
Abstract
Objectives:
Little is known about rates of childhood maltreatment in low-income countries, particularly among marginalised sectors of society. Economic hardships mean that in such countries, many children and young people are exploited in the labour force and/or are trafficked, placing them at greater risk for being exposed to other forms of maltreatment. Cultural norms endorsing the use of physical and emotional acts to discipline children further exacerbate this risk. Here, we assessed the rates of childhood victimisation experiences and associated mental health problems in Nepalese youth rescued from illegal child labour including trafficking.
Methods:
One hundred and three young people aged 12–18 years living in out-of-home care institutions and rescued from child labour/trafficking completed translated versions of selected modules from the Juvenile Victimisation Questionnaire, the Youth Inventory and the Strength and Difficulties Questionnaire. Care-home employees responsible for looking after the young people completed the Adolescent Symptom Inventory and the Strength and Difficulties Questionnaire. Analysis described maltreatment frequencies and compared individuals who had and had not experienced any form of maltreatment on the presence/absence of psychiatric diagnoses.
Results:
Seventy-two percent of participants experienced some form of maltreatment in their lifetime. Rates for each maltreatment type were 46.6% for physical abuse, 40.77% for emotional abuse, 27.2% for sexual abuse and 33% for neglect. Symptoms indicative of anxiety disorders and trauma were commonly reported especially in victims of childhood maltreatment.
Conclusions:
Our estimates of physical abuse in this at-risk juvenile sample were commensurate to those reported in general-population youth samples in Nepal, but sexual and emotional abuse rates were somewhat lower. The potential presence of anxiety and trauma in this sample that may result from maltreatment requires replication, but underscores an urgent need for routine mental health screening in rescued child labourers during rehabilitation efforts.
Introduction
Childhood maltreatment is a significant global health and social problem (World Health Organisation (World Health Organization [WHO], 2002). Early experiences of physical, sexual and emotional abuse and neglect are strongly associated with non-communicable mental (Scott et al., 2012) and physical health conditions (Archer et al., 2017), impacting individuals and the economy (WHO, 2002). Although childhood maltreatment occurs globally (Hovdestad et al., 2015), there is a gap in knowledge about cases from specific low- and middle-income countries (WHO, 2014). Economic hardships in these countries mean that children and young people can be exploited in the labour force, which in turn may increase exposure to other forms of victimisation. Yet cultural practices and social stigma associated with childhood maltreatment in many of these countries means underrecognition of these problems, especially their impact on mental health. Nepal is one such country where there is a paucity of data on childhood maltreatment (Hillis et al., 2016). Where available, studies have assessed abuse and neglect in general-population youth samples using non-standardised definitions. The primary objective of this study is to gather data to inform the scope of child maltreatment in Nepal, but among one of the most disadvantaged sectors of society, by measuring lifetime rates of maltreatment in young people with a history of child labour. A secondary objective is to explore rates of current psychiatric conditions and emotional and behavioural problems in this at-risk juvenile population, particularly elevations in symptoms associated with maltreatment.
Nepal is a landlocked country in South Asia, sharing a border with India and China. Nepal has a population of 28.98 million people and a GDP of 21 billion dollars (Forbes, 2017). Classified as a low-income country, a quarter of the population falls below the poverty line (Forbes, 2017). Because the agriculture industry in Nepal provides a livelihood to approximately two-thirds of the Nepalese population, the country’s geographical location and exposure to natural disasters has had a large impact on economic growth (The World Bank, 2016). The high poverty rate and limited resources available to enforce labour laws have created an environment, in which children are at a great risk of exploitation (Child Labour and Forced Labor Reports, 2017). Indeed, despite the Child Labour (Prohibition and Regulation) Act (2000), which prohibits children below the age of 14 years being employed as labourers, Nepal accounts for 1.6 million children aged 5–17 years in child labour, with estimates of 39.1% of school children employed (Government of Nepal, Ministry of Education, 2016). Among working children, 621,000 are estimated to be involved in hazardous work (Child Labour in Nepal, 2017), such as being employed for farming, making bricks, quarrying, construction or domestic work. Sexual exploitation and forced labour as a result of human trafficking are also common: following the 2015 earthquake, Nepal saw an increase of 40% of human trafficking (Trafficking in Persons [TIP], 2017).
Conditions of economic exploitation in Nepal leave many young people vulnerable to maltreatment. Studies of general-population samples ascertained in Nepal report that the use of physical disciplinary acts is common in youth (Atteraya et al., 2018; Kandel et al., 2017; Rajbanshi, 2012) with almost one in two children experiencing moderate forms, for example, being spanked, hit or slapped on the bottom, and a significant number (21.5%; Atteraya et al., 2018) experiencing severe forms, for example, hit with an object. Emotional abuse is also common with more than three-quarters reporting these experiences (Atteraya et al., 2018; Rajbanshi, 2012). Finally, sexual abuse is also present, with one study of 150 students attending a public high school in Kathmandu reporting rates of 41.3%. Thus, despite using different definitions of these various forms of maltreatment across studies, estimates appear relatively similar. Furthermore, most of these figures fall within the range of figures of past-year violence reported across countries in Asia of 64% and 80% of children and young people (Hillis et al., 2016), respectively; although this systematic review did not include data from Nepal.
In summary, consistent with cultural practices and norms that endorse corporal punishment and verbal humiliation as a way to encourage children to become responsible and competent (Khanal and Park, 2016), the use of physical and emotional acts to discipline young people is common in Nepal with the presence of more severe forms of childhood maltreatment also considerable (Atteraya et al., 2018; Kandel et al., 2017). Although one study reported that children who were engaged in child labour activities were more likely to receive any kind of physical punishment than those not engaged in such activities (Kandel et al., 2017), general-population studies are less informative around rates of childhood maltreatment within more economically marginalised sectors of society in Nepal. Nor are they informative on the effects of childhood maltreatment on psychiatric disorders and psychopathology. This study assessed the frequency of childhood maltreatment in adolescents rescued from illegal child labour. We also assessed potential current psychiatric disorders, as well as current emotional and behavioural problems in this sample, with analyses assessing their associations with the presence of childhood maltreatment. To identify the most vulnerable individuals within our sample, additional exploratory analyses assessed associations between types of maltreatment and gender or age groups. Although data gathered on maltreatment and mental health in rescued child labourers may not be directly generalizable to children and young people currently illegally exploited in the labour force, nonetheless, they do reflect the victimisation experiences of those with a history of child labour and how these can impact their mental health. In turn, this has policy implications for the need for additional resources dedicated to the screening of adverse experiences, mental health needs and treatment in young people who are rescued from child labour.
Methods
Sample
The participants comprised 103 young people aged 12–18 years living in eight different care-homes in Kathmandu valley (11% of participants were from care-home 1, 23% from care-home 2, 2% from care-home 3, 16% from care-home 4, 14% from care-home 5, 15% from care-home 6, 13% from care-home 7 and 9% from care-home 8). All care-homes provide residential facilities for children and young people with a range of referral reasons: rescued child labourers, street children, orphans, those who had run away from home or were lost. Their purpose was to house young people and where appropriate, to facilitate re-integration within their families. We approached 15 care-home directors with our eligibility criteria: participants had to be aged 12–18 years, report a history of child labour and did not have a medical disability (through available medical records and later verified by young person themselves before taking consent). We excluded on the basis of having a medical disability because we wanted to assess the association between victimisation experiences and psychiatric symptoms without the confounding influences of other medical conditions. Eight homes agreed to participate because a large number of the young people who they accommodated met our eligibility criteria. Of the remaining homes, six were excluded from participation because they accommodated very few (<5) young people who were rescued child labourers; rather they were designed to accommodate more specific groups of young people: those who had been sexually victimised, those who had been living on the streets and those who had been abandoned. One remaining home declined participation in the study not only because it was time-consuming, but also because only five young people in their care had been formerly employed as a child labourer. In the eight care-homes who had agreed to participate, all eligible young people were provided with the study information, and all of these agreed to participate (100% response rate). All young people and a designated care-home employee responsible for that young person (the ‘keyworker’) provided informed consent. Of note, a literacy test was used to confirm young people’s ability to consent to the study.
Procedures
Permission for this study was granted by the Research Division Office of the Rector Tribhuvan University and by the Central Child Welfare Board (CCWB) under the Ministry of Women, Children and Social Welfare. Ethical approval was sought from and given by the Nepal Health Research Council (Ref. No. 1386; 14 February 2017). As none of the standardised measures were available in Nepalese, we sought permission from the publishers/authors to create a Nepalese version. The local Nepalese investigators (S.D., S.N., N.P.S. and S.S.) first discussed items for cultural relevance. Where an item was not culturally relevant, an alternative was proposed and discussed with other investigators (R.K., V.K. and J.L.). Once agreement had been reached across investigators, the instructions, existing and modified items for the measure, were translated by a professional translator. This was then back-translated by the local Nepalese investigators and checked by J.L. for any discrepancies in meaning with the original English version. Any discrepancies were noted and returned to the local Nepalese investigators and resolved through another round of translation or back-translation depending on where the discrepancy arose. Up to four rounds of translation and back-translation were conducted for some measures. Where the original authors of the scale were available, they also provided feedback on the cultural modifications and the back-translations. The final Nepalese version was piloted for readability.
During testing, participants completed two tests of non-verbal cognitive ability (Wechsler Abbreviated Scale of Intelligence–Second Edition), the Strength and Difficulties Questionnaire (SDQ, Goodman, 1997), the Juvenile Victimisation Questionnaire (JVQ; Finkelhor et al., 2005) and the Youth Inventory-4R (Gadow et al., 2002). Of note, because the tests of non-verbal cognitive ability were used to select participants to a second study assessing the cognitive phenotype of maltreatment (reported elsewhere), they are not reported further here. In addition, 21 care-home employees (across the 8 care-homes) who were the designated ‘keyworker’ for each participant provided information on the participants’ demographics and work history and the characteristics of the care-home. This information was gathered to describe our sample but also to enable comparisons of the findings of future studies of rescued/non-rescued child labourers who may share some but not all of these characteristics. Keyworkers also completed the Adolescent Symptom Inventory (ASI-4; Gadow et al., 2002) and the parent version of the SDQ. These keyworkers frequently interacted with the participants and were deemed the best informants of the child’s background and behaviour. The length of time a keyworker had known the child ranged from 3 to 96 months (mean length = 22.83 months, SD = 19.46 months). At the end of the assessment, the participants were given a non-monetary gift to say thank you.
Measures
Demographics, work history and care-home characteristics
Keyworkers’ provided participants’ genders, dates of birth, ethnicities, age that the young person started working, length of time in months that they had worked, the (average) amount of time spent working each day (in hours) and each week (in days), the type of work and reasons for working. Keyworkers also reported on care-home details including the total number of employees, the maximum capacity of young people at any one time, the current number of young people, the maximum length of stay for any young person and the availability of medical, psychological and educational services and resources.
Maltreatment history
The JVQ (Finkelhor et al., 2005) assessed maltreatment history and other victimisation experiences. Made up of 34 modules describing offences against youth, these modules cover five domains of victimisation: Conventional Crime (8 modules), Child Maltreatment (4 modules), Peer and Sibling Victimisation (6 modules), Sexual Victimisation (7 modules) and Witnessing and Indirect Victimisation (9 modules). Because of our interest in maltreatment, we administered all 4 modules for Child Maltreatment. This asked the young people to report on experiences of physical abuse, psychological/emotional abuse, neglect and custodial interference. All full modules can be further accompanied by additional supplementary questions. For the neglect module (within Childhood Maltreatment), we included an additional five supplementary neglect items (neglect due to guardian substance abuse, guardian gone missing, guardian inviting dangerous guests, guardian lack of care for child’s hygiene and living in an unsafe home). Given time constraints, abbreviated versions of the Conventional Crime and Witness and Indirect Victimisation were used, with no modules from the Peer and Sibling Victimisation domain and only two modules of the sexual victimisation domain included (sexual assault by known adult and non-specific sexual assault). The Conventional Crime asks participants whether they have experienced robbery, personal theft, vandalism, assault with weapon, assault without weapon, attempted assault, kidnapping and any form of victimisation that arose because of discrimination due to skin colour, religion, ethnicity, physical problems or sexual orientation. The Witnessing and Indirect Victimisation asks whether participants had witnessed domestic violence, parent assault of sibling (with/without weapon), burglary of family household, murder of family member/friend, murder of unknown, exposure to shooting/terrorism/riots and war/ethnic conflict.
Across the events described within all modules, participants were asked whether they had occurred in their lifetime. If the participant answered ‘yes’ to any of these events described in each module, they were scored as experiencing that type of victimisation and were asked whether the event had occurred in the last year, an estimate of the total number of times the event had occurred and the approximate age of onset. Follow-up questions also probed the nature, impact and severity of the event and, if applicable, details of the perpetrator across the lifetime experience. The English version of the JVQ has appropriate reliability and validity (Finkelhor et al., 2005).
Potential psychiatric diagnoses
The YI-4R (Gadow et al., 2002) and ASI-4 (Gadow et al., 2002) are 120-item scales that assess potential psychiatric diagnoses consistent with the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) classification and criteria. For the YI-4R, participants were asked to consider how frequently they experienced each item NOW on a 4-point scale (0 = never to 3 = very often). As it was unlikely that participants could access drugs while living in the care-home, for items on substance use/abuse, participants were asked about their lifetime occurrence. Keyworkers completed the ASI-4, rating the frequency of participant behaviours on the same scale (0 = never to 3 = very often) again considering current patterns of behaviour (except substance use/abuse).
Emotional and behavioural problems
The SDQ (Goodman, 1997) assesses current symptoms of psychopathology across 25 items divided into five subscales: emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems and prosocial behaviour. Participants rated how true the statements were on a 3-point Likert-type scale (1 = ‘not true’ to 3 = ‘certainly true’). Care-home employees completed the SDQ: parent version, which comprises the same 25 items (Goodman, 1997). Cronbach’s alpha for the self-reported scales were 0.662 for emotional problems, 0.440 for conduct problems, 0.278 for hyperactivity/inattention, 0.373 for peer problems and 0.691 for prosocial behaviour. For the carer reported subscales, these were: 0.594 for emotional problems, 0.683 for conduct problems, 0.543 for hyperactivity/inattention, 0.341 for peer problems and 0.781 for prosocial behaviour.
Data analysis
Participant demographics, their work history and care-home characteristics were presented first followed by frequencies and characteristics of any lifetime experiences of the various victimisation events assessed through the JVQ. Gender (male vs female) and age group (12–14 years vs 15–18 years) differences in each type of victimisation using chi-square tests were presented. Potential current psychiatric diagnoses using self and keyworker report (YI-4R and ASI-4) and current emotional and behavioural symptoms (mean SDQ subscale scores) were presented next. To assess the association between experience of childhood maltreatment and potential DSM diagnoses, individuals who had experienced any form of maltreatment (physical abuse, psychological/emotional abuse, sexual abuse, neglect) were compared with those who did not report maltreatment on the presence/absence of each diagnosis, using chi-square statistics. As the internal consistency statistics of SDQ subscales either using self or carer reports limits the interpretations of their associations with victimisation experiences, descriptive analyses and analyses comparing those who had and had not experienced childhood maltreatment on emotional and behavioural problems are not presented.
Results
Participant and care-home characteristics
Demographics
There were 38 boys (36.9%). The mean age of the participants was 14.97 years (SD = 1.53 years). Less than half of the participants (43.7%) were aged 12–14 years; 39.8% of the respondents were Tamangs and 26.2% were Brahman/Chhetri. Other participants were from the Dalit, Newar, Rai/Limbu, Gurung and Terai/Medeshi ethnic groups.
Work history
Participants first started work from the ages of 5–16 years (M = 10.6 years, SD = 2.20 years). The amount of time participants worked as child labourers before being rescued ranged from 3 months to 8 years (M = 2.24 years, SD = 0.25 years). Participants worked 4–21 hours a day (M = 13.0 hours, SD = 4.71 hours) and 2–7 days a week (M = 6.19 days, SD = 1.38 days). More than one-third (35%) of participants were domestic workers, 28.2% worked in factories, 21.4% worked in hotels, 4.9% in transport, 3.9% in entertainment bars, 1.9% in construction and the remaining 5% in either shops, hostels, massage parlours or on the street. Approximately half (53.4%) said that their reason for working was living in poverty.
Care-home variables
The eight care-homes from where these participants resided varied from having 9 to 20 paid keyworkers. Of these care-homes, 1 was for boys only, 3 were for girls only and the remaining 4 were mixed gender. Except for one care-home, which currently housed more young people than the maximum capacity, all other care-homes were not full; current occupancy fell between 8 and 196. All care-homes provided access to medical doctors and psychologists and academic and vocational educational opportunities. All care-homes had provisions for young people to take high-school board exams.
Maltreatment history
Seventy-four (72%) young people had experienced some form of childhood maltreatment (physical abuse, sexual abuse, psychological/emotional abuse, neglect) in their lifetime. Most participants (68.9%) experienced three or more types of victimisation.
Lifetime rates of specific forms of victimisation experiences including physical, emotional and sexual abuse are presented in Table 1 for the whole sample, split by gender and age group. Less than half of the sample had experienced physical abuse, with 62.7% of these acts committed by perpetrators outside of the family and 37.3% within the family, where within family included ‘parent, sibling and relative who lives with you’, while extra-familial included ‘grown up not residing in home, romantic partner, stranger and other’; 20.4% participants thought they experienced more than four physically abusive acts in their lifetime, and the mean age of the first abusive event was estimated at 10.27 years across participants. In terms of severity, 81.3% described themselves as being physically hurt after the event and 22.9% were hospitalised; 72.9% reported feeling ‘very afraid’ to these events. Just less than half of the sample experienced emotional abuse, with 71.4% of these acts committed by perpetrators outside of the family and 28.6% within the family. Of the participants, 19.4% thought they experienced more than four emotionally abusive acts in their lifetime, and 50% described themselves as feeling ‘very afraid’ to these events. The mean age of the first emotional abusive event was thought to be approximately 11.38 years. Just over a quarter of the sample had experienced sexual victimisation, with 92.9% detailing these acts to be committed by a known perpetrator. A third of the sample reported experiencing neglect, with 18.5% participants estimating that the average occurrence of neglect across one’s lifetime being more than four times. The mean age of the first event was approximately 9.67 years. In addition, 23.3% of young people reported experiencing family abduction, 35.9% reported having to look after themselves due to guardians being intoxicated, 40% stated they had to go looking for a parent, 16.5% stated their guardians had people in the family home who the young person was afraid of, 20.4% reported living in a broken down/unsafe/unhealthy home and 20.4% reported their guardians not caring if they were clean or wore clean clothes. When asked to think back to these events, half of the sample recalled feeling ‘very afraid’. Notably, most participants had been exposed to conventional crime and indirect forms (including witnessing) of victimisation.
Victimisation in relation to gender and age group.
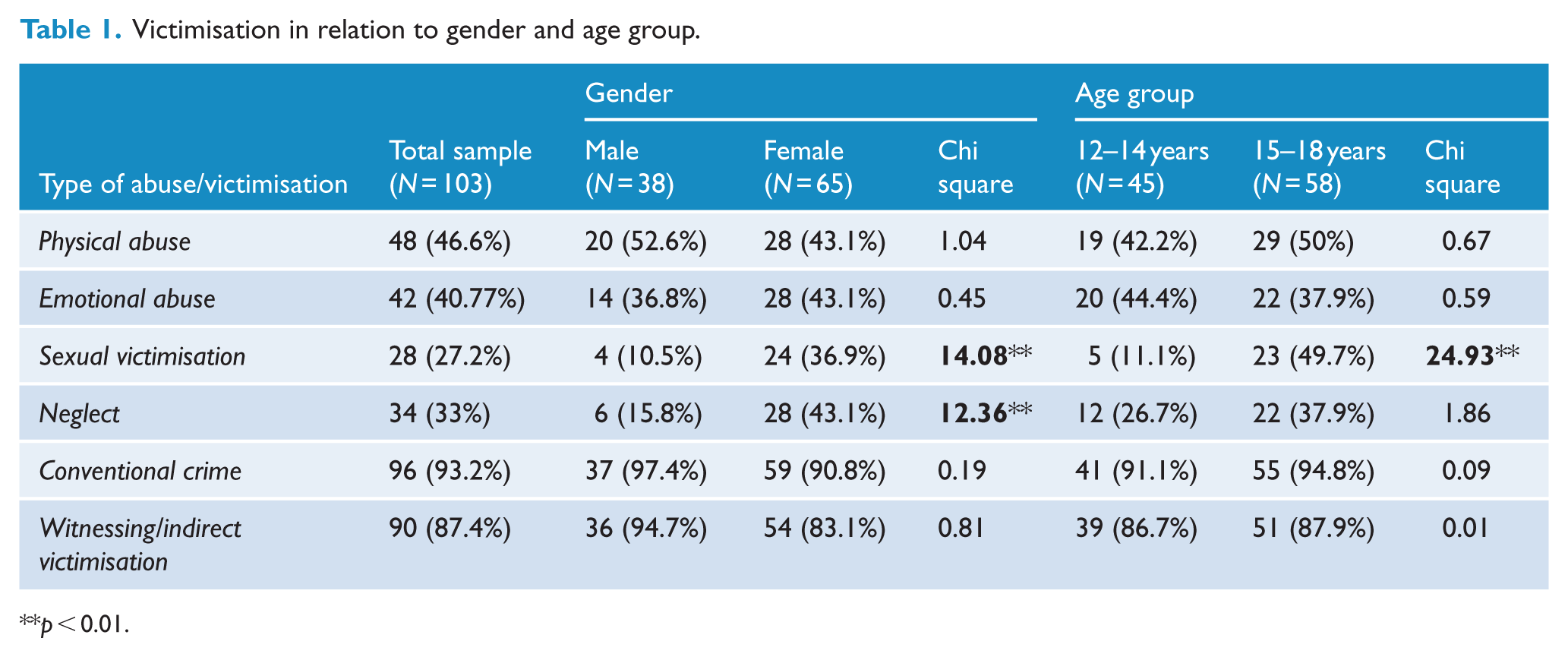
p < 0.01.
Chi-square analyses showed that girls reported more sexual victimisation and neglect than boys, and older adolescents reported more sexual victimisation than younger adolescents (Table 1).
Potential psychiatric diagnoses and current emotional and behavioural problems
Table 2 presents the numbers of individuals potentially meeting DSM-IV criteria for current psychiatric diagnoses using self and keyworker report. The most commonly reported conditions by young people were anxiety disorders (specific phobia, social phobia, separation anxiety and panic attacks); rates of these same anxiety disorders were somewhat lower using keyworker reports. In contrast, keyworkers reported behaviours consistent with posttraumatic stress disorder (PTSD) in around half of the young people, which was far higher than that reported by young people themselves.
Numbers of participants meeting criteria for various DSM-IV diagnoses.
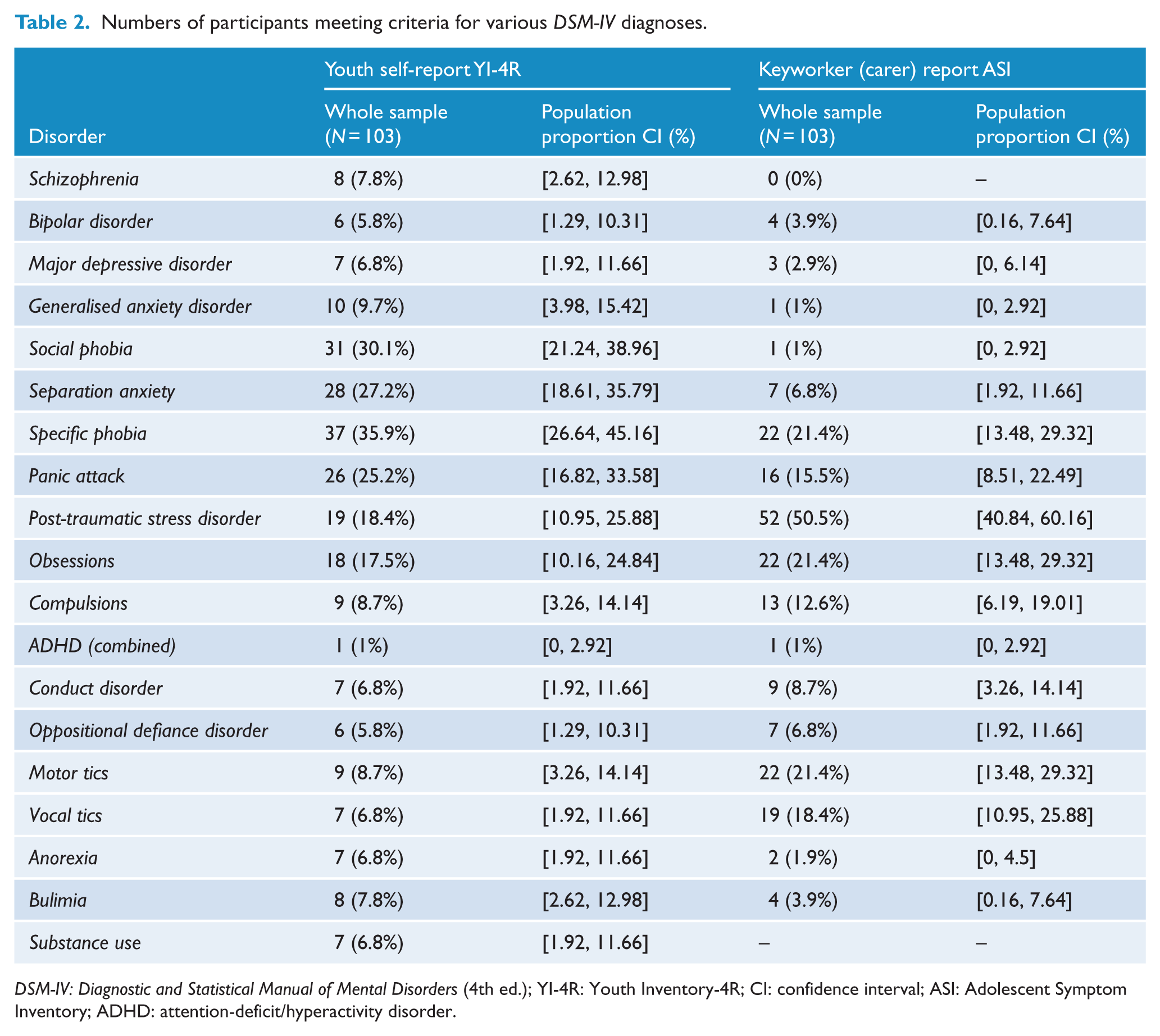
DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); YI-4R: Youth Inventory-4R; CI: confidence interval; ASI: Adolescent Symptom Inventory; ADHD: attention-deficit/hyperactivity disorder.
Links between maltreatment experiences and psychiatric history
Individuals who had experienced any form of childhood maltreatment (n = 74) were significantly more likely to self-report generalized anxiety disorder (GAD), χ2(1) = 7.11, p < 0.01; PTSD diagnoses, χ2(1) = 7.13, p < 0.01; motor tics, χ2(1) = 5.62, p < 0.05 and major depressive disorder (MDD), χ2(1) = 4.89, p < 0.05 than those without a history. On keyworker reports, those without a history of childhood maltreatment were more likely to meet a diagnosis for conduct disorder, χ2(1) = 10.49, p < 0.01; vocal tics, χ2(1) = 4.62, p < 0.05 and anorexia, χ2(1) = 5.14, p < 0.05.
Discussion
In this study, we report on levels of childhood maltreatment and victimisation in a sample of young people rescued from economic exploitation in Nepal. A number of our findings deserve comment.
First, our data from a socially and economically marginalised sample revealed that overall nearly three-quarters had experienced some form of childhood maltreatment – estimates exceeding the 50% rates projected from a recent review of Asian countries likely to have experienced some form of abuse (Hillis et al., 2016) although data from Nepal were not included in such projections. For specific forms of maltreatment, it is striking that our marginalised sample did not report higher rates compared to general-population youth samples. Almost half of young people were victims of physical abuse, which were higher than the moderate physical disciplinary acts reported in nationally representative cohorts of Nepalese youth (Kandel et al., 2017), but commensurate with those reported in students attending a public school (Rajbanshi, 2012). Our rates of sexual and emotional abuse (around a quarter and a half, respectively) were also lower than those reported in general-population samples. Moreover, only about one-third of the sample reported neglect. It may be that being rescued and in care attenuates further reports of maltreatment. Alternatively, any elevation in maltreatment experience in our sample could occur in the intensity and severity of maltreatment rather their presence per se. Discrepancies across studies could also arise from the use of different definitional criteria for each form of childhood maltreatment. Unlike previous studies, here we used standardised definitions (albeit translated) from a measure that has been widely used in Western countries. It may be that by adopting stricter criteria particularly for less overt forms of maltreatment such as emotional abuse, inflated estimates are less likely. As our data indicate the feasibility of using such a measure in Nepalese youth, this measure has potential to be applied to general-population samples to more systematically assess childhood maltreatment. However, the psychometric properties need to be established first. Our data also flagged, commensurate with many childhood maltreatment samples, wide exposure to other victimisation experiences (victims/witnesses of conventional crime) and considerable co-occurrence of these experiences. It was also suggested that particular gender and age groups were more likely to have experienced particular forms of maltreatment. If replicated, these findings may point to special screening of sexual victimisation among females and older adolescents rescued from child labour.
Second, our data add to the growing body of literature pertaining to mental illness in Nepal. Self-reports of symptoms suggested that anxiety disorders could potentially be common in our sample, while keyworkers highlighted symptoms indicative of trauma. While self-reported rates of potential schizophrenia and bipolar disorder were somewhat elevated relative to global prevalence estimates (Charlson et al., 2018), rates of potential attention-deficit/hyperactivity disorder (ADHD; self and keyworker reported) appeared remarkably low, against global estimates (Polanczyk et al., 2007). Given the small size of our sample, the paucity of psychometric data on the translated measurement tools, and the general lack of awareness of mental health diagnoses in Nepal, it is difficult to ascertain without further replications, whether these unexpected findings are a reflection of the adversity experienced by our sample within a new cultural context, which may exacerbate or inhibit the psychiatric expression of economic exploitation and/or victimisation. Importantly, our data speak also to linkages between mental illness and adversity: the presence of any form of childhood maltreatment was significantly associated with many of the more commonly reported psychiatric problems (anxiety, PTSD) when using self-reports to generate potential diagnosis and conduct disorders when using keyworker reports. Data from other countries consistently show powerful associations between early-life maltreatment and behavioural and emotional difficulties during development and a life-course of poor mental health (Afifi et al., 2014; Scott et al., 2012; Taillieu et al., 2016). In Nepal, existing studies also show that child labourers report higher anxiety levels than those attending school (Alaraudanjoki, 2003). There are also overall higher levels of PTSD symptoms in child soldiers in Nepal (Kohrt et al., 2016).
Our findings are caveated by a number of limitations. As well as being small in size, the representativeness of our sample to young people who are currently being exploited economically is unknown given that our participants had been rescued from economic exploitation and in care for some time with access to medical doctors and psychologists, as well as academic and vocational educational opportunities. With 39.1% of school children reportedly employed in child labour in Nepal (Government of Nepal, Ministry of Education, 2016), it is not known what proportion is rescued. Because of this, our findings can only inform outcomes in those who have a history of economic exploitation – which is still important for determining the need for screening and interventions among those who are fortunate to be rescued. Second, while we did attempt to use standardised measures, well-validated in English and among Western populations, we do not know the psychometrics of our translated measures. For example, our continuous measure of psychopathology, the SDQ, showed poor internal consistency, and analyses involving these subscales could not be clearly interpreted. The links between possible psychiatric diagnosis and childhood maltreatment were also somewhat different for self versus keyworker reports. Although multi-rater data are preferable to single-rater data in terms of potential reliability, these discrepancies add to difficulties in interpretation. It is unclear whether these discrepancies emerge because carers are less aware of and therefore under-report internalising symptoms such as anxiety and depression, while over-reporting externalising symptoms such as conduct problems than self-reports (e.g. Sourander et al., 1999; Van der Meer et al., 2008). However, for others, such as trauma, psychosis and bipolar disorder, the discrepant results are more difficult to decipher. Future studies should investigate the psychometric properties of these translated measures in community samples as well as in looked after children in Nepal to aid interpretation of findings. Finally, we used a cross-sectional design and relied on retrospective recall of maltreatment. This limits any interpretations of temporal links with psychiatric disturbances and memory biases may serve to over- and underestimate events and their nature.
In summary, these data are among the first to report the presence, frequency and nature of childhood maltreatment and broader victimisation experiences and their associations with mental health conditions, in a socially and economically marginalised sample. While the prevention of economic exploitation (and associated victimisation experiences) is a long-term goal for Nepal, a short-term intermediate goal could be the provision routine screens for mental health problems in this sample and early referral routes to prevent lifelong effects on mental health. This is particularly true for common, debilitating conditions linked to maltreatment histories such as anxiety, depression, trauma and conduct disorders. However given the limited resources of developing countries, this can be challenging to governments in terms of allocating funds and implementing policies. In Nepal, 3% of the national budget is allocated to health, out of which 1% is allocated to mental health (Jordans et al., 2007). While current care-homes provided access to medical doctors and psychologists, it is unclear whether these are sufficient to protect against the negative impact of childhood maltreatment and victimisation experiences on psychiatric disorders. Before these policy and clinical implications are realised, these findings need to be replicated in larger, longitudinal studies with validated measures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the UK Medical Research Council (MR/N006194/1) and the Department of Biotechnology, India (BT/IN/DBT-MRC/DFID/20/RP/2015-16).