
Abstract
Objective:
People with severe mental illness have similar cancer incidence, but higher mortality than the general population. Participation in cancer screening may be a contributing factor but existing studies are conflicting. The aim of this study was to investigate the frequency of colorectal, prostate and cervical cancer screening among people with and without severe mental illness in Australia, who have access to universal health care.
Methods:
We followed three cohorts using de-identified data from a random 10% sample of people registered for Australia’s universal health care system: those aged 50–69 years (n = 760,058) for colorectal cancer screening; women aged 18–69 years (n = 918,140) for cervical cancer screening and men aged 50–69 years (n = 380,238) for prostate cancer screening. We used Poisson regression to estimate incidence rate ratios and 95% confidence intervals for the association between severe mental illness and rates of faecal occult blood testing, pap smears and prostate-specific antigen testing.
Results:
Having severe mental illness was associated with a 17% reduction in rates of pap smear (incidence rate ratio = 0.83, 95% confidence interval: 0.82–0.84) and prostate-specific antigen testing (incidence rate ratio = 0.83, 95% confidence interval: 0.81–0.85), compared to the general population. By contrast, incidence rates of faecal occult blood testing were only lower in people with severe mental illness among the participants who visited their general practitioner less than an average of five times per year (incidence rate ratio = 0.83, 95% confidence interval = [0.73, 0.94]).
Conclusion:
Our results suggest that differences in screening frequency may explain some of the mismatch between cancer incidence and mortality in people with severe mental illness and indicate that action is required to improve preventive screening in this very disadvantaged group.
Introduction
People with severe mental illness (SMI), such as schizophrenia and bipolar affective disorder, have higher rates of morbidity and mortality (Lawrence et al., 2013; Liu et al., 2017). As a result, their life-expectancy is 10–20 years lower than that of the general population (Lawrence et al., 2013; Liu et al., 2017), even though incidence rates of many cancers, including colorectal and prostate cancer, are similar between people with and without SMI (Kisely et al., 2008). Given the similar incidence rates, differences in risk factor prevalence (smoking, alcohol consumption, obesity) are less likely to be the cause of higher cancer mortality in those with SMI. One explanation might be that people with SMI present with more advanced cancer at diagnosis or receive less cancer-directed treatment, which could be due to either diagnostic delays, poorer access to cancer services or lower participation in cancer screening programmes (Kisely et al., 2013).
Prior studies have investigated particular types of cancer screening in people with SMI, but these were mostly conducted in specific populations and results may not be broadly generalisable (Howard et al., 2010). Furthermore, some studies used self-reported participation in screening, which may not be optimal in this population (Fujiwara et al., 2017; Howard et al., 2010; Mo et al., 2014; Siantz et al., 2017), while others had no comparison group (Howard et al., 2010; James et al., 2017). The aim of this study was to investigate the frequency of colorectal, prostate and cervical cancer screening among people with and without SMI, throughout Australia, using a large, nationally representative administrative data set of 10% of the Australian population.
Methods
We conducted a retrospective cohort study using de-identified administrative data from a sample of 10% of all Australians registered for Medicare. Medicare is Australia’s universal health care scheme that provides access to government-subsidised medical services (via the Medicare Benefits Scheme [MBS]) and prescriptions (via the Pharmaceutical Benefits Scheme [PBS]) for all citizens and permanent residents. The 10% data set included both MBS and PBS information. Within the MBS data, each specific medical service subsidised by the Australian government is denoted by an item number. The PBS data included details of all medicines dispensed to patients at government-subsidised prices. In accordance with the 2014 National Health and Medical Research Council Statement on ethical conduct in human research, ethics approval was not required to use these de-identified data. We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for reporting observational studies (Von Elm et al., 2007).
Defining exposure
We used PBS data to define people with SMI (schizophrenia or bipolar affective disorder). In Australia, the most commonly prescribed medications for these conditions are lithium and second-generation antipsychotic agents. Lithium is specific to bipolar affective disorder and rarely prescribed for other conditions, while second-generation antipsychotics require an indication-specific authority code for subsidy through the PBS. These are almost solely for treatment of either schizophrenia or bipolar affective disorder (Supplementary Table 1). During the study period, the only other PBS indication for second-generation antipsychotics for adults was behavioural disturbance secondary to either dementia or autism, and this was restricted to risperidone. Our study only included people aged 18–69 years (see in the following). As the onset of dementia before 70 years is uncommon (<4% prevalence; Anstey et al., 2010), and the prevalence of autism in adulthood is also very low (<1% in 2012; Australian Institute of Health and Welfare [AIHW], 2017), the few people receiving risperidone for behaviour disturbance in dementia or autism would have been minimal.
We classified a person as having an SMI once they had two prescriptions for one of these medicines dispensed within a 12-month period (Supplementary Table 1). PBS data from the year prior to cohort entry were used to determine exposure status at cohort entry. Participants who had not met the criteria for SMI prior to study commencement (January 2004) were considered unexposed to SMI until they received a second prescription for an SMI medication.
Prior to 2012, lithium prescriptions were only recorded in the PBS for people who held a means-tested concession card, as before that, pharmacies only recorded subsidised prescriptions. As lithium was relatively cheap, people without a concession card would have paid the full cost without subsidy. To minimise any bias as a result of this differential inclusion of people of lower socioeconomic status, we treated people who used lithium, and no other SMI medication, as unexposed to SMI. We conducted sensitivity analyses to (a) treat lithium-only users as exposed from 2012 onwards, (b) include lithium-only users as exposed for the whole study period and (c) exclude lithium-only users entirely. All authority prescriptions for second-generation antipsychotics were recorded for the entire study period for both concessional and non-concessional patients because of the higher costs of these medicines. First-generation antipsychotics are below co-payment, do not require an authority prescription recording indication for use, and make up only a small proportion of prescribed antipsychotics (Hollingworth et al., 2010). They were therefore not used for analysis.
Data were available to 31 December 2014, which was the study end date. We created study cohorts to examine screening for three cancers according to age-specific screening recommendations. In each case, screening is billed to Medicare and therefore captured by MBS records. We did not examine breast cancer screening as the Australian Breast Screen programme is not funded through Medicare. Although there is no formal prostate cancer screening programme in Australia and population-based screening is generally not recommended in clinical practice guidelines, prostate-specific antigen (PSA) testing is both commonly requested by male patients and recommended by clinicians (Pickles et al., 2016). Thus, differences in PSA testing between people with, and without, SMI may serve as a marker of access to preventive care.
The cervical cancer screening cohort included all women aged from 18 to 69 years, the eligible age group for screening under the National Cervical Screening Programme. During the study period, most pap smears were performed by a general practitioner (GP) and billed to Medicare (Lew et al., 2012). The colorectal cancer screening cohort included all men and women aged 50–69 years, while that for prostate cancer was restricted to men aged 50–69 years. The MBS data did not include screening performed through the Australian National Bowel Cancer Screening Programme (NBCSP) that was progressively rolled out over the period covered by our study. This national programme commenced in 2006, and initially, only people turning 55 and 65 years old each year were invited to participate and sent a kit for faecal occult blood testing (FOBT). In 2008, this programme was extended to people in the year they turned 50 years and in 2013 to people turning 60 years (Jenkins, 2016). From 2015 (after the end of follow-up in this study), the programme was extended to people aged from 50 years up to 74 years. Over the transition period from 2006, GPs were still encouraged to screen the many people who fell outside of eligibility for the NBCSP by requesting FOBT via the MBS (Foreman, 2009).
Participants entered our study on 1 January 2004 or the date they reached the minimum age for entry into each cohort. Participants left the study either on 31 December 2014 or when they turned 70 years. Person years were adjusted to include only 12 months before the first MBS record and 12 months after the last MBS record, given we did not have death records or records of participants arriving or leaving Australia. We removed participants with no MBS or PBS records within 12 months of study entry and exit (Figure 1). We performed sensitivity analyses to include person years for both 2 and 3 years from an individual’s first and last MBS record.
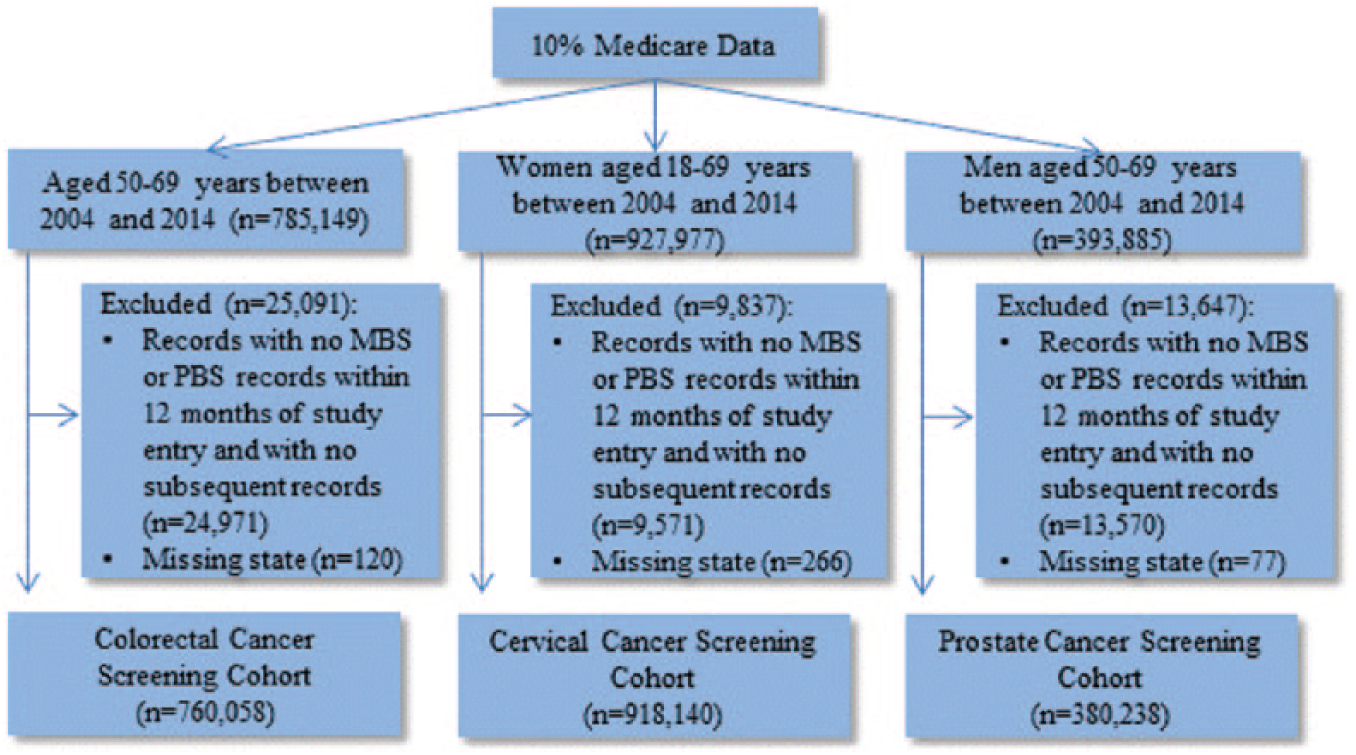
Study population for each cohort.
Variables
FOBT was used to define colorectal cancer screening, pap smears for cervical cancer screening, and PSA testing for prostate cancer screening using MBS item codes (Supplementary Table 2). It was possible for an individual to have multiple MBS items relating to a potential cancer screening test, therefore only one test per calendar year per participant was recorded as an incidence of cancer screening so as to exclude tests repeated for follow-up of an abnormality. For colorectal cancer screening, we recorded the incidence of each of the three specific FOBT item codes, which differed according to whether one, two or three samples were collected during a 28-day period. As noted previously, colorectal cancer screening through the Australian NBCSP was not recorded in the MBS records; we therefore only included FOBT organised by a medical practitioner outside of this programme. We only included the PSA item codes relating to probable cancer screening and not for tests performed as follow-up for previously diagnosed prostate disease.
Covariates included age at study entry, gender, state of residence and average annual number of GP visits. As only the year of birth was included in the de-identified data, we used the year’s midpoint (30 June) to estimate age at entry into the cohort. The MBS data contained five states of residence categories (New South Wales/Australian Capital Territory, Victoria/Tasmania, Queensland, South Australia/Northern Territory and Western Australia), and we defined state of residence as the last category provided in the MBS records for each participant. Participants with missing state data were excluded from the cohort (Figure 1).
We estimated the average number of GP visits per year across the study period using the total number of GP visits for all calendar years, divided by the total number of calendar years that the participant was included in the cohort. If the participant was prescribed an SMI-defining medication, average GP visits for the exposed time included the year they were defined as having an SMI. Average GP visits were also used as a categorical variable, split by less than five and five or more visits per year.
Statistical methods
We used Poisson regression to estimate incidence rate ratios (IRR) and 95% confidence intervals (CIs) for the association between SMI and rates of FOBT, pap smears and PSA testing. We performed multivariable analyses adjusting for age at entry, state of residence and gender (for colorectal cancer screening), with and without average GP visits in the models, as prior studies have shown that the number of GP visits may be a mediator for the association between SMI and cancer screening. As a sensitivity analysis, we split the cohorts into the two categorical groups for average GP visits to explore the association between SMI and cancer screening for people with similar GP contact. We also stratified the data by age categories (50–59 and 60–69 years for FOBT and PSA, and 18–29, 30–30, 40–49, 50–59 and 60–69 years for pap smear screening), to investigate whether associations between SMI and cancer screening varied by age group.
Additional sensitivity analyses were performed for the colorectal cancer screening cohort, by splitting the data into two study periods (2004–2006 and 2007–2014) given the introduction of the NBCSP in 2006, as well as each of the three FOBT MBS codes (66764, 66767 and 66770).
Results
There were 760,058 people in the colorectal cohort, 918,140 in the cervical screening and 380,238 in the prostate cancer screening cohorts (Figure 1). Approximately 2% of each cohort had a diagnosis of SMI (Table 1). The maximum follow-up was 11 years, with a median of 7.5 years for the colorectal and prostate cancer screening cohorts and median of 11 years for cervical cancer screening. Table 1 shows the characteristics of the cohorts by SMI status. For all cohorts, the average number of GP visits was higher for people with SMI than those without SMI (Table 1). Age at entry and distribution by state were similar between the groups.
Characteristics of cohort members with and without severe mental illness (SMI).
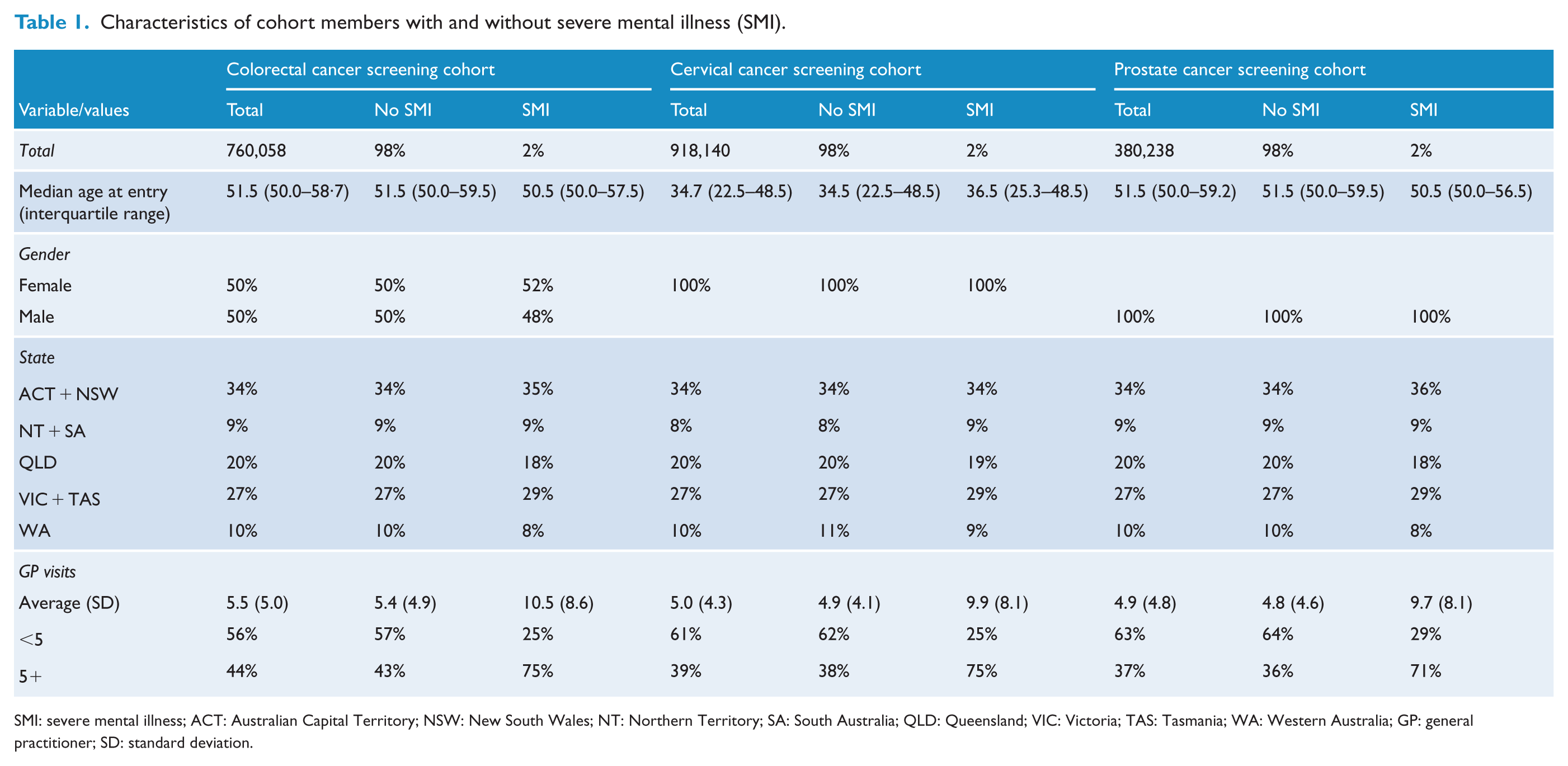
SMI: severe mental illness; ACT: Australian Capital Territory; NSW: New South Wales; NT: Northern Territory; SA: South Australia; QLD: Queensland; VIC: Victoria; TAS: Tasmania; WA: Western Australia; GP: general practitioner; SD: standard deviation.
The associations between SMI and cancer screening are shown in Table 2. Adjusting for age at entry, state and gender (FOBT only) did not materially change the results, and IRRs are adjusted for these factors unless otherwise stated. Having SMI was associated with lower rates of pap smears (IRR = 0.83, 95% CI = [0.82, 0.84]) and PSA testing (IRR = 0.83, 95% CI = [0.81, 0.85]) compared to people without SMI. When the average number of GP visits was included in the model, the IRRs declined further for pap smears (IRR = 0.74, 95% CI = [0.73, 0.75]) and PSA testing (IRR = 0.72, 95% CI = [0.70, 0.74]).
Associations between severe mental illness (SMI) and faecal occult blood testing (FOBT), pap smears and prostate-specific antigen (PSA) testing.
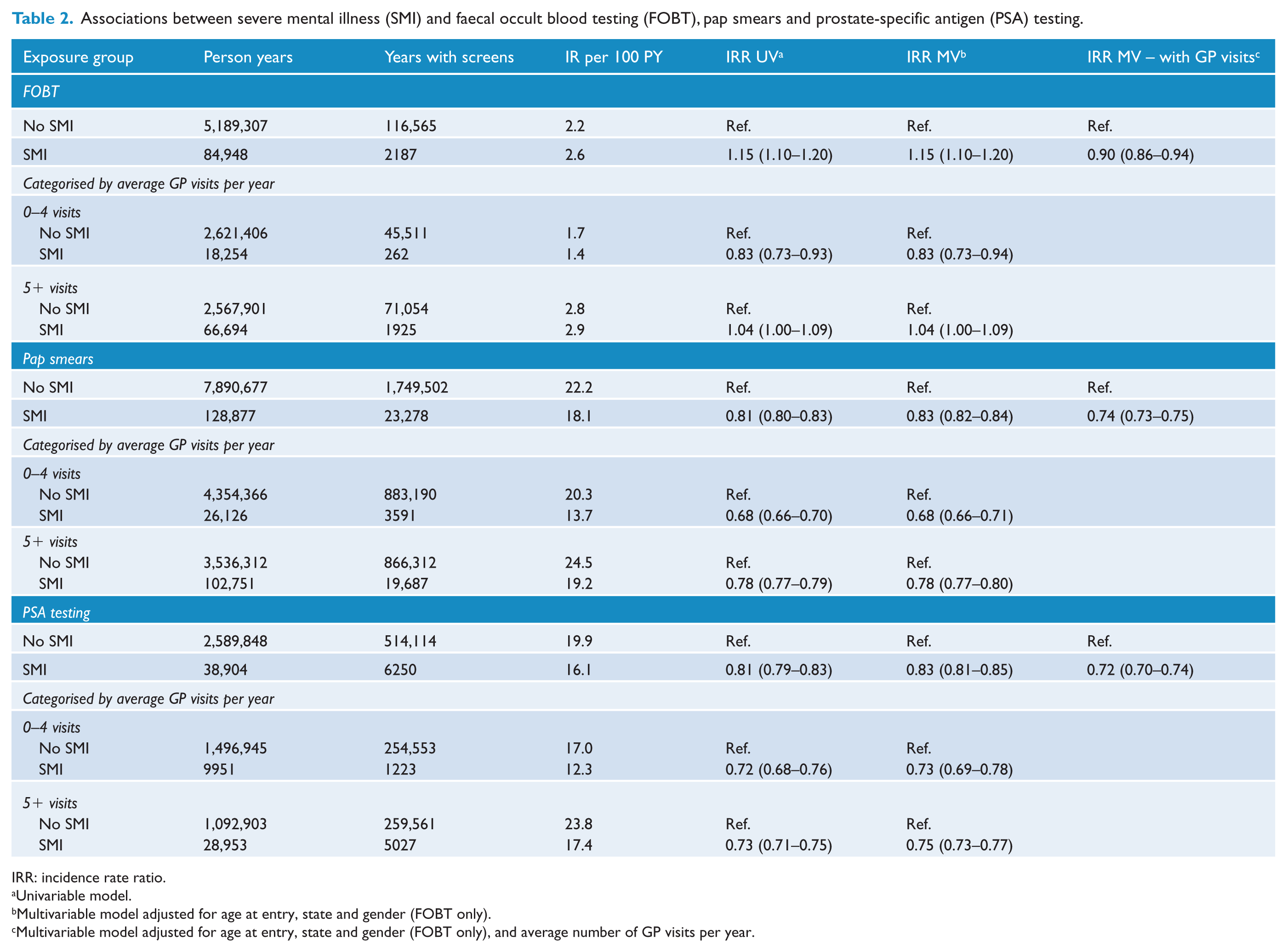
IRR: incidence rate ratio.
Univariable model.
Multivariable model adjusted for age at entry, state and gender (FOBT only).
Multivariable model adjusted for age at entry, state and gender (FOBT only), and average number of GP visits per year.
Having SMI was associated with slightly higher rates of FOBT compared to not having SMI (IRR = 1.15, 95% CI = [1.10, 1.20]) although overall, FOBT rates were low for both people with and without SMI (2.6 and 2.2 per 100 person years, respectively). However, after adjusting for average number of GP visits, people with SMI had lower rates of FOBT (IRR = 0.90, 95% CI = [0.86, 0.94]). To investigate this further, we dichotomised the cohort into those with an average of less than five GP visits per year and those with an average of five or more GP visits per year. In those with an average of less than five GP visit per year, SMI was associated with lower rates of FOBT (IRR = 0.83, 95% CI = [0.73, 0.94]). By contrast, in those who visited their GP an average of five or more times per year, SMI was associated with slightly higher rates of FOBT (IRR = 1.04, 95% CI = [1.00, 1.09]). Incidence rates for FOBT during 2007–2014 were close to double the rates in 2004–2006, but this did not substantially alter our unadjusted or adjusted IRRs (Supplementary Table 3).
Our analyses stratified by age showed that having SMI was consistently associated with reduced rates of pap smear screening in the 30–39, 40–49, 50–59 and 60–69 year age groups but the association was weaker in women aged 18–29 years (IRR = 0.96, 95% CI = [0.93, 0.99]; Supplementary Table 5). When we adjusted for average GP visits, the association between having SMI and pap smear testing was similar across the different age groups (Supplementary Table 5) and was consistent with our main analysis. SMI was associated with slightly lower rates of PSA screening in men aged 60–69 years (IRR = 0.78) than those aged 50–59 years (IRR = 0.84), although rates in both groups were still statistically significantly lower than in those from the general population (Supplementary Table 5). Adjusting for GP visits did not have an effect on the association between SMI and PSA testing in either age group. With respect to FOBT, rates were only statistically significantly higher in those with SMI among those aged 50–59 years (IRR = 1.20, 95% CI = [1.13, 1.28] compared with IRR = 1.06, 95% CI = [0.99, 1.13] for those aged 60–69 years, Supplementary Table 5). When we adjusted for GP visits, results for both age groups were consistent with our main analysis.
People with SMI were more likely to have one or two sample FOBT tests (rather than three) compared to people without SMI. However, there was not a significant difference in screening rates for FOBT screens with three samples taken, which was also the most commonly performed procedure (Supplementary Table 4).
Finally, other sensitivity analyses extending person years to 2 and 3 years from the first and last MBS date, to treat lithium-only users as exposed from 2012 onwards, to include lithium-only users as exposed for the whole study period, and to exclude lithium-only users entirely did not materially alter the results (see Supplementary Tables 6 and 7). Across the three cohorts, 65–75% of identified lithium users were also prescribed another SMI-defining medication.
Discussion
Main findings
These results from a large, national longitudinal study showed that people with a SMI had significantly lower rates of pap smears and PSA testing. Overall, we did not see lower rates of FOBT, although rates were significantly lower among those with SMI who visited a GP on average less than five times per year.
Context and implications
Our results indicate that cervical and prostate cancer screening rates in people with SMI are lower than those from the general population, as has been suggested by some but not all of the smaller studies in less representative populations (Happell et al., 2012; Howard et al., 2010). The findings are also similar to those of a cohort study of pap smears in women with schizophrenia that was restricted to one Canadian province (Martens et al., 2009). Our results may partly explain why the cancer mortality to incidence ratio in these cancers is higher for people with SMI compared to the general population (Kisely et al., 2008) and that those with SMI are more likely to have metastases at presentation than those without SMI (Kisely et al., 2013). Even in the case of PSA testing where the value of screening is contested (Catalona, 2018), reduced uptake in people with SMI may serve as a marker of their access to preventive care in general. People with SMI may have a number of comorbidities or competing needs, and medical practitioners may therefore be less likely to consider preventive screening during consultations. There also may be cognitive and behavioural challenges with patients with SMI making it more difficult to gather medical histories and make treatment plans (Druss et al., 2002). In addition, clinicians may attribute emerging somatic symptoms to the underlying psychiatric disorder resulting in missed diagnoses, sometimes termed ‘diagnostic overshadowing’(Pelletier et al., 2015). It is also possible that people with SMI are treated differently by medical professionals with negative attitudes towards SMI patients leading to disparities in care (Walker et al., 2015).
By contrast, FOBT rates were only lower in people with SMI compared to people without SMI among those who visited GPs less than five times per year. These findings are similar to a study restricted to US veterans that found that frequency of GP contact had an effect on colorectal cancer screening rates (Kodl et al., 2010). Poor access to health care may therefore have a greater impact on cancer prevention for people with SMI than the general population. The higher rates of FOBTs for people with SMI who visited doctors more frequently may also reflect the use of FOBT as a diagnostic tool, rather than screening test. GPs may opt for less invasive approaches to colorectal symptoms because of potential concerns that somatic symptoms reported by people with SMI might actually be a manifestation of their disease (psychosis), as well as the greater challenges of facilitating colonoscopy in those with SMI. We found some evidence of this in that those with SMI had higher rates (compared to those without SMI) of one or two FOBTs in an episode rather than the three recommended for screening. We did not have information on colonoscopy rates after FOBT but FOBT will not lead to a reduction in colorectal cancer mortality if not followed up with further diagnostic testing and treatment (Liss et al., 2016). This needs investigation in future studies.
Strengths and limitations
Our study had a number of limitations. We used medication to define SMI rather than medical records. While this may have created some misclassification of SMI status, it allowed us to investigate screening in a very large nation-wide population. Importantly, the PBS item codes we used to define our exposed population are largely restricted to SMI. The one exception is risperidone, which is also indicated for behavioural disturbance in people with dementia or autism. However, these disorders are uncommon in the age groups included in our study (AIHW, 2017; Anstey et al., 2010). We were also unable to capture first-generation antipsychotics, so there is the potential that our control group included people with SMI taking first-generation antipsychotics only, thus making our estimates more conservative. However, clinical practice guidelines in Australia advise the use of second-generation antipsychotics in the first instance (Galletly et al., 2016), and the use of first-generation antipsychotics (for any indication) is decreasing, with a reduction from 39% to 23% of all antipsychotics prescribed in the period covered by the study (Hollingworth et al., 2010). Lithium use was also inconsistently recorded in the PBS before 2012, but our sensitivity analyses exploring this issue were not materially different from the main findings suggesting the effect was minimal. We were unable to adjust for sociodemographic measures other than age, gender and state of residence. Given that people with SMI are a generally disadvantaged group (Lawrence et al., 2013), other socioeconomic factors could have been mediators on the pathway between SMI and cancer screening. Finally, we did not have data on FOBT performed as part of the NBCSP. Nevertheless, we saw an increase in FOBTs performed after the commencement of NBCSP in 2006, and this may be due to an increase in testing for age groups not covered in the staggered roll out of the NBCSP, as well as additional guidance for GPs recommending FOBT screening during this time (Foreman, 2009). It is unknown whether FOBT rates through the NBCSP would be similar between those with and without SMI, although studies have found that other disadvantaged groups are less likely to participate in NBCSPs (He et al., 2017).
This study has a number of strengths. It is the first nation-wide large-scale cohort study of cancer screening for people with SMI and had a follow-up of 11 years. The 2% prevalence of SMI is in keeping with rates reported in the World Health Organization (WHO) 10-country study (Jablensky et al., 1992). Use of linked administrative health records reduced the very real potential for selection bias that can occur when conducting research with people with SMI and allowed for accurate capture of screening tests performed. This study also provided cancer screening rates for a cohort with access to a universal health care system.
Future directions
Our results suggest that differences in screening frequency may explain some of the mismatch in cancer incidence and mortality in people with SMI. Further research is required to investigate potential variation in other aspects of cancer care including screening for other cancers and treatment pathways, but our results strongly indicate that action is required to improve preventive screening in this very disadvantaged group.
Supplemental Material
Supplementary_Tables – Supplemental material for Colorectal, cervical and prostate cancer screening in Australians with severe mental illness: Retrospective nation-wide cohort study
Supplemental material, Supplementary_Tables for Colorectal, cervical and prostate cancer screening in Australians with severe mental illness: Retrospective nation-wide cohort study by Karen M Tuesley, Susan J Jordan, Dan J Siskind, Bradley J Kendall and Steve Kisely in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
D.J.S., B.J.K. and S.K. conceived the study. S.J.J. and S.K. obtained funding for the study. All authors contributed to the analysis plan. K.M.T. conducted the data analysis and wrote the first draft of the paper. All authors contributed to subsequent revision and drafting of the final manuscript. K.M.T. is the guarantor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a QIMR Berghofer Medical Research Institute internal grant.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.