
Abstract
Depressive disorders in mothers and emotional and behavioural disturbances in children are common and tend to coexist [1]. Previous empirical reviews have documented the influence of maternal mood on child adjustment outcomes [2]. Among preschool children, maternal depression has been linked with severe temper tantrums, difficulty relating to parents or peers, and eating problems [3, 4].
The Achenbach Child Behaviour Checklist (CBCL) has been widely used in both clinical and community populations to measure child behaviour problems [5, 6]. Research has found that children of depressed mothers have more internalizing problems [7]. Other studies have reported the association between presence of maternal depressive symptoms and elevated levels of externalizing problems [8, 9]. In addition, significant correlations have been found between maternal depression and both the internalizing (e.g. inhibition, withdrawal) and externalizing (e.g. aggression, hyperactivity) scores [10–14].
The timing of maternal depressive symptoms may have an impact on child behaviour. Essex et al. reported that initial exposure to maternal major depression during infancy was associated with internalizing symptoms whereas initial exposure in the toddler or preschool years increased the risk of “pure” externalizing symptoms [15]. It is also possible that these effects are due to the persistence or recurrence of maternal depression into the toddler/preschool period, so that it is the length of the exposure, rather than its timing, that is important [16, 17].
Child gender may moderate the influence of maternal depressive symptoms. One study showed that maternal depressive symptoms were associated with emotional disorder in girls but not in boys [18]. Maternal depressive symptoms have also been correlated with parental report of child anxiety for girls but not boys [19].
The finding that depressed mothers report increased problems in their children is likely to be a combination of both negativity in the perceptions of the mothers and the fact that the children of depressed mothers actually have increased levels of internalizing and externalizing problems [9]. Youngstrom et al. concluded that maternal dysphoria measures accounted for an additional 10% of variance in the mothers’ descriptions of their own children [20]. In contrast, dysphoria-related bias did not explain the majority of variance in maternal ratings of the children.
Although a number of cross-sectional and longitudinal studies have been conducted internationally regarding the associations between maternal mental health and child behaviour, only some have dealt with early childhood, specifically toddlers [14, 15, 17, 21–24] and examined the effect of the timing and persistence of maternal depression [15, 17, 21, 23, 24].
The Pacific Island population is one of the fastest growing population subgroups in New Zealand. It forms an integral part of New Zealand society [25], and has a diversity that is manifest in differing cultures, languages, and corresponding access to health and social services. Compared with most New Zealand children, Pacific children are at increased risk of poor health [26, 27].
The Pacific Islands Families (PIF) Study is a longitudinal study of a cohort of Pacific children and their families living in New Zealand. Using the data from this birth cohort, the present study examined the relationship between timing and persistence or recurrence of maternal psychological disorder and early child behaviour problems.
Methods
The study was approved by Auckland Branch of the National Ethics Committee, the Royal New Zealand Plunket Society and the South Auckland Health Clinical Board.
Study design
Data were collected as part of the PIF Study, a longitudinal investigation of a cohort of 1398 infants (22 pairs of twins) born at Middlemore Hospital, South Auckland, New Zealand during the year 2000. Middlemore Hospital was chosen as the site for recruitment of the cohort because it has the largest number of Pacific births and is representative of the major Pacific ethnic groups (Samoan, Cook Island Maori and Tongan). Eligibility criteria included having at least one parent who self-identified as being of Pacific ethnicity and a New Zealand permanent resident. Thus, infants of non-Pacific mothers were eligible for the study in cases where the father was of Pacific descent.
Study sample and recruitment procedures
Of the eligible mothers, 1376 (93%) participated at 6 weeks, 1224 (83%) participated at 12 months, and 1144 (77%) participated at 24 months. No important differential attrition was observed. Female interviewers of Pacific ethnicity who were fluent in English and a Pacific Islands language visited mothers in their homes. Once informed consent was obtained, mothers participated in 1 h interviews concerning family functioning and the health and development of the child. This interview was conducted in the preferred language of the mother. Within the context of a wider interview at the 24 month data point, child behaviour was measured using the CBCL [5].
At 24 months 1030 maternal child behaviour reports were gathered (excluding twins). Seven mother-figures who were not biological birth mothers at the 6 weeks interview and two child behaviour reports with more than eight missing values for CBCL were also excluded from the study.
Of 1021 children included for the present study, 484 (47.4%) were girls and 537 (52.6%) were boys. Detailed information about the PIF cohort and procedures is described elsewhere [28].
Measures
Maternal mental health
At 6 weeks, the depressive symptoms of the mothers were screened with the Edinburgh Postnatal Depression Scale (EPDS). The EPDS required mothers to select an option that best described their feelings during the previous week. Each of the items was scored on a 4-point scale from 0 to 3, with a total score ranging from 0 to 30. A cut-off of 12/13 is recommended for screening major depression [29]. In the present study mothers who scored above the cut-off were referred as symptomatic and those who scored below as non-symptomatic. The reliability coefficient measured by Cronbach's alpha was 0.86.
At 12 and 24 months, maternal health was assessed using the 12-item General Health Questionnaire (GHQ-12) [30], a self-report screening tool widely used to identify minor psychiatric disorder in adults. The GHQ-12 was scored to give a total of 12 using the binary method of scoring. A cut-off of 2/3 is recommended for screening psychological disorder. Mothers who scored above the cut-off were referred as symptomatic, and mothers who scored below as non-symptomatic. The reliability coefficient of the GHQ was 0.87.
Child-rearing practices
Parenting practices in terms of nurturing and discipline were measured at 24 months using a modified version of the Parent Behaviour Checklist (PBC) [31]. The PBC is an empirically derived instrument developed specifically for the parents of children aged 1–4 years. For the purposes of the PIF Study, modified versions of two subscales (nurturing and discipline) were used. Discipline items measure parental responses to problem behaviour, and nurturing items measure behaviour that promotes a child's psychological growth. Items are answered on a 4-point frequency scale and scores are summed. The reliability coefficient in the PIF Study was 0.77 for Discipline and 0.71 for Nurturing. The two scale scores were categorized into four levels using quartiles. Higher scores in each subscale were indicative of greater nurturance and greater use of discipline behaviours.
Cultural orientation
The General Ethnicity Questionnaire [32] is based on the widely used concept of acculturation, the process of change that groups and individuals undergo when they come into contact with another culture. Four different varieties of acculturation (‘assimilation’, ‘integration’, ‘separation’, and ‘marginalization’) have been identified. In assimilation, cultural identity is relinquished and the individual moves into the larger society (low Pacific, high New Zealand). Integration involves maintenance of cultural integrity but also the movement to become an integral part of the larger society (high New Zealand/high Pacific Island). Separation refers to self-imposed withdrawal from the larger society (high Pacific/low New Zealand), and marginalization refers to losing the essential features of one's culture, but not replacing them by entering the larger society (low Pacific/low New Zealand).
Child behaviour problems
At the 24 month phase, behaviour problems were measured with the CBCL toddler version for ages 1.5–5 years [5]. Mothers rated 100 symptoms on a 3-point scale scored 0 (not true), 1 (somewhat true) or 2 (very true). The CBCL includes seven narrow-band syndromes: emotionally reactive, anxious/depressed, withdrawn, somatic complaints, sleep problems, attention problems and aggressive behaviour. Two broad-band scales, internalizing and externalizing scores, are then derived from the seven narrow bands with the first four syndromes together comprising the internalizing subscale and the last two comprising the externalizing subscale. The CBCL has been widely used in both clinical and community populations and extensive information is available about its reliability and validity [5]. In the present study Cronbach's alpha was 0.77 for internalizing and 0.76 for externalizing scores.
In order to determine clinically relevant cases (defined as a need for diagnosis, counselling or treatment), the cut-off for raw scores developed in receiver operating characteristic analysis with the original instrument in US samples was used [5]. The 90th percentile defined the clinical range for internalizing and externalizing scores.
Other sociodemographic characteristics
Mother's age, ethnicity, household income and prenatal exposure to cigarettes collected at the 6 weeks interview, along with education level and marital status collected at the 24 months interview, were taken into account in this analysis.
Statistical analysis
The dependencies between groups of depressive and psychological disorder symptoms at different time-points were explored using χ2 test or Fisher's exact test where appropriate. The kappa (κ) statistic was used to measure agreement between these variables. Due to repeated measure of maternal mental symptoms, effort was made to develop a composite measure using all three time-points to capture the information of timing and persistent or recurrent exposure. Two methods were used. First, a backward selection method was used to select variables from three time-points to predict child internalizing and externalizing problems. Specifically, starting from the saturated model with main effects (three terms) and all interactions (three terms of two-level interactions and one term of three-level interaction), the non-significant effect that contributed least to the logistic regression model was identified and eliminated from the model, and the regression re-run until all the terms remaining in the model were statistically significant. A composite measure was then developed according to the regression result. Second, we compared the prevalence of internalizing and externalizing problems at eight different levels of exposure to maternal postnatal depression and/or psychological disorders, that is, one level as depression at 6 weeks, but no psychological disorder at 12 or 24 months, then combined the groups with similar prevalence to develop a composite measure. The two methods generated the same result and thus a final composite measure was formed with four groups: (i) no symptoms at any interview; (ii) early symptoms of postnatal depression (depression at 6 weeks, but no psychological disorder at 12 or 24 months); (iii) late symptoms of psychological disorder (no postnatal depression at 6 weeks, but psychological disorder existing at 12 or 24 months or both time-points); and (iv) persistent or recurrent symptoms (depression at 6 weeks and psychological disorder at 12 or 24 months or both time-points). Further multivariable logistic regression was used to examine the variation in risk of behaviour problems according to the composite measure of maternal mental symptoms, after adjusting for the sociodemographic characteristics, cultural orientation, maternal smoking during early pregnancy, and child-rearing practices and the interaction between maternal symptoms and child gender. In these analyses the composite measure of maternal mental symptoms was forced to enter to the regression models; whereas all other factors were selected into the models by stepwise method. Crude odds ratios (ORs) were adjusted for risk factors that were significantly related to the outcomes.
All analyses were performed using SAS version 9.1 (SAS Institute Inc., Cary, NC, USA) and SPSS version 14.0 (SPSS Inc., Chicago, IL, USA) statistical software packages, and a significance level of α = 0.05 was used to determine statistical significance for all calculations.
Results
Sample characteristics
Sociodemographic profile of the mothers of 1021 children was similar to the full cohort of 1376 at 6 weeks and of 1144 at 24 months interview. Details of sociodemographic characteristics of this sample are presented in Table 1.
Sociodemographic characteristics for participating mothers (n = 1021)
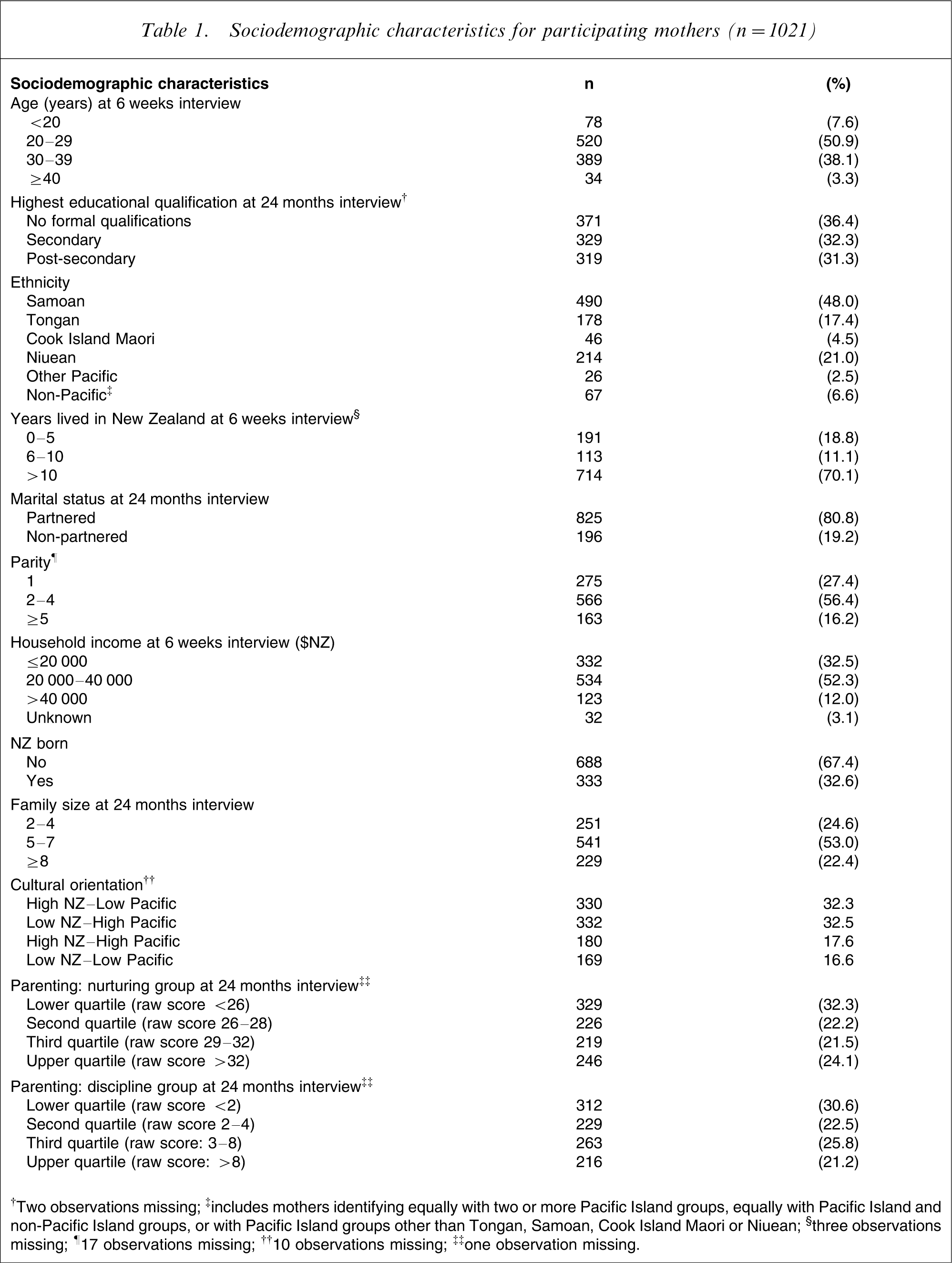
†Two observations missing; ‡includes mothers identifying equally with two or more Pacific Island groups, equally with Pacific Island and non-Pacific Island groups, or with Pacific Island groups other than Tongan, Samoan, Cook Island Maori or Niuean; §three observations missing; ¶17 observations missing; ††10 observations missing; ‡‡one observation missing.
Maternal mental symptoms
Of 1021 mothers, 1016 completed the EPDS at 6 weeks, 967 completed the GHQ at 12 months and 1017 at 24 months. A total of 960 completed three time-point measures. The frequency and prevalence of maternal symptoms of postnatal depressive or psychological disorder were 164 (16.1%), 118 (12.2%) and 97 (9.5%), respectively, for the corresponding time-point.
There was a dependency between any two time-point measures although the agreement (κ = 0.16, 0.13 and 0.13, respectively) was minor due to low prevalence of mental problems.
Child behaviour problems and associations with maternal mental health
The frequency and prevalence of clinically relevant cases were 171 (16.7%) for internalizing and 69 (6.8%) for externalizing in the present study. Table 2 shows that the prevalence rates of clinically relevant cases for internalizing problems were higher in children of mothers who had depressive symptoms at 6 weeks or psychological disorder at 12 or 24 months compared to those who did not have such symptoms at that time (6 weeks, 32.3% vs 13.6%; 12 months, 28% vs 15.1%; 24 months, 25.8% vs 15.8%); all differences were significant. The corresponding comparisons for externalizing were statistically significant at 6 weeks (10.4% vs 6.1%) and at 12 months (11.9% vs 6.4%), but not at 24 months (8.2% vs 6.6%).
Internalizing and externalizing problems by maternal symptoms of psychological disorder
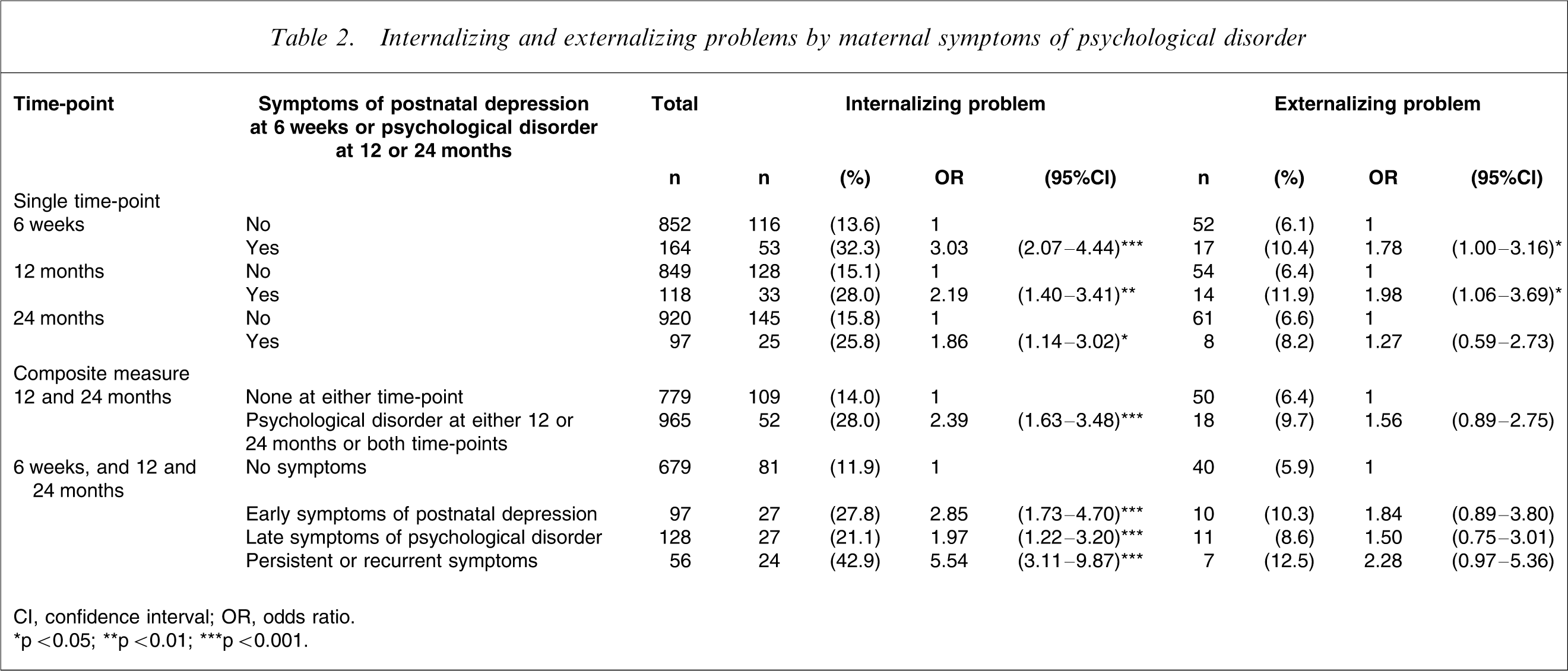
CI, confidence interval; OR, odds ratio.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
The logistic regression to select the variables of maternal symptoms at three time-points for predicting internalizing problems yielded two terms, namely, early symptoms of postnatal depression at 6 weeks and the interaction of psychological disorder between 12 and 24 months. Further exploration of the interaction suggested that prevalence of internalizing problems was similar in the group of psychological disorder at 12 or 24 months to the group with psychological disorder at both time-points. Therefore a binary variable was created to combine 12 and 24 month data: non-psychological disorder at 12 or 24 months; psychological disorder at either or both time-points. The corresponding prevalence of internalizing problems was 14% and 28%, respectively. The composite measure with four levels of exposure to the symptoms at 6 weeks, 12 and 24 months was then derived and the overall difference of prevalence in these four groups was significant (11.9% in no symptoms, 27.8% in early symptoms of postnatal depression, 21.1% in late symptoms of psychological disorder and 42.9% in persistent or recurrent symptoms). The corresponding ORs were 2.85 (95% confidence interval (CI): 1.73–4.70), 1.97 (95%CI: 1.22–3.20), 5.54 (95%CI: 3.11–9.87), respectively, relative to the non-symptomatic group.
The same procedure was used for predicting externalizing problems and it yielded two terms, namely, early symptoms of postnatal depression at 6 weeks and psychological disorder at 12 months. To maintain consistency between the analysis of internalizing and externalizing problems and utilize 24 month interview data, the same composite with four levels of exposure to maternal psychological disorder was developed. No statistically significant differences of externalizing problems were found in these groups.
Upon further examination of the relationship between maternal mental symptoms and child behaviour problems, analysis indicated no interaction effects between maternal symptoms and child gender. Table 3 shows the effects of maternal mental symptoms on clinical behaviour problems following adjustment for sociodemographic and maternal risk factors. For internalizing problems, the adjusted OR was 1.38 (95%CI: 0.79–2.43) in early symptoms of postnatal depression, 1.45 (95%CI: 0.85–2.49) in late symptoms of psychological disorder and 2.93 (95%CI: 1.54–5.57) in persistent or recurrent symptoms compared with the no symptoms group. The effect for persistent or recurrent symptoms still remained significant whereas the other two groups no longer did. Maternal ethnicity and smoking during early pregnancy were also entered into the model. For externalizing problems, the effects of maternal symptoms remained insignificant after adjustment of covariates. Child sex and cultural orientation were independently associated with the externalizing problems.
Internalizing and externalizing problems by maternal symptoms of psychological disorder and covariates
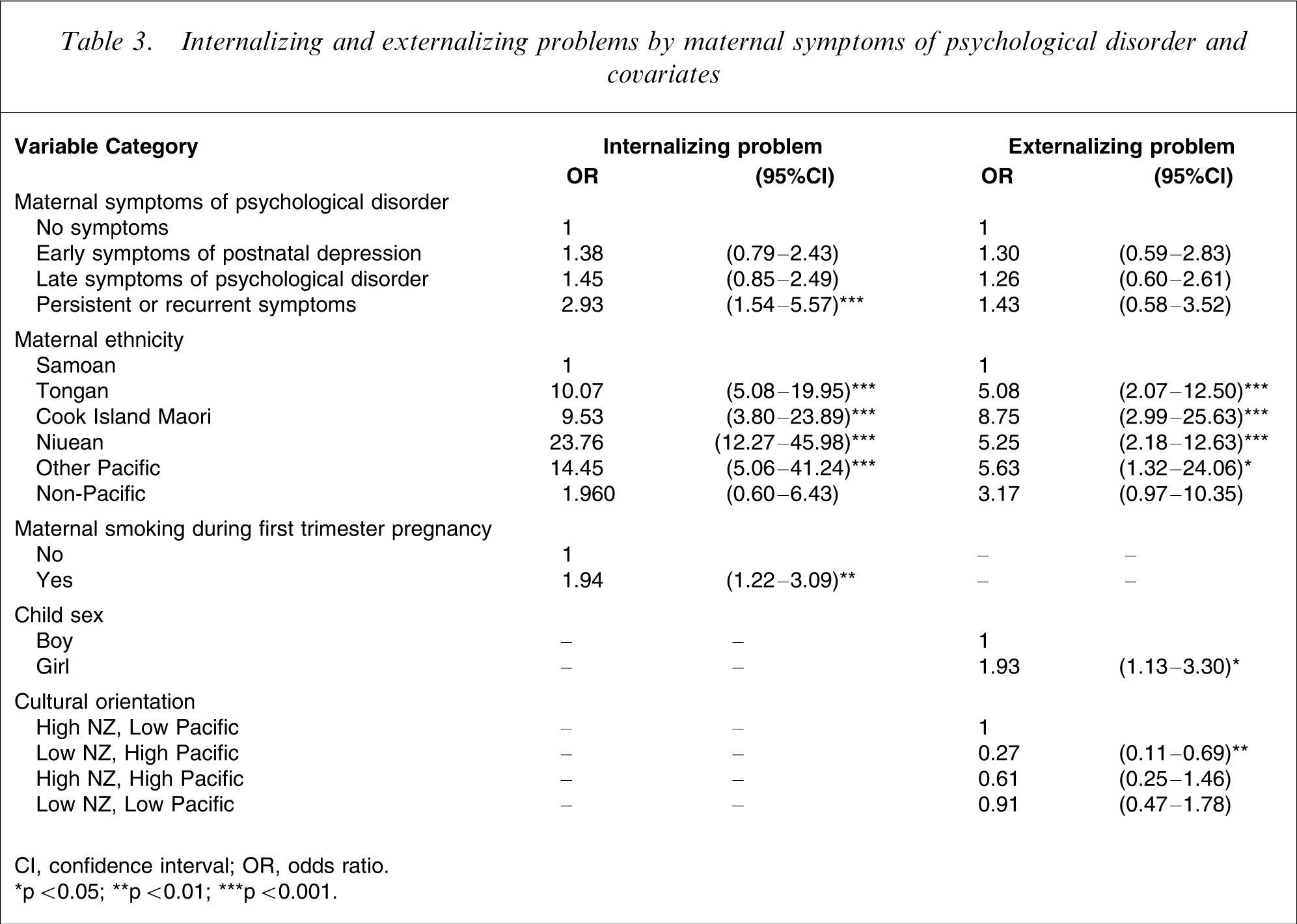
CI, confidence interval; OR, odds ratio.
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Discussion
The aim of the present study was to examine the relationships between maternal symptoms of psychological disorder and child behavioural problems, and to compare the effects of timing and persistence or recurrence of symptoms on early child behaviour problems in a cohort of 2-year-old Pacific Islands children born in New Zealand. The findings suggested that the behaviour of 2-year-old children of mothers who have suffered from persistent or recurrent maternal symptoms of psychological disorder exhibited significantly more internalizing problems than children of mothers who have never had such symptoms. The former group was nearly threefold as likely as the latter to exhibit behaviour problems. However, although the children of mothers who had experienced only early symptoms of postnatal depression or late symptoms of psychological disorder showed increased internalizing problems compared with the same reference group, the effects were no longer statistically significant after controlling for other sociodemographic and maternal health factors. For the externalizing problems, none of the three groups of different exposures showed significantly increased likelihood of being in clinical ranges compared with the non-exposure reference group. These findings demonstrate the importance of taking a longitudinal perspective to investigate the development of behavioural problems in childhood and the way in which factors such as maternal mental health impact on this development.
The present findings are in partial accordance with some international studies. Analysing the data from the 1988 US National Maternal and Infant Health Survey (NMIHS) and a 1991 follow-up survey, Civic and Holt also found that children of mothers with persistent depressive symptoms had the greatest risk of behaviour problems [24]. However, their conclusion that mothers depressed at one time-point had an increased likelihood of reporting child behaviour problems differed from ours. The differences are likely to be compounded by different measurements and a larger sample in a very different geographical area.
It is important to compare the present findings with international findings based on the measure of CBCL [5]. However, differences in study design and sampling remain an important consideration. In the PIF Study maternal depressive symptoms were measured using EPDS [29] at 6 weeks, whereas GHQ [30] was used to measure maternal psychological disorder at 12 and 24 months. At the 6 week interview, 16.4% of mothers reported experiencing depressive symptoms [33]. This rate is at the high end of the range typical of surveys conducted internationally [22, 34] and slightly higher than the rates from earlier domestic studies [35, 36]. While the high internal consistency suggests that the EPDS is valid in the present context, further investigation of its formal psychometric properties, including predictive and construct validity, is warranted [33].
In addition, within the PIF cohort there was a higher prevalence (17.1%) of internalizing problems and lower prevalence of externalizing problems (6.6%) compared with US normal samples [37]. This may be partly due to the difficulties associated with the measurement of behavioural problems at the early preschool age, and may reflect cultural differences in child-rearing practices and attribution among Pacific parents. Pacific researchers have studied some Pacific customs and practices within the Pacific family context and found that parents believe that heavy discipline is necessary because poor behaviour can bring shame to the whole family [38]. This parenting inevitably affects how Pacific children respond in the parent–child equation. Because there is no previous research using CBCL in Pacific children, in-depth qualitative study would strengthen the applicability of the measurement instruments used in this ethnic population.
Despite there being some methodological and cultural differences in international studies using CBCL as the outcome, the PIF findings corroborate internationally recognized conclusions, that is, maternal psychological disorder is associated with child behaviour problems. Whether the association is only with internalizing [7] or externalizing [8, 9] or total problems [10–14] needs to be further researched.
Some suggest that depressed mothers are biased informants about their children's behaviour [39]. Recent empirical studies using advanced statistical methods have concluded that depressed mothers may have somewhat biased reports, but that there is a true association between maternal depression and child behaviour problems [7, 8, 40]. We believe that the present study provides further evidence that the association is not spurious. In the PIF longitudinal study maternal symptoms of psychological disorder were assessed at two measurement points prior to maternal report of child behaviour and the last assessment co-occurred with the report of child behaviour. Apart from the persistent or recurrent symptoms, we did not find significant associations between either early symptoms of postnatal depression or late symptoms of psychological disorder and child behaviour after controlling for other confounding factors. The similar strength of associations (internalizing: OR, 1.39 in early symptoms and 1.42 in late symptoms; externalizing: 1.31 and 1.20, respectively) suggested that the observed relationship between maternal symptoms and child behaviour cannot be due to mothers’ biased assessments of their children's behaviour. If this was the case, the OR would be greater for late symptoms of psychological disorder than for early symptoms of postnatal depression.
Contrary to those reporting the association between maternal depression and child problem behaviour to be generally more prevalent among girls [18, 19], this interaction was not seen in the present findings. It has been suggested that in general, few gender differences in behaviour problems are seen in early childhood and instead tend to emerge at approximately 4 years of age with more consistent findings reported for school-aged children [41, 42]. Differing cultural norms and values may also have an important influence on how child behaviours are perceived overall and between boys and girls [43].
Previous reviews have documented the influences of maternal mood on child adjustment outcomes [2] and mutual influences on maternal depression and child adjustment problems [1]. Three sets of interrelated, mediating factors have been identified to explain pathways of mutual influences; these are biological, psychosocial, and social capital mechanisms [1]. The development of the mother–child attachment in the first year of life is of particular importance [44].
Prolonged postpartum maternal depression interferes with the mother's emotional availability and sensitivity to the child's needs, disrupting the development of a secure attachment bond [45]. The long-term consequences of insecure attachment entail chronic difficulties in emotional regulation, sensitivity to stress, and social functioning[46]. Apart from the mother–child attachment, child discipline practices, modelling, and family functioning also play roles in psychosocial mediation [1].
Several limitations should be noted in the present study. Given that the data are based on maternal reports, the possibility of maternal bias remains. Paternal reports that will be collected in later assessment points may clarify this possible bias. The CBCL is considered a valid and reliable standardized measure of problem behaviour, yet such measurement may fail to capture the full extent of early problem behaviour in this cohort.
The fact that different tools were used to measure maternal mental health across the time points is another weakness. While EPDS measures postnatal depression, GHQ is not a measure of depression. It is a screening instrument for minor or non-psychotic mental disorder/disturbance. Although both the EPDS and the GHQ exhibited good reliability and validity, we acknowledge the difficulties and limitations of generating and defining a composite variable from these two different measures. In addition, we do not have the ability to compare diagnostic consistencies between these two measures. This may have led to some misclassifications of the composite measure of maternal psychological disorder, which, in turn, may affect the relationship between maternal symptoms of psychological disorder and child behaviour and reduce the capacity of comparisons between the present findings and the findings from other international studies that measured maternal depression.
One of the strengths of the present study is that it is prospective in nature. The use of longitudinal data allowed us to determine the associations between maternal symptoms of psychological disorder reported prior to maternal report of child behaviour, establishing more clearly the temporal sequence of the association. The repeated measure of maternal psychological disorder at three time-points also allowed us to compare the importance of timing and persistence or recurrence of such symptoms. Another strength is that mother's ethnicity and cultural orientation were taken into account in the analysis. Previous PIF findings reported that Samoan mothers experienced the lowest prevalence of postnatal depressive symptoms among all ethnic groups within the cohort [33]. The current study demonstrated that Samoan mothers reported the lowest prevalence of both internalizing and externalizing problems compared with all other ethnic groups within the cohort. While there are many similarities between the Pacific Island groups living in New Zealand, it would be useful to identify the protective factors that contribute to the low risk for Samoan women and children. In term of cultural orientation, the present study showed that mothers who adopted a separation strategy, valuing and engaging significantly with Pacific Island cultural norms, had low risk with respect to the child's externalizing problems compared with those who adopted a strategy of assimilation or marginalization. Integrationists were at low risk; but the comparison was not statistically significant. These findings suggest that retention of elements of traditional Pacific culture and identity serve a protective role with respect to child behaviour problems. Further research is required to explore these observed ethnic patterns and to determine which particular values and norms are implicated in Pacific Islands culture and whether integration plays a protective role of reducing child behaviour problems in comparison with marginalization and assimilation.
At later assessment points we will be able to track the stability and change in maternal health and child behaviour problems. These design strengths, together with the size of the cohort and the cultural sensitivity of the methods and procedures demonstrate the robustness of the PIF Study findings.
Findings suggest that persistent or recurrent maternal symptoms of psychological disorder may contribute to an increase in the behavioural problems of children as young as 2 years of age. However, the timing of disorder, whether it is infant or toddler exposure, does not appear to be as crucial. Therefore, we hypothesize that it may be the length of exposure rather than timing of exposure to maternal psychological disorder that is the important contributory factor. Further research is needed to assess this hypothesis.
This study contributes to the limited data available worldwide on behaviour problems specific to toddlers from different ethnic groups. Improved understanding of the associations between maternal psychological disorder and early child behaviour problems may help maternal and child health professionals design appropriate and effective screening and intervention programs to help Pacific mothers and children.
Footnotes
Acknowledgements
The PIF Study is supported by the Foundation for Science, Research and Technology, the Health Research Council of New Zealand and the Maurice and Phyllis Paykel Trust. The authors gratefully acknowledge the families who have participated in the study, the Pacific Peoples Advisory Board and the other members of the research team.