
Abstract
Studying the distribution of age of onset can provide important clues to the aetiology of disorders [1, 2] as well as guide service planning [3]. There is a sizeable literature describing the age of onset for schizophrenia, where earlier onset has been linked to males, as well as to other risk factors such as family history [4] and obstetric complications [5]. When one considers that affective psychosis has a similar prevalence to schizophrenia [6], and comparable disability burdens [7], it is surprising that we do not have a clearer picture of the factors that influence the onset of affective psychosis.
However, this lack of clarity may be related to certain characteristics of the disorder. For example, the cyclical nature of certain psychotic disorders can make it difficult to pinpoint onset (manic episodes may emerge after one or more admissions for depression). In addition, for those engaged in register-based research, there are particular concerns about how to interpret the ICD-9 classification of affective psychosis (296.x). Following the Kraepelinian orthodoxy, ICD-9 lumped together all severe affective disorder regardless of whether they were unipolar or bipolar. One particular subcategory of ICD-9 affective psychosis, 296.1 (‘manic-depressive psychosis, depressed type’), included coding synonyms such as ‘endogenous depression’, ‘involutional melancholia’, and ‘monopolar depression’, in addition to psychotic depression. As a consequence, individuals with nonpsychotic unipolar depression were often coded within the category affective psychosis whereas milder forms of depression were allocated to the ICD-9 category neurotic depression (300.4) where synonyms include ‘reactive depression’ and ‘anxiety depression’.
Thus, there are several potential explanations for the lack of consensus concerning the shape of the onset distribution and sex differences in affective psychosis [8]. Some studies have found a peak in early adult life which declines with age [9–15], while others report a peak in later decades of life [16–21]. Two of the larger studies also produced conflicting results. Eagles and Whalley [22] found linearly increasing rates with increasing age with no sex differences. In contrast, rates for women in Sibisi's [8] study rose to a plateau in years 20–50 and then dropped to a lower plateau, while males peaked in their 20s, stablizing from 30 years onwards until rising again in their 70s. A higher mean age for women has been found in bipolar disorder [19] and major affective disorder [10, 19, 23]. However, another study found women had their first affective or manic episode earlier than men [21]. Hendrick and colleagues [24] found no sex difference in a small study of DSM-IV bipolar. Interestingly, while there were no significant onset differences between bipolar men and women, Perris [25] found men had an earlier onset if their first episode was mania rather than depression, whereas women tended to have earlier episodes of depression.
While there is general consensus that major depression appears more common in women [18, 26, 27], liability to bipolar disorder seems similar in both sexes [8, 23]. However, averaging across the lifespan may cloud important differences in the distribution of onset between the sexes [8, 15, 28]. The shape of the onset distribution can provide important clues to the aetiology of a disorder (e.g. peaks around puberty and/or menopause may suggest a role for sex hormones).
We had the opportunity to examine age-of-onset distribution of ICD-9 affective psychosis in a large data-set, using age-at-first-registration as the proxy measure of onset. In order to examine possible heterogeneity in the ICD system, we compared the distributions of 296.1 versus the other 296 subcategories. In addition, we were interested in exploring possible sex differences in the age-of-first-registration for affective psychosis.
Method
For the period 1979–1991, data on age-at-first-registration for 4985 Australian-born individuals (3005 females and 1980 males) diagnosed with affective psychosis (ICD-9 296.x) were extracted from the Queensland Mental Health Statistics System–a comprehensive, namelinked mental health register. We chose the age-at-first-registration for any ICD-9 296 diagnosis (patients may have had previous registrations for other disorders). Patients were divided into those with 296.1 (henceforth referred to as ‘296.1 only’) versus all other 296.x apart from 296.1 (henceforth referred to as ‘296 other’).
To allow a population-based adjustment, data on the age structure of the general population of Queensland were obtained from the 5-yearly census (1979–1991) conducted by the Australian Bureau of Statistics. Inception rates for each 5 year age division were determined as a rate per 100 000 population per year, following the method used by Eagles and Whalley [22] and Sibisi [8]. These data were plotted for visual inspection, and in addition, we calculated odds ratios for each age band that compared (a) males versus females, and (b) 296.1 only versus 296 other.
Results
For 296.1 only both males and females had near-linear increases in inception rates over the age groups (see Figure 1a,b). Overall, females outnumbered males. For those receiving a 296.1 only diagnosis, there was a male to female ratio of 1: 1.9, while for the 296 other category the ratio was 1: 1.3. The odds ratios confirmed a significant difference between 296.1 only and 296 other in all age-groups except the under 15s and where the distributions ‘crossed over’ in rate (data not shown).
Comparing age-at-first-registration for 296.1 (dotted line) with 296 other (filled line); (a) males; (b) females.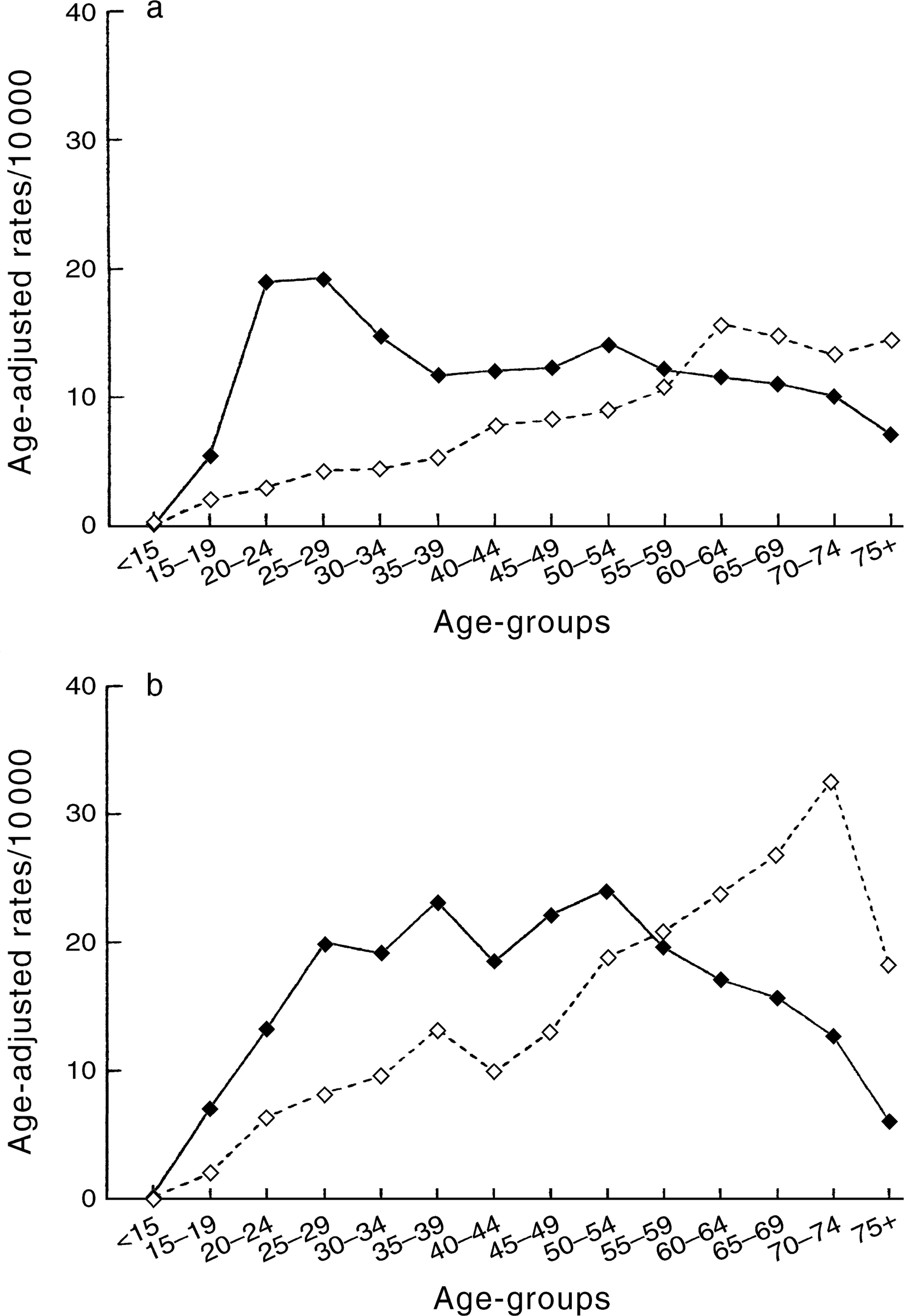
Following population-adjustment, the modal age of first registration for females was 70–74 for 296.1 only, while 296 other had a broad mid-life peak, with a modal age group of 50–54.
Figure 1 shows that both males and females had a ‘cross-over’ effect between the inception rates between the two categories of affective psychosis. For males between the ages of 15–54, rates for 296 other were substantially higher than for 296.1 only (e.g. in the 25–34 group about 4 times higher), whereas by the oldest age-group, rates are higher for 296.1 only. Similarly, for females between the ages of 15–54, rates for 296 other are substantially higher than for 296.1 only, whereas after age 60, rates are consistently higher for 296.1 only (e.g. approximately 3 times higher after age 70). The odds ratios confirmed that these within-diagnosis differences (296.1 only vs 296 other) were significant in 9 of the 14 age bands for males and 12 of the 14 age bands for females (data not shown).
Conclusions
Disaggregating ICD-9 affective psychosis by sex and by subcategory (296.1 only vs 296 other) may provide important clues to help understand the epidemiology of this group of disorders. Figure 1 demonstrates how lumping 296.1 only and 296 other together would: obscure the linear association between age and inception rates for 296.1 only; obscure the declining inception rates for 296 other in those over 60 years; and alter the nature of the sex difference in 296 other. It is not surprising that there is so little consensus in the literature on this topic.
Our finding that women outnumber men in most age groups is consistent with earlier studies [8, 18, 22] and reflects the common finding that depression is more frequently found among women following adolescence [29]. Such differences in men and women's susceptibility to affective disorder as they age are useful to identify potential psychological, social and biological risk factors [3, 8, 22]. However, while our findings do not support the hypothesis that hormonal events or fluctuations during childbearing years in women are risk factors for affective disorders [30], at least for those categorized under 296.1, hormonal events may be related to more frequent recurrence of episodes or prolongation of episodes in women compared to men.
For women, childbirth has been found to explain sex differences in age of onset in affective disorders [31], furthermore, depression associated with childbirth has been found to have an earlier onset than depression not so associated [32]. Unfortunately, we were unable to assess the effect of childbearing in this study–thus further work where such information is available is indicated. Similarly, further work on decomposing age at onset within bipolar disorders is warranted. Interestingly, a recent admixture analysis found equal proportions of males and females within three subgroups [33].
Another limitation of our study is that those who eventually develop an affective psychosis may initially have unipolar depressive disorders, some of who may have been coded 300.4 rather than 296.1; this suggests further longitudinal work on any relationship between unipolar and bipolar disorders. Nevertheless, further work is required in comparing the age-of-onset characteristics of 296.1 with those of non-psychotic depression coded as 300.4. The data are based on first registrations that contacted public hospital (both inpatient and outpatient services) and community psychiatric clinics. An uncertain fraction of those with affective psychosis may attend general practitioners or private psychiatrists, and thus not appear in our register. In addition, age-at-firstregistration clearly lags behind age of onset [34]. Males and females with affective psychosis may have differential pathways to care, and this may influence the sex differences detected in this study. However, the nearlinear rise in inception rates for 296.1 only strongly suggests age is a risk factor for this diagnosis.
The refinements to ICD-9CM and ICD-10 have more clearly separated unipolar and bipolar disorders, thus those interested in register-based research should have an easier task in future. However, there are other sources of heterogeneity that are amenable to an epidemiological approach. For example, further work is indicated by studies that have found phenomenological distinctions between early and late-onset depression in the elderly [35], subthreshold phenomenon [36], and also by studies that discuss the continuity or discontinuity between the affective disorders [37]. We hope that these issues, together with those identified in this study, will stimulate further epidemiological research.
Footnotes
Acknowledgements
The Stanley Foundation supported this project.