10], [11]. There is a specific need to examine early childhood factors that predict early initiation of substance use and development of substance use disorders. We examined 14 potential predictors of substance use over the early childhood period (first 5 years); of those, seven were independently and statistically significant predictors of early onset to nicotine, alcohol or cannabis, and alcohol or cannabis use disorders reported at 21 years of age.
The main findings of the present analyses were that young people who report earlier age of onset of substances are more likely to be from a low SES background (characterized with lower level of mother's education) or to have experienced changes in maternal marital status, maternal smoking and alcohol use when they were 5 years old. As well, child aggressive behaviour at 5 years independently and significantly predicted early substance use. Except for significant gender difference in development of alcohol and cannabis disorder, the same factors that predict early initiation of substance use (alcohol and cannabis) tended to predict the development of a substance use disorder. Moreover, inadequate maternal supervision of child at 5 years predicted a modest increase in alcohol disorder in participants. These data, however, suggest that childhood factors included in the present study are not able to predict nicotine disorder.
The present findings that change in maternal marital status, maternal smoking and drinking, and child aggressive behaviour are associated with early substance use are in agreement with previous investigations that have indicated the impact of these risk factors on young adults’ substance use or use disorders [16], [19], [22], [27]. Hayatbakhsh et al. and Alati et al. indicated that maternal smoking and alcohol consumption when the child was 5 or 14 years predicted that child's alcohol abuse and cannabis use in early adulthood [19], [22]. In addition to their findings, the present study suggests maternal substance use as a predictor for child's early onset of substance use and later alcohol or cannabis disorders.
These results also confirm earlier findings by others of an association between parental monitoring when the child is 8 years old and subsequent use of drugs [18]. While the finding of association between less educated motherhood, marital change, maternal smoking and child aggressive behaviour at 5 years, and early initiation of smoking is congruent with previous research, the present data do not suggest any of these childhood factors as independently predicting development of nicotine disorder by young adults. One could argue that the findings of no association between childhood risk factors and young adults’ nicotine disorder might be due to the present analytical and modelling strategy. Alternative analyses using different approaches to adjustment strategy provided results similar to those presented here. This warrants further investigation to examine risk of nicotine abuse or dependence in relation to exposure to the similar factors in later childhood or adolescence. For alcohol and cannabis, the same variables predict both early onset to use and development of alcohol disorders by young adulthood. When early substance use and substance use disorders were included in the multivariate models, the point estimates of the risk factors attenuated significantly and R2 of the predicting models incrementally increased to 11% for alcohol disorder and 33% for cannabis disorder, confirming the impact of early initiation of substance use on substance use disorder.
The present study makes an important contribution for several reasons. It has used data from a large cohort and has therefore generated relatively precise estimates of effects. Birth cohort studies provide a particular opportunity to study the causal pathways for the links between risk factors in early childhood and outcomes in adolescence through young adulthood. The present work has examined, simultaneously, a wide range of family and individual factors in early childhood and found an impact of each factors on early adolescent substance use and subsequent substance use disorders independent of other variables. To our knowledge, this is the only Australian longitudinal study that, simultaneously, has explored association of a wide range of early childhood factors and substance use and use disorders in adolescence.
Limitations
The present study had some limitations. First, a long-term gap between assessment of childhood factors (5 years) and collection of outcome measures precluded study of the impact of changes in exposure to risk factors before the development of outcomes. Second, age of initiation of use of substances was measured at the 21 year follow up by self-report. This may raise concern about measurement bias when the onset of drug use has occurred long before the measurement. But previous studies have suggested that self-reports of substance use are generally valid, and have been found to be of more use than laboratory tests and collateral reports from family members [45]. In a 10 year study of the stability of reports of substance use, Shillington et al. found that cannabis users reported their age at onset of use consistently [46]. Third, in MUSP we were unable to consider a number of potentially important factors, such as genetic predisposition, paternal mental health, and paternal and sibling smoking and alcohol consumption.
As with almost all population-based cohort studies, there has been attrition from the original cohort. Although MUSP began with 7223 mothers and their singleton offspring, at the 21 year follow up only 50.5% of offspring completed the self-report of substance use and 35.2% completed the CIDI-Auto on substance abuse and dependence. Dropout over successive follow ups was disproportionately greater for children of lower SES and those who had been exposed to family and individual problems. In the present analyses, relationships between family or individual factors and outcomes may have been attenuated or obscured by differential dropout of the more disadvantaged and high-risk participants. Previous studies on MUSP data have tested the possible impact of loss to follow up on the association between each independent variable and young adults’ outcomes [15], [16], [19], [27] using the method of inverse probability weighting [42]. These analyses indicate that it is unlikely that attrition bias would have produced spurious findings with regard to apparent effects of prospective factors. But one should continue to exercise caution in generalizing the findings to the broader population of adolescents and young adults with substance use problems, and in treating these results as a precise estimate of the magnitude of family and individual influences on outcomes.
Implications and conclusion
Notwithstanding the aforementioned caveats, the present study indicates that exposure to certain circumstances is associated with use of substances in early adolescence as well as substance use disorders. These include being children of disrupted families or drug-using parents, having been affected by problem behaviours or having experienced poor parental monitoring and supervision in childhood. Although a minor proportion of substance users or those diagnosed with substance use disorder had been exposed to the four early childhood factors, the present study raises the possibility that prevention programmes could be designed for individuals or subgroups who are at risk for early onset of substance use. Further research that explores the pathway linking these early childhood factors and substance use may help to identify, and lead to testing of, opportunities for prevention of substance use and dependence in adolescents and young adults.