
Abstract
Violence accounts for approximately 14% of deaths among men and 7% among women [1]. For every person killed by violence an estimated 20 to 40 receive injuries needing hospitalization [1]. Between 1996 and 2006 violent crimes rose by 30% in Australia [2]. Considerable numbers of those in the criminal justice system have committed violent offences. Approximately one third of prisoners in New South Wales (NSW) were sentenced for assault (excluding sexual assault) or robbery, with around 50% of violent offenders returning to prison within two years of release [3–5].
The link between impulsivity and offending behaviour is well established in the criminological literature [6–8]. Heilbrun found that violent crimes such as manslaughter, murder, assault, and rape were more likely to be classified as impulsive than offences such as arson or forgery [9]. In a study of men on parole assessed for impulsivity, violent offenders made a significantly higher proportion of impulsive choices than non-violent offenders and exhibited higher self-reported impulsivity scores [10]. Heilbrun found that those who committed ‘impulsive’ homicides had a higher recidivism rate (62%) compared with pre-meditated murderers (45%), and a Finnish study showed that released offenders who committed ‘impulsive’ crimes were more prone to recidivism than the ‘non-impulsive’ group [9,11].
Animal research, human studies, pharmacological evidence, brain imaging, and receptor sub-typing have all demonstrated a relationship between aggression and impulsivity and serotonergic dysfunction [12]. Reduced levels of cerebrospinal fluid concentrations of 5-hydroxyindoleactic acid (5-HIAA), a metabolite of serotonin, have been correlated with measures of aggression and impulsivity in free ranging monkeys [13], young men with personality disorders [14], psychiatric patients [15], and violent offenders [16]. Lower 5-HIAA was found among impulsive recidivists who had committed violent offences or arson compared with matched non-recidivists [16].
The link between serotonergic dysfunction and impulsive aggression has prompted researchers to speculate that: ‘an inverse relationship between central serotonergic system function and impulsive aggressive behaviour has been accumulating for several decades. This suggests that a pharmacological enhancement of serotonin activity should be expected to reduce impulsive aggressive behaviour’ [17], and ‘The serotonergic hypothesis of aggression opens possibilities for anti-aggressive pharmacological treatments’ [18]. This has prompted the use of selective serotonin re-uptake inhibitors (SSRIs) to treat individuals with heightened aggression and impulsivity. Coccaro and Kavoussi [17] showed that fluoxetine resulted in sustained reductions in irritability and aggression in those with histories of impulsive aggression and, more recently (2009) among psychiatric outpatients with intermittent-explosive disorder [19]. Citalopram was used successfully to reduce irritability and anger in a sample of war veterans who scored highly on an aggression screener [20]. Among patients with mild traumatic brain injury and depression, sertraline was associated with improvements in depression, anger and aggression [21]. Similarly, Cherek et al. [22] and New et al. [23] demonstrated that SSRIs reduce impulsive aggression in community-based samples of impulsive violent patients; the former study was conducted in ex-offenders.
The aims of the feasibility study were: (i) establish whether individuals with a history of impulsivity and violence would be willing to undertake a trial of sertraline with the intent of reducing their impulsivity; (ii) whether those who agreed to participate in the study would comply for a duration of 3 months; and (iii) whether there were changes in behavioural measures of impulsivity, aggression, anger, irritability, and depression.
We present the findings from an open label feasibility study using an SSRI (sertraline) in a sample of repeat violent offenders in New South Wales.
Methods
Setting
Between December 2007 and February 2009 32 men were recruited at three NSW local magistrates court complexes (Burwood, Liverpool, and Blacktown) located in the Sydney metropolitan area.
Participants
Participants were recruited either by word-of-mouth or a flyer distributed within the court complex by the research nurse (L.K.) who was employed by the Justice Health NSW's Statewide Community and Court Liaison Service (SCCLS). The SCCLS diverts those suffering from a mental illness away from the criminal justice system and into treatment. Recruitment occurred only on Fridays due to budgetary limitations.
Potential participants were provided with an explanation of the study, the requirements of the trial, and the selection criteria. Eligibility criteria included men over 18 years, a score of over 70 on the Barratt Impulsivity Scale (BIS-11) [24], and at least one prior conviction for a violent offence. Exclusion criteria included: major medical illness (e.g. hepatic or renal impairment), current use of any serotonergic (e.g. SSRI, Serotonin-norepinephrine reuptake inhibitors (SRNI), Tricyclic anti-depressant (TCA) anti-psychotic, or Attention-deficit hyperactivity disorder (ADHD) medication, a history of adverse drug reactions to SSRIs, severe mental illness (e.g. schizophrenia, bipolar disorder, current major depression), inability to provide written consent, current self-reported use of amphetamine, current self-reported use of hallucinogens, conviction for murder or sexual assault, and likely to move to an area with no prospect of follow up (e.g. overseas, interstate, remote setting). The recruitment flow chart for the study is shown in Figure 1.
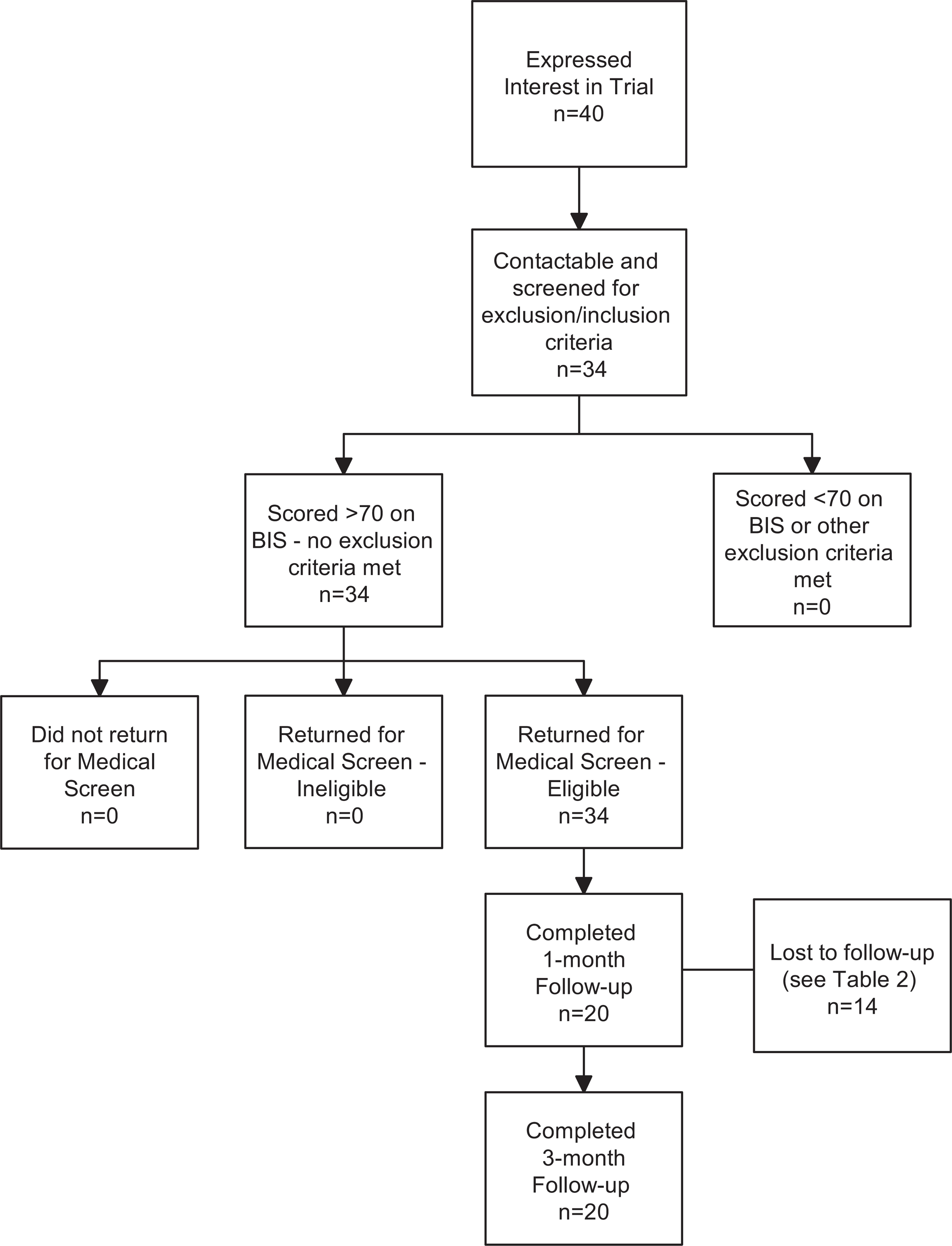
Flow chart of sample recruitment.
Screening measures
The BIS-11 was administered at the initial contact between the participant and the research nurse. Those who scored over 70 on the BIS-11 who satisfied the inclusion criteria, and those who did not meet any of the exclusion criteria were recalled for a medical assessment.
Following a satisfactory medical examination conducted by one of the project psychiatrists (A.E., D.G.), the following baseline measures were administered: the Beck Depression Inventory (BDI) [25], the Kessler Psychological Distress Scale-10 (K-10) [26], the Short Form-12 (SF-12) [27], and the Anger Irritability and Assault Questionnaire (AIAQ) [28]. The AIAQ provides several timeframe options (past week, past month, childhood, adolescence, and adulthood). We used the past two weeks as our reference period. Demographic and criminographic information was also recorded at baseline.
Participants were briefed about possible side-effects from the medication and were provided with a contact telephone number for the research nurse whom they were encouraged to contact should they experience new symptoms or have other concerns. Those taking part in the trial received $50 per assessment to cover transport costs. Follow up assessments were typically held in the SCCLS offices located within the court complex.
Intervention
Participants were prescribed 25 mg sertraline (day 1), then 50 mg (day 2), and 100 mg (day 3) for the remainder of the 3 months. Follow up assessments occurred at one and three months to examine changes in the screening measures. At the conclusion of the trial, participants were given the option of continuing on sertraline under their own GP. Those who wished to do so were provided with a referral letter.
Ethics approval was granted by the NSW Justice Health Human Research and Ethics Committee (GEN59/06). The trial was registered with the Australian and New Zealand Clinical Trials Registry (083214).
Statistical analysis
T-tests, chi-squared tests and tests of proportions were used to examine differences between those who completed the intervention and those who dropped out. Repeated measures analysis was used to examine changes over time in outcome measures. All analyses were conducted using SPSS 17 [29].
Results
Overall, 40 individuals contacted the research nurse to express an interest in the trial of whom 34 presented for further assessment. The others either could not be contacted despite repeated attempts, or met one of the exclusion criteria (e.g. female, scored below 70 on the BIS, or planned to move to an area with no prospect of follow up).
Of the 34 who were invited for further assessment, all were deemed to be medically fit to participate in the trial by a medical practitioner and commenced the treatment. Fourteen (41%) individuals who commenced the trial dropped out. All of those who dropped out did so between the initial assessment and the first scheduled follow up at four weeks. Most of those who dropped out (57%) could not be contacted and we were unable to ascertain the reason for this (Table 1). Three individuals discontinued due to side-effects adjudged to be ‘mild’ by the clinical staff.
Reasons for not completing the intervention for 14 individuals
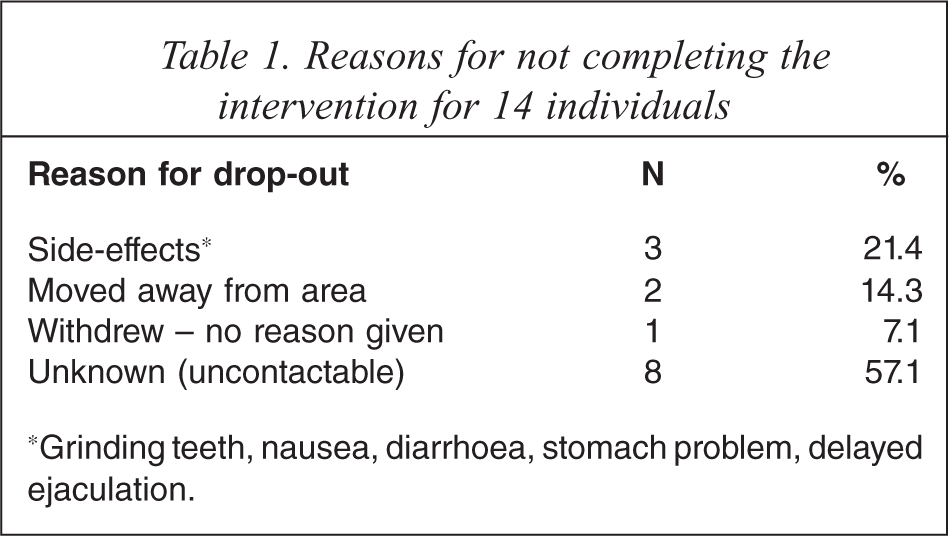
∗Grinding teeth, nausea, diarrhoea, stomach problem, delayed ejaculation.
The median time to the first follow up was 28 days (range 23–31 days) and the median time from baseline to the third follow up was 85 days (range 73–93 days). Those completing the three month trial had a similar profile at baseline to the non-completers with respect to demographic, criminographic, mental health, and behavioural measures (Table 2). While the completers tended to be slightly older than those who dropped out, this difference was not significant.
Demographic and criminographic characteristics of completers and non-completers
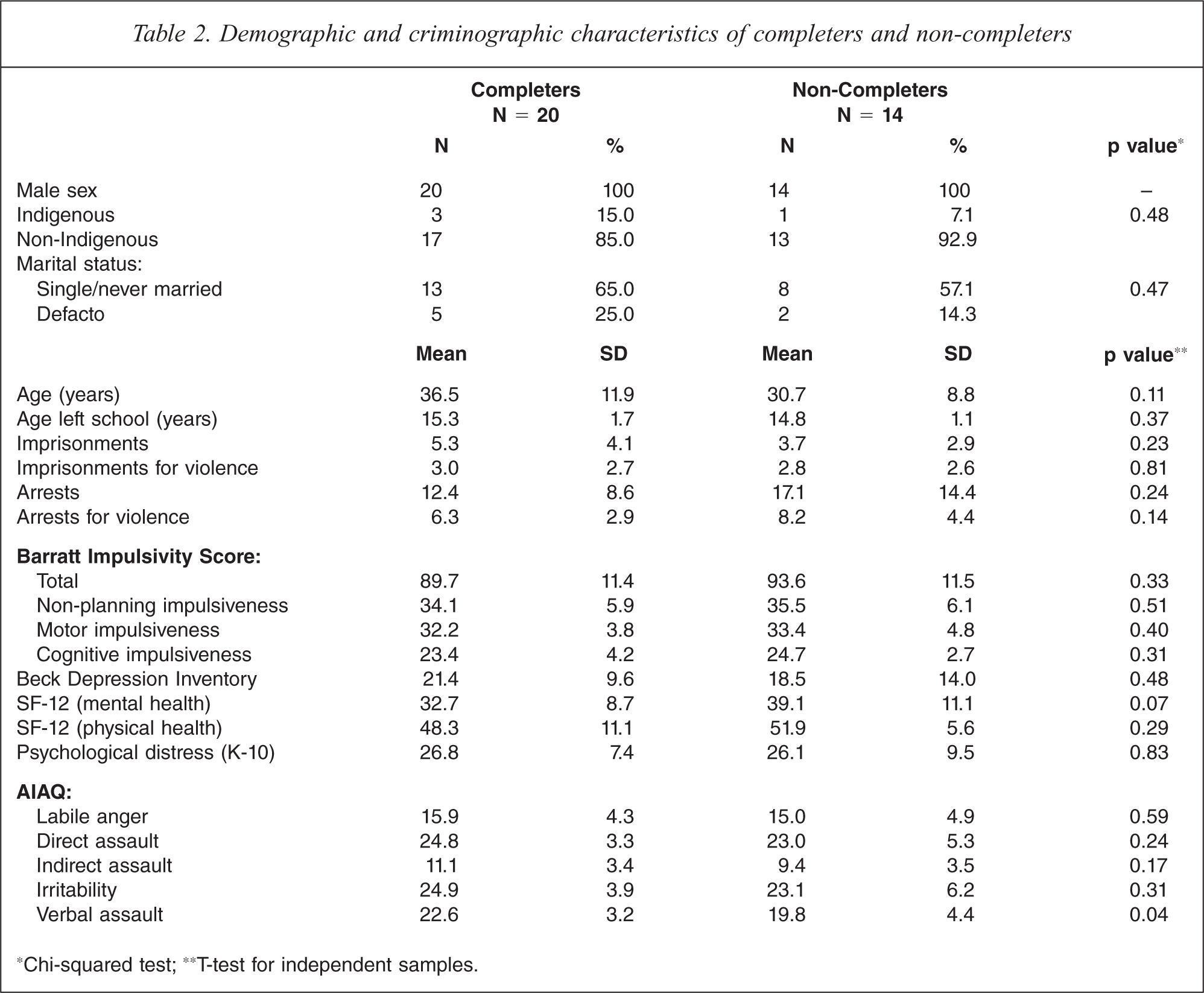
∗Chi-squared test; ∗∗T-test for independent samples.
Table 3 shows the mean scores at baseline, 1 and 3 months for a range of psychological and behavioural measures for those completing the trial. Repeated measures analysis identified significant improvements across all measures, apart from the K-10 and the physical health component of the SF-12 which showed no change.
Mean scores and percentage change at baseline, one, and three months for a range of psychological and behavioural measures
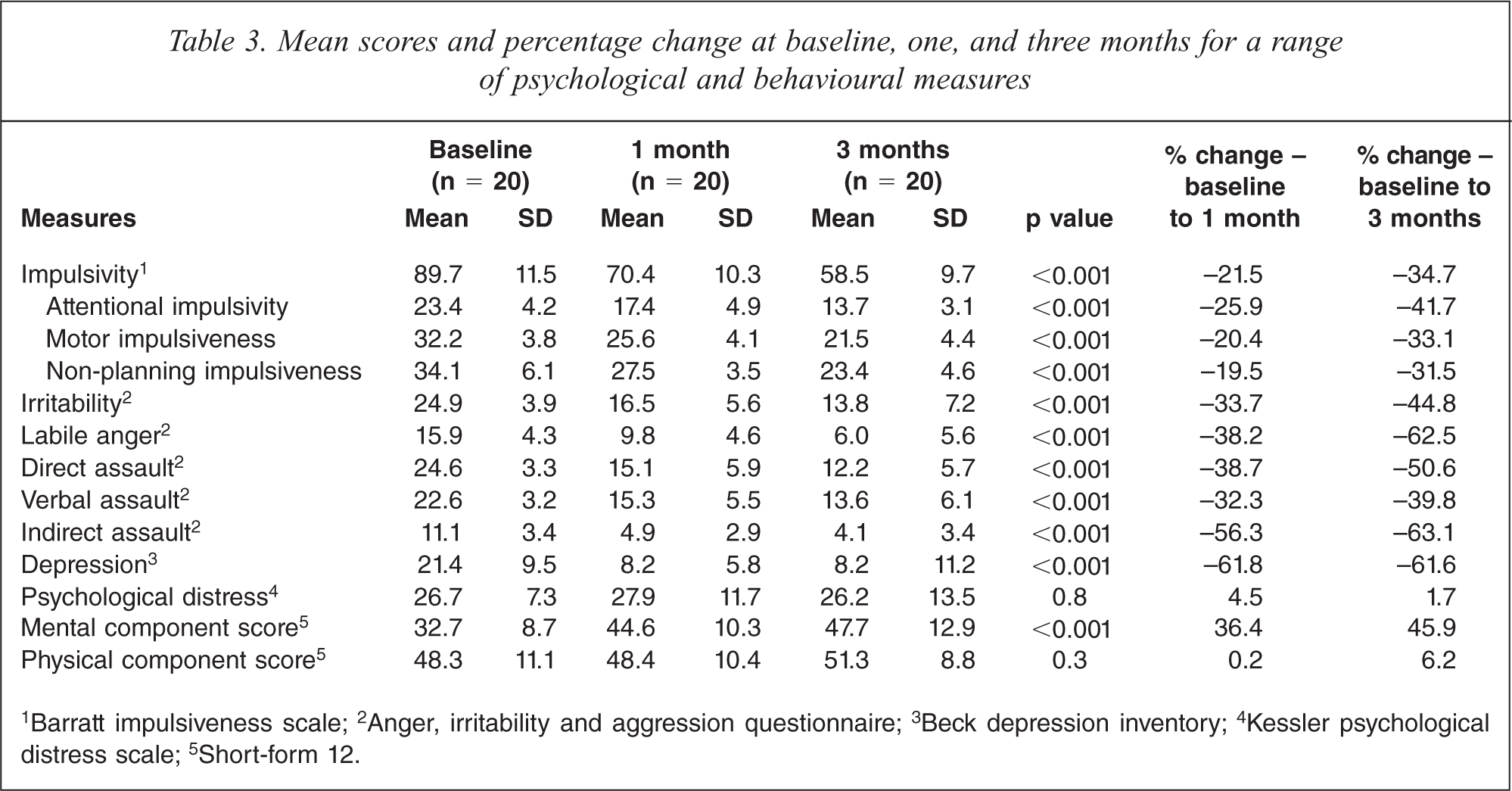
1Barratt impulsiveness scale; 2Anger, irritability and aggression questionnaire; 3Beck depression inventory; 4Kessler psychological distress scale; 5Short-form 12.
Impulsivity was a focus of this study and showed a 34.7% drop according to the BIS-11. While this instrument assesses general impulsiveness, it also allows for the assessment of three second-order factors (attentional impulsiveness, motor impulsiveness, and non-planning impulsiveness (Table 3) [30].
Depressive symptoms as measured by the BDI fell by 62% between the baseline and the one month follow up and by 62% from baseline to the three month assessment.
Discussion
This study is one of the first to examine the potential use of SSRIs to target impulsivity in an offender population and provides some evidence that impulsive violent individuals are willing to participate in such trials to help control this behaviour. Once established on sertraline, all participants continued on the medication until the end of the trial and all who completed the trial expressed a wish to continue taking sertraline under supervision by their own general practitioner.
Reductions were observed across a range of behavioural measures which may be relevant to criminal behaviour (impulsivity, anger, aggression, assaultive behaviour). Whilst the results are compelling, they are from an open-label trial with no control group and are based on a small number of participants. Caution is therefore warranted.
Our findings are consistent with other studies that have used SSRIs to target behavioural problems such as aggression, impulse control, and self-mutilation [19,20, 22,23,31]. Most of these studies have been undertaken in the USA and only one involved an offender population [22].
Many would consider those involved in such a trial (impulsive, perceived to be unreliable and dishonest, and itinerant) to be difficult to follow up. The drop-out rate was 41% with three individuals confirmed to have withdrawn due to side-effects from the medication. However, this drop-out rate is similar to that observed in placebo-controlled trials of anti-psychotic medication [32]. The remaining individuals who dropped out were either uncontactable or had moved out of the area.
All of those who completed the one month follow up continued on the medication for the remaining two months, which highlights the importance of regular contact with participants to address issues that might impact on dropping out. Remarkably, all of those who remained in the trial requested a referral to their own doctor to continue on the treatment post-trial. This is consistent with an observation from Norden (1989) in a trial of SSRIs in borderline personality subjects in which he remarks that ‘all twelve patients continue to take fluoxetine despite what is for some considerable expense’ [33]. The insights of this population into the potential for the treatment to improve functioning and behaviour (and reflected in the request for referral) was reinforced by anecdotal information provided to the research nurse. These related to improvements in relationships with family and friends and an ability to control addictive behaviours (gambling, coffee, cannabis).
Of particular interest was the impact of the treatment on impulsiveness, given the well-established link between impulsivity and offending behaviour [6–8]. We observed a 35% decrease in impulsivity between baseline and the three month follow up according to the Barratt Impulsivity Scale. Whether or not such a change would translate into a reduction in offending over a sustained period needs to be examined by an adequately powered randomized control trial with a placebo group.
Several other behavioural measures relevant to violence and aggression showed significant reductions. The Anger, Irritability and Aggression Questionnaire [17] examines aggressive behaviours using two overarching scales (irritability and aggression) and several subscales (labile anger, irritability, aggression, direct assault, indirect assault and verbal assault). Of particular relevance to behaviour likely to bring an individual into contact with the criminal justice system is ‘direct assault’ which measures behaviours involving physical force (e.g. getting into physical fights, wanting to harm others, and resorting to physical violence). A 51% reduction was observed between baseline and the three month follow up on this measure.
All of those recruited to the trial were screened by a psychiatrist and deemed not to be suffering from a major depressive episode sufficient to warrant exclusion from the trial. Among those who completed the trial, scores on the Beck Depression Inventory at baseline were categorized as ‘minimal/mild’ (n = 7, 35%), ‘moderate’ (n = 10, 50%), and ‘severe’ (n = 3, 15%) dropping to ‘minimal/mild’ (n = 18, 90%), and ‘moderate’ (n = 2, 10%) after one month. We compared impulsivity scores among those in the minimal/mild and severe groups and found falls of 23% and 21% respectively between baseline and one month suggesting that impulsivity was being targeted independently of depression. Furthermore, inclusion in the study was based primarily on impulsivity and not depression.
Participation in the study connotes insight on the part of subjects around their impulsivity/violence and the impact this has on their lives. Given the modest compensation paid to participants ($50 per assessment), it is unlikely that this was the prime motivator for participation. However, it is possible that some of those who were assessed at baseline were interested in making a ‘quick buck’ and had no intention to continue beyond receiving the initial $50. This could explain the loss to follow up of some of the eight individuals between baseline and the first follow up.
Despite the promising results, limitations of the study are apparent. The study was open-label with no control group. The regular contact between participants and the research nurse is likely to have exerted some influence over the findings although it seems highly unlikely that these interactions could explain the results in their entirety, no matter how therapeutic this contact was. The drop-out rate was 40% which is high but consistent with clinical trials of anti-psychotic medications for those allocated to the active medication [32]. Higher drop-out rates are typically observed for placebo groups [32]. It is possible that some of those who could not be contacted had withdrawn due to side-effects. Norden (1989) comments on the benefits of ‘careful dose titration’ in managing agitation, a known side-effect in some individuals taking SSRIs [33].
An advantage of the trial is that it was undertaken in the ‘real world’ and not in a highly controlled clinical setting. However, this likely contributed to our inability to remain in contact with some participants as they had moved away from the area. Should this approach to treating impulsive violent offenders be integrated into the arsenal of treatments available to violent offenders in the criminal justice system, problems of follow up and retention will need to be addressed.
Notwithstanding the logistical problems associated with this (pharmacological) approach to treatment, ethical issues will arise as to how society balances the needs of those individual with a predilection to impulsive violence against those of the general community who want a less violent society. One such ethical issue is the ability of individuals to control biologically pre-determined behaviours. In a recent Italian case a violent murderer's sentence was cut (by one year) due to ‘bad genes’ which, it was argued, were linked to his offending behaviour [34].
The results from this open-label study are promising and warrant the conduct of a carefully designed randomized control trial which includes a placebo group.
Footnotes
Acknowledgements