
Abstract
Objective:
We investigated patterns of service contact for self-harm and suicidal ideation recorded by a range of human service agencies – including health, police and child protection – with specific focus on overlap and sequences of contacts, age of first contact and demographic and intergenerational characteristics associated with different service responses to self-harm.
Methods:
Participants were 91,597 adolescents for whom multi-agency linked data were available in a longitudinal study of a population cohort in New South Wales, Australia. Self-harm and suicide-related incidents from birth to 18 years of age were derived from emergency department, inpatient hospital admission, mental health ambulatory, child protection and police administrative records. Descriptive statistics and binomial logistic regression were used to examine patterns of service contacts.
Results:
Child protection services recorded the largest proportion of youth with reported self-harm and suicidal ideation, in which the age of first contact for self-harm was younger relative to other incidents of self-harm recorded by other agencies. Nearly 40% of youth with a health service contact for self-harm also had contact with child protection and/or police services for self-harm. Girls were more likely to access health services for self-harm than boys, but not child protection or police services.
Conclusion:
Suicide prevention is not solely the responsibility of health services; police and child protection services also respond to a significant proportion of self-harm and suicide-related incidents. High rates of overlap among different services responding to self-harm suggest the need for cross-agency strategies to prevent suicide in young people.
Keywords
Suicide is one of the top five leading causes of death in young people worldwide (World Health Organization, 2018a; Centers for Disease Control and Prevention [CDC], 2020). In Australia, suicide rates are particularly high among young males, Aboriginal and Torres Strait Islander people, and people living in regional and socio-economically deprived communities (Productivity Commission, 2020). Suicide prevention efforts require information about risk of death by suicide (Suicide Prevention Australia, 2022b), such as suicidal ideation (thoughts about wanting to die) and self-harm, including non-suicidal self-harm (self-injury or self-poisoning without intent to die) and suicide attempts (self-injury or self-poisoning with intent to die; Ribeiro et al., 2016). Importantly, self-harm behaviours often cluster with other health risk behaviours (e.g. drug and alcohol use; Noel et al., 2013) making them important targets for intervention.
The number of hospital presentations for suicidal ideation in young people has increased substantially over the past decade in Australia (Sara et al., 2022) and hospital presentations for self-harm have increased globally (Plener, 2021; Spiller et al., 2020). It is estimated that around 10% of adolescents report self-harm, but only about one in eight of those that report self-harm in the community present to hospital with self-harm (Hawton et al., 2012); hospital-treated self-harm may thus represent only the ‘tip of the iceberg’, with most self-harm not coming to the attention of health services (Geulayov et al., 2018; McMahon et al., 2014). Indeed, police and child protection services can also be involved in responding to incidents related to suicide and self-harm in young people.
Understanding patterns of service contact for self-harm and suicidal ideation across multiple agencies is therefore important to identify opportunities to reduce risk of repeat self-harm and prevent deaths by suicide. Research into self-harm has predominately examined continuity of contacts with different types of health services (e.g. Kammer et al., 2021; Spittal et al., 2016). While it is known that rates of self-harm and suicide are higher among children in contact with child protection services (Katz et al., 2011), with a recent Australian study reporting that 70% of adolescents with self-harm hospitalisations had a history of child protection involvement (Leckning et al., 2021), little is known about the experience of children who are referred to child protection services specifically because they are self-harming or at risk of suicide. One study in Canada found that, among children known to child protection services, those who reported self-harm or suicidal ideation were more likely to be referred to mental health services than peers who did not report self-harm or suicidal ideation (Baiden and Fallon, 2018); however, the scale of child protection involvement in self-harm at a population level is not well understood. Furthermore, police services are increasingly responding to incidents of self-harm, although predominantly for adult cases involving violence and/or weapons (Chidgey et al., 2019), with limited research on police contact for self-harm in young people.
The overall aim of this study was to describe patterns of service contact for self-harm or suicidal ideation among children and adolescents in New South Wales (NSW), using ~18 years of longitudinal multi-agency record data for a population cohort of adolescents represented in the New South Wales Child Development Study (NSW-CDS). Specific aims were to: (1) examine the overlap and sequence of service contacts between health services (emergency department, inpatient hospital admissions, and ambulatory mental health services) and social services (child protection and police); (2) describe the patterns of age of first contact for self-harm or suicidal ideation across these different services, and; (3) examine the associations of demographic, community and intergenerational factors with service contacts for self-harm or suicidal ideation.
Method
Participants
Participants were 91,597 young people for whom multi-agency data were collated within the NSW-CDS (http://nsw-cds.com.au/) Wave 3 linkage, which was conducted in 2021 for a population cohort of individuals born between 2002 and 2005 (Carr et al., 2016; Green et al., 2018). Parental records were available for 75,784 young people whose births were registered in NSW. Record linkage was conducted by the Centre for Health Record Linkage (www.cherel.org.au), with an estimated false positive linkage rate of 0.5%. Ethical approval was obtained from the NSW Population and Health Services, Australian Capital Territory (ACT) Health and ACT Calvary Health Research Ethics Committees (HREC/18/CIPHS/49).
Self-harm and suicidal ideation
Health services
Incidents of self-harm or suicidal ideation from health records (2000–2021) were identified in the NSW Ministry of Health or ACT Health’s Emergency Department and Admitted Patient Data Collections and the NSW Mental Health Ambulatory Data Collection, defined as any instance of the International Classification of Disease, revision 10 (Australian Modification; ICD-10-AM) codes (or Systematized Nomenclature of Medicine [SNOMED] codes converted to ICD-10-AM codes) X60-X84, R45.81, R45.851, T14.91 or Y87.0. These health records were also used to determine mental disorder diagnoses among the youth cohort from any instance of ICD-AM codes F00-F99.
Child protection
Incidents of self-harm or suicide risk from child protection records were identified in the NSW Department of Communities and Justice ChildStory (2000–2020) database. Each child protection report is associated with a primary reported issue type; incidents were classified as relating to self-harm/suicide if the primary reported issue was: ‘C/YP [child or young person] self-harming behaviour’, ‘Risk: suicide risk – child’, ‘suicide risk for child’ or ‘C/YP at risk due to own behaviour – serious self-harming behaviour/risk taking behaviour’.
Police
Incidents related to either inflicting self-harm, attempting/threatening suicide or completing suicide, where the individual was categorised as either a ‘victim’ or ‘person of interest’, were identified in the NSW Police Force Computerised Operational Policing System (COPS; 2000–2021). The COPS data contain records of all criminal (e.g. assault, robbery) and non-criminal (e.g. traffic checks, criminal justice system checks) incidents and events reported to, or detected by, the NSW Police Force. In these records, a ‘victim’ is a person who suffers harm as a direct result of an act committed by another person during a criminal or non-criminal incident or offence, and ‘a person of interest’ is an individual who has not necessarily been arrested or formally accused of a crime but is of interest to the police during their investigation. Most incidents related to self-harm recorded in police records were categorised as ‘victim’ incidents, with n < 15 categorised as ‘person of interest’ incidents; all incidents classified as ‘person of interest’ were related to completed suicides. Notably, these records do not allow suicidal ideation to be identified explicitly and do not include other categories of police contact such as children at-risk (i.e. where there is risk of harm requiring mandatory reporting) or other positive police contacts.
Mortality records
Deaths by suicide were identified in the Australian Coordinating Registry’s (on behalf of Australian Registries of Births, Deaths and Marriages; Australian Coroners; and the National Coronial Information System) Cause of Death Unit Record File (COD-URF), using the ICD-10-AM codes X60-X84 or Y87.0. The COD-URF contains information on all deaths registered by the coroner at the conclusion of their inquiry; records were available for deaths that occurred in December 2019 or before (participants’ age ~14 to ~16 years).
Demographic factors
Each child’s sex was determined as that most frequently reported across all record sources, and Aboriginal and/or Torres Strait Islander background was designated for the child if indicated in any record for either the child or their parent(s). An individual’s age at first self-harm or suicidal ideation incident was calculated using information available on the month/year of birth and date of first recorded self-harm/suicidal ideation in any data collection.
Community factors
Socio-economic disadvantage and remote/regional location were based on home postcode recorded at birth (retrieved from the NSW Registry of Births, Deaths and Marriages or the NSW or ACT Perinatal Data Collections, available for 76,349 individuals). A binary indicator of socio-economic disadvantage reflected membership in the lowest quintile of the Socio-economic Indexes for Areas (vs quintiles 2–5), using the Index for Relative Socio-economic Disadvantage (SEIFA IRSD; Pink, 2013). Remote/regional location was determined using the Accessibility and Remoteness Index for Australia (ARIA; Department of Health and Aged Care [Australian Government], 2001), defined as membership in classes 2–5 (inner regional-very remote) vs class 1 (major cities). In addition, we examined the ARIA classes categorically (Supplementary Table 1).
Intergenerational factors
A binary indicator of any parental (i.e. mother and/or father) history of offending was derived from the NSW Bureau of Crime Statistics and Research Reoffending Database (1994–2018), which includes information on all finalised court appearances since 1994 for all individuals convicted of at least one offence. A binary indicator of parental mental disorder was derived from NSW or ACT (2000–2021) emergency department and admitted patient and NSW mental health ambulatory records, based on any incidence of ICD-10-AM codes for specific mental disorders or self-harm (F00-F99, X60-X84, R45.81, R45.851, T14.91 or Y87.0).
Analysis
Analyses were performed in RStudio version 1.3.1093 using R version 4.0.3. Descriptive statistics were calculated to describe the sequence and overlap among different types of service contact, as well as age at first service contact, for self-harm or suicidal ideation. Binary logistic regression was used to estimate the association between demographic, community and intergenerational factors with service use for self-harm or suicidal ideation (for any service contact and for each of the five services individually). Analyses resulted in odds ratios (ORs) with 95% confidence intervals (CIs) as measures of effect size, with ORs of 1.00–1.49 interpreted as small, 1.50–2.49 as medium and 2.50 or more as large (Rosenthal, 1996). Results were considered statistically significant when 95% CIs did not include 1.
Results
Descriptive statistics
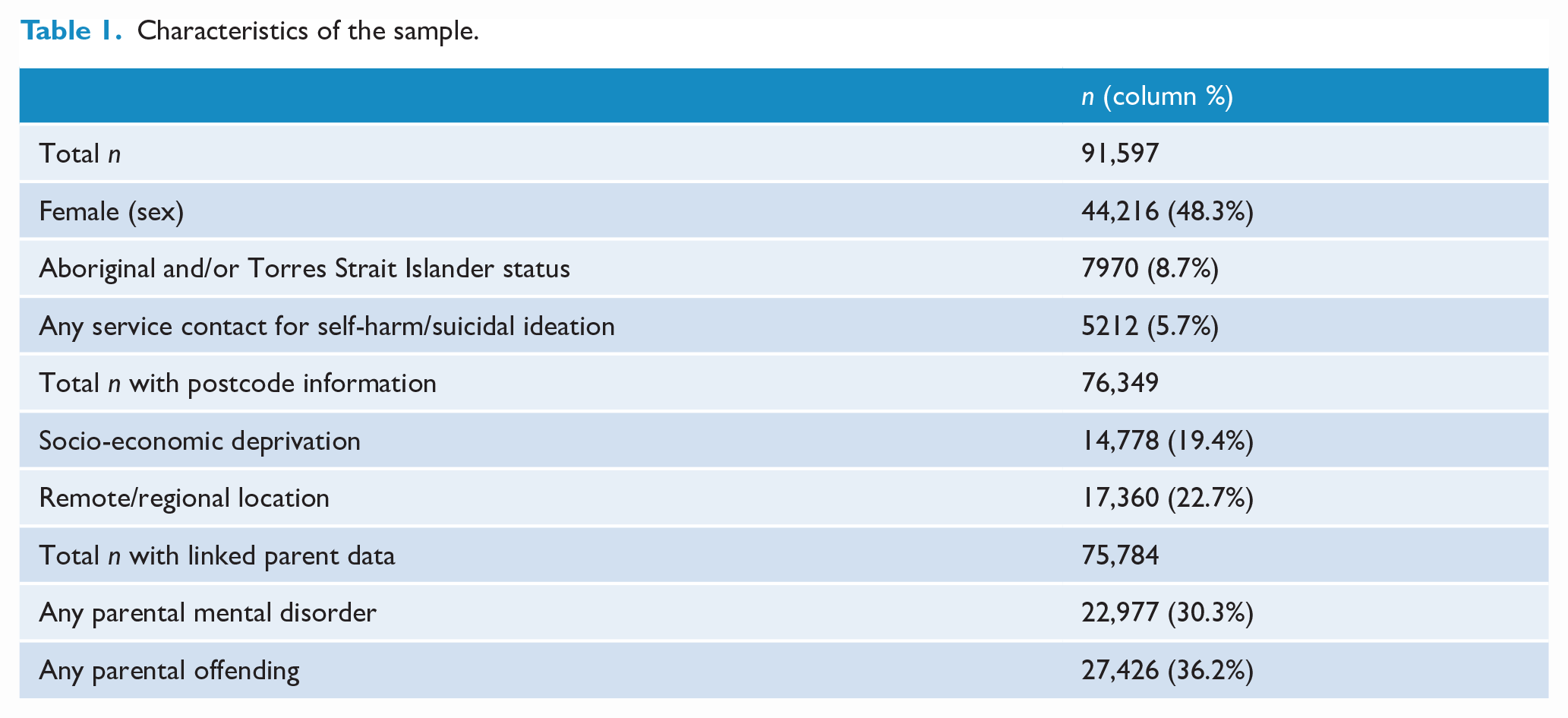
Sample characteristics are presented in Table 1. A total of 5212 young people (5.7% of the total sample) had any recorded service contact for a reported incident of self-harm or suicidal ideation. Fewer than 15 young people had a suicide-related cause of death recorded in coroner’s records and were therefore not analysed further. The most common type of service contact for reported self-harm or suicidal ideation was child protection services, followed by the emergency department (Table 2). Child protection services also had the highest proportion of first contacts.
Characteristics of the sample.
Frequencies of youth with any service contact, various modes of service contact and first service contacts for self-harm/suicidal ideation (n = 91,597).
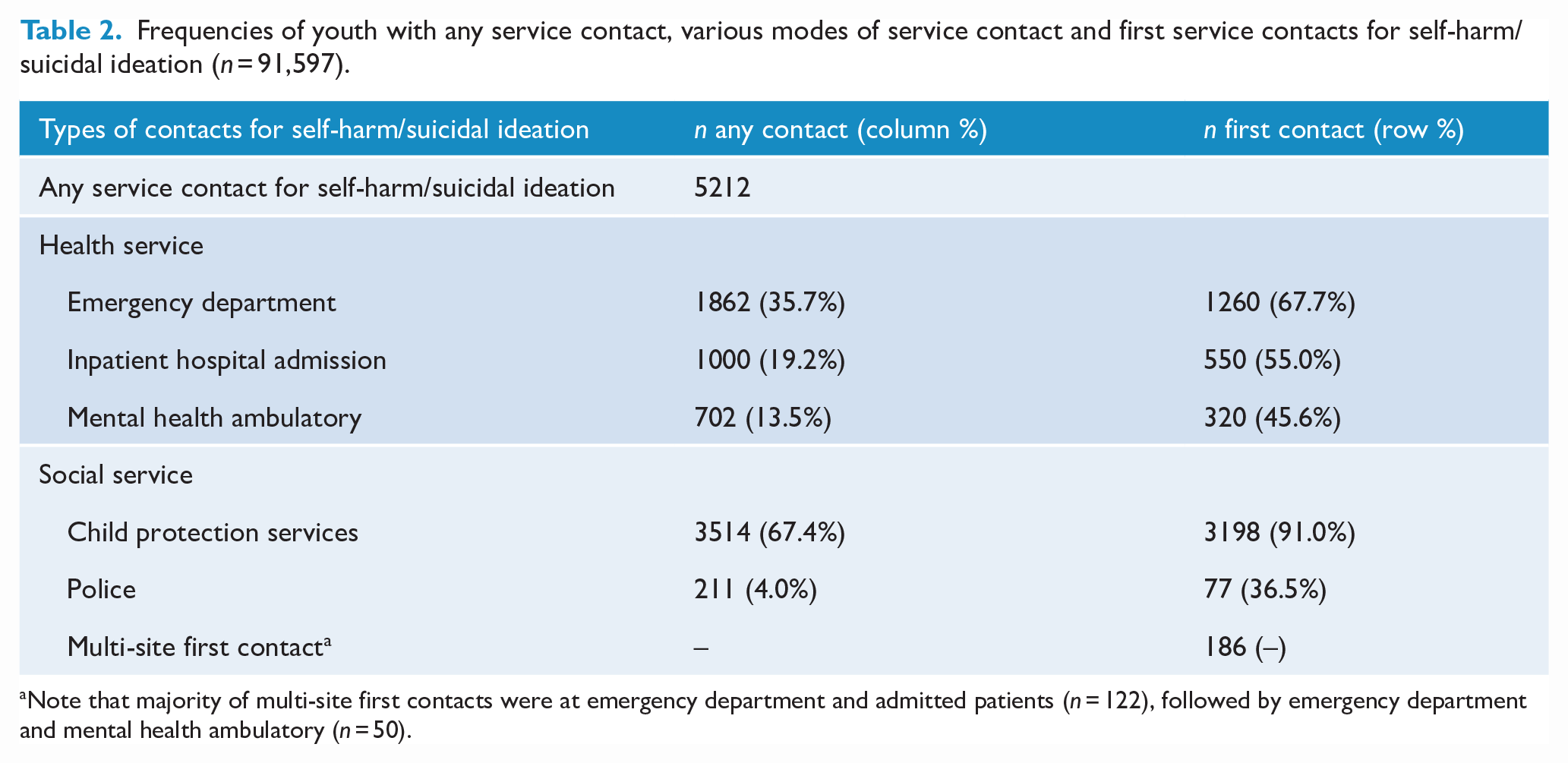
Note that majority of multi-site first contacts were at emergency department and admitted patients (n = 122), followed by emergency department and mental health ambulatory (n = 50).
Among young people with health service contact for self-harm or suicidal ideation, the most common reason was suicidal ideation (n = 2119), followed by intentional self-poisoning with a drug (n = 569) and intentional self-harm with a sharp object (n = 265; Supplementary Table 2). Of those with any service contact for reported self-harm or suicidal ideation, approximately half (n = 2701; 51.9%) had a prior health service contact for a mental disorder; most commonly mental disorders not otherwise specified (n = 1071; 20.5%), followed by neurotic disorders (n = 580, 11.1%; Supplementary Table 3).
Overlap and sequence of service contacts for self-harm or suicidal ideation
Of 2559 young people with health service contact for self-harm or suicidal ideation, almost a third (n = 805; 31.4%) had contact with at least two types of health services (Figure 1). Furthermore, 37.6% (n = 962) of those with health service contact also had contact with child protection and/or police for self-harm or suicidal ideation. Almost three quarters of young people with police contact for self-harm or suicidal ideation also had contact with health and/or child protection services (n = 153 of 211; 72.5%), while approximately a quarter of adolescents who had contact with child protection for reported self-harm or suicidal ideation had contact with another type of service (n = 954 of 3514; 27.1%).
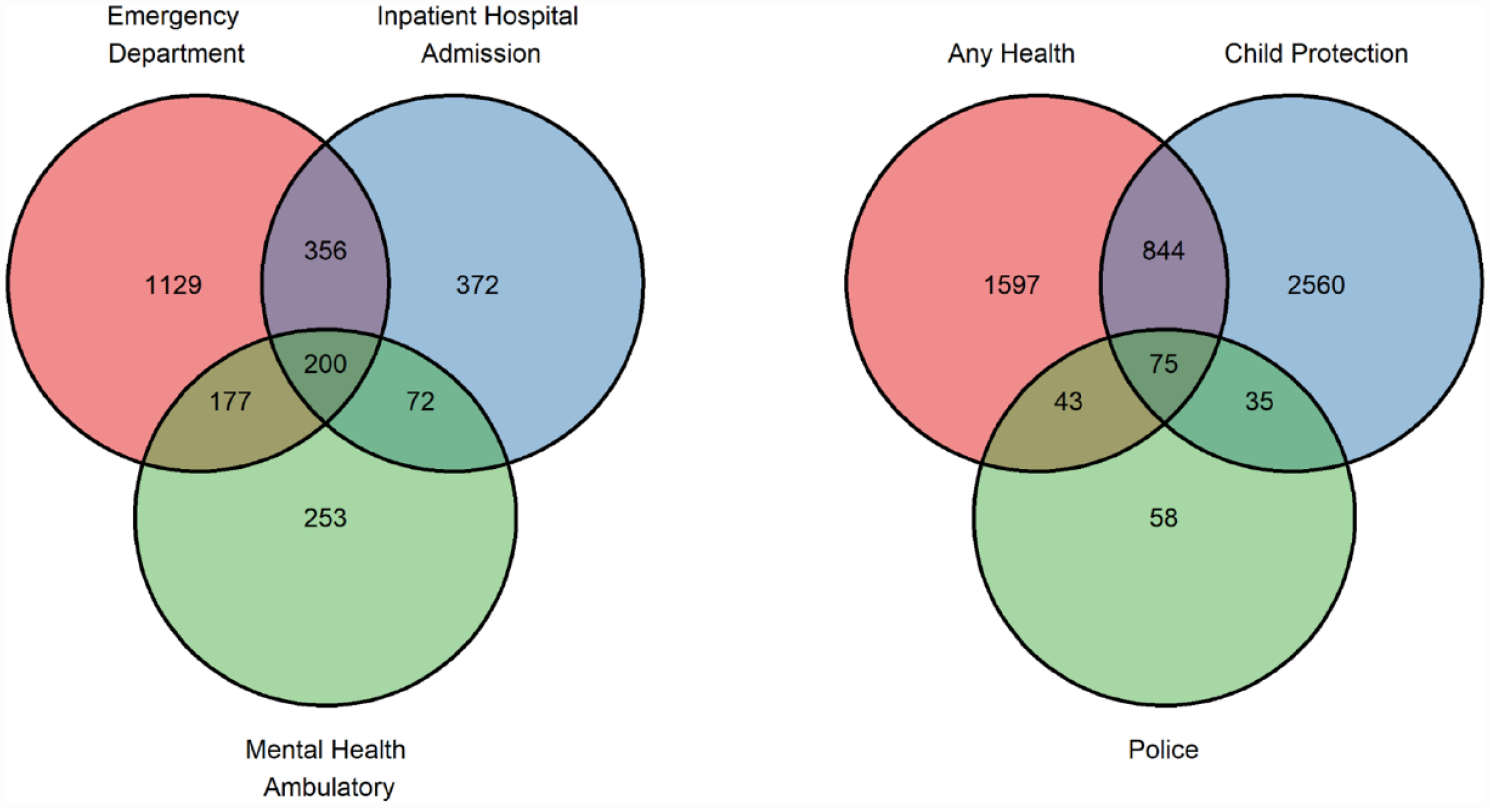
Overlap between service contacts for self-harm/suicidal ideation at (1) the three types of health services and across (2) health, child protection and police services (n = 91,597).
Among young people with any child protection contact for reported self-harm or suicidal ideation, 28.2% also had contact with health services for these issues; specifically, 17.2% (n = 603) had health service contact following the child protection contact, and 9.0% (n = 316) had health service contact for self-harm or suicidal ideation prior to the child protection contact; when health service contact followed the child protection contact, there was an average of 349 days (standard deviation [SD] = 417 days) between contacts (Table 3). For those with any police contact for self-harm or suicidal ideation, 56.3% also had contact with health services for these issues; specifically, 45.5% (n = 96) had health service contact prior to the police contact, and only 10.7% (n = 22) had health service contact after the police contact; for these latter adolescents, there was an average of 753 days between contacts (SD = 607 days).
Sequence of service use of health services and social services for self-harm/suicidal ideation (n = 91,597).
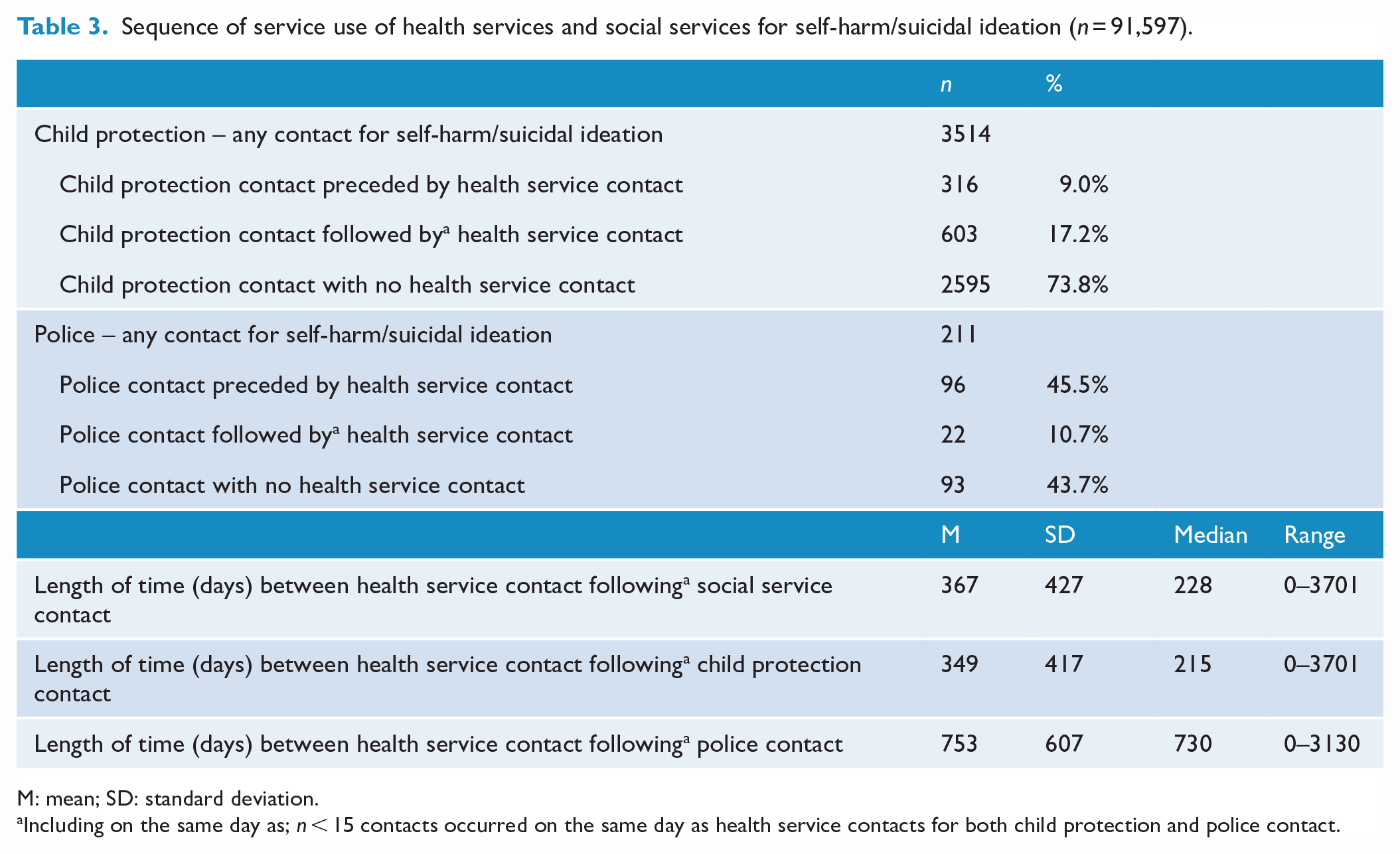
M: mean; SD: standard deviation.
Including on the same day as; n < 15 contacts occurred on the same day as health service contacts for both child protection and police contact.
Age at first service contact for self-harm or suicidal ideation
Patterns of age at first service contact for self-harm or suicidal ideation from 0 to 17 years are displayed in Figure 2 for all participants. Across all services, age of first contact for self-harm was the youngest for child protection services (mean (M) = 13.8 years; SD = 2.8 years), and the oldest for police contacts (M = 16.7 years; SD = 0.5 years), on average. The three health services each had a similar average age at first contact: emergency department (M = 14.8 years; SD = 1.6), inpatient hospital admission (M = 14.8 years; SD = 1.7 years) and mental health ambulatory services (M = 14.5 years; SD = 1.7 years).
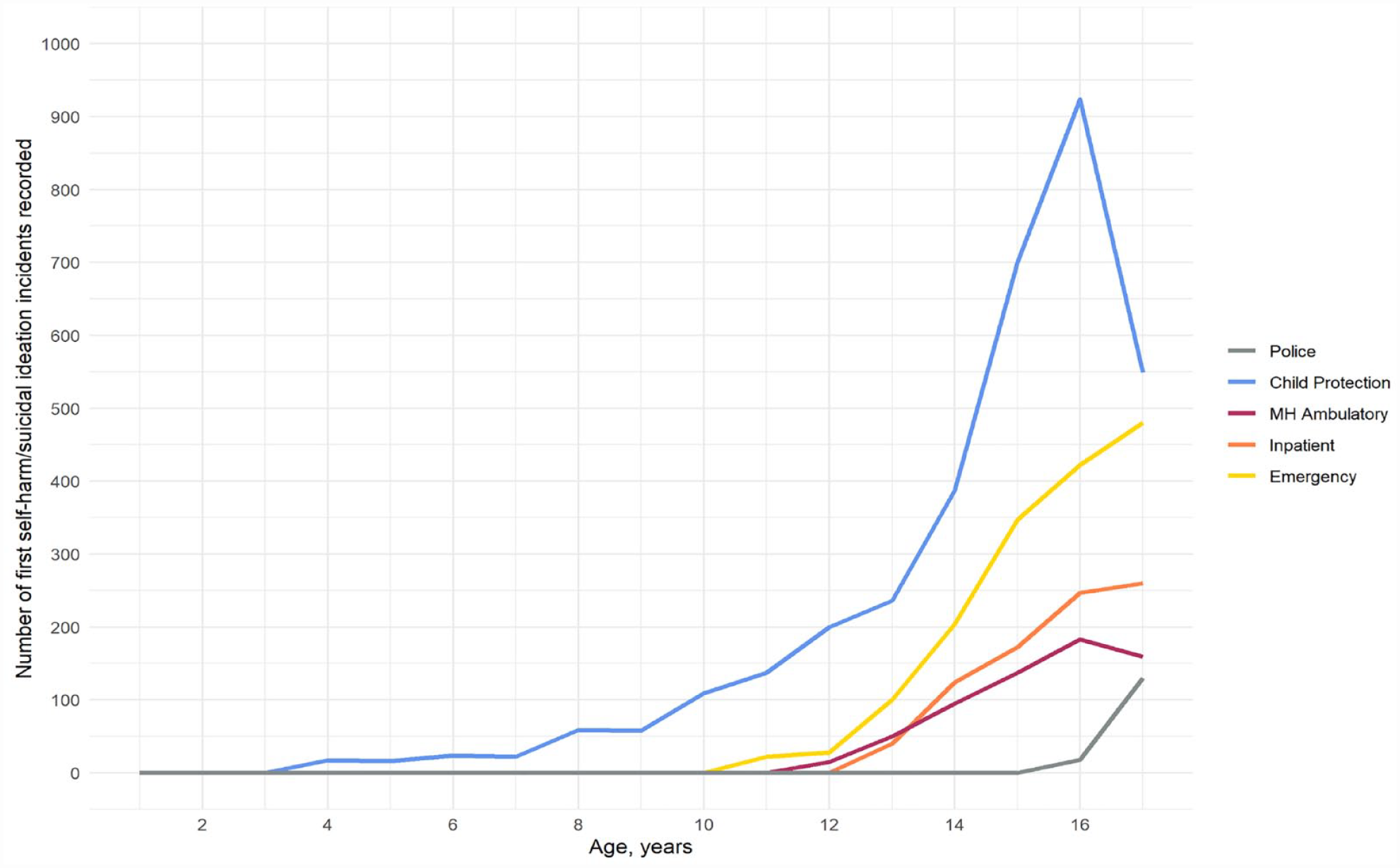
Age (in years) at first service contact (within each service) for self-harm/suicidal ideation (n = 91,597).
Associations with demographic, community and intergenerational factors
All demographic, community and intergenerational factors were associated with any service contact for self-harm or suicidal ideation (Table 4). Female sex was associated with increased likelihood of service contact with all three health services, with a large-sized effect for the association with inpatient hospital admission, medium-sized effects for associations with emergency department and mental health ambulatory services. Sex was not associated with child protection or police service contact for self-harm or suicidal ideation. Young people of Aboriginal and/or Torres Strait Islander background were at greater likelihood of contact with all five types of services compared to non-indigenous youth, with large-sized effects. Socio-economic deprivation was associated with emergency department contact (small effect size) and with child protection contact (medium effect size), but not with inpatient hospital admissions, mental health ambulatory services or police contact. Remote/regional location was associated with increased likelihood of contact with all service types for self-harm or suicidal ideation (of small- to medium-sized effects) except for police contact. Youth with parental history of a mental disorder were at greater likelihood of contact with all five types of services for self-harm or suicidal ideation, compared to their peers, with medium- to large-sized effects. Parental offending was also associated with all types of service contact for self-harm or suicidal ideation, with medium- to large-sized effects. For both parental mental disorder and parental offending, the largest point estimates for associations were with child protection contact.
Frequencies and unadjusted odds ratios (with 95% confidence intervals) for associations between self-harm/suicidal ideation and demographic (n = 91,597), community (n = 76,349) and intergenerational factors (n = 75,784).
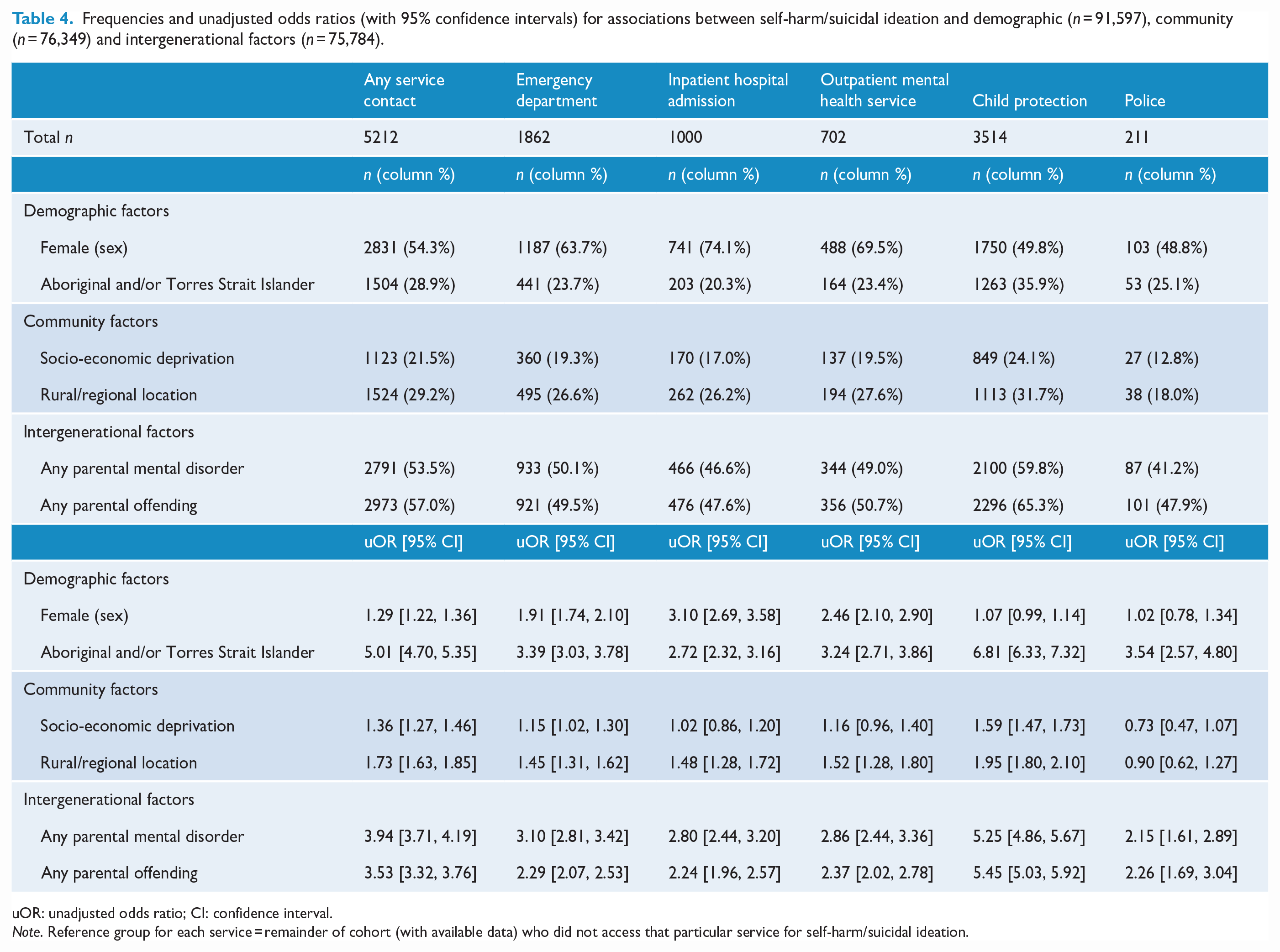
uOR: unadjusted odds ratio; CI: confidence interval.
Note. Reference group for each service = remainder of cohort (with available data) who did not access that particular service for self-harm/suicidal ideation.
Discussion
In this population-based study of service-use patterns for self-harm or suicidal ideation across the first 18 years of life, reported incidents of self-harm or suicidal ideation were most frequently recorded by child protection services among all other health and social service agencies. Child protection services also recorded the highest proportion of first contacts for self-harm or suicidal ideation, at the youngest ages, among all of these human service agencies. While these findings may, in part, reflect differences in methods of recording self-harm and suicidal ideation between agencies, they provide new information to inform cross-agency early intervention services. The majority (73.8%) of youth with reported self-harm or suicidal ideation in child protection records did not have any contact with health services for these conditions. While contact with police for self-harm or suicidal ideation was rare, 43.7% of young people with police contact had no contact with health services for self-harm or suicidal ideation. There were differential associations between demographic characteristics and types of service use; notably, girls were more likely than boys to access health services for self-harm or suicidal ideation.
There was a high degree of overlap between different types of service contacts, with ~40% of youth who had a secondary health service contact for self-harm or suicidal ideation also having contact with child protection services and/or police specifically for self-harm or suicidal ideation. Child protection records contained the largest proportion (nearly 70%) of young people with reported self-harm or suicidal ideation among all service types; however, only around a quarter of young people with child protection contact for self-harm or suicidal ideation also had health service contact. To our knowledge, the prevalence of child protection contacts for self-harm or suicidal ideation has not been previously demonstrated, and this finding suggests that research and policy that focuses on health agencies as primary providers of services for self-harm is overlooking a significant population of youth whose self-harm or suicidal ideation is reported to child protection but not health services. In contrast, while only 211 youth had police contact for self-harm or suicidal ideation, a larger proportion of these children (~56%) also had a health service contact.
The age at first contact with each health service for self-harm or suicidal ideation was largely similar, with records being rare before age 12 years, and then increasing during adolescence, consistent with previous reports of hospital-treated self-harm (Hawton et al., 2012). Police contact for self-harm or suicidal ideation was rare before age 16 years, at which point the number of contacts began increasing. In contrast, child protection services contact for self-harm or suicidal ideation started earliest among the service types and increased sharply between ages 13 and 16 years, at which point they began steeply declining; this likely reflects the lower involvement of child protection in general with this age group (Australian Institute of Health and Welfare, 2022), rather than a drop off in self-harm or suicidal ideation per se.
Demographic, community and intergenerational factors were differentially associated with service use for self-harm or suicidal ideation. Girls were more likely than boys to access all types of secondary health services for self-harm or suicidal ideation, consistent with previous research (e.g. De Leo and Heller, 2004; Marchant et al., 2020; Schmidtke et al., 1996). However, sex was not associated with child protection or police contacts for self-harm or suicidal ideation. This challenges the dominant view, largely borne out of health service data, that self-harm is predominantly an issue affecting girls (Bresin and Schoenleber, 2015) and instead suggests that boys may be primarily alerted to social services rather than health services for self-harm and suicidal ideation. Furthermore, young people living in socio-economically deprived areas were more likely than their more advantaged peers to be recorded in child protection and emergency department services for self-harm or suicidal ideation, but not inpatient hospital, mental health ambulatory or police services. The association between emergency department services for self-harm and suicidal ideation and socio-economic deprivation is consistent with the previous research (Rudge et al., 2013); this finding, and the association between socio-economic deprivation and child protection services, may reflect reduced access to primary health care by those in lower socio-economic strata (Lowthian et al., 2011).
The remaining four demographic, community and intergenerational factors (Aboriginal and/or Torres Strait Islander background, remote/regional location, parental offending and parental mental disorder) were significantly associated with all types of service contact (except for the association between remote/regional location and police contact), indicating their influence in increasing risk of self-harm or suicidal ideation in general but not a particular type of service contact. This extends previous findings of associations between all four of these factors and health service contact for self-harm (Dickson et al., 2019; Harrison and Henley, 2014; Mitchell et al., 2018; Mok et al., 2016; O’Hare et al., 2022) by showing that they are also associated with social service contact for self-harm. The high likelihood of service contact for self-harm among Aboriginal and/or Torres Strait Islander youth is likely influenced by the on-going impacts of colonisation, including social marginalisation, intergenerational trauma and individual/community-level psychological distress (Hunter and Milroy, 2006). This suggests a need for child protection, police, health services and Aboriginal community-controlled organisations to work together to promote culturally safe support for youth.
The findings should be interpreted with consideration of several limitations. First, the assessment of self-harm and suicidal ideation was not necessarily equivalent among health and social services due to differences in the systems used to record information (affecting the detail with which it is recorded), when the information is recorded, and the threshold for recording an incident. Most significantly, child protection services record the issue as reported to them by a third party, while the information recorded in health and police records followed direct interaction with the individual. Administrative records from different agencies may therefore differentially estimate the prevalence of self-harm and suicidal ideation; specifically, child protection reports may capture a greater prevalence of self-harm/suicidal ideation events in comparison to health and police records. In addition, the nature of administrative data means that there is no means of externally validating the self-harm and suicidal ideation incidents, and there may be different interpretations of what should be recorded as a self-harm or suicidal ideation incident by those recording these incidents in non-health settings. Second, we used a broad, heterogeneous index of self-harm and suicidal ideation/behaviour as it was not possible to distinguish suicidal intent from the available data. For example, child protection services recorded data pertaining to self-harm and suicidal ideation/behaviour using a broad category of ‘suicide risk’, whereas health services record distinct instances of self-harm or suicidal ideation specifically. While this limits the specificity of implications that can be drawn from these findings, a recent meta-analysis demonstrates little difference in risk for suicide among those engaging in suicidal ideation or self-harm (Large et al., 2021). Third, community factors were measured at the time of the individual’s birth and may not reflect the circumstances at the time of their self-harm or suicidal ideation incident. In addition, we were unable to account for emigration; as such, individuals who experienced a self-harm or suicidal ideation incident in another state or country would be misclassified as unexposed. Finally, our observations are limited to the five human service records reported here, despite a significant amount of self-harm or suicidal ideation likely to come to the attention of general practitioners, private mental health practitioners, school counsellors and community organisations.
These findings have important implications for policy. Child protection services record large numbers of youth with reported incidents of self-harm or suicidal ideation and are the most common first point of service contact for young people – at the earliest age – with records of self-harm in these NSW administrative data. Child protection services are also more common for boys, who are less likely than girls to present to health services for self-harm, but are known to be more likely to die by suicide (Hawton et al., 2012). Around one-fifth of young people with child protection service records of self-harm go on to receive secondary health services for self-harm (although more may see primary health services), with around a year (on average) between these child protection and health service contacts. Accordingly, child protection services could be a particularly important avenue for self-harm/suicide prevention initiatives. For example, specialised training for case workers to recognise self-harm or suicidal ideation could facilitate early detection and the consolidation of referral pathways between child protection and mental health services could improve timely access to appropriate care. Prior evidence suggests that hospital admission or physician visit after entry to out-of-home care significantly decreases risk of a suicide attempt by 73% (Katz et al., 2011). NSW currently has policy directives to mandate a primary health assessment for young people in out-of-home care (NSW Department of Communities and Justice, 2022), but this does not currently extend to those in contact with child protection who do not enter care. Police may also benefit from specialised training and consolidation of referral pathways. In general, our findings support the need for a ‘whole of government’ response, where suicide prevention efforts are integrated across agencies (Suicide Prevention Australia, 2022a). Other countries that have adopted integrated governmental responses to suicide prevention, such as Japan and the Republic of Ireland, have seen progressive declines in suicide rates (World Health Organization, 2018b).
In conclusion, the current findings suggest that self-harm and suicidal ideation in young people are not solely an issue for health services but also constitute a significant burden on social services. Young people with self-harm or suicidal ideation are, indeed, more likely to present to child protection services than to secondary health services. Child protection services and police need to be adequately resourced to respond appropriately to self-harm and suicidal ideation in children and adolescents. The large overlap between different types of service use for self-harm and suicidal ideation suggests a need for cross-agency interaction to develop strategies for delivering interventions for self-harm and population-level suicide prevention programmes.
Supplemental Material
sj-docx-1-anp-10.1177_00048674231179652 – Supplemental material for Self-harm and suicidal ideation among young people is more often recorded by child protection than health services in an Australian population cohort
Supplemental material, sj-docx-1-anp-10.1177_00048674231179652 for Self-harm and suicidal ideation among young people is more often recorded by child protection than health services in an Australian population cohort by Kirstie O’Hare, Oliver Watkeys, Kimberlie Dean, Stacy Tzoumakis, Tyson Whitten, Felicity Harris, Kristin R Laurens, Vaughan J Carr and Melissa J Green in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research used population data owned by the New South Wales (NSW) Department of Communities and Justice; NSW Ministry of Health; the Australian Capital Territory (ACT) Health; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); NSW Bureau of Crime Statistics and Research; NSW Department of Justice and NSW Police Force. The findings and views reported are those of the authors and should not be attributed to these Departments, or the NSW, ACT or Australian Governments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was conducted by the University of New South Wales with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (APP1148055) and Investigator Grant (APP1175408 awarded to K.D.) and the Australian Research Council (ARC) Future Fellowship (FT170100294 awarded to K.R.L.) and Discovery Early Career Researcher Award (DE210100113 awarded to S.T.).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.