
Abstract
Epidemiological studies estimate that 20% of adolescents experience a depressive episode by age 18 [1]. Anxiety disorders are also common within this age group, with the prevalence of any anxiety disorder ranging from 5.7% to 17.7% [2–4]. The onset of such disorders during adolescence has been associated with a number of adverse outcomes, including increased risk of subsequent anxiety, depression, illicit drug dependence, educational underachievement and early parenthood [5–7], highlighting the importance of early intervention programmes that specifically target this population [8]. Substance use is also prevalent during this developmental stage [9], and young people with co-occurring affective and substance use disorders (SUD) consistently report greater levels of psychopathology as well as more psychosocial difficulties than those with SUD alone [10–12]. For example, adolescents (aged 14–18 years) with an affective disorder and co-occurring SUD reported more academic problems, suicide attempts and impaired role functioning than those with a single diagnosis [10]. Young drug users (aged 16–22 years) with co-occurring depression have also been found to report greater family, housing and substance-related problems, as well as a poorer quality of life than those with SUD alone [11].
Adolescents with co-occurring SUD and psychiatric disorders also appear to demonstrate poorer treatment outcomes at follow up [13–16]. For example, among adolescents admitted to an inpatient drug treatment programme, those with emotional problems reported higher rates of relapse at 2 year follow up than those with an SUD alone [16]. Similarly, Dobkin et al. reported that depressive symptoms at intake were predictive of non-improvement among those adolescents who completed a drug treatment programme [13]. However, most research studies examining the impact of co-occurring SUD and affective disorders on clinical outcomes among young people have typically recruited from residential drug programmes or inpatient psychiatric services [17–20], raising concerns regarding the representativeness of such samples. Some studies have been conducted among young people accessing outpatient mental health treatment, but these studies have primarily focused on young adolescents, and the psychiatric diagnoses of the mental health control groups have varied widely [21–23]. For example, Wilens et al. included adolescents with both psychotic and non-psychotic disorders [23], whereas Kramer et al. did not specifically report the psychiatric diagnoses within their adolescent sample [22].
The current study aimed to build on the existing literature, by examining baseline and 6 month outcomes of young people (aged 15–24 years) with a non-psychotic DSM-IV Axis I disorder and co-occurring SUD, who presented to a youth mental health service for assessment. Based upon the previous literature, we hypothesized that (i) at baseline, those with co-occurring SUD would demonstrate higher levels of psychopathology and suicidal ideation, and report lower levels of functioning than those without co-occurring SUD; and (ii) those with co-occurring SUD would report poorer functioning and greater psychopathology at 6 month follow up than those without co-occurring SUD.
Methods
Sample
The initial sample consisted of a cohort of 204 young people consecutively referred from April to September 2003 to ORYGEN Youth Health (OYH), a public specialist mental health service for young people aged between 15 and 24 years in Melbourne, Australia. This included individuals who were referred and accepted into the clinical service and those who were referred and not accepted (Figure 1). Acceptance into the service was determined by clinicians independent of the study, who conducted separate clinical assessments of clinical need and risk. Those meeting criteria for a DSM-IV psychotic disorder were excluded from the study by the research team.
Flowchart illustrating young people included in the final sample from population referred for treatment during study period. OYH, ORYGEN Youth Health; RA, referred and accepted into clinical service; SUD, substance use disorder.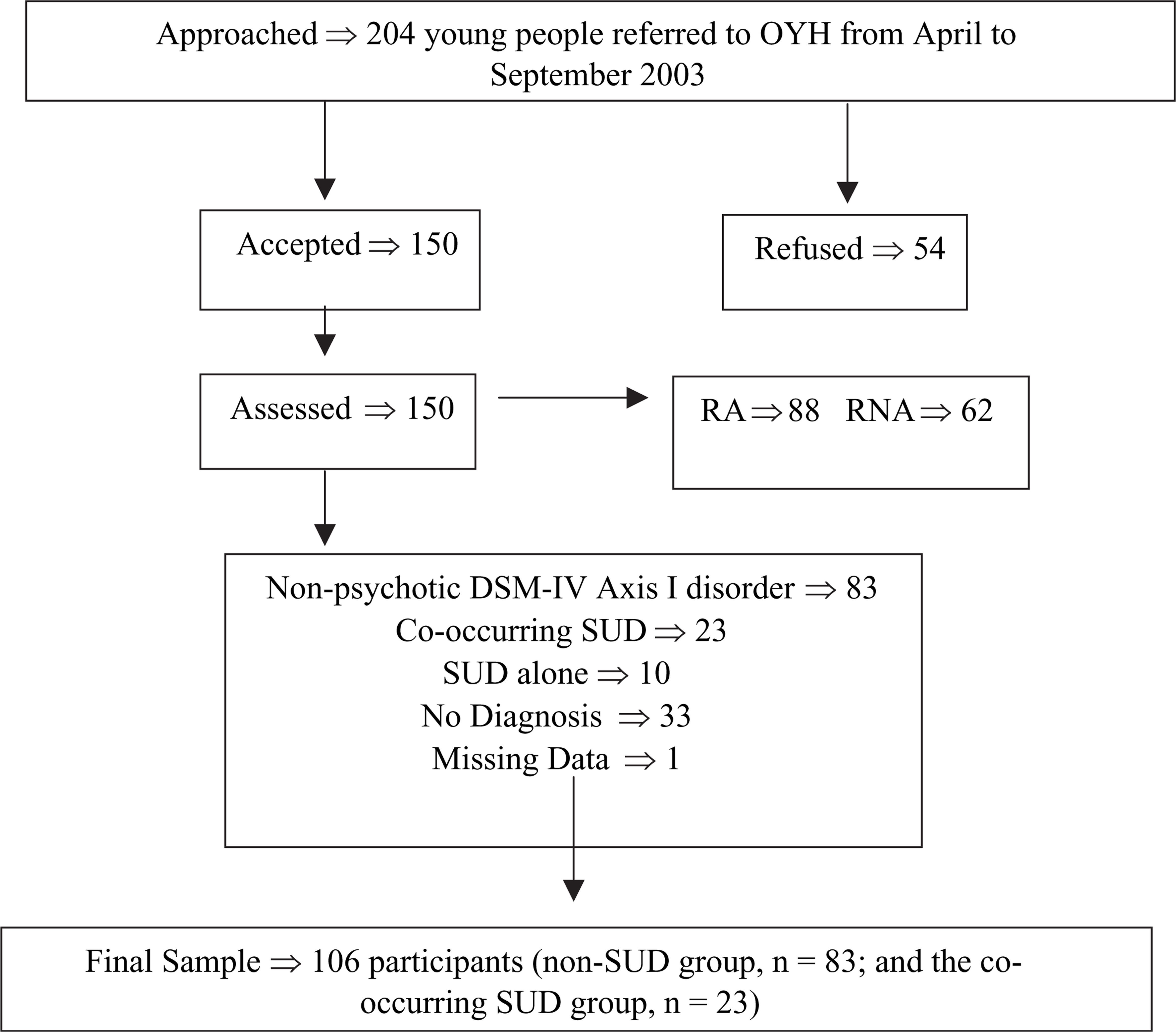
One hundred and fifty young people (73.5%) consented to participate. Of those, 88 were female and 62 were male, with a mean age of 17.7 years (SD = 2.6). This sample included 88 young people who were accepted into treatment at OYH and 62 who were assessed and subsequently referred elsewhere (e.g. primary care providers, school counsellors, drug treatment agencies). Eighty-three participants were diagnosed with a non-psychotic DSM-IV Axis I disorder, 23 with a co-occurring SUD, 10 with an SUD alone, and 33 were given no diagnosis. The final sample for the current study consisted of 106 participants (i.e. the co-occurring SUD group, n = 23; and the non-SUD group, n = 83).
Measures
Participants were given the Structured Clinical Interview for DSM-IV-TR–Patient Edition (SCID-IV) [24] to assess for current psychiatric diagnoses, including SUD (but excluding nicotine dependence). Functioning was measured with either the Global Assessment Scale (GAS; for participants 18–24 years old) [25] or the Childhood Global Assessment Scale (CGAS; for participants 15–17 years) [26]. Both scales give a single-item summary score of overall psychosocial functioning, with lower scores reflecting poorer levels of functioning.
The Center for Epidemiologic Studies Depression Scale (CES-D) was used to assess the level of self-reported depressive symptomatology in the past week. The CES-D consists of 20 items that rate frequency of depressive symptoms [27], with higher scores indicating greater depressive symptomatology. Anxiety levels were assessed on the Mood and Anxiety Symptoms Questionnaire Anxiety subscale (MASQ-A), which consists of 17 items [28]. High scores on this scale indicate high levels of anxiety. Question 83 from the MASQ was used to measure the frequency of suicidal ideation in the past week from 0 (not at all) to 5 (extremely). The Rosenberg self-esteem scale was used to assess levels of self-esteem [29]. High scores indicate low levels of self-esteem.
Procedure
All young people provided written informed consent to participate in the study. Ethics approval to conduct the study was granted by the local Research and Ethics Committee. Trained research interviewers received contact details of all young people referred to OYH during the study period, and invited them to participate. Face-to-face interviews were subsequently conducted within 2 weeks of referral to the service. Participants were than re-assessed face to face at the 6 months post-baseline interview using the same instruments. Each assessment took approximately 1–2 h, and participants were reimbursed $40 for time- and travel-related expenses at each assessment. Attempts to contact participants by phone and/or letter were made twice weekly until the follow-up assessment was 1 month overdue. If the young person could not be reached, family members and/or close friends (this information was given by the young person at baseline) were also contacted to obtain alternative contact details.
Data analysis
Analyses were conducted using SPSS version 12 for Windows (SPSS, Chicago, IL, USA). Data were initially screened for missing values and assumptions of normality, linearity, homogeneity and outliers. Mean scores for CES-D and MASQ-A at 6 months were initially transformed due to non-normality, but the transformed data produced similar results to the original scores so only the untransformed data are reported. At baseline, t-tests and χ2 tests were used to assess differences between groups (i.e. co-occurring SUD vs non-SUD). At 6 months, logistic regressions were used to identify associations between group status and categorical variables, and ANCOVAs were conducted to examine group differences. The interaction effect of acceptance into the service and group status was examined for each variable at 6 months. Because there were no significant interaction effects, only main effects are reported. Fisher's exact test and t-test were carried out to examine study dropout rates and differences between study completers and non-completers.
Results
Demographics
There were no significant group differences between the non-SUD and co-occurring SUD groups in regard to age, gender, school years completed, proficiency of English, number of current and lifetime diagnoses and number of participants accepted for treatment (Table 1).
Co-occurring and non-SUD groups at baseline
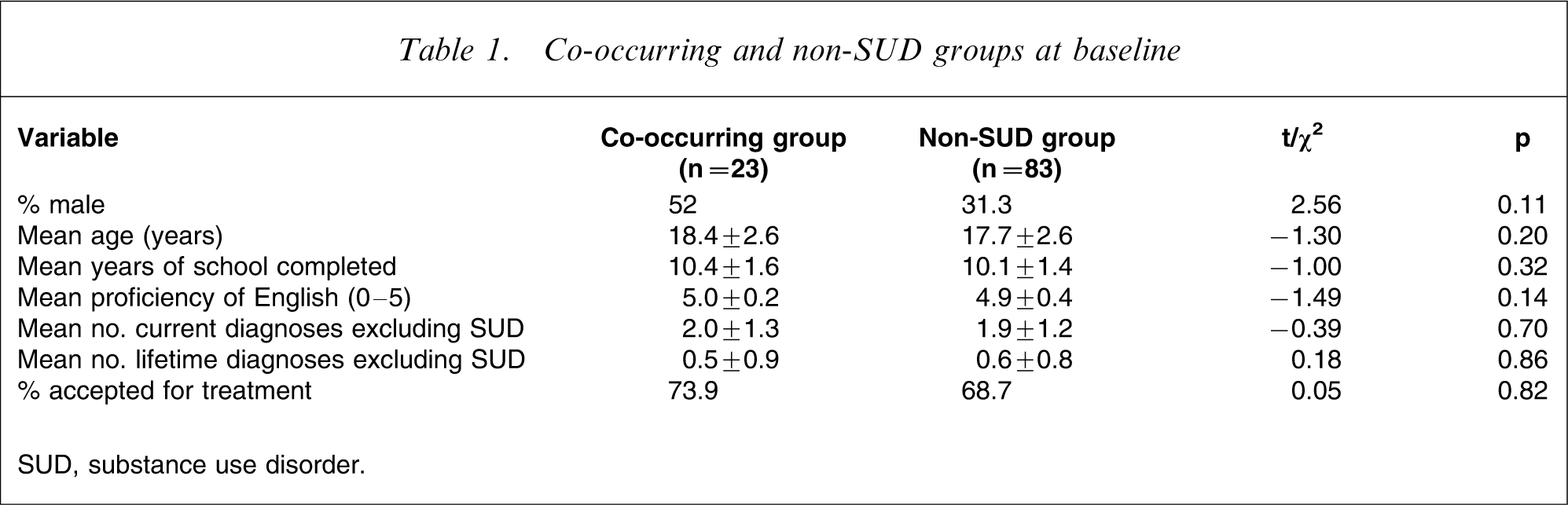
SUD, substance use disorder.
There were high rates of mood and anxiety disorders in the non-SUD group (n = 50, 60.2% for both disorders). Eleven per cent (n = 9) of the non-SUD group had an eating disorder and 15.7% (n = 13) had a disruptive behaviour disorder. For the group with co-occurring SUD, 56.5% (n = 13) met criteria for an anxiety disorder, 82.6% (n = 19) for a mood disorder, 8.2% (n = 2) for an eating disorder and 13% (n = 3) for a disruptive behaviour disorder. There were no significant group differences in regard to rates of disorders (except for SUD).
Ninety-six per cent (n = 21) of the SUD group had smoked a cigarette in the past month (4% had never smoked a cigarette), and the majority smoked on a daily basis (n = 15, 68.1%). In contrast, 63.6% of participants in the non-SUD group (n = 49) had tried a cigarette, 44.2% (n = 34) had smoked in the past month, and 24.5% were daily smokers. Almost 80% (n = 18) of the group with co-occurring SUD met criteria for substance dependence. Cannabis was the most common drug of dependence (35%, n = 8), followed by alcohol (26%, n = 6), stimulant and opioid dependence (9%, n = 2, for both).
Baseline mental health
As shown in Table 2, the co-occurring SUD and non-SUD groups had high levels of depression and anxiety and similar levels of self-esteem. No significant group differences were found, and both groups had serious impairments in functioning. But the impairment was significantly greater for the co-occurring SUD group. At baseline, both groups reported experiencing ‘a little bit’ to ‘moderate’ levels of suicidal ideation, but no significant group difference was found.
Comparison of mental health variables
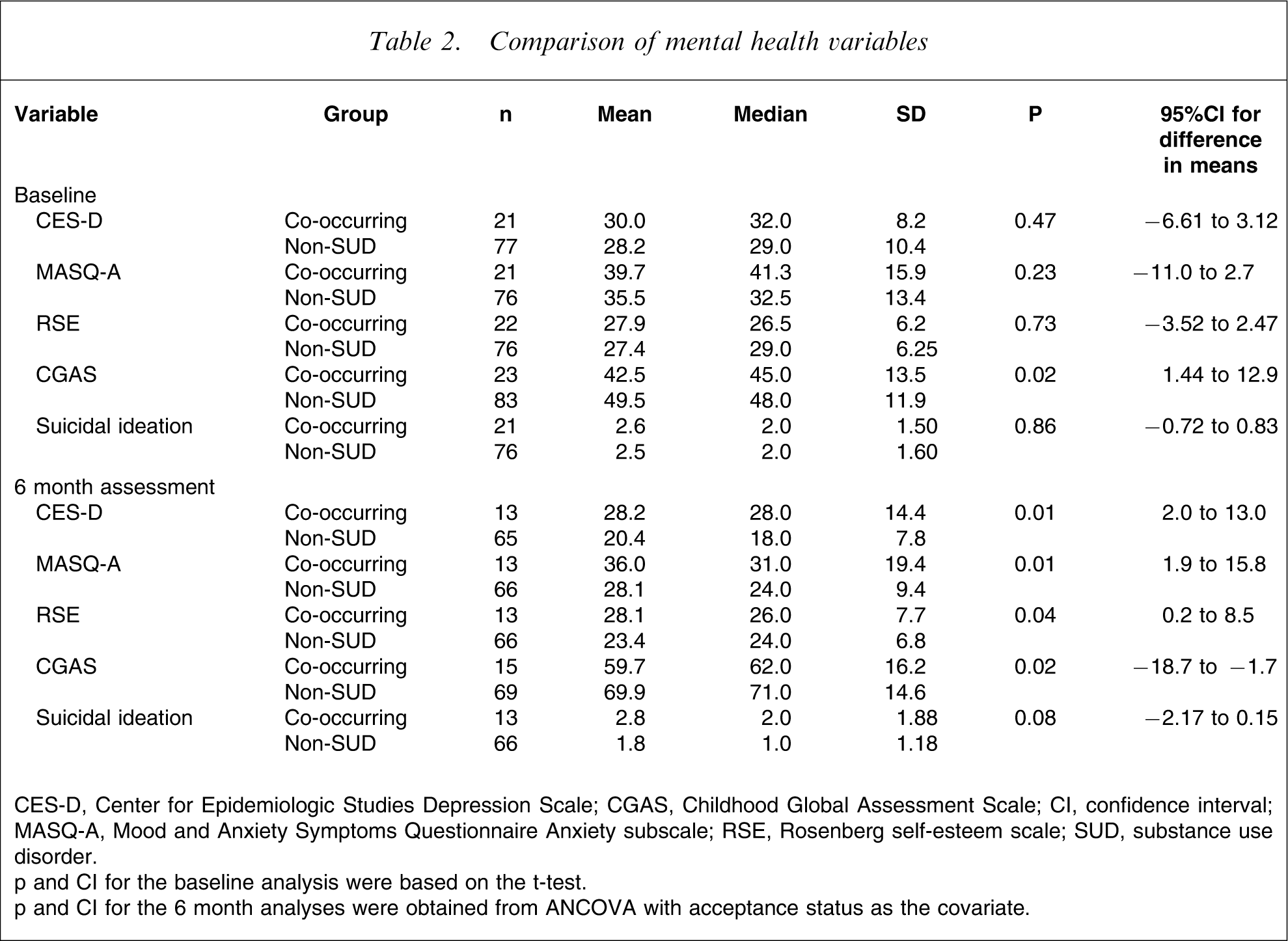
CES-D, Center for Epidemiologic Studies Depression Scale; CGAS, Childhood Global Assessment Scale; CI, confidence interval; MASQ-A, Mood and Anxiety Symptoms Questionnaire Anxiety subscale; RSE, Rosenberg self-esteem scale; SUD, substance use disorder.
p and CI for the baseline analysis were based on the t-test.
p and CI for the 6 month analyses were obtained from ANCOVA with acceptance status as the covariate.
Six month assessment
Participation rate
At 6 month follow up the participation rate for the co-occurring SUD group was 65.2% (n = 15) and 81.9% (n = 68) for the non-SUD group. Despite this, there was no significant difference between groups in regard to dropout rate (Fisher's exact test, p = 0.10).
There were no significant baseline differences between study completers and non-completers for both groups in regard to gender, age, school years completed, English proficiency, number of current and lifetime diagnoses, acceptance status for treatment, level of depression, functioning and suicidal ideation. In the co-occurring SUD group those who completed the 6 month assessment had a significantly higher level of baseline anxiety than those who dropped out (t(19) = − 2.1, p = 0.05).
Mental health
At 6 months the CES-D and MASQ-A scores remained high for the co-occurring SUD group but were reduced for the non-SUD group (Table 2). The co-occurring group had significantly higher levels of depression and anxiety than the non-SUD group. At 6 months, self-esteem improved for the non-SUD group but remained significantly lower for the co-occurring SUD group. C/GAS scores improved for both groups but the level of functioning for the co-occurring SUD group remained significantly lower than for the non-SUD group. While suicidal ideation reduced for the non-SUD group (median score was ‘not at all’), the co-occurring SUD group continued to report a score similar to baseline. Although a trend was evident, no significant difference was found between groups (Fisher's exact test, p = 0.08).
Stability of substance use disorder
A significant association was found between the status of SUD (i.e. absent or present) at baseline and at 6 month assessment (Fisher's exact test, p < 0.001). Among those who had the 6 month assessment, the majority of participants without an SUD at baseline did not meet criteria for a SUD at 6 month follow up (n = 65, 95.6%). The diagnosis of SUD was less stable, with only 46.7% (n = 7) of those with an SUD at baseline continuing to have an SUD at 6 month follow up. It is important to note that eight participants with an SUD at baseline did not complete the 6 month assessment. There were three new incidences of SUD at the 6 month assessment.
Service use
At 6 month assessment, there was no significant difference between groups in regard to use of services (Fisher's exact test, p = 1.00). Eighty-six per cent (n = 59) of the non-SUD group and 87% (n = 13) of the co-occurring SUD group received treatment from OYH and/or another agency in the previous 6 months.
Discussion
In the present study, we hypothesized that young people seeking help from a mental health service with co-occurring SUD and a non-psychotic DSM-IV Axis I disorder would report higher levels of psychopathology and suicidal ideation and poorer levels of functioning than young people with a non-SUD at baseline and 6 month follow up. These hypotheses were mostly supported.
At baseline, both groups had high levels of psychopathology, moderate levels of suicidal ideation and serious impairments in functioning. Participants with co-occurring disorders had significantly poorer levels of functioning but there were no significant group differences in regard to level of psychopathology and suicidal ideation. At 6 months, the non-SUD group significantly improved compared to the group that had co-occurring SUD, who continued to experience high levels of depression and anxiety and low levels of self-esteem and functioning. Although no significant group difference for suicidal ideation was evident at 6 months, a trend was found. The reduction in depressive symptoms in the non-SUD group could possibly account for the decline in their rate of suicidal ideation.
Previous studies investigating the impact of co-occurring SUD among adolescents presenting to mental health services have reported similar findings to the current study. Adolescents with co-occurring SUD have been found to have lower functioning levels and higher rates of psychopathology on referral to a mental health service than non-SUD psychiatric controls [22, 23]. Those with co-occurring SUD have also been found to have a poorer response to treatment than those without an SUD [22]. Differences in sample characteristics may account for the different findings with respect to psychopathology at baseline. For example, Wilens et al. included young people with both psychotic and non-psychotic disorders, and reported a higher prevalence of psychotic disorders within the SUD group (14%) compared to the control group (8%) [23]. Nevertheless, these findings highlight the need for routine assessment and treatment of substance use issues within youth mental health settings.
There are several limitations that need to be considered when interpreting the present findings. All substance use data were based upon self-report, and no objective testing was conducted. As such, there may have been errors of omission in reported substance use, which in turn could have reduced differences between groups. Future studies would benefit from integrating self-report and laboratory testing to more accurately identify individuals with SUD. Further, no diagnostic data were available for those who did not consent to participate. Although the majority (73.5%) of young people seeking help agreed to participate in the current study, it is possible there was a selection bias. Given this, some caution is required when generalizing the present findings to other mental health settings.
A substantial number of participants were unable to be followed up at the 6 month assessment. Although baseline variables were not markedly different between study completers and non-completers, it is possible that participants who dropped out experienced greater difficulties, preventing them from continuing with the study. Stinchfield et al. investigated follow-up bias in a group of adolescents within an inpatient substance abuse treatment programme [30]. They found that the difficult-to-contact group had consistently poorer outcomes compared to the easy-to-contact group across most outcome variables, suggesting that study completers may represent overestimates of outcome and may not be generalizable to the non-completers group. The small sample size at 6 month follow up may also have increased the risk of Type 2 errors, and it also precluded an examination of the relationship between course of SUD and outcome. Finally, no measure of treatment intensity or duration was recorded, raising questions regarding the dosage of treatment received by the SUD and non-SUD groups.
Despite these limitations, the present study provides valuable information concerning the extent of co-occurring SUD among young people seeking help from a specialist mental health service, as well as the impact on 6 month outcomes. The high rates of co-occurring SUD found in the current study, in conjunction with associated poor outcomes, raises important clinical issues in regard to treatment planning and service provision. It highlights the importance of assessing and managing substance use issues as part of, and not separate to, mental health treatment, and supports previous recommendations for the management of co-occurring disorders [31]. Indeed, early intervention of co-occurring SUD is clearly essential if we are to reduce the associated morbidity over the shorter-term. Comprehensive training and support of youth mental health and drug and alcohol clinicians in the assessment and management of both disorders is therefore essential [32, 33], as is the fostering of strong partnerships between the mental health and drug treatment system. The present findings also raise the question of whether more intensive, integrated interventions are required for young people with co-occurring mental health and substance use disorders [34]. Further research is clearly required in this regard.
Conclusions
The present findings extend previous work in the youth comorbidity area by examining the impact of co-occurring SUD among a help-seeking population of young people with a current non-psychotic Axis I disorder. We found that although young people with co-occurring SUD had similarly high levels of psychopathology, impairments in functioning and suicidal ideation at baseline, they demonstrated poorer health outcomes at 6 month follow up compared with a non-SUD group. These findings highlight the importance of early detection and management of SUD as part of routine mental health treatment, and support calls for better coordination of youth mental health and substance use services.
Footnotes
Acknowledgements
The authors wish to thank the Colonial Foundation and the staff and young people at ORYGEN Youth Health who supported this project.