
Abstract
Study Design
Narrative review.
Objective
Despite the numerous treatment options for vertebral compression fractures, a consensus opinion for the management of patients with these factures has not been established. This review is meant to provide an up-to-date overview of the most common treatment strategies for compression fractures and to suggest possible routes for the development of clearer treatment guidelines.
Methods
A comprehensive database search of PubMed was performed. All results from the past 30 years were obtained and evaluated based on title and abstract. The full length of relevant studies was analyzed for level of evidence, and the strongest studies were used in this review.
Results
The major treatment strategies for patients with compression fractures are conservative pain management and vertebral augmentation. Despite potential adverse effects, medical management, including nonsteroidal anti-inflammatory drugs, calcitonin, teriparatide, and bisphosphonates, remains the first-line therapy for patients. Evidence suggests that vertebral augmentation, especially some of the newer procedures, have the potential to dramatically reduce pain and improve quality of life. At this time, balloon-assisted kyphoplasty is the procedure with the most evidence of support.
Conclusions
Based on current literature, it is evident that there is a lack of standard of care for patients with vertebral compression fractures, which is either due to lack of evidence that a procedure is successful or due to serious adverse effects encountered with prolonged treatment. For a consensus to be reached, prospective clinical trials need to be formulated with potential new biomarkers to assess efficacy of treatment strategies.
Keywords
Introduction
In the United States, there are ∼1.5 million fractures attributed to osteoporosis every year. Among them are 700,000 vertebral fractures. 1 Vertebral compression fractures have a greater than 15% reduction in vertebral body height and are most often observed in the thoracolumbar transition zone. 2 Patients typically present with back pain and get diagnosed with a vertebral fracture following X-ray imaging. 3
Currently, many treatment options are available for the management of osteoporotic vertebral compression fractures. However, algorithms for determining the best treatment option have not been developed to help guide physicians treating new patients. In fact, the medical community is undecided as to what the optimal mode of treatment really is. The American College of Radiology has published some appropriateness criteria for the different management options, yet there is still a lack of consensus when it comes to developing a standard of care. 4 The only published clinical practice guidelines have been developed by the American Academy of Orthopedic Surgeons (AAOS), and of the 11 recommendations, only 1 has strong and 1 has moderate evidence backing them; 9 recommendations are weak or inconclusive. The strength of the AAOS guidelines depends on the amount and quality of data currently present: strong and moderate recommendations should generally be followed by clinicians, whereas limited and inconclusive recommendations have insufficient evidence backing them and therefore result in little help for practicing physicians, who are left relying on personal judgment. 5
In clinical practice, once a diagnosis is confirmed, the first line of treatment is usually conservative pain management with or without some degree of back support and physiotherapy.3,6 Percutaneous vertebroplasty and balloon-assisted kyphoplasty are the two commonly used minimally invasive vertebral augmentation procedures to restore normal vertebral height, reduce pain, and minimize deformity.3,4 Unfortunately, there are no clear guidelines defining at what point vertebral augmentation should be performed, and in fact, some authors have suggested utilizing these approaches prophylactically, even in nonfractured vertebral bodies. 7 Other studies have questioned their effectiveness and have proposed that the use of vertebral augmentation may not be beneficial at all when compared with conservative pain management.8,9 One significant reason for the current lack of quality evidence, which the AAOS encountered while developing the current guidelines, is the absence of a dependable biomarker that can predict the development of future compression fractures. This problem influences the ability of researchers to make reliable conclusions when evaluating the currently available treatment options.10–14
The primary purpose of this review is to provide a comprehensive up-to-date overview of the most commonly used treatment strategies for compression fractures, including newly developed vertebral augmentation procedures. The current lack of suitable biomarkers for osteoporotic vertebral compression fractures has led to a shortage of significant evidence in the field and has left physicians no choice but to rely on their own clinical expertise when helping patients. Therefore, a secondary purpose is to suggest avenues for future research that could lead to the development of new biomarkers that could eventually help in the establishment of clearer guidelines for treatment.
Methods
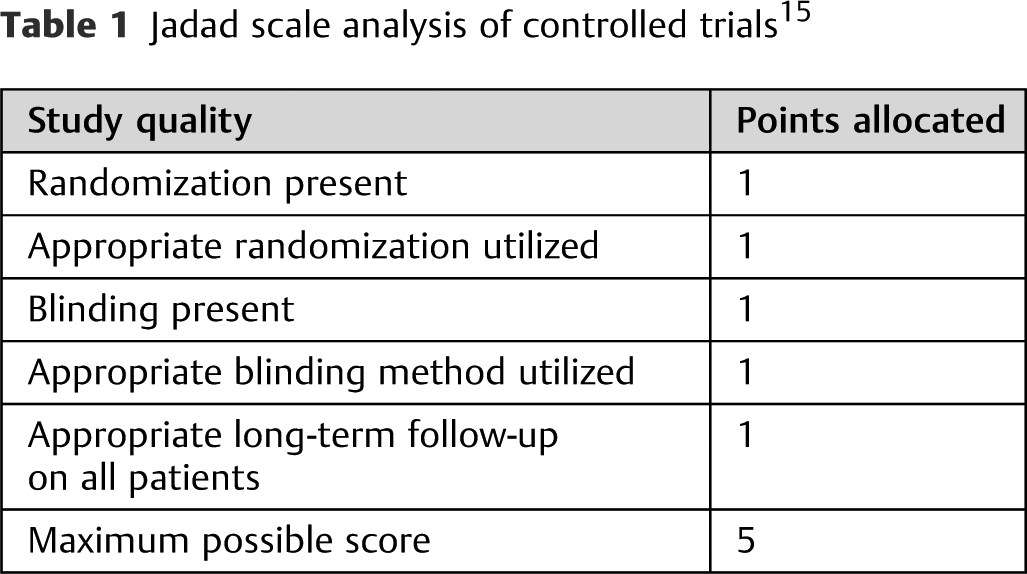
A comprehensive electronic database search of PubMed was performed using the terms “management,” “vertebral compression fracture,” “NSAIDs,” “pain control,” “bracing,” “thoracolumbar compression fractures,” “osteoporosis treatments,” “antidepressants analgesic effect,” “opioid analgesics,” “bisphosphonates,” “calcitonin,” “calcitriol,” “teriparatide,” “PTH,” “physiotherapy,” “physical therapy,” “vertebroplasty,” “kyphoplasty,” “finite element analysis,” and “biochemical marker.” The medical subject headings “Fractures,” “Compression,” “Osteoporosis,” “Postmenopausal,” “Vertebroplasty,” “Kyphoplasty,” “Finite Element Analysis,” and “Braces” were also explored. All the terms were used both by themselves and in combination to provide a more encompassing literature review. All the results from the past 30 years were obtained, and the most relevant randomized, blinded control trial publications were scored using the Jadad scale (
Jadad scale analysis of controlled trials 15
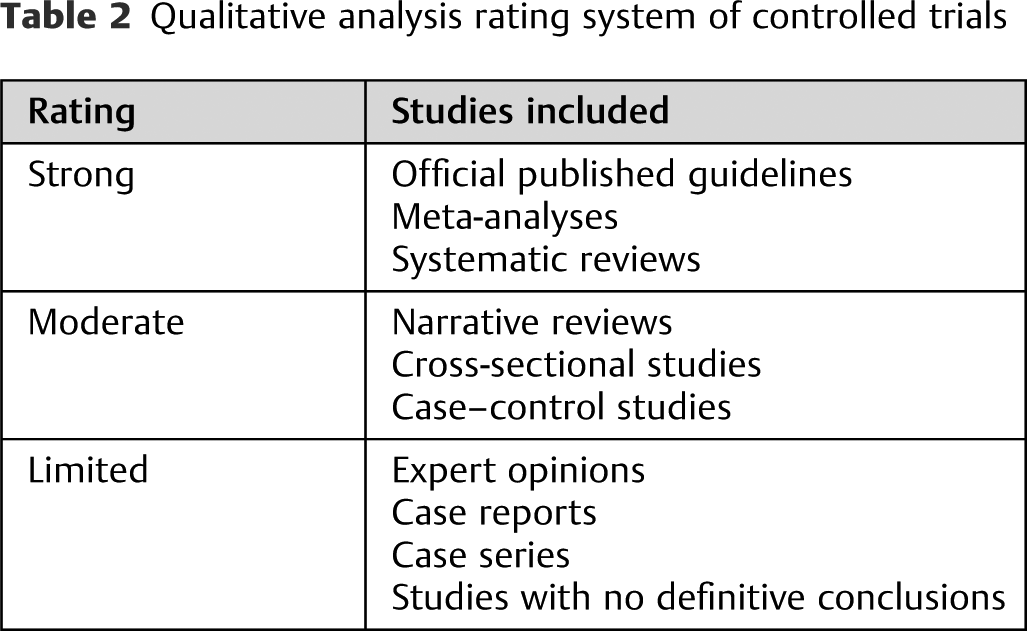
Qualitative analysis rating system of controlled trials
Conservative Pain Management
Overview
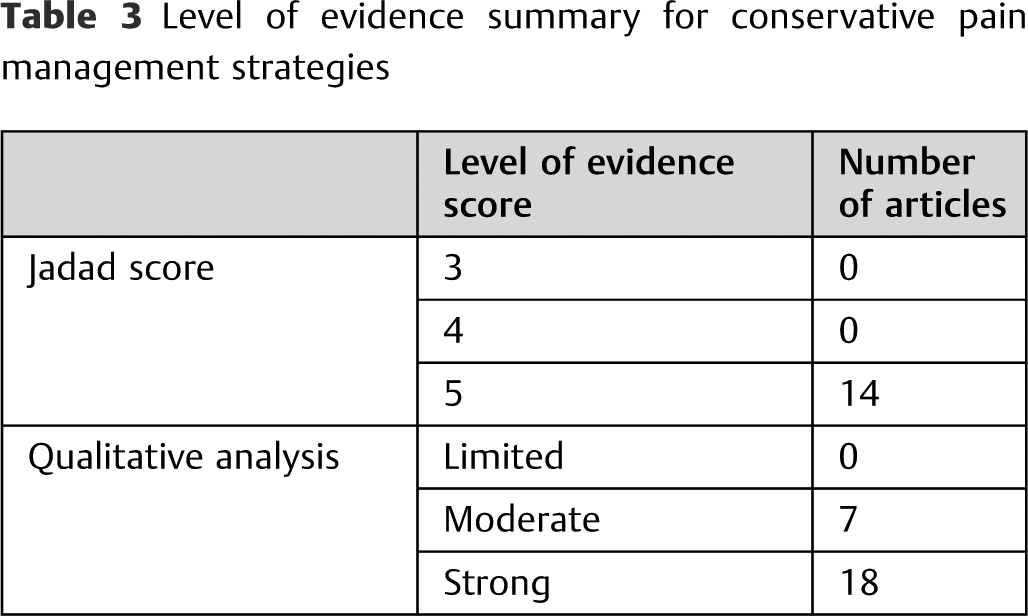
Conservative pain management is usually the first-line treatment for patients with vertebral compression fractures. In this review, there were 14 randomized clinical trials with a Jadad score of 5, 18 qualitative studies with a strong level of evidence, and 7 studies with a moderate level of evidence (
Level of evidence summary for conservative pain management strategies
A common disadvantage associated with conservative medical management of these patients is that vertebral height is not restored so there is no significant effect on residual deformity. 6 Thus worsening of the kyphotic deformity and further complications such as hyperextension of ligaments could occur, which could lead to the development of chronic back pain. 16 However, conservative medical therapy is a noninvasive method of treatment. Furthermore, most patients with these fractures will have spontaneous resolution of their chronic back pain within 8 to 12 weeks.2,4 Consequently, medical management has remained an effective initial treatment strategy.
Nonsteroidal Anti-inflammatory Drugs
NSAIDs are frequently the first medications used when treating spinal compression fractures. A likely reason for their widespread use is their perceived safety, low cost, and over-the-counter accessibility.3,17 However, some significant complications, such as gastrointestinal bleeding, renal impairment, and hemorrhagic cerebrovascular accidents, can arise from the use of NSAIDs, especially in older individuals. 18 A large study conducted in England examined 18,820 hospital admissions over the course of 6 months and found that the most common medications leading to hospitalization for adverse drug reactions were NSAIDs, which were implicated in 30% of the cases. 18 A comprehensive review of 65 medical trials, which encompassed a total of 11,237 participants, concluded that NSAIDs are indeed an effective treatment modality for short-term pain relief in people with both acute and chronic lower-back pain, even though the effects of the medication that were observed were small. 19 Despite the adverse events, clinicians continue to use NSAIDs as a first-line treatment option for spinal compression fractures, which is due in part to the incidence of more serious risks associated with other medications like opioids and tricyclic antidepressants. 17
Opioid Analgesics
The use of opioids for long-term pain control is still controversial. The current literature suggests that there is sufficient evidence that opioids are effective for significant short-term pain relief, but there is no substantial proof for their effectiveness in maintaining that pain relief over longer periods without incurring serious adverse reactions. 20 Some of the adverse effects associated with these medications are constipation, nausea, dependence, addiction, and overdose.4,21 These side effects can potentially lead to unnecessary anxiety, can cause discomfort, and may ultimately result in poor patient adherence to treatment. 21 In addition to these adverse reactions, long-term high-dose therapy with opioids can lead to more severe consequences like decreased immune function, opioid-induced pain sensitivity, and opioid-induced hormonal changes. 22 Consequently, the American Academy of Neurology has published a recommendation against using opioid pain medication in patients with chronic back pain. 20 Despite this recommendation, a meta-analysis of 41 randomized trials involving 6,019 patients concluded that opioids are an effective treatment option for patients experiencing chronic noncancer pain. However, the effects were only seen in those patients receiving strong opioids, and there was no evidence of functional improvement. 23 A randomized outpatient, double-blind, multicenter study found that both tapentadol, which is a centrally acting opioid agonist similar to tramadol, and oxycodone were effective in relieving acute lower back pain, with tapentadol being the more easily tolerated drug with fewer associated gastrointestinal problems. 21 A different study examining the two medications concluded that patient-reported bowel function associated with tapentadol treatment was significantly better than that associated with oxycodone, and in fact the gastrointestinal adverse effects were similar to what was seen in the placebo group. 24 Overall, it is evident that the chronic use of opioids is still not widely accepted, and there is no consensus on what the most effective treatment plan entails. By using safe clinical practices, such as limiting dosage and rotating the medication, opioid analgesics can still be a useful treatment for the management of severe pain due to acute compression fractures.
Antidepressants
Antidepressants, such as selective serotonin reuptake inhibitors, tricyclics, and monoamine oxidase inhibitors, are another possible option for chronic pain control. Although these drugs do have some analgesic properties, they are not primarily used for pain reduction and are used as adjunct therapy at a lower dose (30 to 50% normal dose) to achieve the desired effect.2,25 Limited data supports the use of antidepressants in these patients, but in a randomized, double-blind, placebo-controlled study, maprotiline, a norepinephrine reuptake blocker, successfully reduced chronic lower back pain. 26 Additionally, a month-long, randomized, double-blind study comparing the two different medications fluoxetine and amitriptyline with placebo determined that there was a statistically significant reduction of pain in both groups of patients who received the antidepressant treatments. 27 Although selective serotonin reuptake inhibitors are the safest antidepressants for older patients and are associated with the least side effects, the current literature suggests that they are not as effective at managing chronic pain as other drugs.26,27 However, a high proportion of these patients are older, socially isolated individuals who have existing body image concerns resulting from the kyphosis associated with these injuries. Consequently, a large number of these patients are more prone to depression. In fact, there is a 40% chance of depression developing in patients with chronic pain due to spinal compression fracture. 2 Because of this fact, physicians still utilize antidepressants as adjunct therapy in this patient population.
The long-term effects of using antidepressants to treat back pain are still unknown; however, recent data suggests that the use of antidepressants, even at low dosages, may actually be associated with decreased bone mineral density and increased fracture risk. 28 Therefore, further studies are necessary to determine if antidepressants are beneficial in the management of these patients and under what circumstances they would be best utilized.
Bisphosphonates
Patients with underlying osteoporosis and nontraumatic compression fractures will receive additional treatment to strengthen their bones and prevent additional fractures. Bisphosphonates, hormone replacement therapy, and supplemental calcium and vitamin D are commonly prescribed. 4 Conflicting evidence exists for the use of vitamin D (calcitriol) monotherapy, and it has yet to prove itself as an effective tool in preventing future compression fractures, but it is still often utilized in conjunction with other, more effective, medications like bisphosphonates.29,30 In a randomized, double-blind, controlled clinical trial comparing intravenous pamidronate, a bisphosphonate, and placebo for pain relief in recent osteoporotic compression fractures, the researchers concluded that even after just 30 days of use, there was a significant decrease in pain when patients were on the medication. 31 There is accumulating evidence that bisphosphonates, in addition to inhibiting osteoclasts, have a completely separate mechanism of action, which in the short run results in a reduction of inflammation by modulating peripheral or possibly even central nociception. 32 Though the details of this analgesic mechanism are still debated, these medications have shown promise in other painful conditions such as metastatic bone pain, complex regional pain syndrome, and even ankylosing spondylitis.33–35
In addition to the benefit of pain control, bisphosphonates can reduce the risk of new vertebral fractures. A study of 3,658 women with osteoporosis determined that women who received alendronate therapy for 3 to 4 years had a 48% lower risk of developing a fracture compared with those woman not receiving alendronate therapy. 36 Additionally, a separate double-blind, multicenter clinical trial of 414 patients with established osteoporosis showed that combination therapy of etidronate and alfacalcidol was effective in maintaining bone mineral density and reduced the incidence of new fractures. 37 Similar results were seen in another study investigating etidronate monotherapy as well. 38 However, the long-term use of bisphosphonates can cause oversuppression of bone turnover; therefore, patients taking these medications for significant periods of time are at an increased risk of nonspinal fractures, such as femoral shaft stress fractures.39,40
Calcitonin
Calcitonin is another effective medication used for pain management in compression fractures, especially when they are secondary to osteoporosis. 41 The treatment is available for subcutaneous administration, as a nasal spray, and even as a suppository. A recent meta-analysis of 13 studies with a total of 589 subjects concluded that calcitonin can significantly reduce pain and that it may even enhance functional outcomes. These results, however, were only observed in the patients with recent compression fractures, which was defined as onset of less than 10 days, and there was no convincing evidence to support the utility of calcitonin in patients with chronic pain. 42 The medication's exact mechanism of pain relief is still debated; however, the evidence suggests that calcitonin might act directly on the central nervous system by inhibiting neuronal excitation activity in response to peripheral stimuli. 43 Another popular hypothesis regarding calcitonin's analgesic mechanism of action is that it might increase β-endorphin levels in patients. This effect was noted in a study examining the clinical effectiveness of subcutaneous calcitonin on pain and quality of life. 44 Whatever the actual biochemical pathway may be, numerous studies have found the treatment to be successful in alleviating pain and improving the overall quality of life in patients with compression fractures due to postmenopausal osteoporosis.41,42,44,45 Moreover, a prospective, randomized, double-blind study of patients admitted for painful vertebral compression fractures found that synthetic human calcitonin is as effective in reducing pain as pamidronate. The researchers observed no short-term advantages to using the bisphosphonate and, due to the lower cost of treatment, recommended calcitonin as the preferred method of therapy. 45 The AAOS guidelines also agree with these findings and recommend with moderate certainty that calcitonin should be used in the management of compression fractures for at least 4 weeks after the initial onset of symptoms. 5
Teriparatide
Teriparatide is a recombinant form of the human parathyroid hormone (PTH) and was approved by the Food and Drug Administration for the treatment of osteoporosis in postmenopausal women in 2002. It is an injectable medication that works by encouraging the formation of new bone, thus increasing bone mineral density and reducing the risk of new vertebral fractures in patients with osteoporosis. 46 In a randomized study of 1,637 postmenopausal women with previously diagnosed vertebral fractures, PTH was shown to be effective at reducing the risk of both vertebral and nonvertebral fractures and was well tolerated by patients. Moreover, increases in vertebral, femoral, and total-body bone mineral densities were recorded. 47 A subsequent analysis of this trial concluded that because PTH decreases the risk of future fractures, participants actually had a reduced risk of developing moderate or severe back pain. 48 In a different study of 37 elderly women with multiple spinal compression fractures, teriparatide was found to reduce pain and disability due to back pain as measured by the visual analog scale and the Oswestry Disability Index, respectively. 46 Additional research looking at the medication has also confirmed the previous findings that say that it reduces pain and that it may be useful in protecting patients against developing new osteoporotic compression fractures. 49 Furthermore, teriparatide seems to be well tolerated with only some patients experiencing side effects such as headache and nausea. 40
Orthotic Bracing
Because spinal compression fractures involving the anterior elements of the spinal column are considered stable fractures and most patients remain neurologically intact, back bracing can be utilized during the recovery process. 2 Functionally, orthotic bracing helps to stabilize the injured area by inhibiting flexion of the spine thereby minimizing stress on the vertebra, allowing it to heal properly. 50 Commonly, braces are worn for up to 3 months, as longer periods of time can weaken core muscles.2,50 Because bracing has never been definitively shown to improve quality of life, its use among physicians remains controversial. A study looking at utilization of custom hard braces, custom elastic braces, ready-made elastic braces, and a lack of brace in 362 patients over the age of 65 found no significant difference in patient outcome for any of these treatment options. 51 Additionally, bracing is also known to cause sores, is associated with reduced pulmonary capacity, and, as mentioned previously, can lead to weakening of the core musculature.2,50 Furthermore, these braces are not comfortable for patients, leading to high rates of patient noncompliance. 51 One study, however, compared bed rest, the use of various orthoses, and physical therapy and demonstrated that out of the different nonoperative treatment options being studied, the patients who wore a brace for 6 weeks had the best outcome. 6 Despite the lack of clear evidence supporting the use of back bracing, it seems to be effective at managing some of the pain associated with compression fractures and remains a popular treatment option for many patients.
Physical Therapy
Often used in conjunction with the aforementioned treatment strategies, physical therapy remains a mainstay in the management of these patients. The goal of physical therapy is to strengthen back extensors and to improve overall posture and gait, which would help prevent subsequent falls and injury.52,53 Some studies suggested that weight-bearing exercise may also help to decrease edema after a vertebral fracture and may increase bone density in osteoporotic women.16,54 Bone mineral density alone, however, is not a good biomarker for the prediction of new vertebral fractures, and in fact a review on the effectiveness of exercise in improving the outcomes after osteoporotic compression fractures concluded that there is no definitive proof that patients who exercised had better outcomes. Many patients who did engage in physical therapy though, reported some pain relief and improved daily functioning. 54 The strength of back extensors and the lumbar spinal mobility have been established as important factors for quality of life in patients with postmenopausal osteoporosis.52,55 A cross-sectional study looking at thoracic kyphosis differences in older women concluded that the severity of the patients' kyphosis was likely associated with the degree of strength in their back extensor musculature. 53 This result suggests that physical therapy aimed at strengthening those muscles may be effective in improving the outcomes of patients with spinal compression fractures. In fact, a study investigating the effect of a home-based, low-intensity workout on back extensor strength in 80 postmenopausal women demonstrated that even simple exercise was beneficial in improving the strength of back musculature and as a result improving quality of life. 47 Other studies have suggested that exercise may be beneficial in controlling chronic pain.56,57 Unfortunately, it is extremely difficult to compare studies that examine physical therapy as a treatment option because of the immense difference in exercises being utilized, the order and duration of exercises, and the timing of each program. Just like bracing, the use of physical therapy to treat compression fractures is still controversial, and more research is needed to determine how to optimize its therapeutic value.
Vertebral Augmentation
Overview
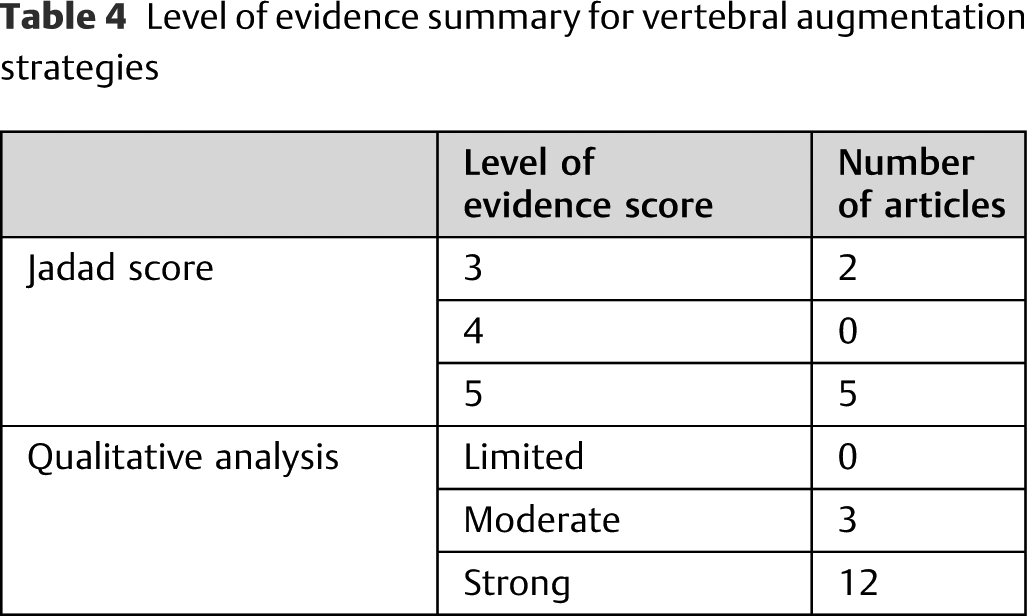
Vertebral augmentation includes a group of minimally invasive procedures used to reduce pain and stabilize compression fractures of the spine.
Level of evidence summary for vertebral augmentation strategies
The two most established vertebral augmentation procedures utilized in the treatment of spinal compression fractures are vertebroplasty and kyphoplasty. Some evidence has suggested that vertebroplasty might not be an effective procedure at all; therefore, the AAOS has recommended against its use.8,9 However, a rapidly expanding body of evidence supports the effectiveness of kyphoplasty for the surgical management of these patients. In fact, newer and improved methods of performing the procedure, like radiofrequency kyphoplasty and Kiva implantation (Benvenue Medical, Inc., Santa Clara, California, United States), have been developed that claim superiority to the traditional balloon-assisted method. More clinical trials are necessary, but the current preliminary evidence supports these claims.58–60
Vertebroplasty
Vertebroplasty is a short outpatient procedure that involves the injection of low-viscosity acrylic bone cement directly into a vertebral body, using a unipedicular or a bipedicular cannula. 4 The effectiveness of the procedure itself though is still in question, with a recent study concluding that percutaneous vertebroplasty was a procedure much better suited for simply improving stability of the spine than for pure pain relief. 61 Furthermore, in another study comparing vertebroplasty to sham treatment, vertebroplasty showed no benefit at 12- and 24-month follow-up visits. 62 Two additional multicenter studies showed the same results of comparable outcomes in patients who had vertebroplasty and those who did not.8,9 In addition to the questionable effectiveness of the procedure, vertebroplasty has been associated with a greater incidence of new fractures in adjacent vertebra when compared with conservative pain management. 63 Currently, the only strong recommendation given in the AAOS clinical practice guidelines for the treatment of symptomatic osteoporotic spinal compression fractures is that vertebroplasty should not be used. 5
Despite the evidence against the use of vertebroplasty, there is still some literature that supports the use of this treatment modality. A study monitoring the long-term effects of vertebroplasty found that when compared with conservative therapy, vertebroplasty showed clinically significant evidence of reducing pain and so reduced the need for pain medication and overall disability while still being reasonably safe. 64 A different trial focused on how vertebroplasty managed pain, how it affected patients' quality of life, and the incidence of new vertebral fractures. At 6- and 12-month follow-up in this study, both vertebroplasty and conservative therapy were effective in the management of pain and in the improvement of patient quality of life. However, this data demonstrates significantly better short-term pain relief and earlier improvements in vertebroplasty patients. 63
Kyphoplasty
Kyphoplasty is similar to vertebroplasty. It involves the same percutaneous unipedicular or bipedicular approach, but then a balloon dilation catheter is inserted and inflated to restore the vertebral body height and create a space for the low-pressure injection of high-viscosity cement. 4 Steinmann et al conducted a superiority study looking at unipedicular and bipedicular kyphoplasty and showed that the two approaches are similar when it comes to the restoration of the mechanical integrity of vertebra, but because the unipedicular approach provides reduced vertebral pedicle cannulation risk, operative time, radiation exposure, and even cost, it would be the advisable approach. 65 A study by Wang et al concluded that 98% of patients experienced pain relief 24 hours after surgery and that there was a demonstrated increase in mobility associated with surgical intervention. 66 Another study of 300 patients (149 kyphoplasty and 151 nonsurgical) determined that balloon kyphoplasty was more beneficial than nonsurgical therapy. Kyphoplasty improved patients' quality of life and mobility and reduced pain, all without increasing the chances of another fracture occurring in adjacent vertebra. 67 A retrospective study by Tolba et al examined the benefits of kyphoplasty. It was determined that the procedure increases vertebral height by nearly 42% and improves function while decreasing pain and the need for opioid analgesics. 68 Similar results were also obtained by Zarate et al, who observed a reduction in pain for the full 2-year follow-up. 69
A substantial amount of literature compares the two original vertebral augmentation procedures, vertebroplasty and kyphoplasty. A review by Lemke, based on case studies and clinical experience on the treatment of painful osteoporotic compression fractures, found that although both vertebroplasty and kyphoplasty may reduce pain and improve quality of life, kyphoplasty results in better mobility, corrects some deformities of the vertebral body, and restores part of its height. 70 A common concern to all vertebral augmentation procedures though, and a source of adverse reactions, is cement leakage from the vertebral bodies into the venous system. It was postulated that more precise control of cement flow may actually help minimize the risk of leakage into the basivertebral veins. 69 Newer methods of performing kyphoplasty promising fewer side effects are now emerging and address this concern.
Radiofrequency Kyphoplasty
Radiofrequency-targeted vertebral augmentation is a relatively new type of kyphoplasty. Instead of using an inflated balloon, ultra-high-viscosity cement is injected into channels created in the body of a vertebra using radiofrequency. This new method infuses the spine with cement at a much slower and more controlled rate, with the hope of ensuring minimal leakage of the cement. 58 Currently data suggests that this improved procedure may provide up to 50% reduction in the occurrence of adverse effects due to cement leakage when compared with standard kyphoplasty, which may be due in part to the improved control of the ultra-high-viscosity cement delivery and in part to the slower rate of delivery. 71 A retrospective study comparing radiofrequency-targeted vertebral augmentation and traditional balloon-assisted kyphoplasty determined that not only was radiofrequency kyphoplasty safe and effective, but it also reduced pain and resulted in much better overall long-term (2+ years) clinical outcomes. 58 Overall, the current literature suggests that increasing the viscosity of the cement being utilized in vertebral augmentation procedures decreases the adverse effects experienced by patients due to leakage into the venous system. Though further research is necessary, radiofrequency kyphoplasty could potentially prove to be a superior technique of performing this minimally invasive procedure in the future.
Polyether Ether Ketone Implants
Polyether ether ketone (PEEK) is a novel polymer with potential advantages when used in demanding orthopedic applications, such as the improvement of vertebral mechanical stability after a compression fracture. 72 Even though this biomaterial is new, a growing body of evidence shows it is suitable for load-bearing implants in the human body. 72 Kiva implants are a type of PEEK implant and have been used as an alternative to traditional kyphoplasty. This new percutaneous uniportal vertebral augmentation procedure was designed to restore the vertebral body height and reduce poly(methyl methacrylate) cement leakage. In this novel system, a coil is first inserted into the vertebral body, which acts like the balloon in a traditional kyphoplasty procedure and as a scaffold for the implant. The Kiva implant is then inserted around the coil, and the coil is removed. The cement is then injected through the implant itself, which is perforated at certain points, providing a much more controlled mode of delivery. 59 Otten et al evaluated the safety and efficacy of the Kiva system in comparison to balloon kyphoplasty and determined that it is indeed a safe and effective procedure for the management of patients with compression fractures. 60 After 6 months of having the Kiva implant, lower pain scores on the visual analog scale were recorded compared with patients who had undergone traditional balloon kyphoplasty. A larger, prospective, comparative, randomized study involving 82 patients who received the Kiva procedure and 86 patients who underwent balloon-assisted kyphoplasty concluded that both treatments resulted in significant increases in vertebral body height, but only Kiva also restored anterior vertebral body wedge deformities. The Kiva system also had a significantly lower rate of cement leakage. 59
The annual cost of osteoporosis to the U.S. health care system is estimated to range between 5 and 10 billion dollars. 1 The Kiva system has the potential to make a considerable impact in this area. The first economic analysis of Kiva implants for vertebral augmentation over regular balloons established that this new procedure has produced direct medical savings of over $1,000 per patient and over $280,000 per hospital. The Kiva implant system is associated with a reduced risk of additional compression fracture development, which is the likely origin of the medical savings. 73
Discussion
The literature search highlighted the numerous treatment modalities that are available to help patients with vertebral compression fractures. Even though some have considerable disadvantages associated with them, it is odd that there is still no developed standard of care, which can be attributed to the obvious need for a better surrogate biomarker for the condition. The most commonly encountered biomarker in the literature at this time was bone mineral density. Although an important determinant of bone strength, this biomarker by itself is not an effective predictor of future fractures because it does not factor in the microarchitecture, the intrinsic properties of bone and its composition, and the existing microdamage in the spine. 10 Some researchers have looked at bone turnover to assess the possibility of new fracture formation. Biochemical markers such as serum bone alkaline phosphatase, serum osteocalcin, urinary deoxypyridinoline, urinary hydroxyproline, and urinary cross-linked N-telopeptide of type I collagen are useful in determining if bone metabolism favors formation or resorption, which in turn could be used in overall risk assessments.11–13 Unfortunately, none of these biomarkers provide researchers with specific information about subsections of the spine that might have an increased probability of compression.
Newer imaging techniques that can better view the areas of the spine at a heightened risk for compression need to be developed, and further clinical trials have to be conducted before an optimal mode of treatment is obtained. In this way, the current treatment options can be better evaluated for effectiveness and the most appropriate treatment strategies can be determined.
For years, engineers have used finite element analysis (FEA) to estimate the behavior of complex structures. Such an analysis can be performed on a patient's vertebral bodies, which would allow researchers to determine the structural stresses experienced by those vertebra. With the advance of three-dimensional imaging technology, such as quantitative computed tomography, it is now possible to create high-resolution three-dimensional models of the human spine. 74 In essence, FEA breaks down complicated structures, like a patient's vertebral body, into a multitude of simpler elements, such as cubes. The more elements a model uses, the more accurate it becomes. Finite element models still take into account bone mineral density, but they also include geometry and loading conditions when estimating bone strength. 74 Graeff et al has conducted a study examining the effectiveness of teriparatide on vertebral body strength. 75 Instead of using only traditional methods like dual-energy X-ray absorptiometry to estimate the effects of the medication, this study performed high-resolution computed tomography scans on the patients and then used a newly developed finite element model to observe how subsections of the spine, which were weaker and prone to compression, responded to the therapy with time. 75 A different in vitro study conducted by Dall'Ara et al determined that finite element models are more sensitive and possess much more predictive power than traditional bone mineral density measurements, which makes it a superior tool for researchers in the field. 14 Further studies utilizing FEA could prove beneficial in investigating the effectiveness of other treatment modalities, like calcitonin, bisphosphonates, and vertebral augmentation. The actual effects of the different treatment options on the vulnerable areas of the spine at heightened risk for compression and the stress and strain forces at those locations can be quantitatively defined and compared with each other, which might ultimately result in a consensus on the most appropriate approach to managing spinal compression fractures.
Conclusions
Based on the current literature, it is evident that there is still a lack of standard of care for patients with osteoporotic vertebral compression fractures. Our results indicate that for patients with recent fractures, the use of calcitonin is advisable, along with bisphosphonates for prevention of new fractures. NSAIDs and opioids are effective in reducing acute pain, yet have to be utilized with caution due to all the possible adverse effects. Though antidepressants have been shown to decrease back pain in the elderly, further research is needed on patients with compression fractures to determine their appropriateness. Teriparatide, an injectable derivative of PTH, is also proving to be effective in controlling pain, increasing bone mineral density, and decreasing the risk for new compression fracture occurrence. Due to the inconclusive nature of the current evidence, physical therapy and orthotic bracing are still controversial methods of treatment. They also need further testing to determine how they can be best incorporated, if appropriate, in the treatment of compression fractures.
Summary of conservative management strategies
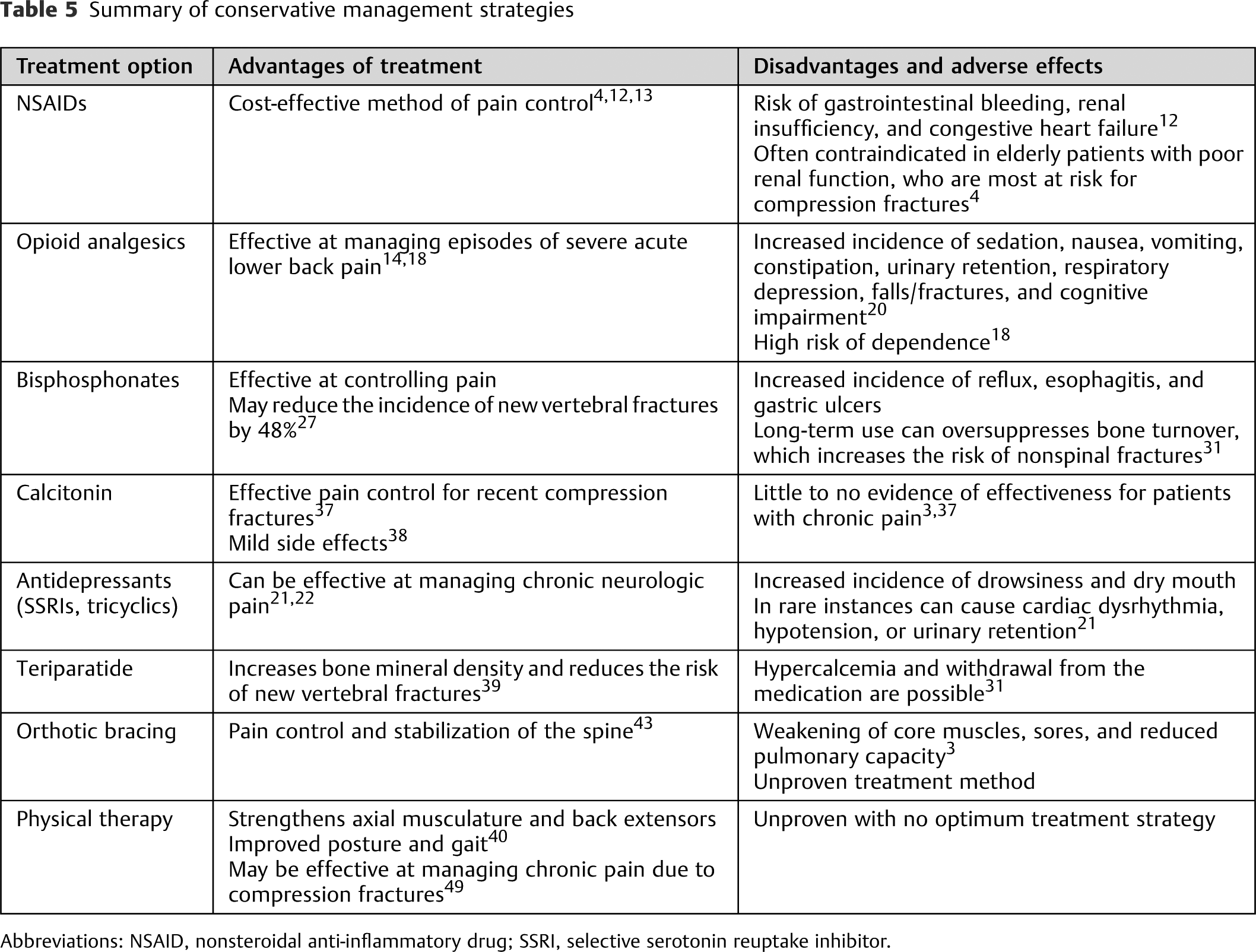
Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; SSRI, selective serotonin reuptake inhibitor.
The most appropriate implementation of vertebral augmentation procedures is still controversial, but evidence suggests that balloon-assisted kyphoplasty might be a very effective method of reducing pain and increasing quality of life, restoring vertebral height, and restoring most range of motion and function. The emergence of improved methods to perform kyphoplasty more cost-effectively and with less adverse reactions suggests that this procedure will most likely have an important role in the future standard of care of patients with compression fractures. Though vertebral augmentation procedures are indeed similar, vertebroplasty has yet to be conclusively proven to be effective in the management of spinal fractures, and based on the current literature, its use is not advisable.
Summary of evidence for vertebral augmentation procedures
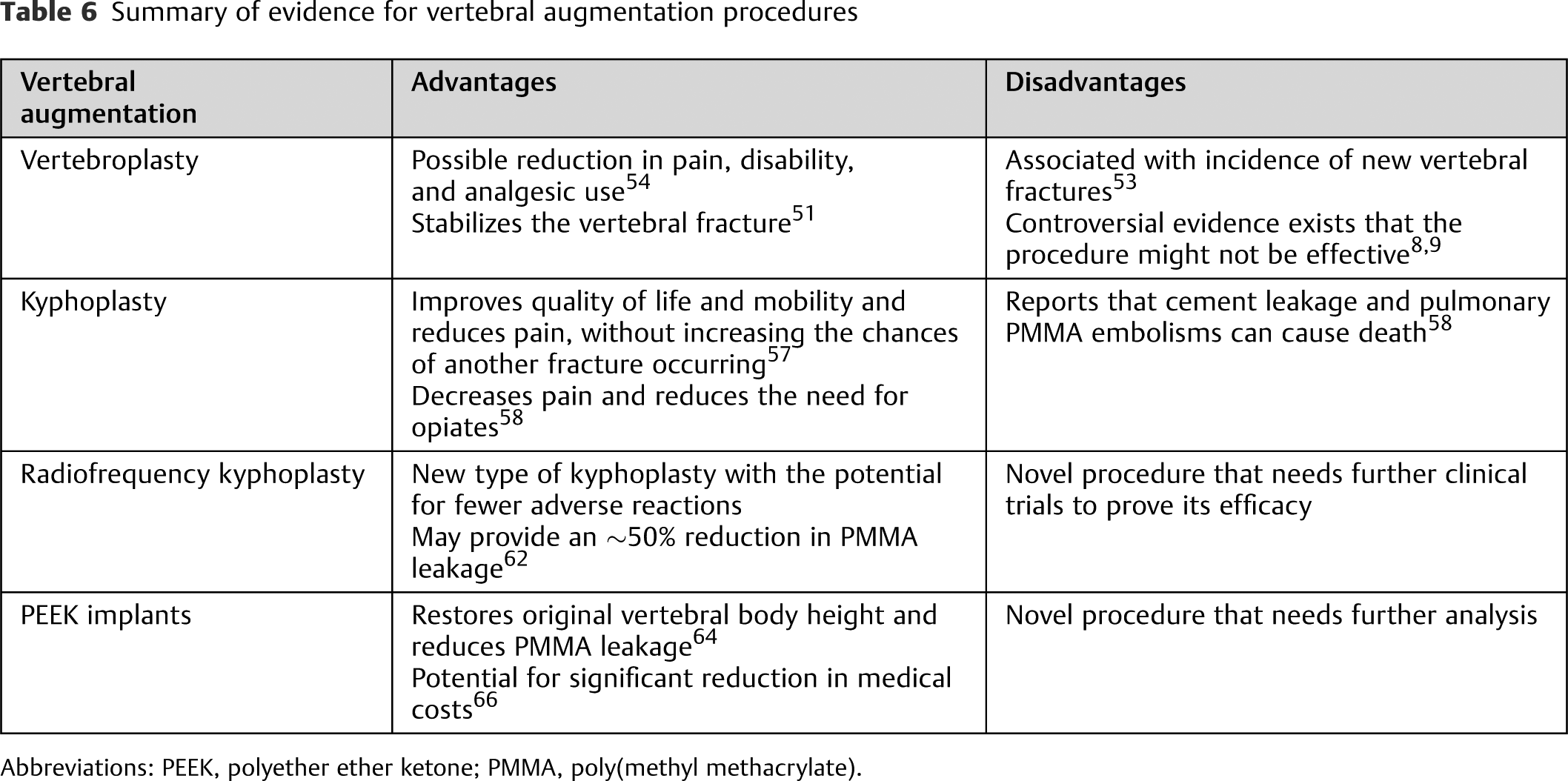
Abbreviations: PEEK, polyether ether ketone; PMMA, poly(methyl methacrylate).
One limitation to this review should be noted: numerous references cited have disclosures of industry funding, potentially biasing their results. We summarize these references and the disclosures that were made in
Summary of reference conflict of interest disclosures
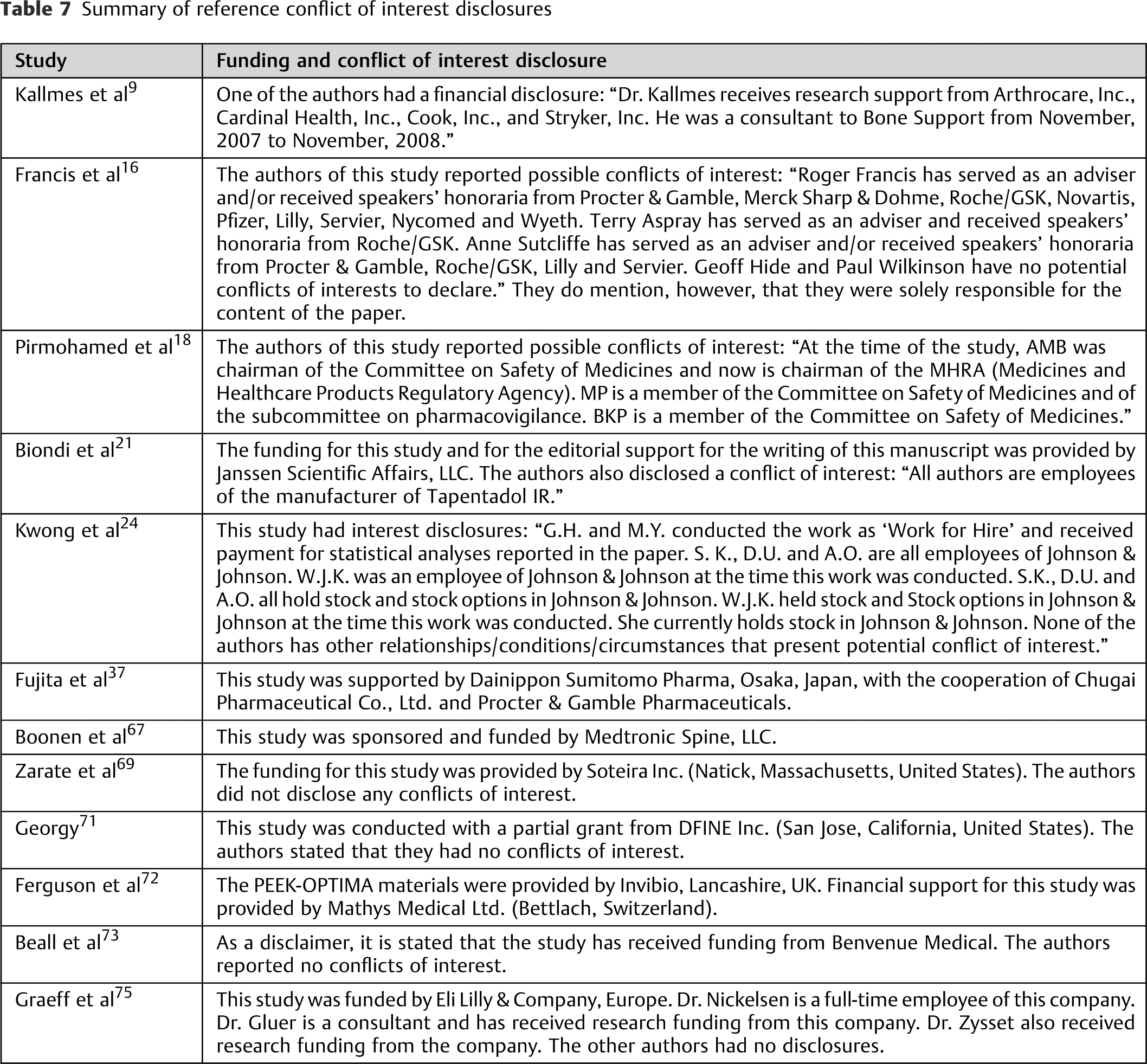
Despite receiving industry funding, which is a definite threat to internal validity, some studies did employ proper blinding and randomization, which can mitigate the aforementioned effects. Kallmes et al, for example, conducted a study examining vertebroplasty that randomized all 131 patients and was blinded to both the patients and the entire research assistant staff involved in patient follow-up after the procedure. 9 Biondi et al conducted a different study, which was also randomized and blinded. 21 The researchers examined the efficacy of tapentadol in treating lower back pain, but unlike the previous source, this study was conducted by tapentadol employees, dramatically increasing the threat to the study's internal validity. Kwong et al conducted yet another study examining the use of tapentadol; it also has authors with conflicting interests. 24 Consequently, as mentioned previously in the text, the use of opioids in the symptomatic management of lower back pain remains a controversial topic among physicians. Due to its uncommon practice, very few researchers have examined the use of opioids for lower back pain. Therefore, this review is unable to make recommendations on any long-term usage of the medications, and it merely summarizes the existing literature.
Other procedures that are not considered standard of care, such as newer vertebral augmentation techniques (e.g., radiofrequency kyphoplasty and polymer implants), also lack significant amounts of evidence. Studies like those published by Zarate et al, Georgy, and Ferguson et al may hold some potential for bias but were still utilized to provide a more comprehensive understanding of currently available treatment modalities and a possible glimpse at the future of the field.69,71,72
A different issue was identified by Pirmohamed et al, who performed a large prospective observational study to investigate the causes of adverse drug reactions in patients admitted to the hospital. 18 They examined 18,820 consecutive patients admitted to two different hospitals over the course of 6 months. The potentially biasing factor reported by these researchers was that two of the authors were members of the Committee on Safety of Medicines. The issue identified was not funding, but rather the safety of patients; therefore, this study was still deemed to have moderate strength and was utilized as evidence.
Finally, it is important to note the randomized controlled trial conducted by Graeff et al. 75 This substudy of a very large trial for postmenopausal osteoporotic women in Europe is an important reference used in the discussion section. Although it has some potential for bias because three of the authors received funding from Eli Lilly & Company, it examines a unique method of evaluating the efficacy of different treatment modalities through the use of a high-resolution computed tomography scan. The use of such an instrument by more researchers truly has the potential to influence the field and to ultimately solidify a treatment plan for patients, and further investigation of this topic is highly warranted.
Footnotes
Disclosures
Ivo K. Genev: none
Matthew K. Tobin: none
Saher P. Zaidi: none
Sajeel R. Khan: none
Farid M. L. Amirouche: Pending patent (62/166,480 “Method to Predict Spinal Compression Fractures”)
Ankit I. Mehta: Grant (AO Foundation Young Investigator Award); Pending patent (62/166,480 “Method to Predict Spinal Compression Fractures”)