
Abstract
Medical internship has been traditionally regarded as an initiation step into a challenging medical career as well as a trial of spirit and stamina [1]. During internship, many issues can challenge the adaptive capacity of trainees. Tremendous changes in this period include relocation away from support system, also sleep deprivation, demands of patient care, financial problems, and reduced time with family [2]. In addition, it has been known that burnout, which is characterized by a severe stress reaction, and increased psychiatric morbidity including anxiety, depression, anger, hostility, substance abuse, and suicide were common during internship [2–6].
Of various psychopathologies, it has been noted that the proportion of subjects with depression was higher than that found in the community and that newer onset of depression was much increased during internship [4], [5]. Depression is closely associated with burnout and the percentage of shared variance is between depression and burnout 20% [7]. In addition, in a prior study with a community sample, it has been suggested that subjects with depression had poor quality of life [8]. Because of adverse psychosocial outcomes of depression as well as the higher proportion of newer onset depression in interns, depression during internship has been the focus of considerable study. In previous studies, higher prevalence of depression during internship has been associated with a number of factors including a stressful work environment, long work hours, conflict between work and personal life tasks, and individual psychological vulnerability [4], [9]. But although depression is prevalent even in the medical school period [10], few data have been collected with respect to the relationship between depression before internship and its subsequent influence during internship, specifically how lifetime depression before internship affects psychopathology and quality of life. In addition, to the best of our knowledge, there has been no report regarding the degree of depression that could cause adverse psychosocial consequences during internship.
A milder form of depression or subthreshold depression, which is significant depressive symptomatology that does not meet diagnostic criteria for major depression, is a highly prevalent condition and has been associated with more disability and work days lost, greater use of services and medical care costs, poorer quality of life, and more lifetime suicide attempts, compared with no depressive symptoms [8], [11–13]. A few categories in the current DSM-IV categories have been proposed to cover those who have subthreshold depression, including dysthymic disorder and minor depression [14]. Subjects with subthreshold depression had an increased risk for developing severe forms of depressive disorders [15], [16]. In addition, the functional impairment of subthreshold depression in some cases might equal that seen in major depression [15]. Thus, it could be suggested that even subthreshold, lifetime depression before internship may have influences on the life of interns. In addition, it seems reasonable that higher prevalence of depression during internship would be partly explained by their lifetime subthreshold depression before internship [10].
Quality of life refers to a subjective evaluation, which is embedded in a cultural, social, and environmental context. The World Health Organization (WHO) has defined quality of life as an individual's perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns [16]. Because of its multi-dimensional nature, it cannot be equated simply with the terms ‘health status’, ‘life style’, ‘life satisfaction’, ‘mental state’ or ‘well-being’. Until now, although much was known about workload, physical strain, and financial burdens of interns [17–19], little was known about quality of life during internship. Moreover, factors (i.e. depression) that can influence various domains of quality of life have not been explored in this population.
The aim of the present study was to investigate the influences of lifetime subthreshold depression and major depression on the changes in psychopathology and subjective quality of life during internship. Based on prior reports on relevant topics [2–6], we hypothesized that changes in psychopathology (hypothesis 1), specifically anxiety, depression, and hostility, and in major domains of quality of life (hypothesis 2) in interns with lifetime subthreshold depression and interns with major depression would be different from those without lifetime depression.
Methods
Procedure
All instruments used in the current study were administered to the interns, who were told that participation in the current study was voluntary and that only group data would be reported. The study protocol was reviewed and approved by the ethics committee of the department of psychiatry and relevant committee in the department of education and research office at Seoul National University Hospital.
Participants
A total of 229 interns at Seoul National University Hospital were enrolled in the study at orientation session. Participants were asked to complete questionnaires twice, at an interval of 6 months. Time 1 was February 2006 (intern orientation) and time 2 was August 2006 (midterm education session). At time 1 (February 2006), the participants consisted of 220 (95.6%, 114 men and 106 women) of 229 eligible interns. The major depression category in Korean version of Mini International Neuropsychiatric Interview (MINI) [20], [21], Modified Form for Self-administration [22] was administered in order to divide subjects into three lifetime diagnosis groups: interns without lifetime depression; interns with lifetime subthreshold depression; and interns with lifetime major depression. Subjects with lifetime subthreshold depression were defined as those who had minor depression in DSM-IV research criteria or dysthymia in DSM-IV according to the Korean version of MINI, Modified Form for Self-Administration. In addition, all participants were asked to complete the Korean version of the Beck Depression Inventory (BDI) [23], [24], Symptom Checklist-90-Revised (SCL-90-R) [25], [26], and WHO Quality of Life Assessment Instrument, Brief Version (WHOQOL-BREF) [27], [28].
At time 2 (August 2006), 151 (65.9%, 79 men and 72 women) of 229 eligible interns also participated and completed BDI, SCL-90-R, and WHOQOL-BREF. There were no significant differences in demographic variables including age (independent sample t-test; t = −0.66, df = 218, p = 0.511), sex (χ2 test; df = 1, p = 0.937), socioeconomic status (χ2 test; df = 1, p = 0.403), or prior education level (χ2 test; df = 2, p = 0.790) as well as diagnostic distribution (χ2 test; df = 2, p = 0.898) between participants and excluded subjects. In addition, we found no significant between-group differences in baseline score of BDI, SCL-90-R, or WHOQOL-BREF. Finally, information on the remaining 151 interns was used for statistical analysis.
Measures
Mini International Neuropsychiatric Interview, Modified Form for Self-Administration
The MINI is a validated and reliable diagnostic structured interview, covering 17 axis I disorders based on DSM-IV criteria [20], [21]. In order to detect lifetime diagnosis of major and subthreshold depression among interns, we used the major depression category in the Korean version of the MINI, Modified Form for Self-administration [22]. Reliability and validity of the major depression category in Korean version of the MINI, Modified Form for Self-Administration were successfully tested in a recent study using a sample of 906 non-clinical subjects in Korea [22].
Beck depression inventory
The BDI is a standardized instrument that has been frequently used to evaluate numerous signs and symptoms of depression [23], [24]. The BDI has 21 items scored on a 4-point Likert scale, from 0 to 3. The Korean version of the BDI also had high reliability and validity measures [24].
Symptom checklist-90-revised
The SCL-90-R, a 90-item multidimensional questionnaire [25], [26], was used for detecting a broad range of psychopathology among interns. Each item is rated on a 5-point Likert scale. The instrument is a self-report clinical rating scale that measures subjective symptoms on nine primary symptom dimensions including Somatization, Obsessive–Compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism. In addition, three global indices provide measures of overall psychological distress: the Global Severity Index, the Positive Symptom Total, and the Positive Symptom Distress Index. For both nine primary symptom dimensions and three global indices, standard T score is calculated by converting the score according to Korean normative data [26]. SCL-90-R has been widely used as a valid and reliable tool for detection of changes after treatment as well as for measurement of overall psychopathology across cultures and ethnic groups [29].
World Health Organization quality of life assessment instrument, brief version
The WHOQOL-BREF, a 28-item self-report questionnaire [27], [28], was used in the current study to assess subject quality of life in interns. Each item has a 5-point Likert scale. All domain scores are scaled in a positive direction (i.e. higher scores denote higher quality of life) and presented as a 0–100 scale. This scale assesses perceived subject quality of life across four particular domains including Physical Health, Psychological Health, Social Relationships, and Environment. There are also two separate items that are composed of questions about an individual's overall perception of quality of life and their own health, respectively. Korean version of WHOQOL-BREF has shown high reliability and validity measures [28].
Data analysis
Differences between 151 participants and 69 excluded subjects were tested using a independent sample t-test for continuous variables and a χ2 test for categorical variables. In addition, differences in baseline demographic variables among the three groups were tested using a one-way analysis of variance (ANOVA) with post-hoc Scheffe test for continuous variables and a χ2 test for categorical variables. Changes in depressive symptoms, overall psychological problems, and quality of life across three groups were assessed using mixed ANOVAs with post-hoc Scheffe test, considering each domain score of the WHOQOL-BREF, each item score of the SCL-90-R, and total scores of BDI as dependent variables, and diagnostic group and time as independent variables. All statistical analyses were two-tailed and conducted using the Windows version of SPSS 11.0 (SPSS, Chicago, IL, USA). p < 0.05 was considered to be statstically significant.
Results
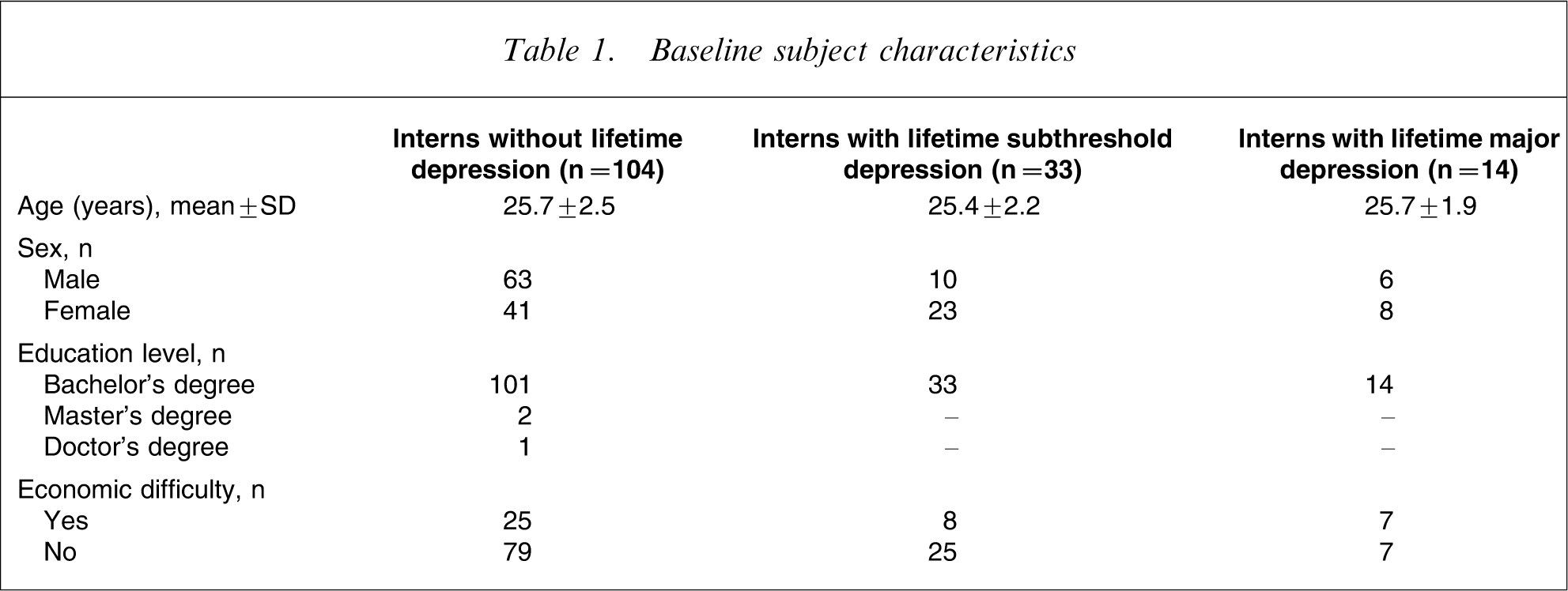
The baseline demographics are summarized in Table 1. A total of 151 participants completed questionnaires twice at an interval of 6 months. They were divided into 104 interns without lifetime depression (63 men, 41 women), 33 interns with lifetime subthreshold depression (10 men, 23 women; 30 subjects with lifetime minor depression and three with lifetime dysthymia), and 14 interns with lifetime major depression (six men, eight women; three subjects also had lifetime dysthymia). While other significant differences could not be found in terms of age, socioeconomic status, and prior education level, there was significant difference in sex distribution (χ2 test; df = 2, p = 0.006) among the three groups.
Baseline subject characteristics
Significant changes over time were detected in the primary symptom dimensions in SCL-90-R including Somatization (F1,147=7.17, p = 0.008), Depression (F1,147=4.73, p = 0.031), Anxiety (F1,147=6.06, p = 0.015), and Phobic Anxiety (F1,147=4.68, p = 0.032) as well as in all total scores of the BDI (F1,147=28.01, p < 0.001). In contrast, significant differences were found among the three groups at time 1 and time 2 for all independent variables, except the Somatization dimension, on the SCL-90-R (F2,148=2.39, p = 0.095). Post-hoc comparisons using the Scheffe test indicated that changes of psychopathology in interns without lifetime depression differed significantly from that in interns with lifetime subthreshold depression and interns with lifetime major depression, but no differences were found between the two depression groups. Significant group×time interaction was observed only for the Obsessive–Compulsive dimension (F1,149=3.80, p = 0.025) in SCL-90-R (Table 2).
Score changes on the BDI and SCL-90-R
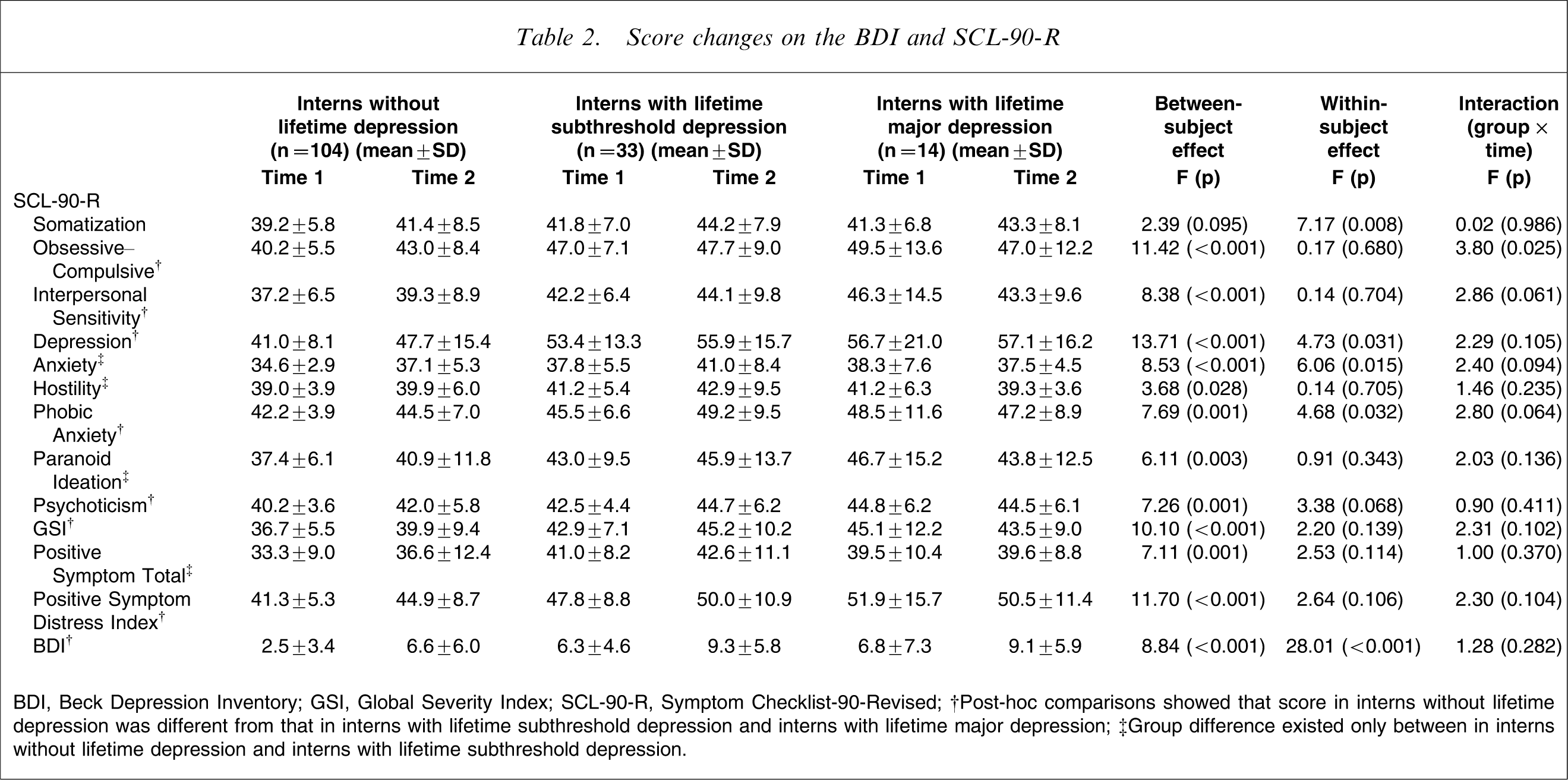
BDI, Beck Depression Inventory; GSI, Global Severity Index; SCL-90-R, Symptom Checklist-90-Revised.
†Post-hoc comparisons showed that score in interns without lifetime depression was different from that in interns with lifetime subthreshold depression and interns with lifetime major depression.
‡Group difference existed only between in interns without lifetime depression and interns with lifetime subthreshold depression.
Scores were significantly decreased at time 2 in all four domains of the WHOQOL-BREF including Physical Health (F1,147=38.31, p < 0.001), Psychological Health (F1,147=11.31, p = 0.001), Social Relationships (F1,147=10.39, p = 0.002), and Environment (F1,147=68.00, p < 0.001). In addition, significant group differences were found at time 1 and time 2 in Physical Health and Psychological Health domains on WHOQOL-BREF (F2,148=5.06, p = 0.008; F2,148=7.12, p = 0.001, respectively). Using post-hoc Scheffe test, significant differences were detected only between interns without lifetime depression and interns with lifetime subthreshold depression. There was no significant group×time interaction (Table 3).
Score Changes on the WHOQOL-BREF
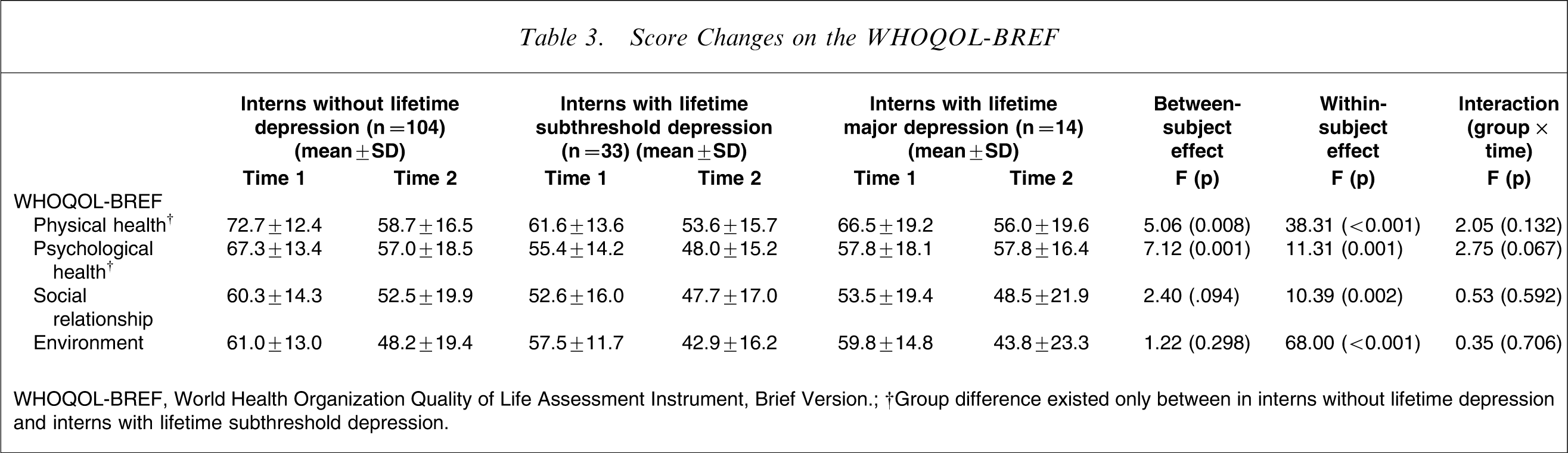
WHOQOL-BREF, World Health Organization Quality of Life Assessment Instrument, Brief Version.
†Group difference existed only between in interns without lifetime depression and interns with lifetime subthreshold depression.
Discussion
In the current study the influences of lifetime depression before internship on subsequent changes in psychopathology and subjective quality of life were investigated in a sample of interns in Korea. The present findings of increased psychopathology during internship, that is, somatization, anxiety, phobic anxiety, and depression, may concur with the results of the previous studies [4], [5], [30–32]. In previous studies, along with other psychopathology including higher anger–hostility, higher tension–anxiety, higher fatigue–inertia, and lower vigour–activity score on the Profile of Mood States (POMS) [30–32], it has been reported that depression affects approximately 30% of interns [5]. Using the Schedule for Affective Disorders and Schizophrenia-Research Diagnostic Criteria (RDC), Clark et al. reported that a newer-onset depressive episode had developed in 27% of the interns during the first 6 months of internship [4].
Until now, although a concurrent relationship between depression and decreased empathy, elevated level of burnout, and loss of idealism has been suggested [11], [33], [34], few data have been collected with respect to the influences of depression that occurred before internship, specifically how lifetime depression before internship affects overall psychopathology and quality of life during internship. In addition, there has been no report regarding the degree of depression that could cause adverse psychosocial consequences during internship. In the current study, interns with lifetime subthreshold depression and those with major depression exhibited higher psychopathology at both time 1 and time 2, while there were no differences between the two depression groups. Thus, in accord with the results of previous studies in a general population sample [15], the influences of subthreshold depression before internship on overall psychopathology seem to be equal to that seen in major depression. Furthermore, the current results suggest that interns with lifetime subthreshold depression have an additional morbidity including higher anxiety, hostility, and paranoid ideation on SCL-90-R, compared to interns without lifetime depression.
In the present study, scores were significantly decreased at time 2 in all four domains of the WHOQOL-BREF. In addition, group difference existed only between interns without lifetime depression and interns with lifetime subthreshold depression. The Psychological Health domain in WHOQOL-BREF incorporates those facets including body image and appearance, negative feelings, positive feelings, self-esteem, spirituality/religion/personal beliefs, and thinking [16], [27]. This domain also addresses questions on the meaning of life and how much people can enjoy their lives. The domain, Physical Health has questions about physical health, sleep, pain, and coping with everyday life: all related to somatic symptoms of depression [16], [27]. We suggest that interns with lifetime subthreshold depression may be susceptible to this challenging period in terms of physical and psychological quality of life. In addition, considering the high prevalence of subthreshold depression before internship and the psychopathology and poor quality of life associated with it, we suggest that the screening of lifetime depression even at the subthreshold level, and further intervention, should be done at the beginning of internship.
Limitations of the present study were as follows. First, because the diagnosis of depression was made on self-administered instrument, the risk of recall bias is high. In addition, although overall psychopathology was estimated on the SCL-90-R, other clinical diagnosis except depression could not be made, which hinders the exploration of the influence of other comorbid psychiatric conditions. Second, because scores in SCL-90-R, BDI, or WHOQOL-BREF may be relative, the interpretation of the current results should be done with caution. If a subject with a higher score on certain characteristics in these instruments is regarded as having a definite psychopathology, the risk for oversimplification of mental health status is inevitable. Third, because we recruited a small number of subjects from one training hospital, the present findings may not be replicated in future, larger-scale studies. Fourth, although it seems that once changed, psychopathology was stable in the course of internship [30–32], we explored changes only over a 6 month interval, which precludes the generalization of the findings over total intern years. Fifth, the dimensions of subjective quality of life resemble diagnostic criteria for depressive symptoms and impairments, which leads to the problem of a partial overlap between the constructs [33], [34]. And last, the present findings may not be easily generalizable to other sociocultural environments. The issue of psychosocial outcomes in subthreshold depression has not been delineated in a representative sample of the Korean population. Furthermore, although depression has been a major issue for medical training in Korea, because of the higher proportion of specialist among medical doctors (83% of total medical doctors) and the resulting long training period [35], this is the first study regarding mental health in Korean medical doctors. Although the overall psychosocial impact of subthreshold depression seems to be equal to that of major depression in the present study, it was suggested in another study using a general population sample that the effect size of subthreshold depression is small and less than major depression [8].
Better understanding of influences of lifetime depression on changes in mental health status may lead to earlier detection of subjective distress and potential psychosocial problems of at-risk subjects in training programmes. Careful regulation of duty hours, monitoring of mental health status, regular supervision of programme directors, and proper intervention may be essential throughout the intern year and, perhaps, beyond.
Footnotes
Acknowledgements
This research was supported by a grant from the Institute of Human Behavioural Medicine and the Department of the Education and Research Office in Seoul National University Hospital.