
Abstract
Obsessive–compulsive disorder (OCD) is a heterogeneous condition and its symptoms and behaviours vary a lot from one person to another. The heterogeneity of OCD also manifests itself through the variety of functions served by different compulsions, although the dominant view has been that the key function of compulsions is to alleviate anxiety or distress caused by the obsessions. Compulsions may also have other functions, but it is unclear to what extent some of these are only about decreasing anxiety or distress. Furthermore, different ‘types’ of distress that underlie compulsions may actually represent different phenomena.
For example, distress about ‘not having things right’ appears to differ from distress about feeling disgusted. The former distress has been related to ‘sensory phenomena’ (‘not-just-right experiences’ and sense of incompleteness [1–4]) and to a need to ‘get things just right’ or to experience a sense of completeness [5,6], which is often an underlying reason for performing ordering, arranging, repeating, and counting compulsions. Disgust-related distress characterizes people who wash compulsively to reduce the feeling of contamination [7]. Likewise, patients with sexual, religious, or aggressive obsessions may believe that a failure to control these obsessions would lead to catastrophic consequences [8,9] or that having such obsessions is equivalent to overt unacceptable actions and that some obsessions increase the likelihood of certain frightening events occurring [10]. Compulsions performed in response to these obsessions (e.g. checking) may serve the purpose of neutralizing specific belief-related distress and thereby ‘undoing’ the obsessions and preventing harm. Hoarding compulsions may have functions that are quite different from ‘simple’ distress reduction. Thus, it has been observed that hoarders are emotionally attached to possessions [11–13] and have a distorted judgement about the need for possessions in the future, in addition to being indecisive and overly concerned over making a mistake about their possessions [11] and maintaining control over possessions [12,13]. These characteristics may account for hoarding behaviour.
Possibly as a result of the influence of the broad distress-reduction model of compulsions, more specific functions that compulsions may serve in OCD have been relatively neglected by research. This is despite recognition that the function of compulsions in OCD is their phenomenologically important aspect [14]. Only recently has there been some interest in the ‘motivational dimensions’ of OCD, which, however, refer only to incompleteness and harm avoidance [4].
The main aim of this study was to ascertain what motivates individuals with OCD to perform compulsions. In accordance with some of the aforementioned research, we hypothesized that the functions of compulsions are largely related to the type of compulsions. That is, we hypothesized that a frequent reason for ordering, arranging, repeating, and counting compulsions was distress about ‘not having things right’; that disgust-related distress was a common reason for performing washing compulsions; that belief-related distress (with the person believing that catastrophic consequences are likely to follow if the compulsion is not performed) was characteristic of checking compulsions; and that hoarding was often performed for reasons relating to the person's appraisal of the objects of hoarding. We also hypothesized that compulsions were often performed automatically, for no particular reason and without resistance, although at other times the same compulsions could be performed for reasons that were clear to the person. Finally, based on our clinical experience, we hypothesized that the majority of compulsions were performed for more than one reason.
A better understanding of the functions of compulsions is likely to improve our understanding of the phenomenology of OCD, that is, of the links between obsessions and compulsions. This may help clarify the heterogeneity of OCD [15]. A better understanding of the functions of compulsions might also have important treatment implications in that treatments might be tailored to particular compulsions in accordance with their function. This would be especially important in those cases of OCD in which compulsions are performed for two or more reasons, as targeting one reason in the course of treatment may not be sufficient.
Materials and methods
The study was conducted in Sydney, Australia. Participants over the age of 18 were recruited for the Nepean OCD Study through the Nepean Anxiety Disorders Clinic, OCD support groups, newspaper advertisements, and referrals from general practitioners, psychiatrists, clinical psychologists, and mental health services. The key inclusion criterion was a principal diagnosis of OCD established by the clinician on the basis of a semi-structured interview. To qualify as a principal diagnosis, OCD had to be a condition for which help was sought or which caused the most distress or impairment in functioning. Therefore, individuals with co-occurring psychosis, bipolar disorder, and other conditions that were judged to be more severe or disabling than their OCD were not considered eligible to participate. Approval for the study was received from the local ethics committee and all participants provided informed signed consent prior to commencing the study.
Assessment instruments
Participants underwent a comprehensive assessment, which included the administration of the Mini International Neuropsychiatric Interview (MINI) [16], the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) [17], the Functions of Compulsions Interview, and several self-report instruments. For the purpose of this article, only results obtained from the Y-BOCS and the Functions of the Compulsions Interview are reported.
The MINI was used to establish OCD as the principal diagnosis and determine the presence of co-occurring disorders based on the DSM-IV criteria. It is a semi-structured diagnostic interview which has been validated against other widely used structured diagnostic interviews and has been found to have good psychometric properties [18–20]. For example, the concordance (kappa value) between the MINI and the Structured Clinical Interview for DSM-III-R, Patient Version, was 0.63 for OCD [19]. A test–retest reliability of 0.85 was reported for MINI-based diagnosis of OCD [20].
The Y-BOCS is a semi-structured interview used to measure the severity of obsessions and compulsions in individuals already diagnosed with OCD. It consists of a comprehensive checklist of obsessions and compulsions and a 10-item severity scale. On the severity scale, up to three most prominent obsessions and compulsions are rated in terms of time spent, interference with functioning, distress, efforts to resist, and perceived degree of control. Each response is rated on a 5-point Likert scale, and ratings are summed to generate a total Y-BOCS score as an index of the severity of OCD. The Y-BOCS is a widely used instrument, usually considered to be the ‘gold-standard’ assessment tool for OCD. Numerous studies have demonstrated its excellent psychometric properties [21–25].
The Functions of Compulsions Interview is a brief instrument designed specifically for the Nepean OCD Study. Its aim is to assess the functions of compulsions and it was administered alongside the Y-BOCS. Participants were interviewed about their most important compulsions, up to a maximum of three, to parallel the identification and rating of three most prominent obsessions and compulsions in the Y-BOCS. The importance of compulsions was determined by the participants and it was generally based on distress and interference with functioning associated with them. Participants were asked about their current (past month) reasons for performing each compulsion. The reasons for any given compulsion could be present simultaneously or at different times (even if only occasionally), as long as they occurred within the past month. Participants could choose from the following reasons listed in the Functions of Compulsions Interview: i) To decrease distress or anxiety associated with the obsession, ii) Because you feel/believe something bad/unpleasant would happen if you didn't do it, iii) Because you want to get rid of, ‘cleanse’ yourself of, or ‘undo’ the obsession, iv) To correct things, so that they look ‘just right’ or perfect, v) Because you felt disgusted as a result of the obsession, vi) It happens automatically, without your thinking why you do it, and vii) For some other reason (state which). Participants could endorse as many of these reasons for performing each compulsion as they thought were applicable to them.
Procedure
Participants were interviewed by a psychiatrist or clinical psychologist who had been trained in the use of the MINI, Y-BOCS, and Functions of Compulsions Interview. To ensure the integrity of the MINI-derived DSM-IV diagnoses of OCD, we obtained inter-rater reliability estimates based on 46 of the interviews. Raters were in agreement in 97.8% of cases (45 of the 46 interviews).
The identified main compulsions were classified into several groups: i) checking, ii) washing/cleaning, iii) mental compulsions, including counting, iv) ordering/symmetry/repeating, v) hoarding, and vi) miscellaneous compulsions, including compulsions about having to tell/ask/confess and touching/tapping.
Data analysis
All analyses were conducted in SPSS 17.0. Numbers and percentages for each of the demographic variables as well as for the compulsions and functions of compulsions were calculated. To determine whether the number of functions of compulsions was associated with the severity of OCD, Pearson's correlations were calculated between the total number of different functions of compulsions reported by participants across the three main Y-BOCS compulsions and their total Y-BOCS score.
We conducted a series of two (presence or absence of a given function of compulsion in any of the three main compulsions) times three (number of compulsions reported, ranging from one to three) factorial analyses of variance (ANOVAs) to determine whether the presence of each respective function of compulsion was associated with higher Y-BOCS total scores, averaged across the number of compulsions reported. We adopted this procedure because any function of compulsions would be more likely to be endorsed if the participant had a greater number of compulsions.
The possibility that any participant could endorse multiple compulsions and multiple functions for each compulsion precluded us from performing additional statistical tests that required an independence of observations.
Results
The study sample consisted of 108 participants with OCD, of whom 65 (60.2%) were women. Their mean age was 44 years (SD = 16.1). Forty-one (38%) participants were in a marital/de facto relationship and also 41 (38%) were never married; 39 (36.1%) participants were engaged in full-time or part-time paid employment and 28 (25.9%) were unable to work due to illness-related disability. There were 46 (42.6%) participants with post-high school qualifications.
Taking into consideration that participants were limited to reporting no more than three main compulsions, a total of 218 compulsions were reported by 108 participants. Therefore, the mean number of compulsions per participant was 2.02; 31 (28.7%) participants had only one compulsion, 44 (40.7%) reported two compulsions, and 33 (30.6%) had three compulsions. Table 1 shows the frequency of the main types of compulsions in the study sample.
Frequency of the main compulsions
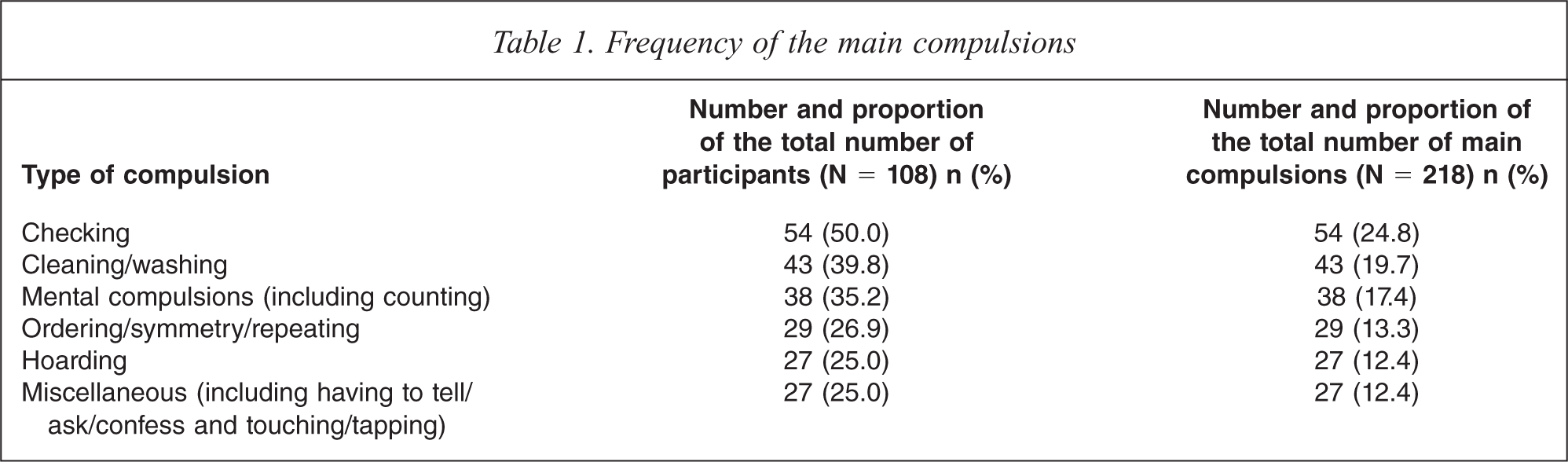
Table 2 shows the numbers and proportions of all participants who endorsed specific functions of compulsions for one or more of their compulsions. A high proportion performed one or more of their compulsions automatically (84.3%) or to decrease distress or anxiety (74.1%). In contrast, only 20.4% performed one or more of their compulsions to alleviate the feeling of disgust. Table 2 also summarizes the results of the 2 × 3 factorial ANOVA. They indicate that participants who performed one or more of their compulsions to decrease anxiety or distress, get rid of or ‘undo’ the obsessions, or alleviate the feeling of disgust, had significantly higher mean total Y-BOCS scores than those who did not, averaged across the number of compulsions (i.e. there was a significant main effect of the respective function of compulsions on total Y-BOCS score). The total number of different functions of compulsions endorsed for the three main compulsions was correlated with Y-BOCS total scores (r = 0.37, p < 0.001).
Number and proportion of the total number of participants (N = 108) who did and did not endorse specific functions of compulsions for one or more of their compulsions and their mean total Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores
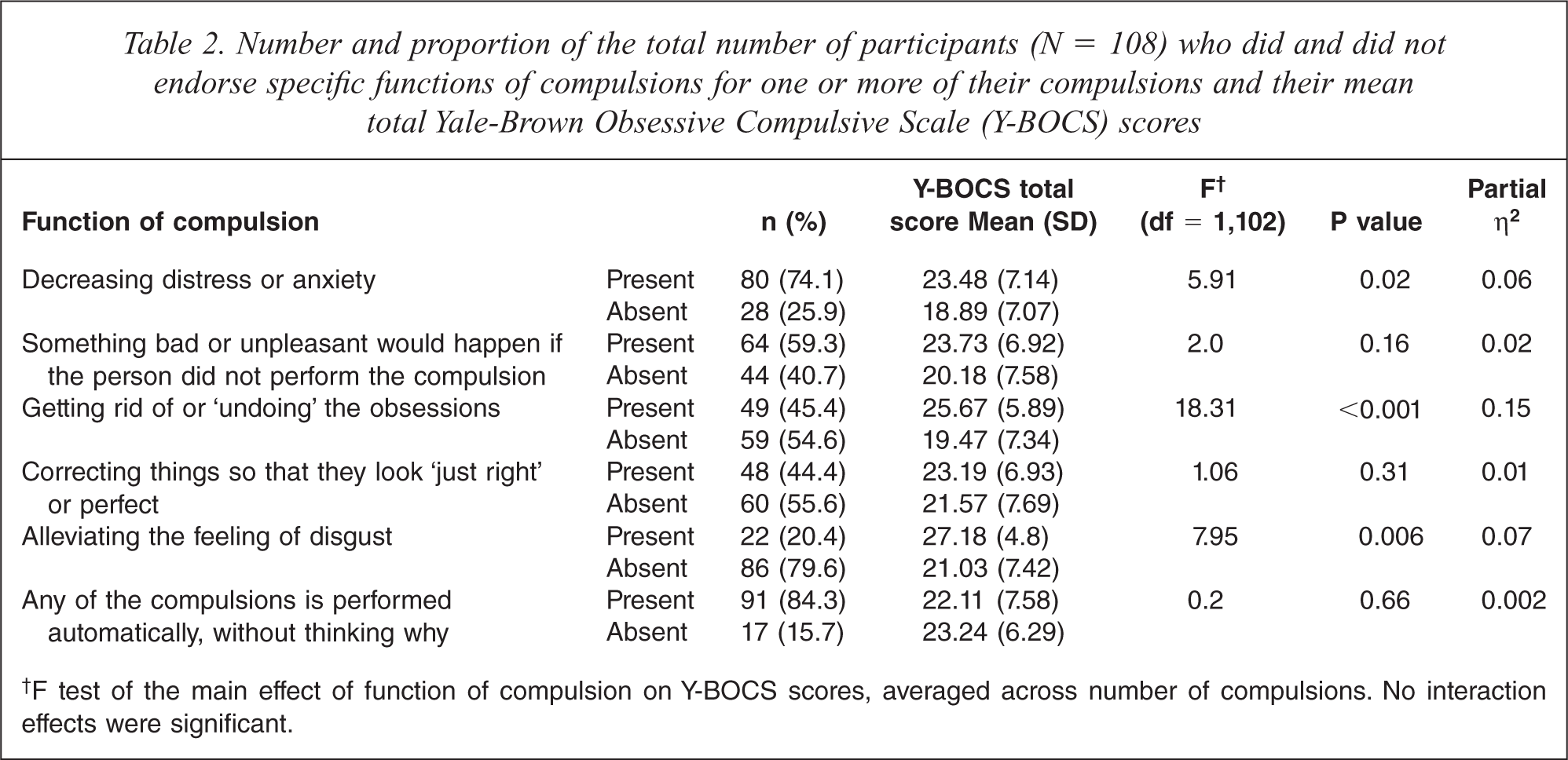
†F test of the main effect of function of compulsion on Y-BOCS scores, averaged across number of compulsions. No interaction effects were significant.
The vast majority of compulsions (85.3%) were performed for more than one reason. To investigate the interrelatedness of the various functions of compulsions we calculated the frequencies with which they co-occurred with one another, and Table 3 presents these results. The functions of decreasing distress or anxiety, something bad or unpleasant would happen if the compulsion was not performed and getting rid of or ‘undoing’ the obsessions, as well as performing compulsions automatically, co-occurred with each other frequently (in at least 50% of the cases). The only exception to this pattern was a lower percentage among the participants who performed compulsions automatically and who also endorsed the function of getting rid of or ‘undoing’ the obsessions. Participants who performed compulsions to correct things so that they look ‘just right’ or perfect also frequently performed compulsions automatically and to decrease distress or anxiety, whereas those who performed compulsions to alleviate the feeling of disgust also frequently performed them to decrease distress or anxiety, get rid of or ‘undo’ the obsessions, because something bad or unpleasant would happen if the compulsion was not performed, and automatically.
Frequencies with which various functions of compulsions occurred with one another in compulsions that were performed for more than one reason (N = 186)
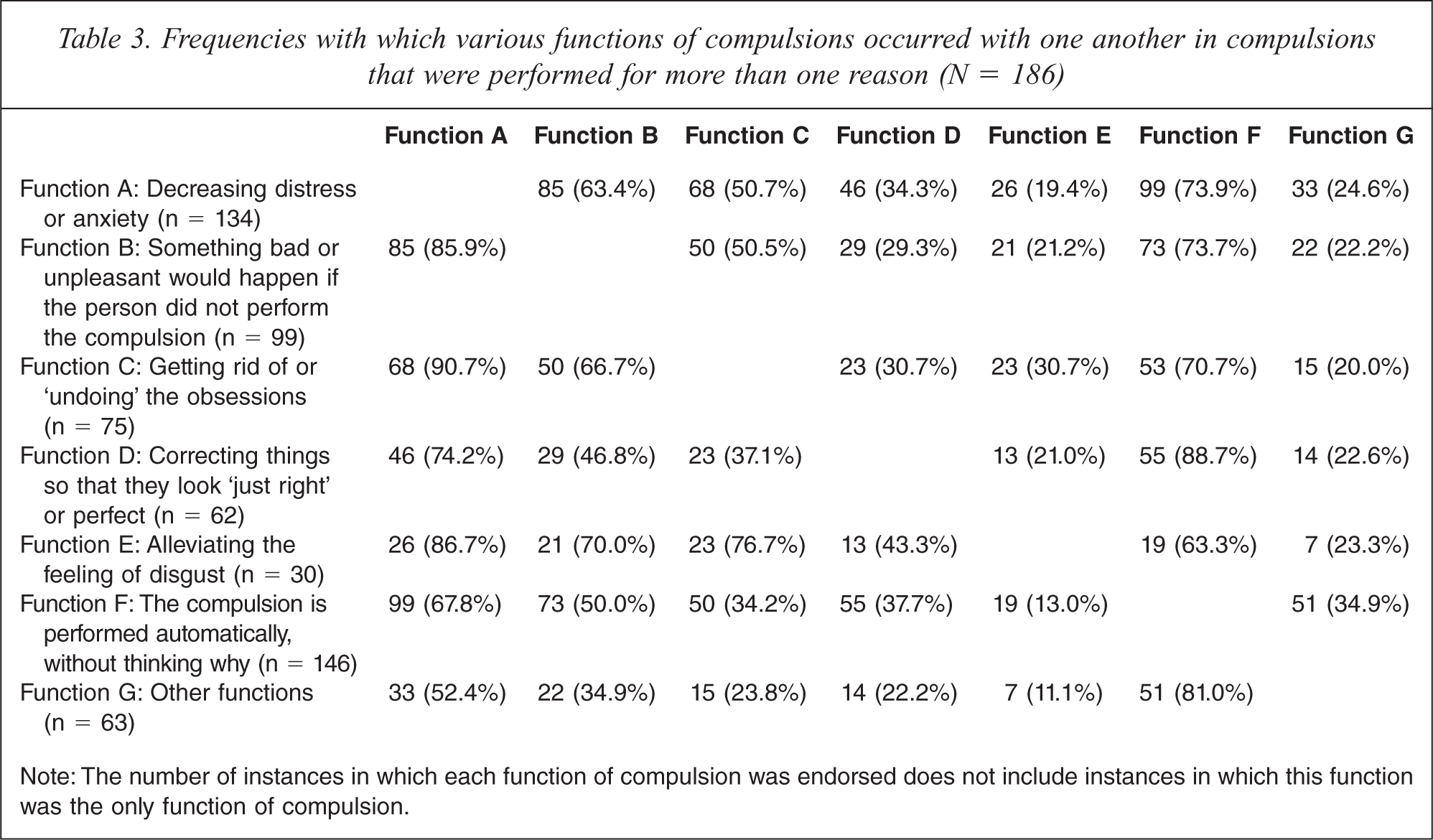
Note: The number of instances in which each function of compulsion was endorsed does not include instances in which this function was the only function of compulsion.
Table 4 shows the functions of compulsions in participants with various compulsions. The mean number of functions per compulsion in the whole sample was 2.94, and hoarding tended to be performed for fewer reasons than other types of compulsions (Table 4). Across all the compulsions, the majority were performed automatically (71.6%) and/or to decrease distress or anxiety associated with the obsession (62.4%). For almost one half of the compulsions, the reason for performing them was that something bad or unpleasant would happen if the person did not perform them.
Functions of compulsions in various types of compulsions
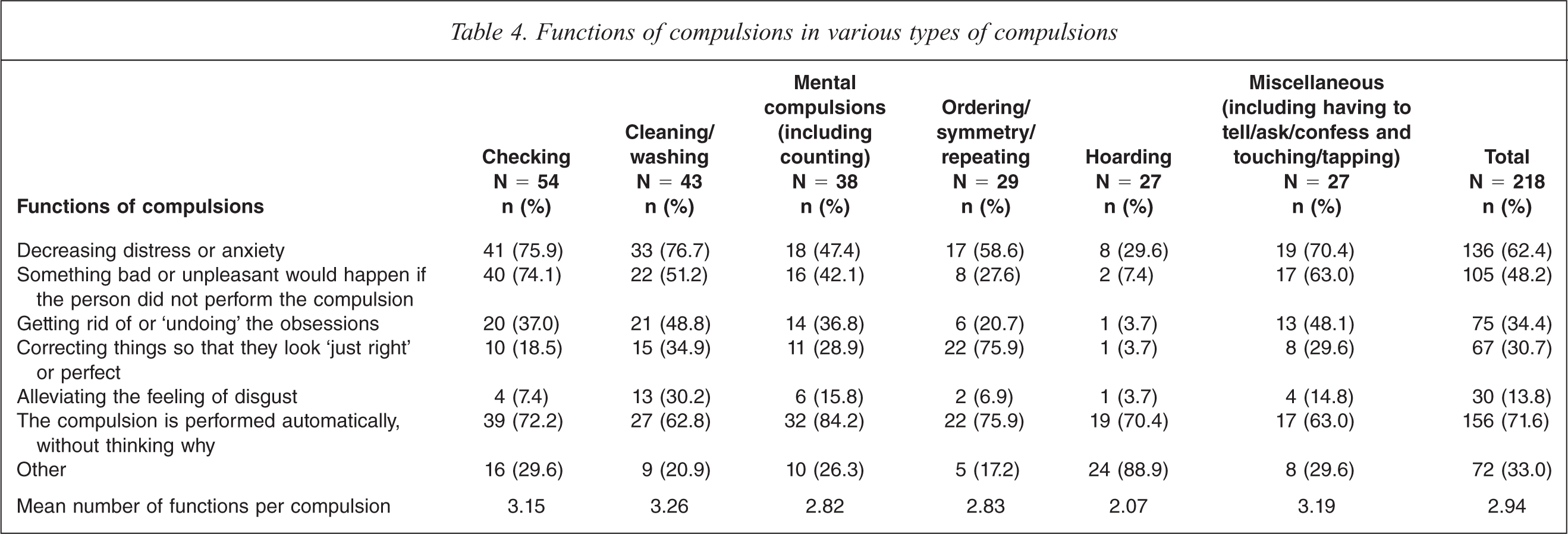
The reasons for performing compulsions varied substantially, depending on the type of compulsion (Table 4). The pattern was most strikingly different for hoarding, as in less than one third this compulsion was performed to decrease distress or anxiety. In contrast, hoarding was performed much more frequently (88.9%) for other reasons. These included a possible need for the collected objects in the future (44.4%), attachment to the collected objects (37.0%), and meeting the need for safety or security provided by the collected objects (7.4%).
Table 4 also shows that the ordering, symmetry and repeating compulsions were most frequently performed to achieve a ‘just right’ feeling (75.9%) or automatically (75.9%), whereas checking was most frequently performed to decrease distress or anxiety (75.9%), because of the belief that something bad or unpleasant would happen if the participants failed to check (74.1%), and automatically (72.2%). Cleaning/washing compulsions were most frequently performed to decrease distress or anxiety (76.7%) and automatically (62.8%). Alleviating the obsession-related feeling of disgust as the reason for performing compulsions was most frequently encountered in cleaning/washing compulsions (30.2%). Mental compulsions were performed automatically far more often (84.2%) than for other reasons.
Discussion
The main aim of this study was to investigate the functions of compulsions in OCD. In agreement with our hypothesis, we found that the majority of compulsions were performed for more than one reason, that is, that they had more than one function. A similar suggestion was made by Pietrefesa and Coles [6], who found that a sense of incompleteness, in addition to harm avoidance, was an underlying motivation for performing washing/cleaning, checking, and mental compulsions. Ecker and Gönner [4] reported ‘motivational heterogeneity’ only for checking, in that this compulsion was associated with both incompleteness and harm avoidance. We also found that people with OCD who endorsed a greater number of different functions of compulsions were more likely to have a more severe OCD. This suggests that individuals with a severe OCD may perform compulsions for several reasons, which may need to be addressed in the course of treatment.
Our results provide support for a more nuanced approach where avoiding catastrophic outcomes, alleviating the feeling of disgust, achieving a ‘just right’ feeling, etc., are considered as separate functions from decreasing distress or anxiety. In view of the high frequency with which they co-occur, there may be a conceptual overlap between some functions of compulsions, for example between the function categories of ‘decreasing distress or anxiety’ and ‘something bad or unpleasant would happen if the person did not perform the compulsion’ (Table 3). However, performing compulsions to decrease distress or anxiety was significantly associated with greater severity of OCD, whereas performing compulsions because something bad would happen in case of a failure to perform compulsion was not (Table 2), supporting the notion that these functions are distinct.
We also hypothesized that the functions of compulsions might be different in different types of compulsions, and to a large extent this hypothesis was also supported by our results. Thus, ordering, symmetry and repeating compulsions were often performed to achieve a ‘just right’ feeling, checking was commonly performed because of the belief that something bad or unpleasant would happen in the absence of checking, and the frequent reason for hoarding pertained to the perceived need for the collected possessions (e.g. a need for these objects in the future and attachment to the possessions). Contrary to our hypothesis, disgust-related distress was not a very common reason for performing cleaning and washing compulsions. Still, alleviating the obsession-related feeling of disgust was a more frequent reason for performing these compulsions than it was for performing any other type of compulsion.
In accordance with our hypothesis, compulsions were very often performed automatically, although at other times the same compulsions were performed for the more specific reasons. This was a pattern that we found across all types of compulsions, but it was especially striking for mental compulsions.
Our results have implications for current debates about the potential symptom subtypes of OCD. This is particularly pertinent to hoarding, as it had a function profile distinct from all other compulsions. As already noted, the reason for hoarding often involved the appraisal of the need for collected objects, which is in agreement with previous research findings about the value of possessions among the hoarders [11–13]. Moreover, unlike other compulsions, hoarding was performed relatively infrequently to decrease distress or anxiety. These findings support a notion that hoarding may be different from OCD to the extent that justifies its conceptualization as a distinct condition [26,27].
Achieving a ‘just right’ feeling (and possibly a sense of completeness) was a prominent function of the ordering, symmetry and repeating compulsions, but was less common in other compulsions. This finding, in agreement with previous research [1–6], provides some support to the idea that ordering/symmetry/repeating compulsions may constitute a distinct symptom subtype or symptom dimension of OCD [28,29].
Our findings may also have implications for treatment of OCD insofar as compulsions performed for different reasons may call for different cognitive-behavioural therapy (CBT) approaches [4,6]. It has been speculated that exposure and response prevention may achieve better results when compulsions are driven by a need to decrease distress or anxiety, whereas addition of cognitive techniques may be useful when compulsions are linked to certain beliefs, e.g. about some catastrophes occurring in case of a failure to perform compulsions [30]. When compulsions are performed to achieve a ‘just right’ feeling, as in ordering, symmetry and repeating compulsions, they may be somewhat less responsive to the standard CBT techniques for OCD [30–33], and a modified psychological treatment has been proposed for patients with this clinical presentation [5]. Perhaps pharmacotherapy might also be useful in such cases [34–36]. Compulsions that are performed to alleviate the feeling of disgust may require a modified treatment approach, considering that habituation to disgust stimuli in the course of exposure may occur more slowly and to a lesser degree [37].
When several functions are identified for one compulsion, targeting only one function in the course of CBT may not be sufficient, and may even help explain treatment resistance in such cases. For example, our results indicate that checking compulsions are frequently performed both to decrease distress or anxiety and because of the belief that a failure to check would lead to some catastrophic outcomes; if an OCD patient performs checking rituals for both of these reasons, it may be useful to combine exposure and response prevention with cognitive restructuring targeting relevant beliefs. Of course, it needs to be tested whether such treatment approach to patients with these particular functions of checking compulsions produces better results than either of these techniques used alone.
Treatment implications of performing compulsions automatically are unclear and deserve further study. On one hand, it may seem difficult to link compulsions to the corresponding obsessions in these situations; this might interfere with CBT-based treatment and perhaps portend a poorer prognosis, because such treatment largely relies on the understanding of the functional link between obsessions and compulsions. On the other hand, our results show that people with OCD who stated that they performed one or more of their compulsions automatically actually had their mean total Y-BOCS score slightly lower (when controlling for effects of other functions of compulsions) than those who did not perform one or more of their compulsions automatically, suggesting a lack of the relationship between performing compulsions automatically and the severity of OCD.
Aside from the issue of the distinctness of functions of compulsions, the results of this study should be viewed in light of its strengths and limitations. We did not ‘force’ the categorization of one dominant compulsion per participant and one dominant function per compulsion, because it would not have reflected the reality of many people with OCD exhibiting more than one compulsive behaviour and having more than one motivation for performing compulsions. This, however, precluded us from creating mutually exclusive, non-overlapping categories of compulsions and functions of compulsions, and performing the relevant comparisons. Another limitation is the fact that the psychometric properties of the Functions of Compulsions Interview are yet to be established.
Conclusion
This study contributes to the literature on OCD first by showing that the majority of compulsions have more than one function and that they are often performed automatically. Secondly, functions of compulsions differed somewhat in different types of compulsions, providing some support to the symptom-based subtyping of OCD. Identifying functions of compulsions allows better understanding of the functional relationship between obsessions and compulsions. This may have implications for CBT in that targeting various functions in the course of treatment may lead to better outcomes.
Footnotes
Acknowledgements
The authors are grateful to Colin Slocombe, Michelle Graeber, Dr Scott Blair-West, the Blacktown OCD Support Group, Julie Leitch of the Kogarah OCD Support Group, Linda Junee of the Mental Health Association of New South Wales, the Penrith Mental Health Practitioners Network, and all mental health staff, psychologists, psychiatrists and general practitioners who referred patients to the study.