
Abstract
Several symptom subtypes of obsessive–compulsive disorder (OCD) have been identified on the basis of the predominant obsessions and compulsions. The objectives of the present article were to review the literature on the relationship between OCD symptom subtypes and treatment response and to suggest strategies that might assist with the choice of treatment and improve treatment outcome in patients with various subtypes. An extensive literature search was performed, relevant studies were identified, and their results reported. Overt compulsions were generally associated with a relatively good response to the behaviour therapy technique of exposure and response prevention (ERP) and with poorer response to serotonin re-uptake inhibitors (SRIs). Washing/cleaning and checking compulsions tend to respond well to ERP, whereas the majority of studies show that washing/cleaning compulsions are associated with a poorer response to SRIs. Most studies suggest that patients with the symmetry, ordering and arranging subtype do not fare worse with ERP and SRIs than patients with other symptom subtypes. Some studies suggested that obsessions might respond to SRIs somewhat better than to ERP. In the majority of the studies, hoarding and the subtype characterized by sexual or religious obsessions and absence of overt compulsions (‘pure obsessions’) have been associated with poor response to ERP and SRIs. It was concluded that treatment strategies cannot be precisely tailored to OCD symptom subtypes. Many other factors influence the outcome of treatment and need to be considered along with the symptom subtypes when making decisions about treatment. While ERP and SRIs remain the mainstay of treatment regardless of the symptom subtype, the addition of cognitive therapy techniques and/or antipsychotic medications may enhance treatment response in the presence of certain features discussed in the article.
Keywords
Patients with obsessive–compulsive disorder (OCD) present with various symptoms and behaviours. Subtypes of OCD based on the type of obsessions and compulsions (henceforth referred to as ‘symptom subtypes’) have been identified by many factor and cluster analytic studies. The results of these studies have been more consistent for some subtypes and less consistent for others, but they converge to suggest that there are approximately five subtypes [1–12]. These include (i) contamination obsessions with washing/cleaning compulsions; (ii) doubting obsessions with checking compulsions (but in some studies aggressive obsessions are linked with checking compulsions or referred to as ‘harming’); (iii) obsessions (often of a sexual, religious, aggressive or somatic nature) without overt compulsions, also known as ‘pure obsessions’; (iv) symmetry obsessions with ordering and arranging compulsions (sometimes also accompanied by obsessions related to exactness/perfectionism, compulsions involving repeating and counting, and ‘obsessional slowness’); and (v) hoarding obsessions and collecting compulsions (referred to as ‘hoarding’).
The boundaries between these OCD subtypes are not always clear, and many patients exhibit obsessions and compulsions from different subtypes. For example, some patients with contamination obsessions resort to excessive checking to make sure that they have not been contaminated. One study found that 72% of OCD patients presented with more than one obsession and 58% had more than one compulsion [13]. Despite this, certain obsessions and compulsions often dominate the clinical picture when multiple symptom subtypes exist. Studies also show that over time, adult patients tend to maintain symptoms within the same subtype [14], [15].
The behaviour therapy technique of exposure and response prevention (ERP) and serotonin re-uptake inhibitors (SRIs; clomipramine, fluvoxamine, fluoxetine, sertraline, paroxetine, citalopram, and escitalopram) are widely accepted as first-line treatments for OCD [16], [17]. Cognitive therapy for OCD may be administered alone, but it is usually delivered with ERP as cognitive behaviour therapy (CBT). When patients fail to respond to ERP or SRIs, other psychological techniques or pharmacological agents may be added. Psychological and pharmacological treatments are commonly combined, but opinions differ as to whether such a combination is superior, and when and how to administer it. Treatment of OCD can be effective, but results are often not impressive, especially considering that the usual criteria for treatment response in OCD (30–35% decrease in the Yale–Brown Obsessive Compulsive Scale scores (Y-BOCS) [18]), although clinically meaningful, are less stringent than the corresponding criteria for many other psychiatric disorders. For example, one study reported that during a 2 year period only 12% of patients achieved a full remission after treatment and 47% showed some improvement [19]. At least 30% of adequately treated OCD patients are considered treatment resistant, with disabling symptoms and significantly impaired functioning [20].
This article reviews the existing literature with regards to the relevance of OCD symptom subtypes for treatment outcome. Different psychopathological and psychobiological mechanisms underlying different OCD symptom subtypes may affect treatment in ways that contribute to the generally unsatisfying treatment results. The present article aims to shed more light on the links between OCD symptom subtypes and response to various treatments and to suggest strategies that might assist with the choice of treatment and improve treatment outcome in patients with particular subtypes.
Methods
Electronic searches were conducted on Medline, PsychINFO, CINHAL, EMBASE, and Cochrane. Search terms included, but were not limited to, the following: obsessive–compulsive disorder (OCD); factor analysis; cluster analysis; obsessions; compulsions; symptoms; subtypes; subgroups; contamination fear; compulsive washing/cleaning; checking; pathological doubt; symmetry; ordering; ‘just right’ experiences/perceptions; ‘sensory phenomena’; perfectionism; pure obsessions; sexual/religious/aggressive; insight; age of onset; early onset; schizotypal; Tourette; tics; hoarding; treatment; behaviour therapy; exposure and response/ritual prevention (ERP); cognitive therapy; cognitive behaviour therapy (CBT); pharmacological treatment; serotonin re-uptake inhibitors (SRIs); selective serotonin re-uptake inhibitors (SSRIs); clomipramine; fluoxetine; fluvoxamine; paroxetine; sertraline; citalopram; escitalopram; treatment response/outcome; treatment non-response; predictors of treatment response/outcome. Only journal articles and book chapters reporting original research results were considered.
Results
Psychological treatment
A number of studies have reported an association between OCD symptom subtypes and outcome of ERP and CBT. While certain subtypes (washing/cleaning and checking compulsions) appear to be well represented in these studies, others (hoarding, pure obsessions and symmetry, ordering and arranging) have been underrepresented [21]. Some studies used a categorical conceptualization of the subtypes, based on the division of patients into mutually exclusive groups [7], whereas others conceptualized subtypes dimensionally, so that patients could belong to more than one subtype, depending on their scores on the symptom dimensions [22], [23].
Hoarding was associated with poorer response to ERP [7], [22] and CBT [23], [24]. A lack of compliance with ERP and premature termination of treatment were reported to be common in hoarding patients, contributing to their poor treatment results [22]. In one study, 70% of patients also received pharmacotherapy, but hoarding predicted a poorer response even after medication use has been controlled for [23]. There were 61% of patients who received medications in another study, but the significance of this was downplayed because patients commenced pharmacotherapy at least 3 months prior to beginning ERP and the dose of medications was unchanged throughout ERP [7]. One study reported that only 18% of OCD patients who responded to either CBT or paroxetine exhibited hoarding, compared to 67% of hoarding patients among non-responders [24].
An early meta-analysis demonstrated that patients with a predominance of obsessions and relative absence of overt compulsions (pure obsessions subtype) responded less well to ERP [25]. In one study, patients with ‘unacceptable thoughts’ (a subtype that corresponds to the pure obsessions subtype) responded to ERP as well as patients with other subtypes, although they were relatively close to the poorly responding hoarding patients based on the criterion of a clinically significant improvement [7]. With regards to the type of obsessions, sexual/religious obsessions have been associated with poorer response to both ERP [22], [26] and CBT [23].
Patients with the symmetry, ordering and arranging subtype did not respond to ERP worse than patients with other subtypes [7], [22], [23]. Interestingly, in one study, these patients did quite well based on the criterion of a clinically significant improvement, but their post-treatment mean Y-BOCS score was not significantly lower than that of the poorly responding patients with hoarding [7].
Studies have found that ERP is associated with improvement in compulsions in general [26], [27]. Having a fear of contamination predicted improvement with ERP [27]. Patients with contamination/cleaning subtype and aggressive/harming/checking subtype were significantly more likely than those with hoarding to respond to ERP [7], [22] and CBT [23]. Although checking compulsions predicted a poorer response to ERP in one study [28], other research reported no differences in response to ERP [7], [22], [29] and CBT [23] between patients with washing and checking compulsions. In one study of severe, chronic and treatment-resistant OCD inpatients in which ERP was the main treatment modality, checking compulsions were associated with good outcome [30].
Pharmacological treatment
Some studies have reported association of OCD symptom subtypes and other features of clinical presentation with the outcome of pharmacotherapy, while other studies directly investigated the efficacy of pharmacological treatment for particular subtypes.
With regards to hoarding, the results have been mixed. Three studies identified hoarding as a predictor of poorer response to treatment with SRIs [5], [11], [24], and another reported that only one of 18 patients with hoarding had a ‘marked’ response to SRIs, administered alone or in combination with other medications and CBT [31]. But two other studies found that responders and non-responders to SRIs did not differ significantly in terms of the percentage of patients with hoarding [32], [33]. One open-label study reported no difference between hoarding and non-hoarding OCD patients with regards to their response to paroxetine [34].
Earlier research has found that obsessions in general are either not associated with pharmacotherapy outcome [35], [36] or that they are associated with good response [37]. But an early meta-analysis showed that patients with obsessions who did not exhibit compulsions (pure obsessions) responded less well to clomipramine [25]. When specific types of obsessions were considered, sexual and sexual/religious obsessions predicted poorer response to SRIs in two studies [26], [33], but responders and non-responders to SRIs did not differ significantly in terms of the percentage of patients with sexual and religious obsessions in three studies [5], [32], [38]. In one of these studies, 62% of patients were treated with ERP in addition to medications [26]. Prominent aggressive, sexual and religious obsessions predicted a somewhat better outcome of pharmacotherapy in one study [11]. Somatic obsessions were significantly more frequent among non-responders to SRIs [32], and one small study has indicated that response to a classical monoamine oxidase inhibitor phenelzine may be associated with the presence of somatic obsessions [39].
No association between symmetry, ordering and arranging obsessions and compulsions and outcome of pharmacotherapy has been reported [5], [32], [33], [38], except in one study [11], in which factor analysis grouped patients with symmetry obsessions and compulsions together with those with hoarding, and found them to respond worse to pharmacotherapy. A finding that this OCD subtype was not associated with poorer outcome of pharmacological treatment was speculated to be a consequence of excluding the often co-occurring tic disorders in one study [5], but the presence of tic disorders does not necessarily suggest a poorer response to pharmacological [40] or psychological [41], [42] treatment. Jenike et al. reported that patients with symmetry obsessions were more responsive to phenelzine than to fluoxetine, although phenelzine was generally not effective in the treatment of OCD [39]. But this finding has not been replicated.
The predominance or severity of compulsions was associated with poorer outcome of the SRI treatment [37], [43], [44], as was the presence of ‘miscellaneous compulsions’ [33]. But earlier studies did not find this relationship [35], [36]. In terms of the specific types of compulsions, washing/cleaning predicted a poorer response to SRIs [11], [33], [43], [45], although not in all studies [5], [32]. Checking compulsions were not identified as a specific predictor of outcome of pharmacotherapy [5], [33], [38].
Combined psychological and pharmacological treatment
Although psychological and pharmacological treatments for OCD are commonly combined, there is much inconsistency in the way the use of these components is reported in the literature on symptom subtypes. As a result, it has been difficult to classify combined treatment studies: some relied more on ERP or CBT, for others medications were the primary treatment modality, and only a few studies were clearly labelled as involving combined treatment. Moreover, the impact on different symptom subtypes of various modes of delivery of combined treatment (simultaneous or sequential) has not been studied.
The hoarding OCD patients had a poorer response to a combination of CBT and SRIs than the non-hoarding patients [46]. In another study, patients with the hoarding and symmetry, ordering and arranging subtypes responded less well than patients with other subtypes to a combination of ERP and pharmacotherapy [12]. As noted before, in two studies in which hoarding was associated with poorer outcome of ERP and CBT [7], [23], many patients also received medications. One study did not identify hoarding as a predictor of poor response to either SRIs in combination with ERP or SRIs alone [26].
The presence of sexual/religious obsessions was the unique predictor of a worse long-term outcome of treatment involving either pharmacotherapy in combination with ERP or pharmacotherapy alone [26].
Two studies comparing combined treatment to either pharmacological therapy alone [26] or psychological therapy alone [47] related their results to the clinical presentation of OCD. Patients treated with ERP and SRIs had a significantly greater decrease in the Y-BOCS compulsions subscale scores than patients treated with SRIs alone, while no difference between the two groups was found on the Y-BOCS obsessions subscale scores [26]. The other study reported that obsessions were significantly more improved in the group of patients treated with ‘multi-modal behaviour therapy’ (ERP with some cognitive restructuring) and fluvoxamine than in the group treated with ‘multi-modal behaviour therapy’ alone [47]. In contrast, there were no significant differences between these groups regarding compulsions [17].
Discussion
The results of this review should be interpreted in light of the findings that OCD symptom subtypes represent only one of many factors that influence the outcome of treatment. Therefore, the choice of treatment in OCD cannot be based only on the type of obsessions and compulsions, but should also take into account other factors that have often (although not always) been associated with treatment response. These factors include severity of the OCD symptoms [5], [22], [33], [38], [44], [45], [48–51], age of onset [32], [33], [36], [43], [52], level of insight [32], [33], [51], [53–55], and co-occurrence of schizotypal personality disorder [43], [44], [56–58], chronic tics [59–61] and depression [27], [28], [33], [36], [47], [55], [62–64]. With this in mind, the following text discusses the relevance of OCD symptom subtypes for treatment and considers options for improving treatment outcomes.
Hoarding
The most consistent finding of this review is that OCD patients with hoarding tend to respond poorly to ERP, CBT, SRIs and combinations of these treatments [5], [7], [11], [12], [22–24], [31], [46]. Still, several studies did not report significant differences in treatment response between hoarding and non-hoarding OCD patients [26], [32–34], but no study found hoarding patients to have a superior treatment outcome to patients with other OCD subtypes. Patients with hoarding may fare worse with ERP perhaps because they tend to be less motivated for and less compliant with this treatment [22]. In contrast, they were apparently as compliant with pharmacotherapy as patients with other OCD subtypes [34].
In addition to their lower motivation for psychological treatment, several other reasons may account for the generally poorer treatment response in patients with hoarding. They often have a greater overall severity of OCD [65], [66], which is in itself a predictor of poorer treatment outcome [5], [22], [33], [38], [44], [45], [48–51]. Some studies reported a strong association between hoarding and poor treatment outcome even after controlling for the severity of OCD [5], [23], suggesting that hoarding may adversely affect treatment in other ways. For example, patients with hoarding commonly exhibit poor insight [66–68] and traits of various personality disorders, including schizotypal personality disorder [66], [68]. Poor insight [32], [33], [51], [53–55] and schizotypal personality disorder [43], [44], [56–58] have both been associated with poor treatment outcome in OCD.
In view of their poor compliance with and poor response to standard psychological treatments for OCD, modifications to CBT have been proposed for patients with hoarding [69]. These include incorporation of motivational interviewing, learning skills for better attention focusing, organizing, decision making and problem solving, and longer duration of treatment (26 sessions). The outcome of pharmacotherapy could also be improved, because some studies suggest that poor insight [70] and schizotypal personality disorder [71], [72], which often accompany hoarding, may predict a better response to the antipsychotic augmentation of SRIs. Moreover, a demonstration in animal models that the dopaminergic system may play a key role in hoarding [73] supports addition of antipsychotic drugs in the treatment of hoarding.
Pure obsessions and sexual and religious obsessions
A subtype of OCD characterized by obsessions and absence of overt compulsions (pure obsessions) may be generally associated with a poorer response to ERP and SRIs [25], but other studies indicated that patients with this subtype (or patients with a predominance of obsessions) responded to ERP [7] and pharmacotherapy [35–37] relatively well or at least not worse than patients with other OCD subtypes. There was more consistency with regards to certain specific obsessions, because several studies showed that sexual and religious obsessions responded poorly to ERP [22], [26], CBT [23] and SRIs [26], [33]. But sexual and religious obsessions were not associated with poor response to SRIs in other studies [5], [11], [32], [38].
Why are OCD patients with sexual and religious obsessions apparently difficult to treat with standard psychological and pharmacological interventions? It is widely believed that ERP is primarily effective for overt compulsions (possibly because exposure programmes are more easily designed when these compulsions are present) and less effective in their absence. These patients may also have a greater overall severity of OCD [7], but when the severity of OCD has been controlled for, sexual and religious obsessions still predicted a poorer response to ERP [22]. The nature of these obsessions may largely account for the resistance to ERP, because they are usually associated with beliefs about the importance of the underlying intrusive thoughts [74], [75], catastrophic appraisals of a failure to control these thoughts [74], [75] and/or beliefs that having unacceptable (immoral) thoughts is equivalent to overt unacceptable actions or that some thoughts increase the likelihood of certain frightening events occurring [76]. If such appraisals and beliefs are not addressed in the course of treatment, it may be difficult for the obsessions to abate. Moreover, patients often attempt to neutralize sexual or religious obsessions through strategies (such as reassurance-seeking, avoidance and/or mental compulsions) that they may be unwilling to abandon because of the high danger attributed to their obsessions.
Considering the importance of the specific appraisals of intrusions and neutralization responses in pure obsessions, identifying, challenging and modifying these appraisals in the course of cognitive therapy and extinguishing neutralization responses could be important components of a psychological treatment suitable for this OCD subtype. A CBT protocol for pure obsessions incorporating these procedures has been developed by Rachman [77]. The results of a few studies in which cognitive techniques were combined with a modified ERP in the treatment of pure obsessions are encouraging [78], [79], but more research is needed. Although there is some evidence that ERP combined with an SRI may be more effective than ERP alone in the treatment of obsessions in general [47], it is uncertain whether modified CBT for pure obsessions (especially sexual or religious ones) in combination with SRIs would be more effective than modified CBT alone.
Symmetry, ordering and arranging obsessions and compulsions
Patients with symmetry obsessions and ordering and arranging compulsions tend to seek help less often [80] and to experience their obsessions and compulsions as more ego-syntonic [81]. This may account for their underrepresentation in OCD studies [21], and results of these studies should be interpreted accordingly. Most research suggests that these patients do not fare worse with ERP, CBT or pharmacotherapy than patients with other subtypes of OCD [5], [7], [22], [23], [32], [33], [38], but in one study they responded worse to pharmacotherapy [11], and in another their response to a combined treatment with ERP and medications was poor [12]. In some of the studies in which patients with symmetry, ordering and arranging fared relatively well, certain methodological issues raised some doubt about the validity of this result [5], [7], thereby requiring replication.
The reasons for a relatively unfavourable treatment response in some patients with this symptom subtype can be found in its associations with features that may suggest a poorer prognosis. These include greater overall severity of OCD [12], earlier onset [5], [11], [12], [52], [82], [83], and frequent co-occurrence with Tourette's disorder and chronic tic disorder [5], [84–86]. In addition, the sensory phenomena (‘not-just-right experiences’ and sense of incompleteness) [87–89] that are often associated with the symmetry, ordering and arranging subtype, may call for a different treatment approach, especially with ERP.
A modified psychological treatment was proposed for patients with symmetry, ordering and arranging when compulsions are driven more by a need to ‘get things just right’ or to experience a sense of completeness than by an attempt to neutralize harm [90]. The co-occurring tics can be treated by adding a dopamine antagonist [61], [91] and/or a behavioural technique of habit reversal [92]. Symmetry and ordering obsessions and compulsions, as well as hoarding, predicted a better response to the neurosurgical procedure of cingulotomy [93].
Contamination obsessions and washing/cleaning compulsions
Washing and cleaning compulsions have been associated with a good response to ERP [7], [22] and CBT [23] and poor response to SRIs [11], [33], [43], [45]. There was no relationship between this subtype and outcome of pharmacotherapy in two studies [5], [32]. Contamination fears and obsessions were also associated with good response to ERP [27] and CBT [23]. The ERP has been used in the treatment of patients with washing and cleaning compulsions for a long time, which has allowed development of the strategies for improving compliance and outcome. Patients with this subtype who are able to clearly articulate the feared consequences of contamination and of not performing their compulsions are usually responsive to ERP [54].
The subtype with contamination obsessions and washing/cleaning compulsions may itself be heterogeneous. Two types have been identified [8]. The first is a classic contamination–decontamination type in which contamination obsessions are associated with harm (e.g. becoming ill or spreading an illness), and washing/cleaning compulsions serve the purpose of preventing that harm. This type of OCD is well suited for ERP. The second type is characterized by discomfort about feeling contaminated, with patients engaging in excessive cleaning or washing to reduce the feeling of contamination, and not to prevent any particular contamination-related harm; these patients seem to have strong feelings of disgust [94]. While patients in the second group are likely to benefit from ERP, they may also need to be exposed to the feelings of disgust [95]. A cognitive intervention would aim to reappraise discomfort about contamination.
Patients with contamination fears and washing/cleaning compulsions who are unwilling to embark on ERP or who are resistant to it may improve with danger ideation reduction therapy [96], [97]. This treatment does not involve any component of ERP, but includes a number of cognitive and other procedures that aim to reduce danger-related expectancies about contamination.
The treatment with SRIs does not seem to be particularly useful for patients with a mild form of OCD in which clear-cut contamination obsessions are associated with washing/cleaning compulsions. But SRIs could still be used to treat this OCD subtype. The antipsychotic augmentation of SRIs may be of benefit in the presence of the factors that seem to increase the likelihood of a favourable treatment outcome. These include particularly severe obsessions [98], poor insight [70], and co-occurrence of schizotypal personality disorder [71], [72].
Doubting obsessions and checking compulsions
Little is known about the appropriate treatment strategies for patients with checking compulsions, despite their overrepresentation in treatment studies. This is because checking compulsions are often associated not only with doubting, but with a range of OCD phenomena from other subtypes, so that it is difficult to study checking compulsions in isolation. Still, checking compulsions appear to respond as well to ERP and CBT as washing/cleaning compulsions [7], [22], [23], [29]. Checking compulsions predicted a poorer response to ERP only in one study [28]. With regards to pharmacological treatment, little information is available on checking compulsions apart from a tendency for overt compulsions in general to be associated with poorer response to SRIs [33], [37], [43], [44]. But checking compulsions did not predict a poor outcome of pharmacotherapy [5], [11], [33], [38].
Although ERP has fared relatively well in the treatment of checking compulsions, there is room for improvement. The main drawback of ERP is a requirement that patients tolerate high levels of anxiety and discomfort elicited by this technique; for this reason, approximately 25% of all patients refuse ERP [99], 20% drop out [100], and 25% fail to adhere to it [101]. Also, 50–60% of OCD patients in general show a clinically significant change after ERP and only 25% are asymptomatic [102]. Besides modifications and refinement of ERP, improvements in the psychological treatment of checking compulsions may occur through a greater use of the cognitive therapy strategies, which would target the associated cognitive abnormalities. These include inflated responsibility for potentially catastrophic outcomes [103], exaggerated appraisal of harm [104], intolerance of uncertainty [105], and memory distrust [106].
Checking compulsions may be treated with medications, although it is uncertain to what extent they contribute to treatment outcome. As with washing compulsions, the nature and severity of the associated obsessions, level of insight and co-occurrence of schizotypal personality disorder may provide some guidance regarding pharmacotherapy.
Summary
The results of this review do not suggest a precise match between OCD symptom subtypes and specific treatments. Treatment decisions will probably continue to be made on the basis of the criteria such as motivation to undergo ERP or CBT, severity of OCD, presence of co-occurring conditions (e.g. depression or chronic tics), and patient preferences. The clinical presentation can still aid in making some treatment recommendations, which renders OCD symptom subtypes relevant for treatment.
If overt compulsions, especially washing and checking, predominate in the clinical presentation, ERP is a reasonable, evidence-based choice of treatment. In the presence of pure obsessions, ERP can still be administered, but cognitive strategies and/or SRIs may need to be added to enhance treatment response. Those compulsions that seem less likely to respond to ERP – hoarding, in particular, and ordering and arranging to a lesser extent – may need a modified psychotherapeutic approach, which would entail addition of cognitive techniques. But a decision to use cognitive techniques may not necessarily be based on the symptom subtype, but on the presence of the underlying cognitive mechanisms and abnormalities, which cut across various symptom subtypes (e.g. beliefs that intrusive thoughts are important and that they have to be controlled, inflated responsibility for potentially catastrophic outcomes, intolerance of uncertainty, perfectionist tendencies).
The benefit of adding cognitive therapy to ERP or of using cognitive therapy alone in the treatment of OCD symptom subtypes has been controversial. First, ERP is adaptable to various manifestations of OCD [107], which probably accounts for its efficacy across various symptom subtypes. Second, some research suggests that ERP may be just as effective as cognitive therapy alone in changing OCD-related cognitions [42], raising a question about a need to add cognitive techniques to ERP. Third, findings that changes in compulsions predict all treatment effects better than changes in obsessions and that decreasing compulsions is the process through which both ERP and cognitive therapy lead to improvement [108], suggest that the primary aim in the treatment of OCD should perhaps be a decrease in compulsions, regardless of the symptom subtype. As already noted, most research indicates that ERP is well suited for this task.
The debate about the mechanisms of change occurring in the course of exposure-based therapy continues, and there has been an upsurge of views suggesting cognitive mediation as the main mechanism. For example, Hofmann has recently proposed that exposure treatment represents a form of cognitive intervention that specifically decreases the expectancy of harm [109]. If so, perhaps a strict dichotomy between cognitive and behavioural therapies might be artificial.
Beyond a general suggestion that medications may be more effective for treating obsessions than compulsions, OCD symptom subtypes appear less useful in guiding pharmacological treatment. Therefore, OCD patients for whom pharmacotherapy is considered are likely to receive SRIs regardless of the symptom subtype. A decision to augment SRI therapy with antipsychotics may be based on features that seem to increase the likelihood of response, such as severity of the obsessions [98], poor insight [70], co-occurrence of schizotypal personality traits or disorder [71], [72], and presence of tics [61], [71]. While some of these features are more commonly encountered in the hoarding and symmetry, ordering and arranging subtypes, they are by no means subtype specific.
Table 1 summarizes treatment options for various OCD symptom subtypes beyond the use of ERP and/or SRIs as first-line treatments.
Treatment options for OCD symptom subtypes beyond the use of ERP and/or SRIs
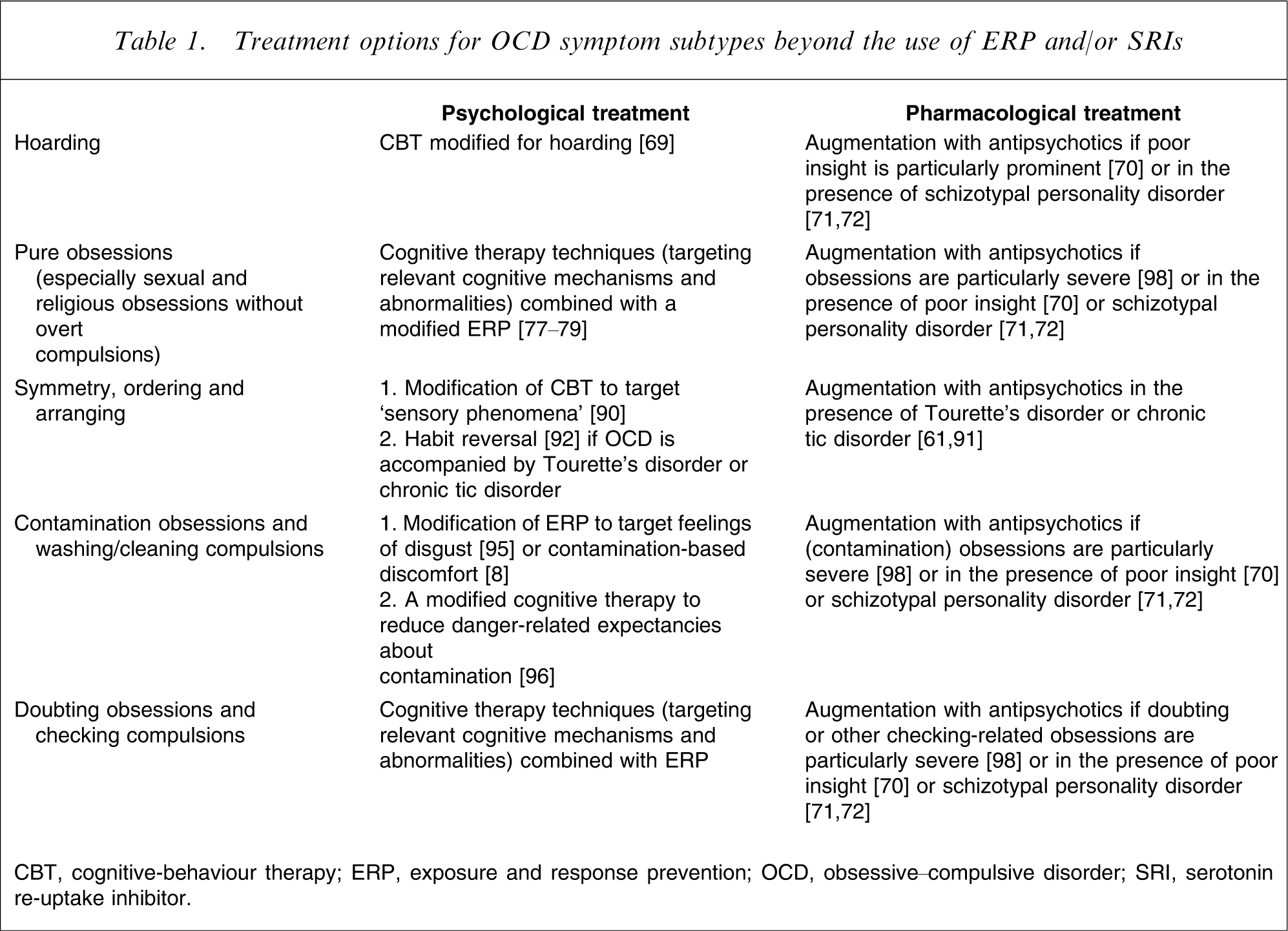
CBT, cognitive-behaviour therapy; ERP, exposure and response prevention; OCD, obsessive–compulsive disorder; SRI, serotonin re-uptake inhibitor.
Larger samples of patients with each OCD symptom subtype are necessary for future research, to make sure that each subtype is adequately represented and to examine associations between various subtypes. It would be important to conceptualize the subtypes both dimensionally and categorically. Future studies would benefit from taking into account factors (e.g. levels of insight and disgust, presence of schizotypal personality disorder and chronic tics, specific underlying cognitions) that may mediate relationships between specific symptom subtypes and specific treatment outcomes. There is clearly a need to establish the role of cognitive therapy techniques in the treatment of OCD symptom subtypes. Considering the extent of overlap in the underlying cognitions between various OCD symptom subtypes, cognitive techniques may be used more to target specific cognitions than specific symptom subtypes. It would also be important to elucidate whether cognitive therapy and ERP operate through different or similar mechanisms. Pharmacological treatment could be improved by investigating whether certain OCD symptom subtypes tend to be associated with the relatively specific neurobiological abnormalities. For example, a demonstration of the prominent dopamine system abnormalities in some subtypes – as it was preliminarily suggested for hoarding [73] – would make the case for augmentation with antipsychotic drugs in these subtypes more convincing.
Footnotes
Acknowledgements
This article originated from a project funded by the Nepean Medical Research Foundation.