
Abstract
Spinal cord injury (SCI) brings sweeping changes to life. SCI is associated with increased mental health problems, which predict poorer outcomes such as increased pain, medical complications and substance abuse [1–7].
In spite of often small sample sizes and methodological differences, contemporary studies of the acute stage of SCI (hospitalization and early rehabilitation phase) find that around one-third of patients suffer significant symptoms of depression [8–10]. There is less agreement regarding the prevalence of depression in the longer term, after injury. For example, the prevalence of depression within the first 6 years since injury was 28.9% (6.5% with major depression) in a Canadian cohort (n = 201) [11]. In contrast, 11.4% of a larger US cohort (n = 849) met the criteria for major depression at their first year follow-up assessment [12]. Another US study found the prevalence of probable depression was 28% at time 1 and 21.5% the following year [13]. For all the participants (n = 163) the time since injury was more than 2 years (mean = 4.6 years; SD = 1.3 years) at the first measurement time point. In a large robust US study of 1391 individuals averaging 9.7 years since injury (range = 1–50 years), 48% reported clinically significant symptoms of depression, with half of those (24% of the total sample) suffering a probable major depression [14]. In contrast, a small Australian study found that the level of depressive symptoms in 60 individuals who were injured 11 years previously on average (range = 5–33 years) indicated that they were as psychologically well-adjusted as non-disabled groups [15].
There have been few studies of anxiety after SCI. A small Australian study (1 year after SCI, n = 41; 2 years after SCI, n = 31) found that depression and/or anxiety was suffered by 30% of individuals with SCI and this prevalence persisted over the first 2 years since injury [16]. In contrast, a small UK study with a variable participation rate (n = 104) found that the prevalence of anxiety fluctuated across the first 3 years after injury: the highest prevalence (60% of n = 5) was at week 48 after injury, the lowest prevalence (10% of n = 40) was at 6 months after discharge, and the prevalence at 2 years after discharge was 16% (n = 36) [8]. An Italian study (n = 100) found that symptoms of anxiety and depression were 13% and 16%, respectively, within a cohort in which time since injury ranged from 3 months to 28 years (mean = 4.6 years) [7].
Despite the sudden and traumatic nature of SCI, the phenomenology of post-traumatic stress disorder (PTSD) and SCI has been less well studied. Twelve per cent of a cohort of 125 US veterans who averaged 19 years since injury met the diagnostic criteria for current PTSD [17–19]. In a small UK study (n = 85) of civilians with SCI who were ≤6 months since SCI, 14% scored within the clinically significant range of intrusion and avoidance symptoms [20]. In contrast, a small Danish study (n = 69) found that 20% of individuals who were all less than 1 year since SCI suffered from PTSD [21].
A consistent finding of most studies of psychopathology and SCI is that the level of SCI is not related to mental health outcomes. There were two exceptions: individuals whose SCI had resolved had significantly better mental health outcomes compared to individuals with persisting SCI [11]; and veterans who sustained a high-level SCI (tetraplegia/quadriplegia) had a lower likelihood of current PTSD [17], [18].
There is a lack of large-scale studies of the long-term mental health of individuals with SCI living in the Australian community. The aim of the present study was to investigate the mental health and phenomenology of emotional disorders in Australians with SCI living in the community.
Method
Procedures
Data were collected in 2004–2005. The participants were aged ≥18 years, with a history of sudden-onset SCI and living independently in the community. They were ≥6 months since injury and on the registry of the only hospital in Victoria that treats patients with traumatic SCI. Individuals on the registry (n = 929) were initially mailed an invitation to complete the survey by either the internet or telephone or by mail. A hard copy of the survey questionnaire was sent approximately 4 weeks later to anyone who had not responded. Finally a follow-up telephone call to non-responders was used approximately 4 weeks later. Excluding those who had died, were untraceable, had insufficient English-language skills, or had serious mental illness (such as dementia or schizophrenia) that impaired their ability to complete the survey, there was an overall 44% response rate.
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. The research project was approved by Monash University, Austin Health and Bayside Health Ethics Committees. Each subject gave informed consent. The surveys were strictly confidential but not anonymous. Each subject whose survey results indicated they were likely suffering emotional distress, were approached and offered referral for psychological care.
Individuals who completed the survey did not differ significantly from non-responders, in current age or gender distribution (current age t = 1.546, (df = 927), p = 0.12; gender χ2 with Yates continuity r = 1.812, (df = 1), p = 0.18). No other demographic information was available from the registry list.
Additionally, further participants with sudden-onset SCI of a non-traumatic cause, such as an infection, who were not on the State SCI register were recruited through the outpatient clinic at the only other SCI unit in Victoria, specializing in non-traumatic SCI (n = 32). Overall, 14% (n = 62) of the cohort had non-traumatic SCI.
Measures
The reliable and valid self-report short form of the Depression, Anxiety and Stress Scale (DASS-21) was used to discriminate between symptoms of depression, anxiety and clinical level of stress using the scoring system and cut-offs published in the manual [22]. Each subscale (depression, anxiety and stress) consists of seven questions, has a clinical cut-off score and four levels of symptoms severity (mild moderate, severe, and extremely severe). Respondents are asked to indicate on a 0–3 scale how much each statement has applied to them over the previous week.
Normative DASS-21 data were available from a study of a large adult non-clinical UK population (n = 1794; 815 male) with a mean age of 41.0 years (SD = 15.9 years, range = 18–91 years) [23]. Participants were unpaid volunteers recruited from a wide variety of sources including commercial and public service organizations [23].
The Impact of Events Scale–Revised (IES-R) [24] is a reliable and valid self-report measure of symptoms of PTSD with a cut-off score that indicates a likely diagnosis of PTSD [25].
The DASS, DASS-21, IES and IES-R have been successfully used within general populations [23], [26], clinical populations with psychological disorders [25], [27], populations with significant physical illnesses [28], [29] and populations with physical disabilities including SCI [18], [30]. The terms ‘Depression’, ‘Anxiety’, ‘Stress’ and ‘PTSD’ will be used to indicate that the individual with SCI had a score on the relevant scale that was above the published clinical cut-off. These terms are not synonymous with a clinical diagnosis but indicate a likelihood of such a diagnosis.
Health consisted of a 1–10 score where higher scores indicated better health and was derived from two questions. One question asked about the frequency of visits to the doctors over the previous 3 months. The other question asked for the names of medications taken daily. Each question was scored on 1–5 scale and then summed.
Results
Participants
A total of 443 adults with SCI participated in the study. Seventy-eight per cent were male; 30.9% had incomplete paraplegia, 30.7% had complete paraplegia, 25.3% had incomplete quadriplegia and 10.2% had complete quadriplegia. The average age of participants in 2004–2005 was 51.78 years (SD = 14.44 years, range = 18–86 years). The average time since injury was 19.2 years (SD = 13.27 years, range = 1–66 years). The majority of participants were married (58.8%) and had completed ≤12 years of education (57.9%).
The Cronbach alpha coefficient for the overall DASS-21 scale was 0.927; alpha coefficient for the subscale domain Depression was 0.902, for Anxiety, 0.748, and for Stress, 0.864. The Cronbach alpha coefficient for the overall IES-R scale was 0.944; alpha coefficient for the subscale domain Intrusion was 0.894, for Avoidance, 0.873, and for Hypervigilance, 0.823.
Prevalence of emotional disorders
Approximately half (51.5% or n = 222) of the cohort scored within the normal non-clinical range for Depression, Anxiety, Stress and PTSD. But 37% suffered from depression, 30% suffered anxiety, 25% suffered clinically significant stress and 8.4% (n = 37) suffered from PTSD.
The distribution of age in the normative data [23] was similar to that of the cohort but the proportion of female subjects was higher in the normative data (54%) compared to the present cohort (22%).
In comparison to the normative sample, the odds ratio (OR) for any Depression was OR = 2.09 (95%CI = 1.67–2.62). The OR for Anxiety was OR = 2.19 (95%CI = 1.72–2.79). The OR for Stress was OR = 1.35 (95%CI = 1.057–1.72). The risk was consistent across the levels of severity of psychopathology as indicated by the DASS-21 subcategories of mild, moderate, severe and extremely severe. In comparison to the normative sample, the likelihood of experiencing any emotional disorder whether that was Depression, Anxiety or Stress was OR = 1.81 (95%CI = 1.46–2.23).
The risk of experiencing Depression, Anxiety or Stress did not significantly differ according to gender within the cohort. The OR of female subjects with SCI experiencing Depression over male subjects with SCI was OR = 1.55 (95%CI = 0.98–2.44), for Anxiety it was OR = 1.44 (95%CI = 0.90–2.33) and for Stress it was OR = 1.19 (95%CI = 0.72–1.98).
When compared with the normative data, the risk of experiencing Depression did significantly vary by gender: the odds of Depression for female subject with SCI was OR = 2.74 (95%CI = 1.79–4.19) and for male subjects with SCI it was OR = 2.09 (95%CI = 1.58–2.77). The increased risk of Anxiety compared with the normative sample also varied with gender: the odds of Anxiety for female subjects with SCI was OR = 2.43 (95%CI = 1.56–3.79) and for male subjects with SCI it was OR = 2.59 (95%CI = 1.90–3.53). The risk of experiencing Stress was not significantly different to the normative sample for female subjects with SCI but just reached significance for male subjects: the odds of Stress for female subjects with SCI was OR = 1.43 (95%CI = 0.89–2.29) and for male subjects with SCI it was OR = 1.44 (95%CI = 1.06–1.95).
Comorbidity of emotional disorders
Around 60% of those with one probable diagnosis were also likely to suffer at least one other disorder, indicating a substantial comorbidity of psychopathology (Table 1).
Comorbidity of depression, anxiety and clinically significant stress
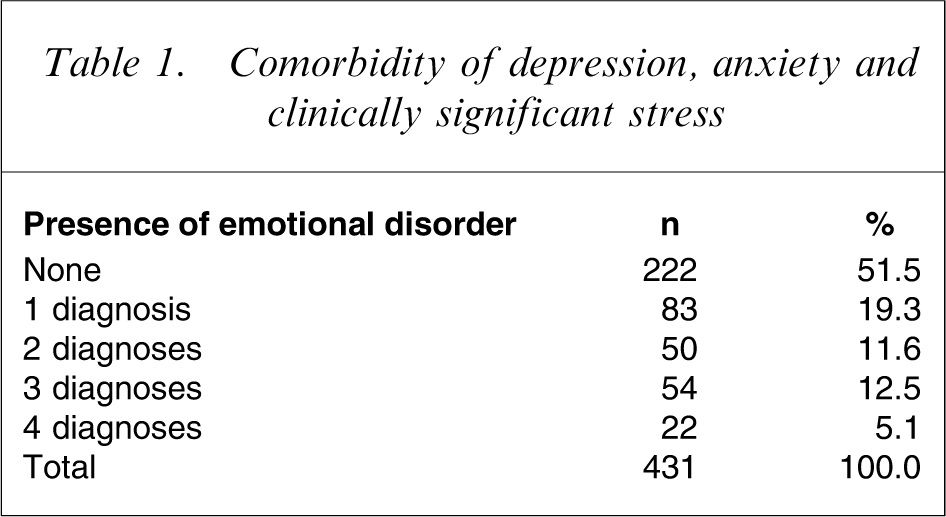
Comparing this cohort with normative data for the DASS-21, the OR of comorbidity of Depression, Anxiety and/or Stress was OR = 1.56 (95%CI = 1.13–2.15), representing a 56% increase in the likelihood of comorbidity over the non-SCI population.
Individuals with PTSD were highly likely to suffer Depression, Anxiety and Stress. Scores of the IES-R (total scores) when compared with scores from the DASS-21 were significantly correlated (p = 0.01 level, two-tailed): IES-R/Depression r = 0.577; IES-R/Anxiety r = 0.559; and IES-R/Stress r = 0.577. Eighty-six per cent of those with PTSD also scored within the clinical range of Depression, 78% within the clinical range of Anxiety and 78.4% within the clinical range of Stress. To express this in another way: if a probable case of PTSD was indicated then the odds of Depression also being present was OR = 12.98 (95%CI = 4.93–34.15), the odds of Anxiety being present was OR = 9.96 (95%CI = 4.40–22.55), and the odds of Stress being present was OR = 14.15 (95%CI = 6.23–32.10).
Associations with psychopathology
A logistic regression with ‘presence of psychopathology’ as the dependent variable found that only three variables were associated with the outcome (Table 2). They were time since injury, health and level of injury. Both time since injury and health had a negative association with psychopathology. Each year since injury decreased the likelihood of psychopathology by 2.6% (OR = 0.975, 95%CI = 0.956–0.994) and each unit increase in health decreased the likelihood of psychopathology by 30% (OR = 0.768, 95%CI = −.687–0.858). Further examination of the level of injury variable showed that it was only the discrete dummy category of Complete Quadriplegia that was substantially less likely to coexist with the presence of psychopathology. Those with complete quadriplegia were more than threefold less likely to be experiencing psychopathology compared to the other levels of SCI OR = 0.323, 95%CI = 0.139–0.753). Pseudo R2 statistics indicate that the independent variables accounted for only a modest portion (13–17%) of the variance in the outcome (Cox & Snell R2=0.127, Nagelkerke R2=0.170).
Logistic regression with the presence of psychopathology outcome (n = 413)
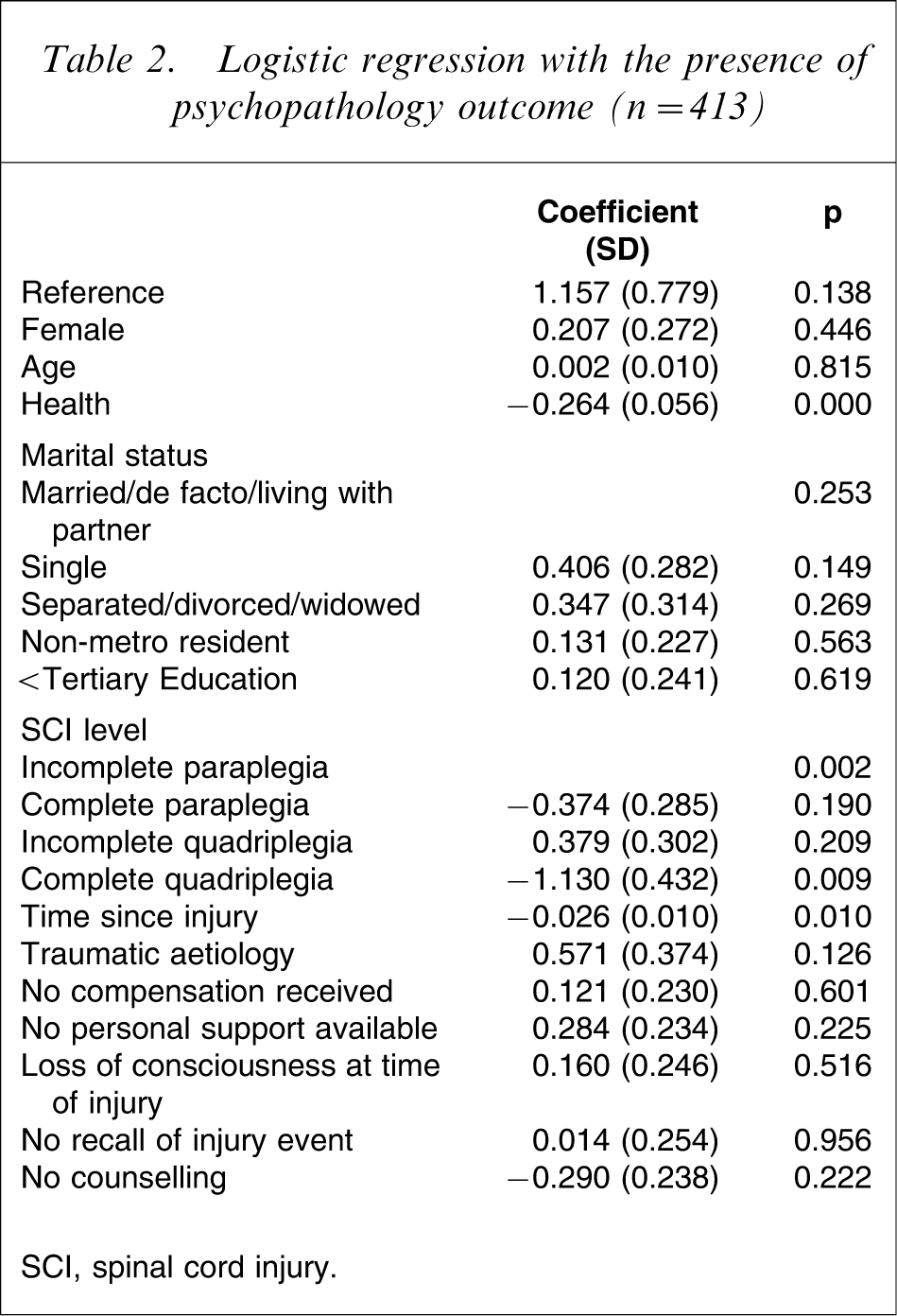
SCI, spinal cord injury.
Discussion
This large-scale study of an Australian community population of people with SCI found that 37% suffer from depression. This relatively high level of depressive symptoms is similar to that reported in a large overseas study [14]. The prevalence of anxiety (30%) was in accord with a previous small Australian study [16] but higher than other small overseas studies of community-dwelling adults with SCI [7], [8]. The 8.4% prevalence of PTSD was less than that in previous overseas studies of adults with SCI (12–14%) but not substantially so [19], [20]. PTSD has not been studied in an Australian population with SCI previously. The prevalence of PTSD is higher than that found in the general Australian population (12 month prevalence = 1.33%) [31] but is consistent with a previous Australian study of non-SCI individuals who had experienced a significant physical trauma (10% prevalence) [32].
Clinically significant stress has not been used as a mental health outcome in any previous population study of individuals with SCI. It must be emphasized that this measure represents a tension–stress syndrome that is more than the tension or stress felt by most during taxing times of life. Nor is it simply a range of non-specific symptoms related to depression or anxiety but is a construct distinct from depression and anxiety [33]. The correlations of stress with depression and anxiety in the present study (Spearman's ρ with depression rs=0.656, p = 0.000, n = 435; and anxiety rs=0.611, p = 0.000, n = 436) are high but do not account for all the variance, thus supporting it as a separate aspect of psychopathology.
Three variables significantly impacted on the likelihood of psychopathology: health, level of injury, and time since injury. Each improvement in health decreased the likelihood of the presence of psychopathology by 30%. Each year since injury decreased the likelihood of the presence of psychopathology to the order of 2.6%. And those with complete quadriplegia were more than threefold as likely to not suffer psychopathology compared with any other level of injury. The latter might seem counterintuitive. The most likely explanation for these findings became apparent when exploring the cohort demographics in more detail. The cohort may be a large sample but the distribution according to the level of injury and time since injury was not equal. This is to be expected because SCI aetiologies are not an equally distributed phenomenon. Those with incomplete injuries were injured significantly more recently compared to those with complete injuries (F(3, 437) = 0.6.551, p = 0.000). What is more, individuals with a high-level complete quadriplegia are more likely to reside in supported accommodation compared to other levels of SCI and were therefore not included in the present study of adults with SCI living independently in the community. Those with complete quadriplegia formed the smallest subgroup (n = 45 or 10%). A large proportion of those with complete quadriplegia were injured many years ago; 45% (n = 20) were injured ≥20 years ago and 27% (n = 12) were injured ≥30 years ago. But those with complete paraplegia had the highest mean time since injury compared to the other levels (complete paraglegia mean = 23.02 years, SD = 13.21; incomplete paralegia mean = 16.89 years, SD = 14.03 years; complete quadriplegia mean = 20.58 years, SD = 11.77 years; incomplete quadriplegia mean = 17.14 years, SD = 11.86 years). Therefore the finding of relative mental health in those with complete quadriplegia and for the longest survivors is a systemic sample bias probably created by a healthy survivor effect. Although there was a small to medium effect size (η2=0.04) of injury level on time since injury, the overall impact of those variables on the likelihood of psychopathology was small. All the independent variables in the logistic regression model accounted for only 13–17% of the variance.
The present study found that many with SCI were remarkably resilient but there remained around 50% who suffered from emotional disorders, 60% of whom suffered two or more emotional disorders. This is a substantial 56% increase in the likelihood of comorbidity in emotional disorders over the general population. The likelihood of comorbid emotional disorders has a number of consequences. It means that any emotional disorder associated with SCI is likely to be more complex to treat. Much of the previous research into the emotional consequences of SCI focused on either depression or depression and anxiety [7], [8], [11–14], [24]. Treatments that focus on only one aspect of the profile of psychopathology suffered by a person with SCI, such as depression, are less likely to be effective.
Study limitations
A post-hoc examination for the potential confound introduced by the physical sequelae of SCI with the physical symptoms diagnostic of psychological disorders was conducted. The anxiety subscale was chosen because this scale included the highest number of items relating to physical symptoms (three autonomic arousal items out of a total of seven items). The sample was divided into anxious and non-anxious groups based on scores that passed the published threshold. Participants in both the anxious and non-anxious group responded to the autonomic and non-autonomic items, but the anxious group responded more positively to the non-autonomic items while the non-anxious group responded more positively to the autonomic items (Table 3). The results indicated that, rather than confounding the results, the autonomic items played a legitimate role indicating the presence of anxiety. This is congruent to previous research [12].
Correlations of autonomic and non-autonomic items of anxiety subscale
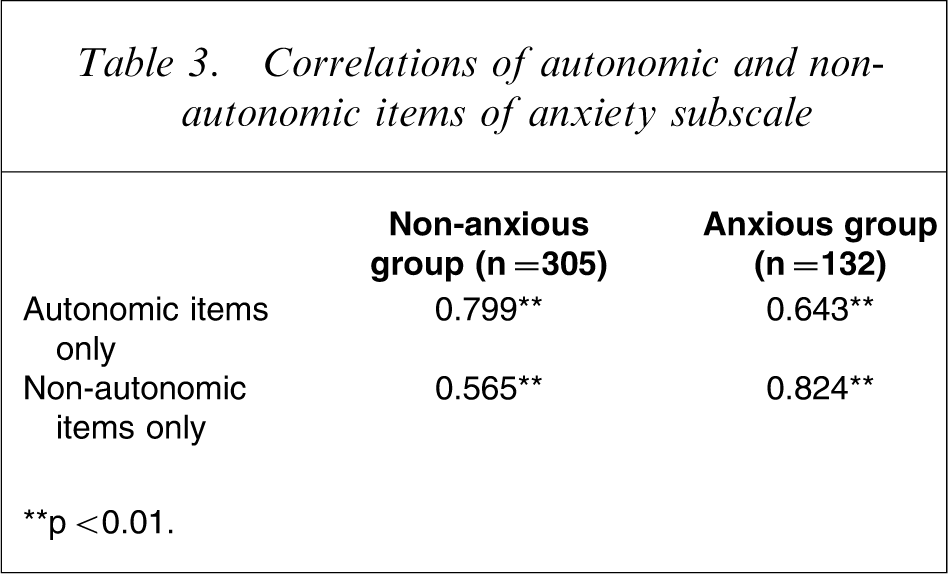
∗∗p < 0.01.
The measures of psychopathology were self-report scales and did not include a diagnosis confirmed by clinical interview, but the scales used had demonstrated good predictive and discriminatory validity in normative and clinical populations as well as in populations with disabilities. On the whole, the representativeness and size of the sample should enhance the generalizability of the findings for Australian people with SCI who live in the community.
Clinical implications
Although the number of people in Australia with SCI is relatively small (estimate 2007 n = 10 000) [34] the suffering and the burden from clinical levels of depression, anxiety, stress and PTSD is high, affecting around 50% of this group. Given that 60% of the sample could not recall receiving any specific treatment for their mental health problems there is a need for better mental health assessment and treatment services that recognize the problems of mobility, access and stigma faced by those with SCI.
Footnotes
Acknowledgements
The Monash University Postgraduate Publications Award and the Robert Rose Foundation PhD Scholarship (Migliorini), the provision of the normative data by J. Henry, University of NSW Australia and J. Crawford, Kings College, University of Aberdeen UK, and support by Assoc Professor D. Brown, Austin Hospital and Dr. P. New, Caulfield General Medical Centre.