
Abstract
Prostate cancer (PCA) is the most commonly occurring cancer and the second major cause of cancer deaths in Australian men [1], even though a majority of sufferers will survive for a decade or more following diagnosis. Despite its significance for men's health, far less is known about the psychosocial impact of PCA and its treatment than that for breast cancer [2].
Research directed at quality of life in PCA has focused mainly on physical aspects of well-being, such as the side-effects of treatment, rather than the psychological facets, including emotional distress. Given the trajectory of the disease and its many effects on sufferers, the psychological and social adjustment of men with PCA is likely to be complex. Longitudinal studies of men's psychological reactions to living with the disease are particularly valuable in terms of understanding these complexities [2].
Psychosocial adjustment is likely to vary according to disease stage. Most early stage diagnoses emerge on routine check-ups that include prostate-specific antigen (PSA) testing. Many men will not experience symptoms and be unaware that they have problems [3]. Others may have relatively mild symptoms, such as bladder outflow obstruction, which they attribute to aging rather than cancer. In contrast, those whose disease has advanced (metastatic) may present with bone pain or other symptoms of spread. Or again, they may be asymptomatic, with disease advancement detected by a routine PSA check. Therefore, it is crucial to consider stage of disease in analysing psychological and social adjustment.
Several treatment options for PCA exist, with debate about the optimal indications for each. All are capable of affecting patient well-being. Options for localized disease include radical prostatectomy, external beam radiotherapy, transperineal brachytherapy or regular monitoring of progress without administering any active treatment [4]. Treatment for advanced disease is mostly androgen ablation and, later, chemotherapy and radiotherapy. Androgen ablation results in loss of libido, diminished genital sensation, loss of a firm erection, and limited return to sexual activity [5]. Body image changes, related to effects such as hot flushes and gynaecomastia, may lead to emotional distress. Overall, side-effects, particularly urinary incontinence, impotence and bowel symptoms, are common, and have psychosocial implications [2].
One crucial limitation of much research in this field is the lack of an appropriate comparison group [2]. Controlled studies are uncommon. Psychosocial problems in PCA patients could be due to other factors such as socioeconomic concerns or fears of aging, while depression could represent grieving for family members or friends who have died or become seriously ill. To address this limitation, we included men recruited from the community, of similar age and residential area, currently free of cancer.
The aim of the present paper was to report the initial data from a longitudinal study of psychosocial adjustment in men with early stage and advanced PCA, following diagnosis, compared to men from the community, of similar age and residential area. We hypothesized poorer psychosocial adjustment in patients with advanced disease, and poorer adjustment in both patient groups than in the comparison group.
Methods
Participants
We recruited cohorts of men differentiated by PCA disease stage and treatment method. Newly diagnosed patients with either early or advanced stage PCA attending participating clinics were invited to take part before receiving any definitive treatment. Inclusion criteria for the early stage group included histologically confirmed PCA, T1–T3, N0, M0. For advanced disease, the criterion was evidence of spread to lymph nodes or elsewhere, thus N1 or M1. Exclusion criteria included inability to give informed consent, diagnosis of another cancer, minimal understanding of English, psychosis, intellectual disability or dementia. In the early stage category, recruitment was initially monitored to ensure comparable numbers of ‘watchful waiting’, surgery and radiotherapy treatment conditions, and in the advanced group, good representation of hormone-responsive, newly progressive, and hormone-resistant and progressive subgroups. Community comparisons were men of similar age and residential areas, randomly selected from the phone directory and invited by telephone to take part. Their exclusion criteria included any current cancer diagnoses, although other states of ill-health were not exclusionary.
Design
The research committees in all participating hospitals granted ethics approval. Research assistants obtained informed consent from eligible men who had expressed a willingness to participate. They administered self-report questionnaires, face to face whenever possible, and assisted with interpretation of items as necessary. Completion of questionnaires took around 30–45 min. In order to avoid excessive burden on the men at the time of the PCA diagnoses, we undertook the structured psychiatric interview by telephone up to 3 months later. The CIDI computer software generated DSM-IV psychiatric diagnoses from their responses.
Measures
Self-report measures included the following.
Short-Form 36-item Health Survey
The Short-Form 36-item Health Survey (SF-36) [6] is a well-validated and reliable measure both of physical and mental aspects of health-related quality of life [7]. It has eight subscales, four covering physical health and four relating to mental health, which are used here. ‘Vitality’ refers to the balance of energy and fatigue levels. ‘Social functioning’ is related to performance of normal social activities without interference from physical or emotional problems. ‘Role-emotional’ refers to performance of work or other daily activities without interference. ‘Mental health’ is related to the balance between feelings of nervousness and depression and feeling peaceful, happy and calm. Low scores on these subscales indicate poorer functioning.
Brief Symptom Inventory
The Brief Symptom Inventory (BSI-53) [8], comprising 53 items covering diverse psychological symptoms, has good reliability (e.g. coefficient alphas 0.68–0.91), and established convergent and predictive validity [9]. It has been extensively used with cancer populations. The BSI-53 has nine subscales and a General Severity Index (GSI).
Dyadic Adjustment Scale
A short form, consisting of seven questions, of the Dyadic Adjustment Scale (DAS), was used. The first six items comprise a subscale for marital satisfaction (reliability 0.96) [10]; higher scores indicate better relationship adjustment, with the potential range from 0 to 30.
Family Relationships Index
The Family Relationships Index (FRI) is used to measure cardinal features of family functioning [11]. It contains three subscales of four items each, covering cohesiveness, expressiveness, and conflict. A total score, within a range of 0–12, indicates level of family functioning. Families dealing with cancer find it acceptable and it is reliable and valid in this context [12].
Composite International Diagnostic Interview
We used the anxiety and depression modules of the Composite International Diagnostic Interview (CIDI) [13], because these psychiatric categories are the most common in cancer patients. The CIDI generates psychiatric diagnoses according to criteria of the DSM-IV [14], and has confirmed reliability [15] and validity [13]. The CIDI takes account of symptoms associated with physical illness (including cancer and its treatments) when determining depression or anxiety diagnoses.
Statistical analysis
Descriptive statistics for the patient groups were examined to exclude effects of site and treating clinician. Because no significant differences emerged, they were combined for further analyses. Multivariate analyses of variance (MANOVA) were conducted using SPSS 14.0 software package [16] to detect any differences between the three groups. Post-hoc Scheffe tests determined the direction of significance.
Results
Respondents
Initially, 367 men with early (211, 57.5%) or advanced stage (156, 42.5%) PCA took part. The community comparison group consisted of 169 men who were free from PCA. Details of their sociodemographic characteristics are summarized and compared in Table 1. A greater proportion of the advanced group were retired and they were older, on average, than the early and the comparison group. Splitting the comparison group at the median age showed that there were no differences in age between the advanced disease and older of the two subgroups. No other differences were apparent. This suggests that differences were essentially disease related and further analyses were conducted using the original three categories.
Subject sociodemographic characteristics
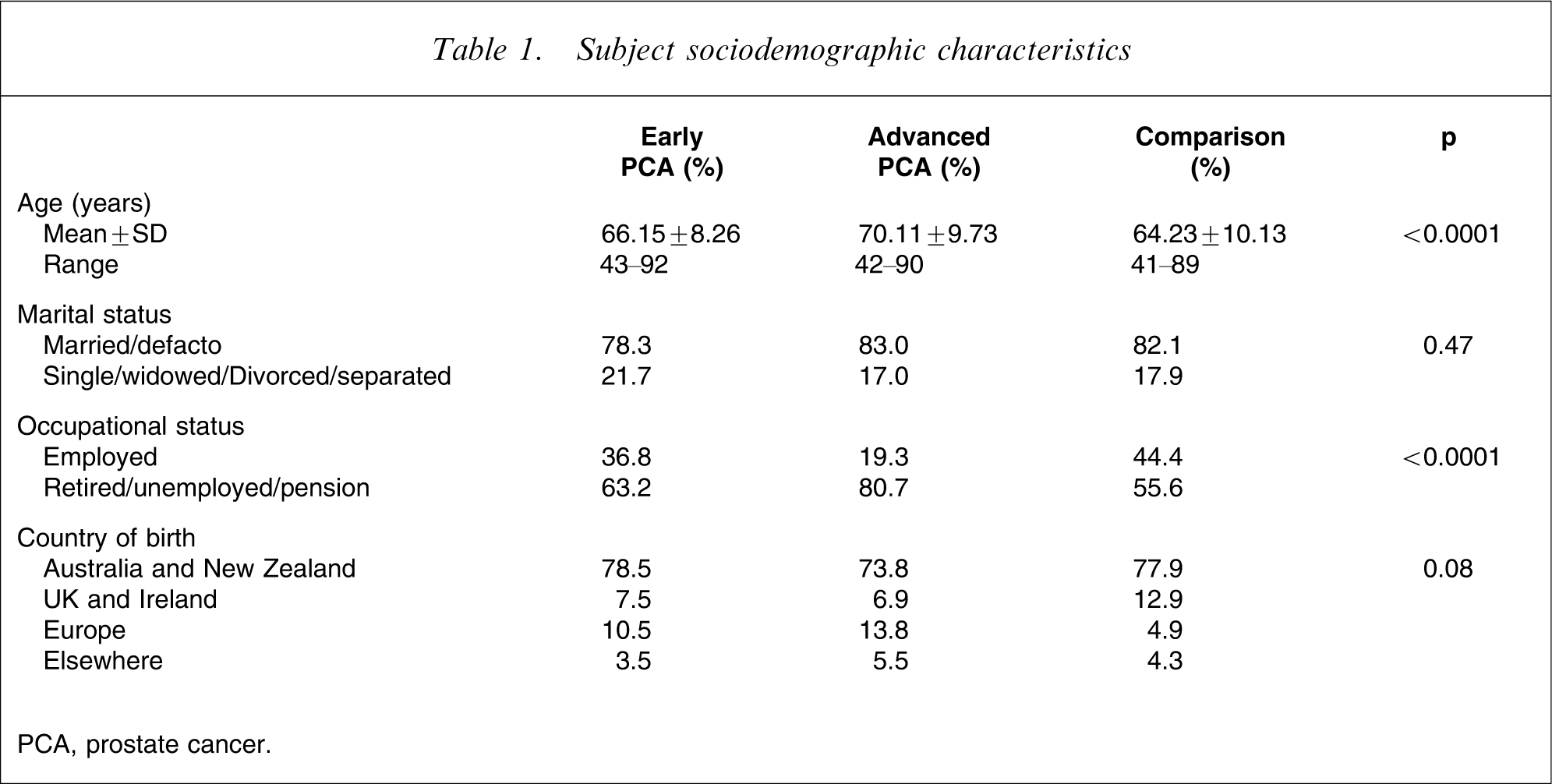
PCA, prostate cancer.
Clinical features
According to medical records, at recruitment, 57.5% of patients had early stage and 42.5% had advanced disease. The majority of the clinical sample (80%) had not had cancer before their prostate diagnosis. Gleason scores ranged from 2 to 10, with the modal score being 6–7 (59%). Mean Gleason scores for the early group (6.5±1.2) differed significantly from the advanced disease group (7.8±1.3). Mean PSA values at baseline were 84.9 (±332.4). Non-parametric analysis showed that the advanced disease values were significantly greater than those of the early group. Metastases had occurred for 41%: one-third had bone, one-sixth, nodal, and 6% visceral. In terms of treatment, 17% had been in a watchful waiting condition, 53% radiotherapy, and 30% surgery. More than 50% of those with metastatic disease were receiving hormone therapy in the form of luteinizing hormone-releasing hormone analogues and 45%, anti-androgens.
Psychosocial adjustment
Descriptive statistics for each of the three groups on the self-report measures and their subscales appear in Table 2.
Self-report measures and subscales
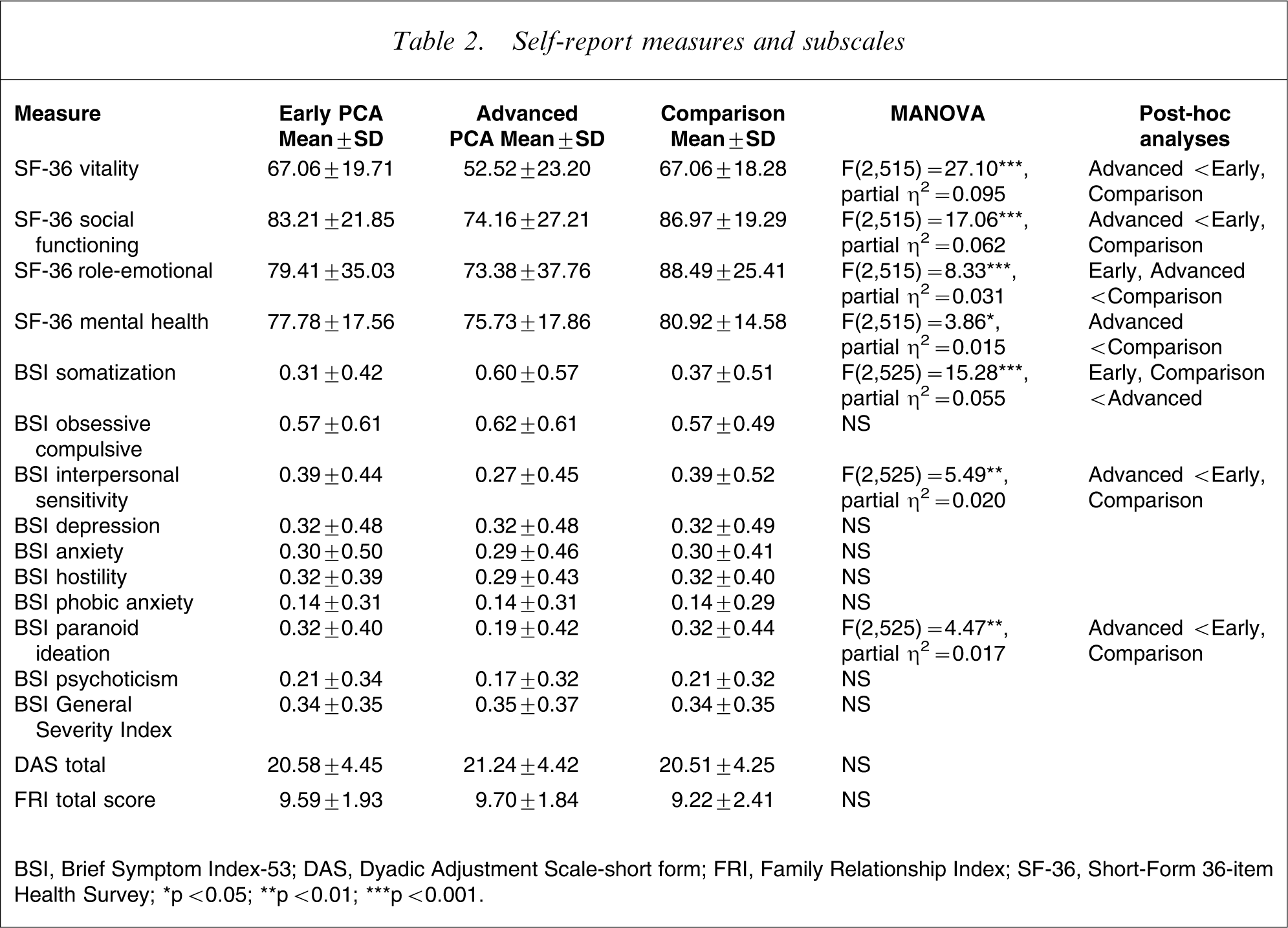
BSI, Brief Symptom Index-53; DAS, Dyadic Adjustment Scale-short form; FRI, Family Relationship Index; SF-36, Short-Form 36-item Health Survey.; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Differences between the three groups on all four mental health subscales of the SF-36 were significant. For the vitality and social functioning subscales, the differences were between the advanced group and both the other two groups. For the role-emotional subscale, the differences were between both the two clinical groups and the comparison group. For the mental health subscale, the advanced and comparison groups differed significantly.
Global distress, as measured by the GSI of the BSI, did not differ significantly between the three groups. But subscale scores were significantly different for men with advanced stage PCA compared to both the early PCA and comparison groups on somatic symptom distress, interpersonal sensitivity and paranoid ideation.
Analyses of the DAS and the FRI scores indicated no significant differences between the comparison, early and advanced groups.
Psychiatric morbidity
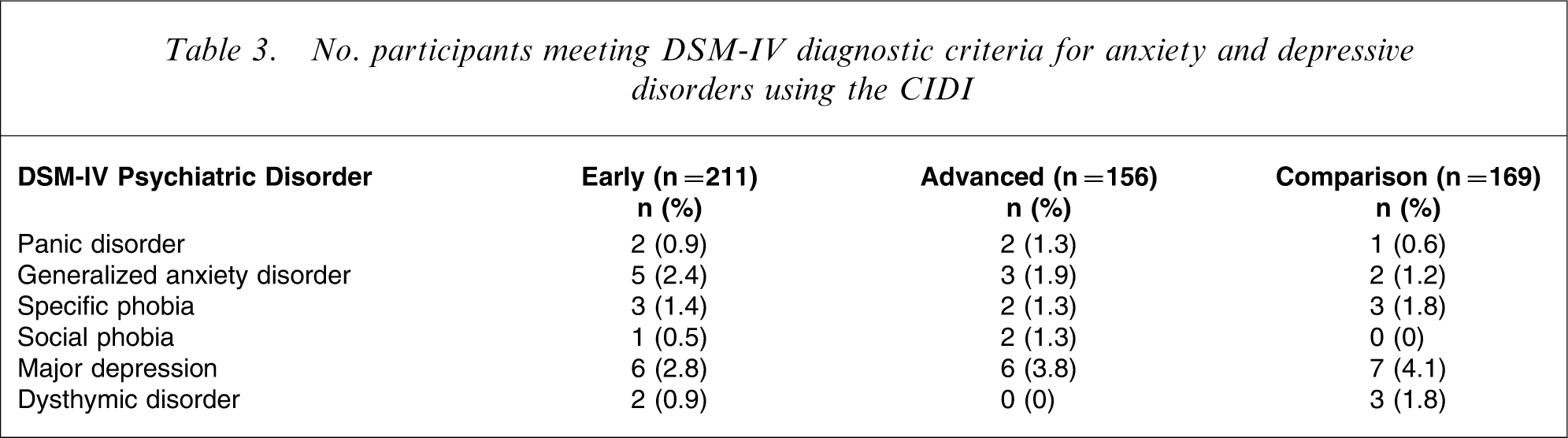
Diagnostic rates, derived from the CIDI interviews, are summarized in Table 3. Rates overall were low, with no difference in the prevalence of depressive disorders, but a slight increase in the rates of anxiety disorders for early (n = 11, 5.2%) and advanced stage (n = 9, 5.8%) PCA compared to the comparison group (n = 6, 3.6%).
No. participants meeting DSM-IV diagnostic criteria for anxiety and depressive disorders using the CIDI
Discussion
Our aim was to examine differences in psychosocial adjustment between men with early and advanced stage PCA shortly after diagnosis, and those in a community comparison group. In terms of psychiatric disorder, few differences emerged. Rates of depression and anxiety were low overall, and although anxiety disorders were a little higher in the patient groups, the difference was not as great as might be anticipated given the men's serious illnesses. Taken together, the results suggest that diagnosis of PCA does not contribute directly to an increased prevalence of diagnosable psychiatric states.
This picture differs markedly from that encountered in women facing a diagnosis of breast cancer [17]. The differences are possibly related to men with PCA being diagnosed at a much later point in the life cycle [2] and their relatively lesser biological vulnerability to affective disorder. Coping strategies they deploy to deal with the major stressor of cancer diagnosis [18] may also play a role. Men may be more inclined to construe treatment, an active problem-solving strategy, as a solution to their problems and be less concerned with the meaning of the complex and dynamic events that represent adaptation to a major chronic, and potentially lethal, illness [19]. Finally, several studies have shown that the physical side-effects of treatment used in PCA become the focus of patients’ emotional preoccupations [2].
All four psychosocial dimensions of the SF-36 – vitality, social functioning, role-emotional, and mental subscales – were significantly affected by a diagnosis of PCA. The questionnaire indicated notable differences between the groups in terms of social and emotional reactions, demonstrating that men with PCA do experience forms of psychological distress, even if they do not meet criteria for a diagnosable psychiatric disorder. Previous research using the SF-36 with prostate cancer patients has produced mixed results. In one major study, men with PCA reported some psychological symptoms, but these were at a similar level to those found in healthy controls [20]; in another sample, psychological aspects were affected as much as the physical ones [21]. In the present study men with advanced stage PCA had lower vitality and poorer social functioning than the other two groups and their mental health scores were lower than those of the comparison group. Both clinical groups were more affected than the controls in terms of emotional role. These reactions point to burdens borne by the men (and possibly their partners), as they struggle with physical problems in the aftermath of treatment [22]. As mentioned here, appropriate psychosocial intervention at this critical juncture might facilitate patients developing more effective coping strategies for the stresses they face.
On the BSI subscales, men with advanced stage PCA had higher somatization scores (a greater physical symptom burden, as one would expect), but lower interpersonal sensitivity and paranoid ideation levels than both early stage patients and the comparison group. While the latter finding might mean that the men become more self-focused as a result of their condition, it also suggests that those with advanced disease might experience less social discomfort about the disease and its effects and are less vulnerable to perceived social criticism. Men with PCA who are psychologically distressed have difficulty discussing their condition with others [23]. If their distress is related to perceived social criticism, it might explain why they are less likely to talk about their condition with others. This, in turn, may impede the ‘processing’ (a term familiar to those working in trauma-related areas) of their experiences with members of their support networks, a coping strategy that typically has the effect of reducing distress [23].
We were surprised that no differences emerged between the three groups in terms of couple adjustment and family relationships, key spheres of psychosocial functioning. Couples and family members in the present sample might have enjoyed sufficiently robust relationships to be able to deal with the stresses of diagnosis and initial treatment and cope effectively, foster closeness and elicit a sense of mutual support. Alternatively, men's partners might be better able to communicate any distress the couple or family experience. In a related study, we have produced preliminary results that support this likelihood [24]. Continuing psychosocial distress may exert a long-term deleterious effect on relationships, a possibility that deserves closer study.
It is also possible that the measures we used were not sensitive enough to capture the types of dysfunction that result from the diagnosis and treatment of PCA. The need for a more sophisticated measure of intimacy and communication stands out in this context. A qualitative approach in which interview-derived data are analysed is more likely to reveal unique dimensions of relational distress than conventional measures of adjustment.
It should be noted that the time difference between participants’ completing the distress measures (at recruitment) and the CIDI interview (up to 3 months later) may also help account for the discrepancies between the two indices. The delay was designed to reduce the initial burden of participation at a very sensitive time for the men and also to allow for diagnoses that include a time specification (e.g. major depression). But, consistent with crisis theory [25], it is possible that any initial distress reactions to the acute stressor of receiving a diagnosis would have been captured by the self-report but would have settled by the time of the interview. This explanation would not account for all the findings, because the overall level of distress soon after diagnosis was lower than expected based on comparable studies of other cancer patient groups. Further research of men's reactions to diagnosis of prostate cancer is required to address this question.
Other limitations of the study include the recruitment of participants via clinics, which may have introduced potential selection bias because not every patient has an equal chance of being involved. Recruitment of consecutive clinic attendees is an accepted form of sampling in psycho-oncology research, because it represents a practical way to access PCA cases at a critical juncture. Alternative methods face other potential hazards. Sampling through cancer registries may reduce selection bias, but creates inevitable delays at the time when men are dealing psychologically with diagnosis. Seeking recruits through advertisements, at information sessions, or from self-help group members, risks potential self-selection bias.
Given the aforementioned findings, we cannot but be impressed by the resilience of the men in both PCA groups. Yet, as we follow these men (research we have in progress), we anticipate that treatment side-effects such as incontinence, erectile dysfunction and bowel symptoms, and related psychosocial forces, may have adverse effects on health-related quality of life [2]. These will no doubt in turn become the focus of greater clinical and research attention. Psychosocial interventions and supportive care for men with PCA is not widespread currently, possibly because men's needs are not fully understood. While research progress of this kind has been made in relation to women with breast cancer, the full picture in PCA remains to be drawn. The data we have reported here, complemented with our follow-up investigation, will help shed light on how we can best assist both patients and their partners.
Footnotes
Acknowledgements
This work was supported by the National Health and Medical Research Council of Australia and the Bethlehem Griffiths Research Foundation.