
Abstract
Study Design
Ex vivo human cadaveric study.
Objective
The development or progression of adjacent segment disease (ASD) after spine stabilization and fusion is a major problem in spine surgery. Apart from optimal balancing of the sagittal profile, dynamic instrumentation is often suggested to prevent or impede ASD. Hybrid instrumentation is used to gain stabilization while allowing motion to avoid hypermobility in the adjacent segment. In this biomechanical study, the effects of two different hybrid instrumentations on human cadaver spines were evaluated and compared with a rigid instrumentation.
Methods
Eighteen human cadaver spines (T11–L5) were subdivided into three groups: rigid, dynamic, and hook comprising six spines each. Clinical parameters and initial mechanical characteristics were consistent among groups. All specimens received rigid fixation from L3–L5 followed by application of a free bending load of extension and flexion. The range of motion (ROM) for every segment was evaluated. For the rigid group, further rigid fixation from L1–L5 was applied. A dynamic Elaspine system (Spinelab AG, Winterthur, Switzerland) was applied from L1 to L3 for the dynamic group, and the hook group was instrumented with additional laminar hooks at L1–L3. ROM was then evaluated again.
Results
There was no significant difference in ROM among the three instrumentation techniques.
Conclusion
Based on this data, the intended advantage of a hybrid or dynamic instrumentation might not be achieved.
Keywords
Introduction
Spondylodesis with transpedicular screw fixation is widely used for the treatment of different spine pathologies. Yet a potential conflict exists between the immediate benefit and later consequences or complications of this technique. The term adjacent segment degeneration is used to describe radiologic changes seen at levels adjacent to a previous spine fusion, which do not necessarily correlate with any clinical findings. Adjacent segment disease (ASD) involves the development of new clinical symptoms that are compatible with radiographic changes adjacent to a previously fused segment. 1,2 Many studies have shown an accelerated degeneration of the segment adjacent to a fused level. 3 –7 Some authors have suggested a genetic predisposition as a main factor for developing ASD. 8,9 Biomechanical studies have shown increased mobility in adjacent segments after fusion. 10 –12 This mobility may be caused by a compensatory hypermobility in the adjacent segment due to the fusion. This hypermobility is even greater when intervertebral cages are used for fusion. 4,13,14 ASD may also be more likely to occur when the adjacent segment has already shown signs of degeneration at the time of the initial fusion. 15,16 Therefore, prophylactic dynamic stabilization of segments adjacent to a spondylodesis seems promising. The idea is to provide stability by reducing loads while allowing motion in the treated segments, which could reduce hypermobility and possibly hinder the progression of degeneration.
Several dynamic implants have been developed and assessed for their biomechanical efficacy throughout the last decade. 17 –21 In general, all devices appeared to reduce the range of motion (ROM) of the instrumented spine segment. However, the resulting stiffness of the dynamic segment was very close to a rigid fusion. 22 Also, a clinical benefit in terms of protecting the adjacent segment could not be shown. 23,24 The Elaspine system (Spinelab AG, Winterthur, Switzerland) is a pedicle screw device with an elastic polycarbonate urethane (PCU) rod for posterior dynamic stabilization (Fig. 1). In an initial biomechanical evaluation, the system is more flexible and allows a more physiologic motion closer to the intact functional spinal unit compared with the better-known Dynesys system (Zimmer Biomet, Warsaw, Indiana, United States). 21 Laminar hooks have not been evaluated in this context. The existing studies compare the pullout failure of hybrid instrumentations and pedicle screw-only constructs or the strains during loading. 25,26 In the present study, lumbar spinal motion using two different types of hybrid instrumentation was evaluated. A four-level rigid instrumentation was compared with a two-level rigid instrumentation connected with either a two-level dynamic Elaspine system or a two-level laminar hook instrumentation.
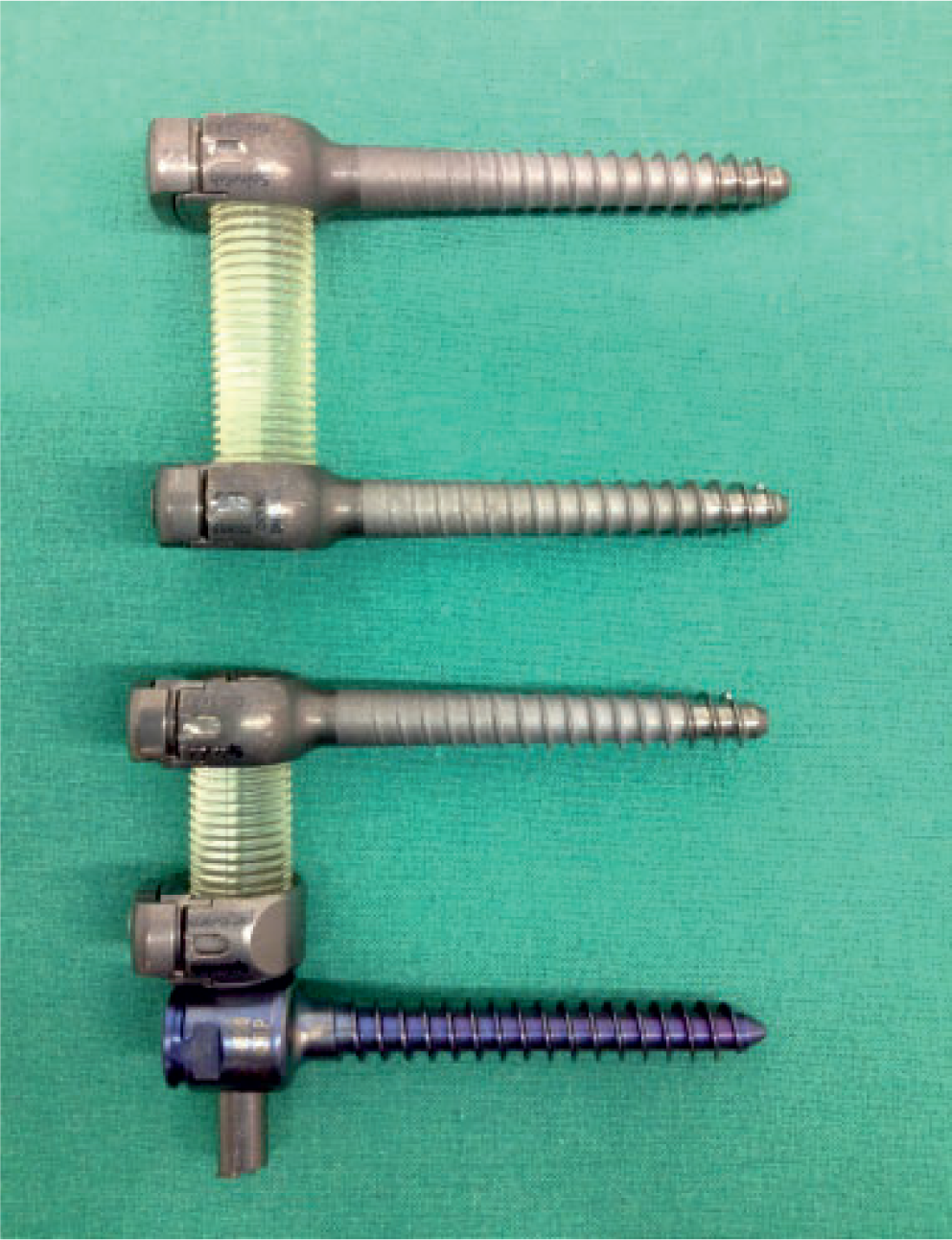
The Elaspine system (Spinelab AG, Winterthur, Switzerland) consisting of two monoaxial pedicle screws with an elastic polymer rod (upper implant) as well as an additional metal adapter (lower implant) required to connect a titanium rod to a polycarbonate urethane rod.
Materials and Methods
Eighteen human cadaveric spines with a mean age of 52.3 years (range, 40 to 63) were harvested, double-sealed, and stored at −22°C until testing day. Prior to testing, a quantitative computed tomography can (Somatom Definition Flash Siemens AG, Munich, Germany) was performed on each specimen to determine the apparent volumetric bone mineral density (BMD) and to screen for any pathologic condition or deformity. The exclusion criteria were a history of spinal surgery, trauma, or cancer involving the spine; deformity (i.e., scoliosis > 15 degrees); and age younger than 40 years or older than 65 years. The apparent BMD for each specimen was calculated using Avizo software (FEI Visualization Sciences Group, Burlington, Massachusetts, United States) by cropping a 25 × 25 × 25 voxel cube from the center of the T12, L1, and L2 vertebral bodies. The average Hounsfield unit value was scaled linearly to the reference densities of a QRM-BDC phantom (QRM GmbH, Moehrendorf, Germany) containing 0, 100, and 200 mg/mL calcium hydroxyapatite.
The specimens were divided into three experimental groups: rigid (group R), dynamic (group D), and hook (group H) based on the donor's age, body height, body weight, body mass index, and BMD. The baseline characteristics were similar among the test groups (Table 1). Prior to testing, the specimens were thawed overnight at 8°C. On the day of testing, specimens were prepared according to Wilke et al. 27 The soft tissue was dissected while leaving capsules of the facet joints, supporting structures, and ligaments intact. To reduce tissue degradation, the specimens were repeatedly sprayed with Ringer's solution during the entire preparation and testing period.
Spine donor demographics
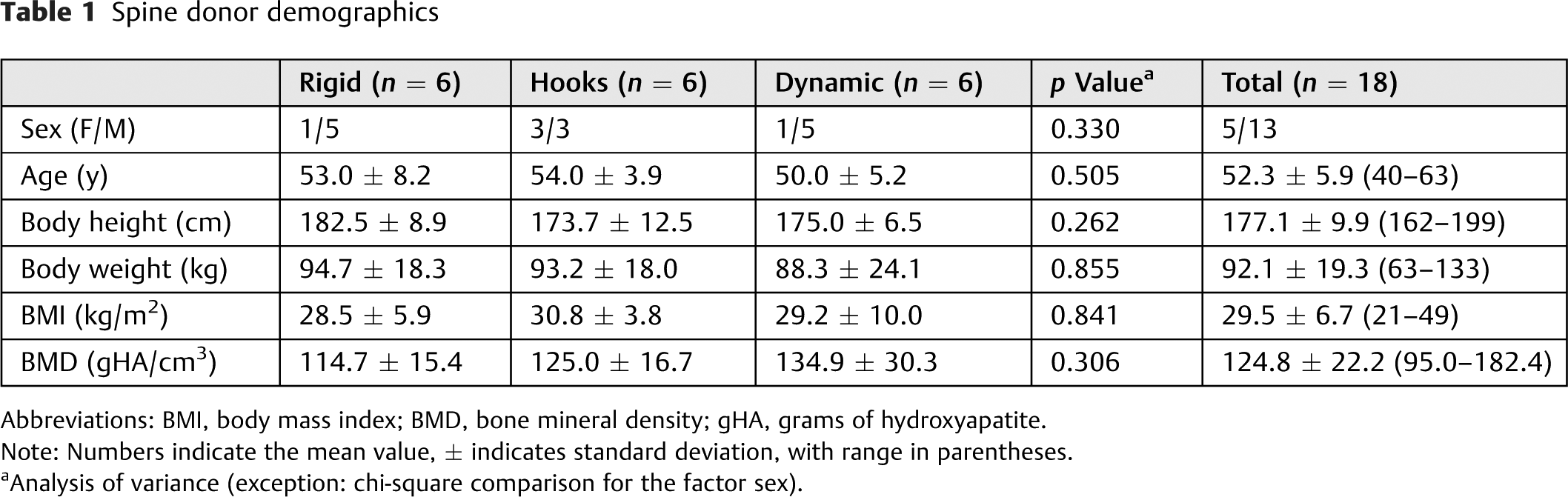
Abbreviations: BMI, body mass index; BMD, bone mineral density; gHA, grams of hydroxyapatite.
Note: Numbers indicate the mean value, ± indicates standard deviation, with range in parentheses.
a Analysis of variance (exception: chi-square comparison for the factor sex).
An experienced spine surgeon applied all instrumentations. Lateral and anteroposterior radiographs of each specimen were taken to ensure that proper positioning of the pedicle screws was achieved. Group R (Fig. 2) contained spine specimens fixed with an OCPS (OrthoCube Posterior Rod System) rigid four-segment (L1–L5) spinal rod instrumentation system (OrthoCube AG, Baar, Switzerland) consisting of self-tapping, conical, titanium pedicle screws (diameter: 5.5 to 7.2 mm; length: 40 to 55 mm) connected by a titanium alloy rod (diameter: 5.5 mm). Specimens of group D (Fig. 2) were fixed with OCPS rigid two-segment (L3–L5) instrumentation connected to a two-segment (L1–L3) dynamic Elaspine system consisting of self-tapping, titanium pedicle screws (diameter: 6.5 mm, length: 45 mm) connected by a semiflexible PCU rod (diameter: 10 mm). The PCU rod was directly linked to the conventional titanium rod via a rod adapter (Fig. 1). For group H, the spines were fixed with OCPS rigid two-segment (L3–L5) instrumentation connected to Expedium two-segment (L1–L3) laminar hook instrumentation (Depuy Synthes Inc., Raynham, Massachusetts, United States) including two supralaminar placed hooks on each side connected by a titanium alloy rod (diameter: 5.5 mm; Fig. 2). The specimen ends were embedded in Ureol Rencast FC 53 two-component polymer resin (Huntsman Advanced Materials GmbH, Basel, Switzerland) using custom-made casting containers for mounting in the spine testing device. The specimens were positioned such that a neutral posture was maintained and the L2–L3 lumbar disk was aligned horizontal to the embedding plates.
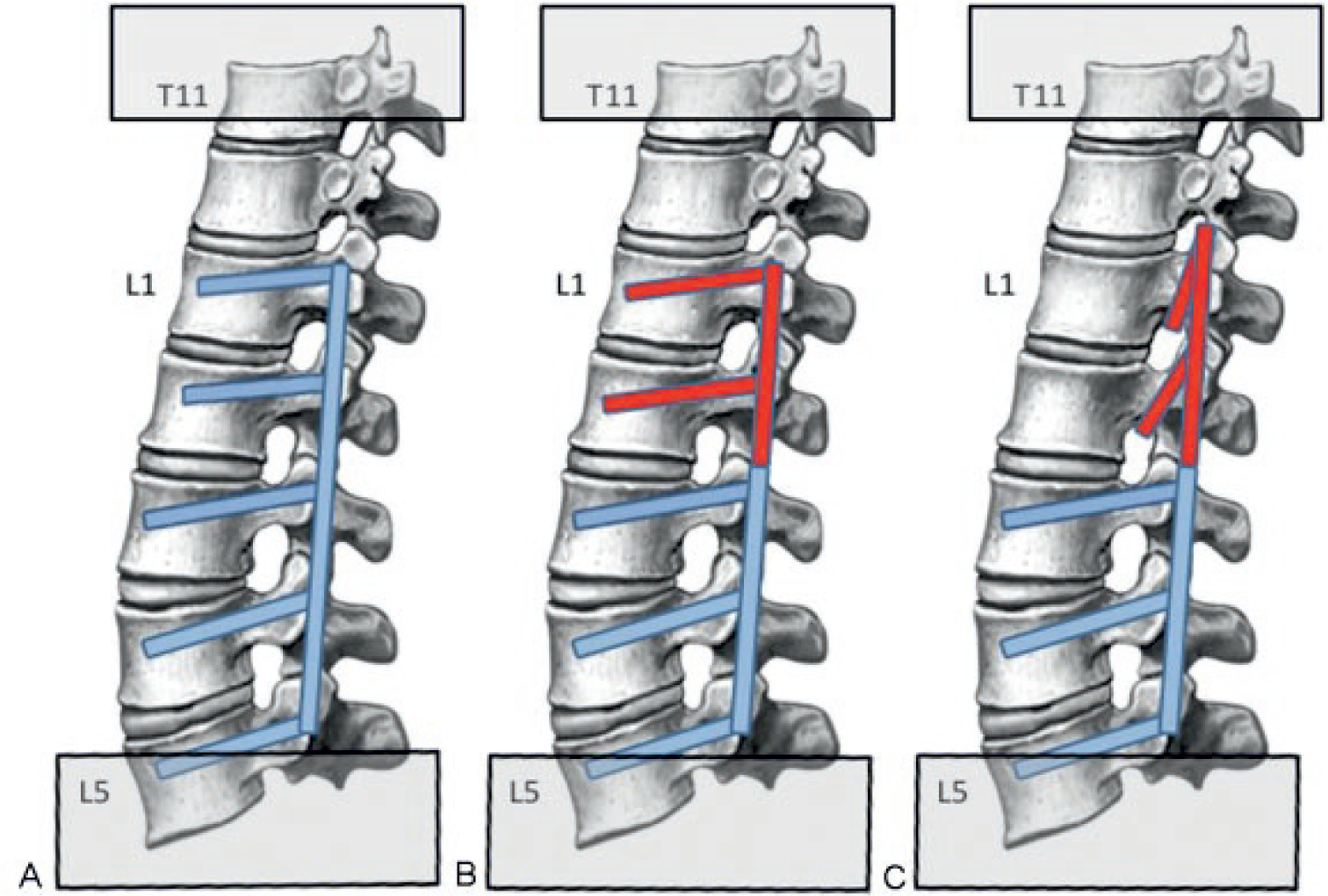
Schematic overview showing the setup of the three test groups. (A) Group R: four-level rigid instrumentation; (B) group D: two-level rigid instrumentation (L3–L5) combined with the Elaspine system (Spinelab AG, Winterthur, Switzerland) (L1–L3); and (C) group H: two-level rigid instrumentation (L3–L5) combined with laminar hooks (L1–L3).
Each specimen was mounted in an MTS Bionix servohydraulic material testing machine (MTS, Eden Prairie, Minnesota, United States) and underwent mechanical testing in two different configurations:
Two-segment rigid L3–L5 instrumentation (n = 18) Four-segment instrumentation subdivided into three groups (n = 6 each)
Prior to that, the similarity in mechanical behavior of the native spines was initially evaluated with solely pedicle screws implanted (n = 18).
A cranially located, driven rotational axis was used to impart five cycles of 5 degrees of extension and 5 degrees of flexion at a frequency of 0.1 Hz in angle control. The caudal rotational axis was held stable, and the vertical axis was set to maintain 0 N during the testing period by a cranially placed x-y table, which was free to move in the transverse plane. A caudally located six-degree-of-freedom load cell recorded all forces and moments.
A Vicon-460 motion capture system (Oxford Metrics Ltd., Oxford, UK) set at a frame rate of 102.4 Hz was used to measure the ROM of the whole spine as well as each segment. L-shaped sets of three reflective markers were attached to the head of each screw on the left side of the instrumentation (L1–L5), to the top embedding plate (T11), and to the bottom embedding plate (L5). Additionally, a pedicle screw with an L-shaped set of three reflective markers was implanted in T12. This screw was not included in the instrumentation but was necessary to measure segmental motion. For the segments L1–L3 that were fixed with the various types of instrumentation, an additional marker set was attached to the spinous processes of each vertebra. For group H, the markers attached to the spinous processes were used to measure ROM in the L1–L3 segments during the first and second test cycles, because the laminar hooks could not be fixed to the spine without the use of a titanium rod. Fig. 3 shows an exemplary experimental setup.
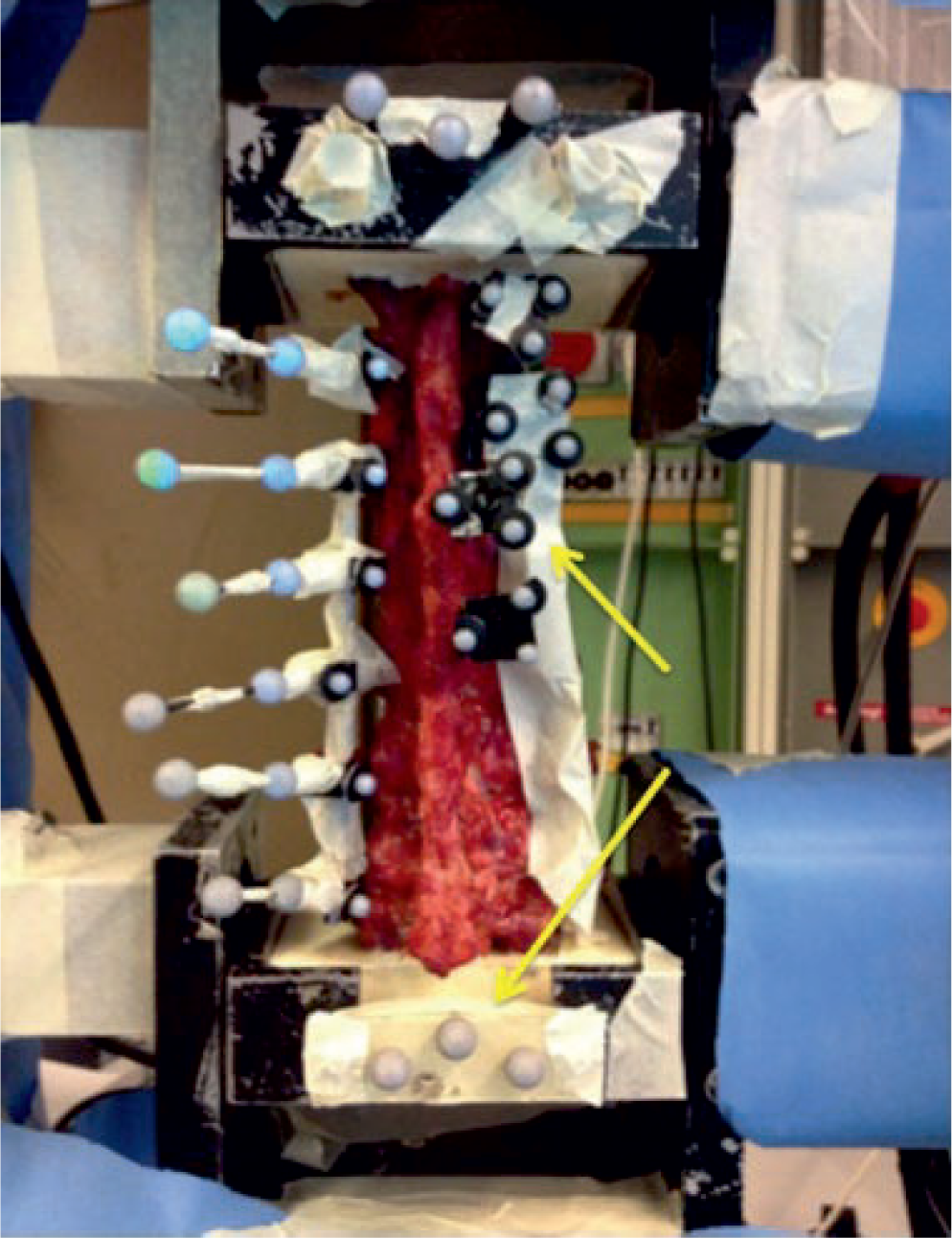
An example cadaveric spine specimen setup for range-of-motion measurements. Reflective markers are indicated by the arrows at the potting (top and bottom), screw heads, and/or hooks located at L1–L5 and spinous processes of T12–L3. All reflecting parts are covered to prevent interference with the motion capture system.
Segmental ROM data was evaluated during the third cycle and was used to determine the angular ROM (flexion and extension) for each spinal segment (i.e., T11–T12, T12–L1, L1–L2, L2–L3, L3–L4, and L4–L5). From the L-shaped three-marker sets mounted on each pedicle screw (L1–L5), a vector was defined from the central to the most posterior marker and then projected to the sagittal plane. For T11, the plane defined by the triangular three-marker set was calculated then projected to the sagittal plane. The segmental ROM was then defined as the angle measured between the sagittal projections of two adjacent levels. The segmental ROM between the native, two-segment rigid and the four-segment test groups (i.e., groups R, D, and H) were assessed using two-way analysis of variance with post hoc analysis. All statistical analyses were performed using SPSS Statistics Version 20 (IBM Corp., Armonk, New York, United States) with a type I error probability set to 5%.
Results
Table 2 shows the mean segmental ROM for each spinal segment in every instrumented condition. Comparing the native spines of each test group (i.e., groups R, D, and H, n = 6 per group), the spinal segments showed different ROMs within the specimens (p = 0.016). However, there were no significant differences among the three test groups (p = 0.978, power 0.053) or the interaction (p = 0.228, power 0.642). Looking more closely at the segments (post hoc, Bonferroni), only significant differences between T12–L1 and L1–L2 were found (p = 0.018).
Mean flexion–extension range-of-motion values for each spinal segment of the native, two-segment rigid, and the test groups
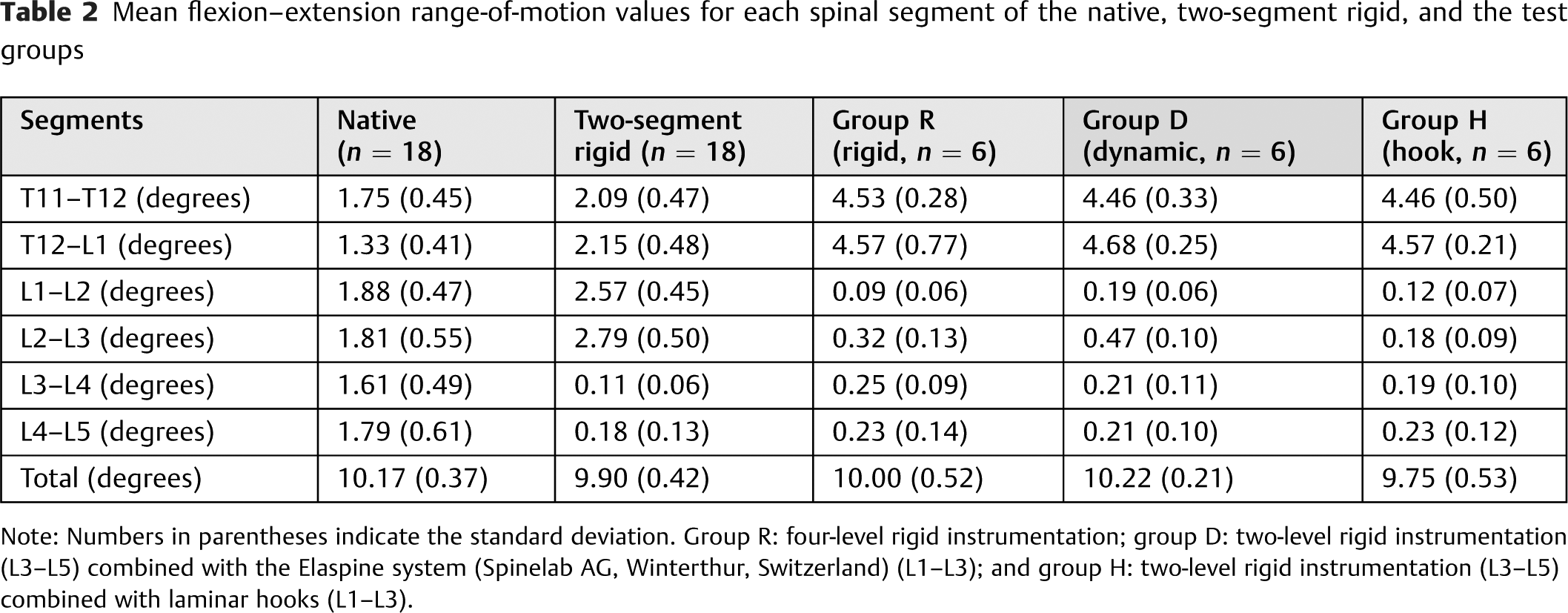
Note: Numbers in parentheses indicate the standard deviation. Group R: four-level rigid instrumentation; group D: two-level rigid instrumentation (L3–L5) combined with the Elaspine system (Spinelab AG, Winterthur, Switzerland) (L1–L3); and group H: two-level rigid instrumentation (L3–L5) combined with laminar hooks (L1–L3).
Pooling the data from the three test groups and comparing the native spines to the subsequently performed two-segment rigid instrumentation, a significantly reduced ROM of the instrumented segments compared with the native spine was observed (p < 0.001). The Tukey post hoc test spotted three homogeneous subsets consisting of the instrumented segments L3–L4 and L4–L5, the adjacent segments (L1–L2 and L2–L3), and the thoracic segments (T11–T12 and T12–L1). The adjacent segments cranial to the two-segment rigid instrumentation increased in ROM by +54% at L2–L3, +37% at L1–L2, +62% at T12–L1, and +19% at T11–T12.
Finally, comparing the segmental ROM of the three test groups (Fig. 4), no difference between the three instrumentation techniques (p = 0.454, power 0.182) and no interaction between instrumentation technique and segmental ROM could be found (p = 0.955, power 0.185).
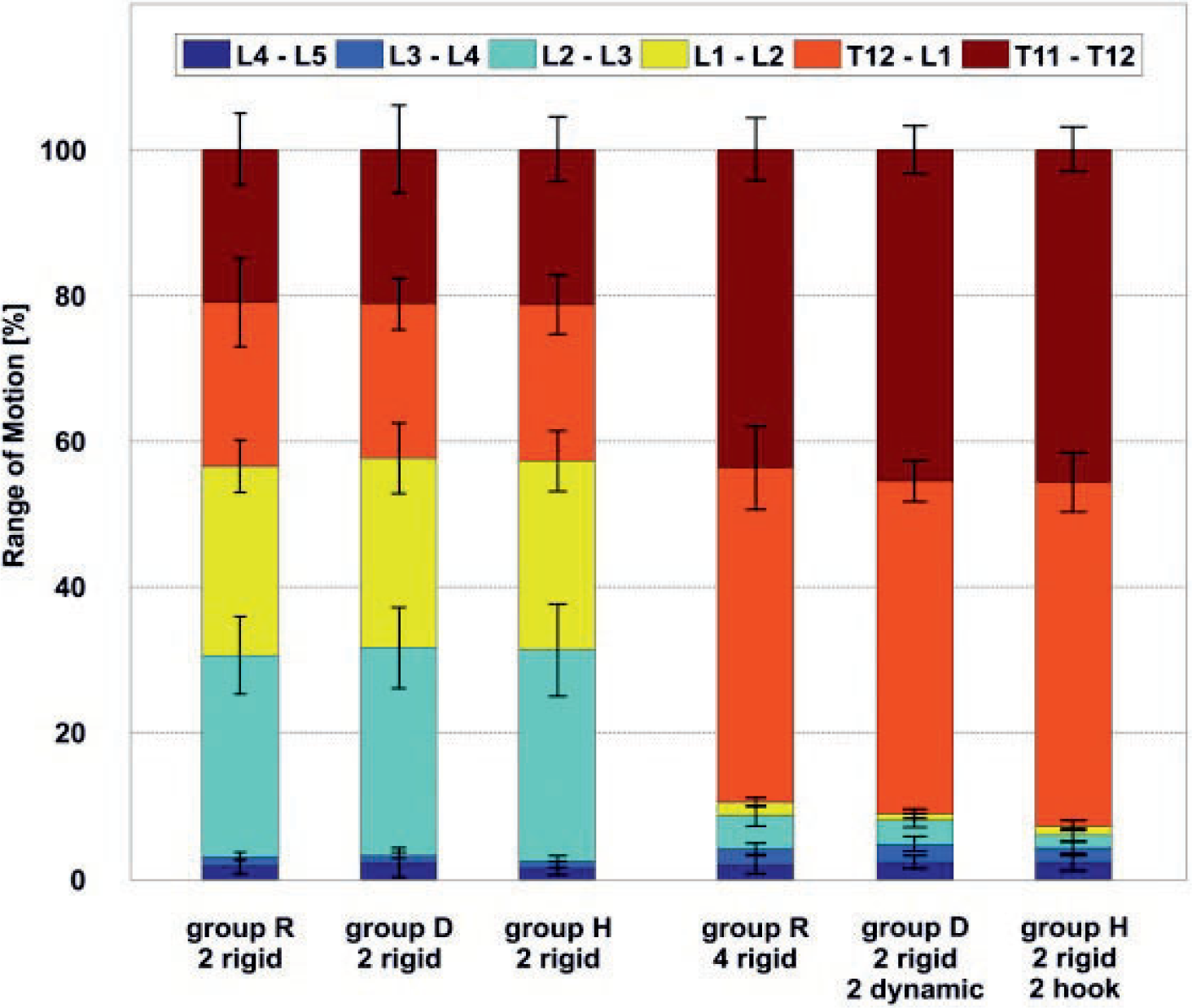
Overview showing the segmental range of motion (ROM) for every segment in any instrumented condition in percentage of total ROM. Please note that for a better visualization, the segmental ROM is shown as percentage of total ROM. The statistical analysis was performed with the degree values. Group R: four-level rigid instrumentation; group D: two-level rigid instrumentation (L3–L5) combined with the Elaspine system (Spinelab AG, Winterthur, Switzerland) (L1–L3); and group H: two-level rigid instrumentation (L3–L5) combined with laminar hooks (L1–L3).
On the other hand, a significant difference between ROM of the instrumented (L1–L5) and adjacent segments (T11–L1) among all groups was observed. The Tukey post hoc test showed that the adjacent segments (T11–T12 and T12–L1) are a homogenous subset compared with the other four segments (p < 0.001).
Discussion
With an aging population, the incidence of degenerative spinal disorders rises. Simultaneously, the number of spine surgeries performed increases. 28 Long pedicle screw constructs are used in the lumbar and thoracolumbar spine to treat these conditions. The perceived increase in accelerated adjacent-level degeneration following spinal fusion has provided the impetus for the development of motion-preserving or “dynamic” devices. This study investigated the effect of two different long hybrid constructs on the instrumented and adjacent spinal segments. To the best of the authors' knowledge, this study is the first to evaluate the effects of a long four-level hybrid construct on the lumbar spine and the thoracolumbar junction. Due to the orientation of the facet joints, the lumbar spine mainly moves in the sagittal plane. 29 Therefore, this study focused on the principal direction of movement, which is supported by Schmoelz et al, 21 because significant differences between movement in the sagittal and frontal plane were not observed.
The hypothesis that hybrid constructs limit the ROM in the dynamic instrumented levels but allow more motion than the rigid instrumentation could not be proven. The rigid instrumentation led to an overall decrease of 91% in ROM of the instrumented segments. This decrease appears to be even more severe if the contribution to the total ROM is regarded and considering that the overall moment was increasing during testing. There was no difference among the test groups with a two-segment rigid instrumentation. There was a decrease in segmental ROM (despite higher moments) at the instrumented segments. Obviously, in the chosen setup the adjacent segments showed an increase in segmental ROM. Although there was a small difference among the test groups between the rigid and hybrid instrumentations, this difference was not statistically significant. Furthermore, this difference is not relevant when compared with the noninstrumented segments (Fig. 4).
It is obvious that the relative ROM of the untreated segments (~4.55 degrees) is higher than the rigid segments L3–L5 (~0.22 degrees) or the “dynamic” segments L1–L3 (group R: ~0.21 degrees, group D: ~0.33 degrees, and group H: ~0.15 degrees).
Both the Elaspine system and laminar hooks reduced the ROM in the instrumented levels close to that of the rigid instrumentation, resulting in similar increasing mobility in the segments adjacent to the instrumentation. From the biomechanical point of view, the small differences between ROM among the three instrumentation types (rigid, dynamic, hook) can hardly be argued to result in differences in clinical outcome. In summary, the hybrid constructs used in this study cannot be recommended to prevent adjacent-level hypermobility and thus to reduce the possibility of ASD. These results confirm other studies that showed that hypermobility of adjacent segments increases with the number of instrumented segments. 22,30,31 As with other in vitro biomechanical studies, the results of the present work have to be carefully interpreted, because they were conducted in an idealized spine testing apparatus, where muscle forces and everyday loading patterns are difficult to mimic. 32 Naturally, in vitro studies are unable to describe the clinical effects such as pain and quality of life, which are dependent on several biological and physiologic factors including fusion rate, bony ingrowth of the pedicle screws, muscle regeneration, or wound healing and may only represent direct postoperative conditions. There is no consensus advocating a definitive method for testing the effects of spinal instrumentation in vitro. Some studies followed the recommendations of Wilke et al for in vitro stability testing of spinal implants and showed that the adjacent level is unaffected by fixation; the authors believe that for the testing of spinal implants, applying pure moments under load control is more appropriate. 27,32,33 Using the hybrid multidirectional test method of Panjabi to evaluate adjacent-level effects, two investigations showed increasing ROM in the adjacent levels of a rigid and hybrid construct. 22,34,35 This study used an angle-controlled movement of 5-degree flexion and extension with a free bending load applied at the cranial end of the specimen. Under the clinically derived assumption that a treated patient would try to preserve the preoperative spinal motion, the presented method was chosen to detect differences in hypermobility of the adjacent levels among the test groups.
The current study was conducted at room temperature, and the overall long-term effect of body temperature on the Elaspine system is unknown. Therefore, it is possible that the construct could influence spinal motion at body temperature. Some theories postulate a difference in PCU material stiffness properties between room temperature testing (25°C) and in vivo functionality (37°C). 10,36 Schmoelz et al had custom PCU tubes made in an attempt to approximate and account for the effects of the temperature difference. 32 Although the specific hardness of the PCU used in the device tested is uncertain, the Vicat softening points for Bionate Thermoplastic PCU are 78°C and 90°C, respectively. Assuming these values are representative, it is unlikely that the temperature difference between 25°C and 37°C will have a significant impact.
Little data is available on the biomechanical effects of laminar hooks, and very limited data is available on hybrid constructs using laminar hooks. Some retrospective studies (mainly in idiopathic scoliosis collectives) suggested that the use of hooks at the end of long constructs might be beneficial to prevent ASD or proximal junctional failure. 37,38
In this study, no potential benefit of laminar hooks regarding the prevention of ASD could be shown. Taking the disadvantages of laminar hooks into consideration, 39,40 they cannot be recommended to prevent hypermobility of adjacent segments.
There are some limitations in this investigation. It was not possible to test all different configurations on the same specimen because the structural design of the different implants prevented the interchanging of the different rods with the screw heads or hooks. Only one movement direction (extension or flexion) was investigated. This loading was chosen because in daily life extension and flexion play the most important role in spinal movement. Although previous studies indicate that there might not be a significant difference, it is not possible to transfer the results of extension and flexion to other directions of movement.
Conclusion
No relevant difference in ROM between the instrumented or adjacent segments among the test groups could be found. Thus, according to this data the use of hybrid instrumentation techniques in the lumbar or thoracolumbar spine with either laminar hooks or the Elaspine system to prevent ASD cannot be supported.
Footnotes
Disclosures
Peter Obid: none
Reza Danyali: none
Rebecca Kueny: none
Gerd Huber: none
Michael Reichl: none
Alexander Richter: none
Thomas Niemeyer: none
Michael Morlock: none
Klaus Püschel: none
Hüseyin Übeyli: none
Note
The study was funded by ASKLEPIOS proresearch (Hamburg, Germany).